
ABSTRACT
Social Determination of Health (SDH)/Collective Health is a Latin American framework that sees the Marxist core concept of social class as fundamental for understanding health inequalities. In contrast to social stratification approaches, Marxist proposals seek to understand health as part of the historical transformations of capitalism’s mode of production. In this article we aim to analyze the relationship between social class and health inequalities using data from the IV Oral Health National Study in Colombia. We conducted hierarchical cluster analyses to classify the population in five class positions and three living conditions clusters, which reflect how the spheres of production and social reproduction relate to social classes in Colombia. To measure oral health we use DMFT, as well as care and treatment needs indexes. Through variance analysis models we found that people from more exploited class positions and worse living conditions have more active disease and higher treatment needs. Despite technical and conceptual challenges, we conclude that a social class analytical framework can be operationalised via the interrelated spheres of production and social reproduction, which sheds light on the relationship between health inequalities and the class structure of the capitalist system.
This article is dedicated to the memory of Dr. Ignacio Méndez Ramírez, for his kindness and generosity sharing his wealth of knowledge.
Introduction
Even though Rudolph Virchow is considered the father of Social Medicine, Frederick Engel’s The Condition of the Working Class in England, published in 1845, stands as the pioneer study that merged critical political economy with morbidity and mortality analyses. Engels demonstrated with great level of quantitative and qualitative detail how the capitalist class structure at the hype of the industrial revolution in England not only influenced the poor health outcomes of workers (from the industrial, mining and agricultural sectors), but also affected the whole living conditions of the working class. At the factories, mines, or fields, men women and children faced over exploitative working conditions. In their neighbourhoods, they confronted misery, filth, famine, and disease. The prolific friendship between Engels and Marx gave rise to the most powerful theory to explain the contradictory nature of the capitalist system given that the two socially constituted classes, the capitalist and the proletariat, have opposing interests. It is precisely the Marxian grounding of social medicine which has allowed this interdisciplinary tradition to continue illuminating the relationship between capitalist accumulation patterns, class formation and struggle, and the health of the population.
While some social theorists have proposed ways to update the Marxian social class analysis considering the transformation of labour relationships, mode of production and class structure within the last fifty years (Portes & Hoffman, Citation2003; Wright, Citation2000), social medicine scholars have continued to unveil how the transformation of capitalist accumulation patterns influences health (Birn, Nervi, , & Siqueira, Citation2016; Breilh, Citation2007, Citation2010; Iriart & Emerson-Elias, Citation2017; Navarro, Citation1976, Citation2007; Waitzkin, Citation2016; Waitzkin, Citation2018). In particular, mental health, self-reported general health, health behaviours, and mortality are all health domains that exhibit differential outcomes with those whose employment relationships indicate higher rates of labour exploitation (the proletariat) exhibiting worse health in comparison to those who own the means of production (the capitalist) (Muntaner et al., Citation2010, Citation2012; Rocha et al., Citation2013). Importantly, however, several studies support Wright’s theoretical category of ‘contradictory positions’ of the ‘intermediary class’ that Marx characterised as the petit bourgeoisie (Wright, Citation2000). Middle managers and supervisors, the petit bourgeoisie, have less-favorable mental health outcomes than workers without authority or higher managers (Muntaner et al., Citation2010, p. 2138), which is very likely the result of their responsibilities to increase profits to the companies’ owners (the capitalists) by inflicting enhanced exploitation techniques on the workers (the proletariat). Given that a proper class analysis requires analytical abstractions from social relationships of production to the workings of the capitalist system, the studies that aim to unveil how social class influences health need to use ‘proxy’ indicators such as ‘employment relations’, ‘class position’, or ‘social insertion’.
While it is challenging to think of direct relationships between oral health and social class, we do know that the development of the capitalist system has shaped historical processes that influence oral health epidemiological profiles. Sugar, the most important cariogenic food, was perhaps the first transnational agribusiness built around slave work within the plantation economy of the Caribbean colonies (Mintz, Citation1985). Importantly, sugar consumption patterns around the world changed between 1650 and 1900. Sidney Mintz’s (Citation1985) groundbreaking ethnographic and historical study showed how sugar as a commodity went from being a privileged and pricy food consumed only by the monarchy and the imperial elites, or because of its ‘medicinal properties’, to becoming a cheap and popular ingredient constitutive of people’s diets around the world. Studies that inquire about changes in sugar consumption and presence of dental caries do demonstrate that the rates of this oral pathology grow hand in hand with higher patterns of sugar consumption and inadequate exposure to fluoride (Duque Naranjo & Mora Díaz, Citation2012). Currently, the WHO indicates that ‘the burden of oral disease is particularly high for the disadvantaged and poor population groups in both developing and developed countries’ (Petersen, Bourgeois, Ogawa, Estupinan-Day, & Ndiaye, Citation2005, p. 661). Epidemiological studies in different countries demonstrate an association between socioeconomic variables and the greater presence and severity of oral diseases among poor and marginalised social sectors (Bernabe & Hobdell, Citation2010; Medina-Solís et al., Citation2006; Vettore, Marques, & Peres, Citation2013; Zurriaga, Martínez-Beneito, Abellán, & Carda, Citation2004).
While we know that these stratification indicators, such as level of poverty, do not correspond to a social class analysis, we find them informative as they show that oral health inequalities do exist between social groups hierarchically differentiated by income and property assets. Hence, our task for this study is to bring a social class analysis to oral health and inquire if the social structure of the capitalist system does or does not reflect unequal patterns in oral health.
In order to advance in our task and before moving on to the methods and results sections, the remaining of the introduction presents: first, a brief synthesis of the historical transformation of the class structure in Latin America and Colombia. Then, we offer a summary of how social class has been operationalised for statistical analysis. Last, we discuss briefly our efforts to assess oral health from a Marxist framework, particularly from the Latin American Social Medicine tradition.
Class structure in Latin America and Colombia: a brief synthesis
As a difference from the high levels of employment that characterised Europe during the second half of the twentieth century, Latin American countries maintained low levels of formal employment and high levels of informality and agricultural labour. The persistence of so-called ‘traditional, backward, secondary, residual or marginal sectors of the economy’ characterised what came to be known as underdeveloped economies (Petersen et al., Citation2005, p. 661). Assessing this level of ‘economic development’, however, requires an understanding of the consolidation of a class system in the region after independence. In Colombia, which has important resemblances to other countries in the region, the agroindustrial class became the dominant fraction of the bourgeoisie. During most of the nineteenth and twentieth century, industry owners entered into conflict and partnership with the other fractions of the capitalist sectors: landowners for agricultural and livestock businesses, commercial sectors, and financiers, all of whom were consolidating their economic and political power (Misas Arango, Citation2002; Ogliastri & Guerra, Citation1980; Ospina Vásquez, Citation1979; Safford & Palacios, Citation2001; Sáenz Rovner, Citation2007). Although with some changes in composition and regional differences, these capitalists class fractions have since maintained power, in part because the class struggles of the different fractions of the proletariat have been dominated by the bourgeoisie ideology. Also, leftist social movements and parties that have represented the interests of the proletariat have become political victims of the many cycles of civil and military violence (Cardenas, Citation2010; Misas Arango, Citation2002; Safford & Palacios, Citation2001; Sáenz Rovner, Citation2007).
As it happened in other countries in the region, during the mid-twentieth century, Colombia changed its economic policies towards a model known as ‘import substitution and industrialisation’, which transformed in important ways the regional class composition (Misas Arango, Citation2002). A rapid urbanisation process resulted in a significant, albeit partial, increase in formal employment. Indeed, by 1980, unemployment and underemployment (self-employed and unpaid family members) comprised around 40% of the economically active population (EAP) (Couriel, Citation1984; PREALC, Citation1991). The agricultural sector shrank to only 32% of the EAP (Couriel, Citation1984; PREALC, Citation1991). Only 47% of the EAP in non-agricultural sectors had formal employment and, consequently, paid taxes (PREALC, Citation1991), which meant both union protection and access of social security.
As a way to reduce informal labour and decrease unemployment rates, neoliberal ideologues pushed market-based reforms during the 1980s and 1990s in the whole region. Governments, responding to the needs of global capitalist sectors (Waitzkin & Jasso-Aguilar, Citation2015) attacked unions and union contracts in order to impose new labour regulations that made labour ‘flexible’ (E. De la Garza, Citation2000; N. Klein, Citation2007). Changes in bargaining agreements altered work-related entitlements, working conditions, and employment relations, allowing for a reduced work force and a deregulated labour context characterised by temporal, third-party, and informal labour (Benach, Muntaner, Solar, Santana, & Quinlan, Citation2014; Cruces & Ham, Citation2010). Against neoliberal predictions, unemployment rates remained at high levels (De la Garza, Citation2000; Portes & Hoffman, Citation2003).
As a way to increase social security coverage, neoliberal ideologues proposed privatisation. These reforms offered national and transnational insurance companies new markets for their pension funds and their health and work-disability policies (Benach et al., Citation2014; Iriart, Elías, & Waitzkin, Citation2001). For those who could not afford private insurance, state-sponsored subsidies signified the direct transfer of public funds to private insurance companies (Iriart et al., Citation2001).
Social class and statistical analysis
While the historical situation in Colombia largely reflects the Latin American region, scholars highlight how the proximity of Colombian elites with International Financial Institutions, resulted in a deeper entrenchment of neoliberal logics around labour and social security (Garay, Citation1998; Restrepo, Citation2003). A challenge to analysis around social class and labour in the country originates in the ways in which labour-related indicators have been transformed under the new ‘business and accountability’ norms that regulate social life and state politics in neoliberalism (Centro de Investigaciones para el Desarrollo CID, Citation2006; Erikson, Citation2012). Indeed, the National Department of Statistics (NDS), and other public entities, have largely abandoned traditional work-related categories and replaced them with ‘occupation-related’ indicators. Official surveys define occupation as people who have worked at least one hour in the previous week, whether they received any economic compensation or not (DANE, Citation2014). Using some of the survey parameters, the NDS estimates that 47% of the occupied population are ‘informal laborers’ (DANE, Citation2018).
Scholars in economics and statistics have voiced their critiques with the new classification schemes, given their multiple technical and political problems. Not only has it become very difficult to trace working relationships, which impedes proper social analysis, but new classification schemes also obfuscate informality, underemployment, and unemployment (Centro de Investigaciones para el Desarrollo CID, Citation2006; Portes & Hoffman, Citation2003). Hence, updating the social class category needs to take into account: 1) the context of labour precarization and flexibilization previously described, 2) the rise of inequalities out of the concentration of capital in global elites (Robinson, 2004), and 3) the neoliberal disruption of national statistics that undermine labour as part of social class contradictions.
The most important challenge continues to be understanding the complexity and historical specificity of class relations within the shifting capitalist accumulation patterns. The other important challenge is to operationalise this conceptual framework (class relations within a class structure) into specific empirical studies, primarily those that are quantitative in origin. Portes and Hoffman (Citation2003) attempted to develop a new category of social class attuned to the neoliberal transformation of labour in the Latin American region. Their neo-weberian framework, which emphasises the position of subjects within the market, is important in that it shows the heterogeneity of social classes in Latin America given the coexistence of multiple modes of production (Naveda, Citation2014; Wright, Citation2015). Nonetheless, this classification is produced with data coming from labour national statistical reports, which results in a partial picture given that the unemployed, reserved army of labour in a Marxian framework, and other people outside of the production process such as retirees and rentiers are not included. Furthermore, a risk of Porter and Hoffman’s scheme is to conclude that people belonging to formal and informal labour have different class interests or that the neoliberal precarization of labour and informality has originated a class that is different from the proletariat (Elbert, Citation2015).
The issue of precariousness of labour and precariousness of material living conditions had been already presented by Engels and later conceptualised as part of Marx’s understanding of the fluidity and interconnectedness between the working class (formal and informal) and the reserve army of labour (Antunes, Citation2018, p. 2; Jonna & Bellamy Foster, Citation2016). While the nature of class relations needs to remain central, this does not negate that a neo-marxist analysis can benefit from incorporating other social science traditions. Wright (Wright, Citation2015), for example, proposes to integrate the Marxist analysis based on conflicts around the ownership of means of production with the Weberian analysis around rent distribution and market relationships, and with the other stratification schemes that highlight how individual levels of economic wellbeing and individual attributes are specific to different classes.
A recent neomarxist analysis in Colombia shows that the petite bourgeoisie in directorship positions and independent workers in Colombia have increased substantially from 1994 to 2010, which might be the result of changes in classification surveys, modifications in the organisation of industries or the new entrepreneurialism demanded of the professional class (Ó. Fresneda, Citation2016). They comprise as much as 36.6% of the EAP while the percentage farmers and workers without directorship roles in all sectors of the economy have shrunk (Ó. Fresneda, Citation2016).
Oral health and social class
Latin American Collective Health has long advocated for the importance of unveiling how capitalist social relationships influence the health-disease-treatment process of different population groups (Breilh, Citation2003; Laurell, Citation1982; López, Citation2013). Studies in Venezuela, Brazil, Argentina and Chile all indicate that health care outcomes in terms of prevention, health behaviour, or specific pathologies are influenced by social class (Benach et al., Citation2014; Muntaner et al., Citation2012; Rocha et al., Citation2013). Bronfman in México (Citation1984) and Breilh in Ecuador (Citation1989) respectively, operationalise Lenin’s social class definition to differentiate population groups. For Lenin, classes are ‘large groups of people distinguished from one another by [1] their status in an historically-determined system of social production, [2] by the proportion of the means of wealth production they possess, [3] by the part they play in the social organisation of labour, and [4] by the kind and the quantity of socially produced wealth they have at their disposal’ (Lenin, Citation1919). For Bronfman and Breilh, each of these four distinguishing aspects result in dimensions, which can be assessed with one or more qualitative variables (i.e. survey questions) and allow for conforming different class positions within the class structure. A version of this operationalisation of social class was used for data collection of the National Survey as we will later explain.
While it is difficult to explain how higher or lower rates of labour exploitation influence oral health, it is possible to see how the living conditions of workers and families allow them to care for their oral health in a way that disease is prevented or treatment is accessed in a timely way. Importantly, the relationship between poorer oral health outcomes and higher consumption of sugars that we eluded to before, speaks not only to the conditions of production (i.e. labour exploitation as the centre of the labour theory of value) but, importantly, to the possibilities for social reproduction (i.e. the reconstitution of worker’s labour power via food, sheltering, rest, and care). As such, we see that health, understood both as developing diseases and caring for one’s health, is at the core of the contradiction between production and social reproduction of the capitalist system (Fraser, Citation2016). On the one hand, profit depends on the exploitation of labour power and the conditions of workers’ exploitation directly affect each worker’s health (i.e. visual health, musculoskeletal health, environmental hazards, and so on). Furthermore, the rate of exploitation influences the progress of those diseases (i.e. amount of hours being exploited, higher productivity demands, and so on) (Breilh, Citation2003; Laurell, Citation1982). On the other hand, the social distribution of accumulated wealth influences the living conditions of the working class and sets up the possibilities for social reproduction including enough rest, sufficient and good quality food, and, importantly, the possibility to recover from disease to reconstitute the physical strength needed for work. As we approached our interest in connecting a social class analysis with oral health, we argue that it is best to approach oral health through the contradictions between production and social reproduction of the capitalist system (Fraser, Citation2016).
Jaime Breilh, one of the most reputed Latin American Collective Health scholars by bridging social class analysis with epidemiology, served as advisor in the IV National Oral Health Survey (ENSAB IV) in Colombia. The ENSAB IV survey is an adaptation of his class position classification proposal to the Colombian context. The ENSAB IV survey contained 13 class positions, which equates to what Breilh calls ‘social insertion’ (Breilh, Citation1989) in his own studies in Ecuador. Most importantly, however, Breilh has clarified that a proper social class analysis only occurs through a historical interpretation of the data. Hence data are meant to reflect ‘social insertion’ or ‘social position’ and only a Marxist analysis of such classification produces adequate interpretations of social class. Thus, the debate should not be about the best technical parameters included in a given instrument exclusively, but how to best merge data with a critical political economy framework. Data may always be insufficient or limited given technical difficulties and the changing landscape of the contradictions that characterise social relationships in Capitalism. We aim to propose one way to analyze the relationship between social class and health in Colombia and explore its potentials and limitations when using oral health as an example.
For oral health, then, we reiterate that it is of outmost importance to think about the sphere of social reproduction, both in terms of the possibilities to care for one’s oral health, the consumption patterns around healthy or unhealthy food, and the access to health care services which comprises prevention actions, treatment of oral disease (which also avoids further destruction of oral health tissues), and rehabilitation of already damaged tissues (Abadía-Barrero & Martínez-Parra, Citation2016). Our analysis made us realise that we needed an integrated approach in which social position based on class (sphere of production following Breilh’s initial proposal) had to be paired with the living conditions that make the proletariat more or less vulnerable to developing oral disease (sphere of social reproduction). It is this proposal which we will now explain in more detail.
Methods
The ENSAB IV methodology
ENSAB IV is a cross sectional study with a stratified and multistage sampling design. The sample size of 20.533 people represented the six geographical regions most commonly used for official surveys. The sample included people belonging to the following age groups 1, 3, 5, 12, 15 and 18; adults between the ages of 20 and 79; and pregnant women between the ages of 20 and 49.
Data collection instruments included four modules: 1) Household information, 2) sociodemographic data, 3) social determination, and 4) clinical exam. Data were collected during 2013 and 2014. A detailed description of the survey and data collection parameters can be found in the official report (Ministerio de Salud y Protección social, Citation2014a).
Population for this analysis
For the assessment of the influence of social class in oral health presented in this article we included the population between 20 and 79 years old only. The sample for this age group is 8040 people, which represents 29,444,964 Colombians (expanded sample). The sociodemographic characteristics of the population according to class position are included in .
Statistical analysis
Class position
Following Lenin’s definition of social class, Breilh proposes four variables to differentiate populations among different class positions. The ENSAB IV’s social determination module contained these variables: Occupational Category (17 categories), Income Source (16 categories), Possession of Means of production (6 categories), and Labour-related Tasks (4 categories). The original proposed algorithm should have resulted in 13 class positions. Because of data collection errors and unforeseen characteristics of labour flexibilization, informality and underemployment, a significant number of people could not be classified in any of the 13 class positions. In order to address this data problem, we decided to use a statistical technique that guided by contemporary debates around social class (briefly sketched in the introduction) allowed us to reclassify the total sample into new categories of class position. The reclassification also allowed us to reduce the original number of categories for the Occupational Category variable (from 17 to 7) and Income Source variable (from 16 to 8).
We found particularly appealing Wright’s integrated model to assess social class. We used hierarchical cluster analysis that included Breilh’s four original variables (that follow a more classic Marxist framework) and added the income and educational level of the main breadwinner, which are used by Wright and Bronfman in some of their analyses (Bronfman & Tuirán, Citation1984; Wright, Citation1985). To locate family members in a given class position, we used the breadwinner’s information.
We used hierarchical cluster analysis to reduce data dimensions, summarise data, and classify individuals into different groups. The main characteristic of the groups in a cluster analysis is their homogeneity (internal cohesion) and separation (external isolation) (Everitt, Landau, Leese, & Stahl, Citation2011; Johnson, Citation2000). For the hierarchical classification, data are split into a series of partitions, from 1 group with all individuals and to n number of groups with just one individual (Everitt et al., Citation2011). In order to assess the ideal number of clusters, we did a variance analysis among groups (F test). As dependent variables, we used all variables included in the clusters once they were standardised. We obtained the mean square error for different numbers of clusters and run a scree plot. (see ). The driver of our cluster analysis was social class, meaning that we only allowed the conformation of clusters that made sense for the class structure of Colombia.
Table 1. Description of class position clusters.
In addition to these class position clusters, we also wanted to include some ‘living conditions’ that could allow us to include a proxy for social reproduction into the analysis. Some Latin American Collective Health authors think of these differences as part of an ‘intermediate sphere’ that connects class structure with individual life styles (Almeida-Filho, Citation2000; Blanco & Sáenz, Citation1994; Breilh, Citation2010; Samaja, Citation2004). Wright’s integrated approach, in contrast, considers that living conditions (i.e. material conditions of existence, which include household characteristics and individual attributes) could also help define class positions (Wright, Citation2015). We also run a hierarchical cluster analysis of the following ENSAB’s living conditions variables, included in the household module: area (urban vs rural), socioeconomic strata, monthly household income, lack of money during the previous week to buy food, housing tenure, type of housing, and water supply variables. (see , results section.) We think of these living condition clusters as reflecting, albeit partially, how the sphere of social reproduction influences oral health care and consumption patterns. Importantly, given the historical conformation of social classes in Colombia, we wanted to unveil the differences between the precarious living conditions of the agricultural labour force as compared with the living conditions of the labour force and petite bourgeoisie in the cities.
Table 2. Percentage frequency distributions of sociodemographic characteristics and means and standard errors of the oral health indexes by class position.
Clinical indexes
In order to analyze clinical data we use 3 main indexes: 1) DMFT (Decayed Teeth + Missing Teeth + Filled Teeth), which is the index most frequently used and is recommended by the WHO to account for the severity of dental caries damage and treatment received (H. Klein, Palmer, & Knutson, Citation1938). 2) Treatment Needs Index (TNI = Decayed/decayed + filled). 3) Care Index (CI = filled teeth/DMFT). Both treatment needs index and care index measure access and equity in health care (Agudelo Suárez & Martínez Herrera, Citation2009). Our social class analysis drove the search for these indexes given that we wanted to see clinical evidence of worse oral health and worse access to health care. While we hypothesised the DMFT index obfuscated inequalities, TNI and CI should make inequalities evident. Worse care and treatment indexes should indicate higher consumption of unhealthy foods, poorer prevention strategies, and poorer access to health care services.
Variance analysis model
The effects of social position and living conditions clusters in oral health were assessed with variance analysis models for each categorical variable (social position with 5 categories and living condition with 3 categories) and a different variance analysis model with both categorical variables and their interaction. Given the importance of age in oral health, we added age (continuous variable) as a co-variable in all the models. We run one model per each clinical index as a dependent variable using the stata 13.0 function for complex surveys (svy). In cases in which the interactions were not statistically significant, we run Sheffé tests for each of the principal effects on the dependent variables to compare the means within groups of the same variable (StataCorp, Citation2013).
Results
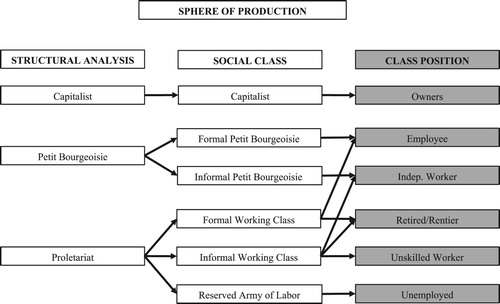
The cluster analysis in light of the theoretical debates around social class allowed us to group the sample in the following five class position clusters: Employee, Retired/Rentier, Unskilled Worker, Independent Worker, Unemployed. This National sample confirms what a review paper on social class and health found: it is almost impossible to include capitalist fractions in these samples, both because of their inaccessibility and also because of their small number as a percentage of the population (Muntaner et al., Citation2012). Hence, we are left with a range of fractions of the proletariat amidst a context of increasing precarization during neoliberalism and an increase in the ‘intermediary class’, meaning the petit bourgeoisie and independent workers (Ó. Fresneda, Citation2016). The characteristics of these clusters are presented in .
The sociodemographic characteristics of the population according to each class position are presented in .
shows the analytical correspondence between the social position clusters and social classes.
Figure 1. Class position as a proxy for social class.
The additional cluster analysis for living conditions generated three groups: Urban Adequate, Urban Precarious, and Rural Precarious. The characteristics of these clusters are presented in .
Table 3. Description of the living conditions clusters.
shows the analytical correspondence between the living condition clusters and social classes.
Figure 2. Living conditions as a proxy for social class.
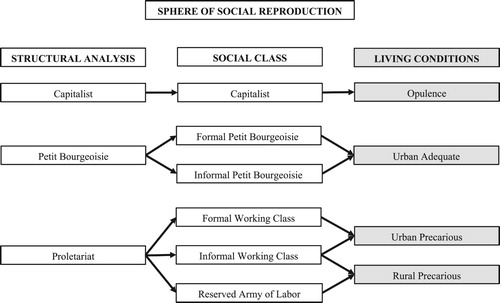
Importantly, with our diagrams we wanted to show two different expressions of how social class influence oral health. While for statistical analysis the most adequate comparison would be between the proletariat and the capitalist, we are forced to use the petite bourgeoisie as the contrasting class.
The distribution of the population according to class positions and living conditions can be found in .
Table 4. Distribution of living conditions by class position.
In order to assess oral health inequalities in relationship with class position and living conditions we did variance analysis models. In all of them we included age as a co-variable, given that it is well known that caries rates increase throughout the lifespan.
The variance analysis models for all oral health indicators (DMFT, TNI, and CI) including both class position and living conditions and their interaction resulted in models in which only living conditions was statistically significant for both TNI and CI. In order to assess if this result was due to a strong association between class position and living conditions, we conducted a correspondence analysis with a Pearson chi square test, which confirmed their association (p < 0.001). This result suggests that production (i.e. social position) and social reproduction (i.e. living conditions) are intimately related, which validates the importance of an integrated production/social reproduction approach. The correspondence between these two variables also prompted us to run separate variance analysis models, one for social position and another for living conditions, to assess their relationship with oral health.
DMFT (decayed, missing, and filled teeth)
Our DMFT variance analysis model for class position was statistically significant (p < 0.001, R2 = 0.37), meaning that class position and age have an effect on DMFT. The assessment of the principal effect of each of these two variables (class position and age) showed that class position no longer had any effect. Age did have a statistically significant effect (p < 0.01) and the correlation coefficient showed that for each year of age the DMFT increases 17%.
The variance analysis model for living conditions was also statistically significant (p < 0.01, R2 = 0.36), meaning that living conditions and age have an effect on DMFT. Similarly, the assessment of the principal effects showed that age, but not living conditions, had a statistically significant effect on DMFT (p < 0.01). In this case, the correlation coefficient showed that each year of age represents an increase of 16% in the DMFT.
These results are not surprising and confirm that DMFT is not the best indicator to assess oral health inequalities (Broadbent & Thomson, Citation2005). While it is very likely that people from different class positions and living conditions do exhibit significant differences in terms of the presence of active disease or the ability to access health care, DMFT obscures these differences by lumping together teeth with active disease and treated and lost teeth.
Treatment needs index (TNI)
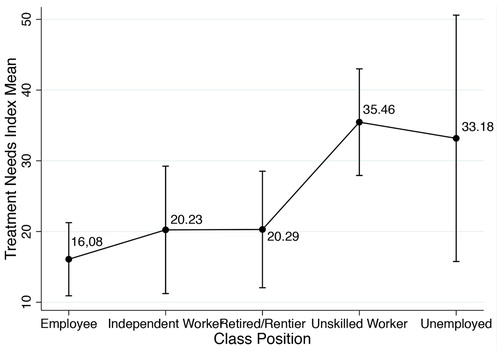
The variance analysis model for TNI (Decayed teeth/decayed teeth + filled teeth), class position, and age was statistically significant (p < 0.001, R2 = 0.05). In this case, class position, rather than age, was the statistically significant principal effect (p < 0.001). We used Sheffé test to compare TNI means among class positions. Statistically significant differences were found between Unskilled Worker and Employee groups (p < 0.001) and between Unskilled Worker and Independent Worker groups (p < 0.05) ().
Figure 3. Average treatment needs index by class position adjusted by age.
For living conditions, the variance analysis model was also statistically significant (p < 0.001, R2 = 0.06) and, as in the class position model, living conditions rather than age was the statistically significant principal effect (p < 0.001). The Sheffé test that compared means between groups confirmed that differences between all living condition groups were statistically significant (p < 0.001) ().
Figure 4. Average treatment needs index by living conditions adjusted by age.
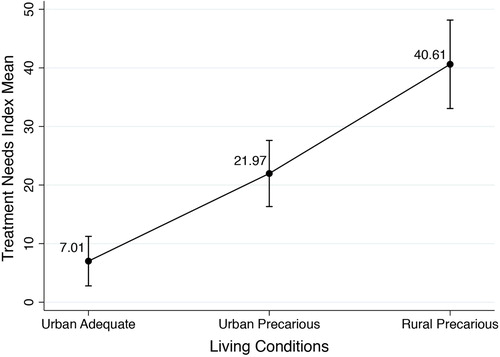
These results show that unskilled workers and the unemployed have more treatment needs than those who belong to the employee, independent worker, retired/rentier class positions. In addition, the results show that people belonging to urban precarious and rural precarious living condition groups have more treatment needs in comparison to those who belong to urban adequate living conditions.
Care index (CI)
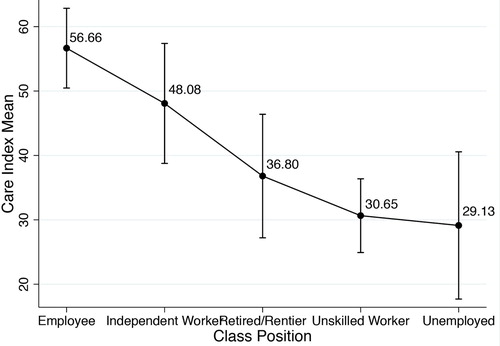
The variance analysis model for care index (filled teeth/DMFT), class position and age was statically significant (p < 0.001, R2 = 0.17). In this case both class position and age were statistically significant principal effects (p < 0.001). The correlation coefficient showed that for each year of age the CI reduces by 7.6%, meaning that with age people have either more active caries lesions or more missing teeth. Another way to explain this result would be that with age the proportion of filled teeth reduces in comparison with the proportion of teeth with active caries or teeth that have been extracted. This means that there is longer time of exposure to the event. In order to compare means among class position groups we run a Sheffé test. Statistically significant differences were found between Unskilled Worker and Employee (p < 0.001), between Unemployed and Employee (p < 0.01), and between Unskilled Worker and Independent Worker (p < 0.05) ().
Figure 5. Average care index by class position adjusted by age.
For living conditions, the variance analysis model was statistically significant (p < 0.001 R2 = 0.17), and both age and class position were statistically significant principal effects (p < 0.001). Sheffé test showed statistically significant differences among all living condition groups: between Urban Precarious and Urban Adequate (p < 0.05); between Rural Precarious and Urban Adequate (p < 0.001); and between Rural Precarious vs Urban Precarious (p < 0.001) ().
Figure 6. Average care index by living conditions adjusted by age.
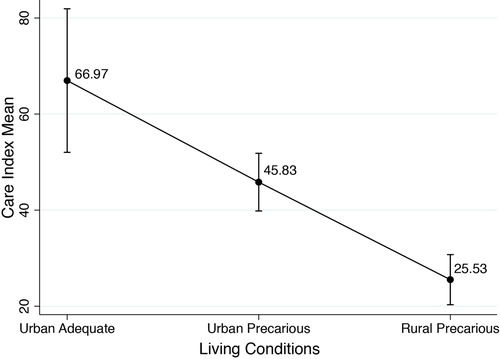
According to these results, people who belong to employee and independent worker class position groups have better care index than people who belong to unskilled worker and unemployed groups. This means that people in better class positions have more access to treatment, as measured in the percentage of filled teeth in comparison to active caries or missing teeth. In terms of living conditions, people with urban adequate living conditions have better care index in comparison to people with urban precarious and rural precarious living conditions. presents our final model that brings together the theoretical approach with the analyzed data.
Figure 7. Final model. Social class (production and social reproduction) and oral health.
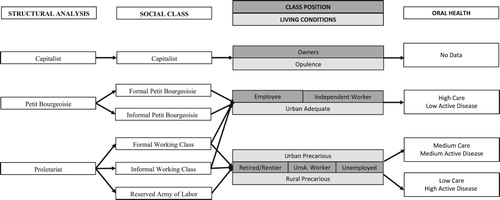
Both Class Position and Living Conditions are proxies for social class. Conceptually, one social class can manifest in two or more class positions or living conditions, which also corresponds statistically to the range of each of these categories. The range in findings regarding class position and oral health (expressed in this diagram as different connecting arrows) indicates that besides being statistically significant one class position can have different oral health outcomes. Interestingly, the range is less prominent and the differences among all groups are statistically significant when testing for the relationship between living conditions and care index. This finding might indicate that the sphere of social reproduction is a stronger predictor of access to care.
Discussion
The operationalisation of social class for statistical analysis brings many technical and conceptual challenges. It is very important to take into account the historical conditions of capital accumulation patterns, the transformation of labour dynamics, and the particularities of each country. As we mentioned in the introduction, the increasing rates of informal labour in Latin America as a result of neoliberalism come with an array of labour relationships in which lack of formal contracts, underemployment and self-employment are difficult to quantify in national statistics. Some authors recognise that the challenge to classify contemporary class positions resides in the difficulty to measure labour flexibility and informality. We experienced similar challenges classifying the population in different class position groups that allowed us to conduct a robust statistical analysis while maintaining a social class theoretical framework.
Portes and Hoffman (Citation2003) propose to correct the overestimation of formal employment by considering social security contributions. In their analysis for Latin America, the largest social class is the ‘informal proletariat’, which comprises 47% of the economically active population (EAP) and corresponds to people without social security coverage. For the Colombian context, we could not apply their proposal because of the extend of neoliberal social security reforms, which forced both formal and informal workers to contribute to the market of pension funds, health insurance, and work-related insurance.
The Colombian National Health Observatory follows the social class structure proposed by Fresneda (Citation2014) to assess the relationship between social class and health inequalities (Instituto Nacional de Salud & Observatorio Nacional de Salud, Citation2016). In their analysis, the ‘petite bourgeoisie’ represents around 30% of the EAP and corresponds to the largest social class in the country (Instituto Nacional de Salud & Observatorio Nacional de Salud, Citation2016). However, the authors of the reports of the observatory acknowledge that the petite bourgeoisie is a very heterogeneous group that includes different types of self-employment and other informal labour relationships. In addition, we believe that given the limitations of the national survey they use, they ended up including under ‘petite bourgeoisie’ different groups in terms of social position, income, rents and assets. Because of the framework of the ENSAB IV, we were able to include ownership of means of production. Furthermore, we considered that we could use Wright’s insights and statistical tools to add additional variables and increase the level of specificity among class positions. We added income and education levels of the breadwinner to produce the five class positions.
While we also wanted to add some characteristics of the living conditions to produce a simpler version of Wright’s integrated model (or to advance in the intermediate level according to the SDH proposal), the statistical analysis revealed collinearity between class position and living conditions. As such, we could not explain oral health inequalities as a result of an integrated class position and living conditions model. Two aspects are worth highlighting: 1) While this represents a setback in this kind of integrated proposal, we do not want to discourage further attempts to elaborate such integrated models. We think that thinking deeper about the interactions among the material conditions of labour, people’s living conditions, and oral health parameters can shed light into new ways to measure these interactions. We are planning to go back to our data and make new attempts. 2) The separate class position and living conditions models of oral health inequalities did produce remarkable results.
Our objective was to assess the relationship between social class and oral health inequalities and, in fact, we found that class relationships do influence the ways in which Colombian populations experience oral disease and access to treatment. Noticeable, the ENSAB IV did not report any data that could represent the class position of capitalist sectors. Thus, all of our class position groups reflect the different configurations of the proletariat and the petite bourgeoisie that are more or less exploited and have better or worse standing within the class structure of Colombian society. Finding a relationship between social class and oral health, however, was not only a matter of using adequate social position and living conditions categories. In several analytical sessions, we tried to understand how social class in Colombia influence oral disease progression considering the added difficulty that caries disease increases throughout the lifespan. Hence, we concluded that the sphere of production had to be more clearly linked with the sphere of social reproduction as care and consumption patterns seemed fundamental for Marxists analysis in oral health (Abadía-Barrero & Martínez-Parra, Citation2016). We discussed how the widely accepted DMFT index had the problem of lumping together active caries, with treated teeth and missing teeth, obfuscating the differential impact of the relationship between social class and access to health care. TNI and CI seemed more promising in allowing to grasp that relationship (Agudelo Suárez & Martínez Herrera, Citation2009). The results in fact showed that people who belong to class positions with higher levels of labour exploitation or are altogether excluded from even the most precarious forms of labour (the unemployed) do experience higher levels of active disease and less access to treatment. Other studies use descriptive statistics to report this relationship for specific ethnic or age groups (A. M. Franco & Ochoa, Citation2012; Morón & Córdova, Citation2008). While the ENSAB IV did report some differences in terms of class positions and other inequality indicators (Ministerio de Salud y Protección Social, Citation2014b), we were able to operationalise better class position and offer more robust statistical and social class analysis.
While living conditions are not a direct class structure indicator, we do know that the transformation of labour in Colombia during the last 50 years have resulted in a further pauperisation of rural areas and growing urban inequalities. We also know that historical access to treatment inequalities due to the lack of health care networks in rural and urban poor areas have increased due to the neoliberal health reforms (Franco Agudelo, Citation2003; Hernández, Citation2002a, Citation2002b). Thus, our results might indicate that class-based oral health inequalities are the result of not only the precarization of labour during neoliberalism, but also of the transformation of the living conditions of fractions of the proletariat (flexible agricultural workers versus flexible workers in urban settings). While the privatisation of the country’s health care infrastructure affected both of these class fractions of the proletariat, our data indicates that rural workers continue to exhibit more vulnerability to develop oral health and less access to treatment.
Conclusions
Conducting a social class analysis for collective health is not merely a technical discussion. Researchers working under a critical framework need to combine a robust social class analysis that considers how capitalist accumulation patterns transforms labour relationships across the globe, with efforts to operationalise social class concepts (such as class positions and living conditions), and a careful reading of the given health condition that they aim to study. In our case, the relationship between social class and oral health was possible by selecting carefully the best clinical indicators and by proposing a combined production/social reproduction framework in which both the transformation of labour conditions reflected in class positions and the correspondent living conditions of the population indicate unequal oral health outcomes. Indeed, statistically significant differences were found in more exploited classes for higher oral health care needs and lower access to oral health care treatment.
Importantly, our analysis of social class in Colombia does not include upper classes and other capitalist sectors. Rather than an error in terms of social class sampling or analysis, we think that this is the result of the global reconfiguration of labour in the new financialized economy with a capitalist elite in the global north and proletariat classes in the global south. Hence, our analysis points to differences among proletariat fractions by using the petit bourgeoisie as the ‘dominant’ class.
In spite of the precarization of labour, a sound social class classification proposal built on the contradiction between production and social reproduction and an adequate reading of the specific health condition can unveil important health inequalities.
Acknowledgements
We would like to thank Hanner Sánchez, Elizabeth Suarez, for their valuable contributions to understand technical issues from the ENSAB IV and Alejandra Moreno, Sergio López for their valuable contributions to think in oral health index and collective health. We also want to thank Jaime Breilh for his leadership role in advancing the understanding of how social class affect health and for his advisory role in the ENSAB.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
César Ernesto Abadía-Barrero http://orcid.org/0000-0001-7157-0842
Additional information
Funding
References
- Abadía-Barrero, C. E., & Martínez-Parra, A. G. (2016). Care and consumption: A Latin American social medicine’s conceptual framework to comprehend oral health inequalities. Global Public Health, 1–14. doi: 10.1080/17441692.2016.1171377
- Agudelo Suárez, A. A., & Martínez Herrera, E. (2009). La salud bucal colectiva y el contexto colombiano: un análisis crítico. Revista Gerencia y Politicas de Salud, 8, 91–105.
- Almeida-Filho, N. (2000). La ciencia tímida. Ensayos de Deconstrucción de la Epidemiología. Buenos Aires: Lugar Editorial.
- Antunes, R. (2018). The New service proletariat. Monthly Review, 69(11), 23. Retrieved from https://monthlyreview.org/2018/04/01/the-new-service-proletariat/ doi: 10.14452/MR-069-11-2018-04_2
- Benach, J., Muntaner, C., Solar, O., Santana, V., & Quinlan, M. (2014). Employment, work and health inequalities: A global perspective. Barcelona: Icaria Editorial.
- Bernabe, E., & Hobdell, M. H. (2010). Is income inequality related to childhood dental caries in rich countries? The Journal of the American Dental Association, 141, 143–149. doi: 10.14219/jada.archive.2010.0131
- Birn, A-E., Nervi, L., & Siqueira, E. (2016). Neoliberalism redux: The global health policy Agenda and the politics of cooptation in Latin America and beyond. Development and Change, 47(4), 734–759. doi: 10.1111/dech.12247
- Blanco, J., & Sáenz, O. (1994). Espacio Urbano y Salud. México: Universidad de Guadalajara.
- Breilh, J. (1989). Breve recopilación sobre operacionalización de la clase social para encuestas en la investigación social. Quito: CEAS.
- Breilh, J. (2003). Epidemiología crítica. Ciencia emancipadora e interculturalidad. Buenos Aires: Lugar Editorial.
- Breilh, J. (2007). Nuevo modelo de acumulación y agroindustria: las implicaciones ecológicas y epidemiológicas de la floricultura en Ecuador. Ciência & Saúde Coletiva, 12, 91–104. doi: 10.1590/S1413-81232007000100013
- Breilh, J. (2010). La epidemiología crítica: una nueva forma de mirar la salud en el espacio urbano. Salud Colectiva, 6, 83–101. doi: 10.18294/sc.2010.359
- Broadbent, J. M., & Thomson, W. M. (2005). For debate: Problems with the DMF index pertinent to dental caries data analysis. Community Dentistry and Oral Epidemiology, 33, 400–409. doi: 10.1111/j.1600-0528.2005.00259.x
- Bronfman, M., & Tuirán, R. A. (1984). La desigualdad social ante la muerte: Clases sociales y mortalidad en la niñez. Cuadernos Médico Sociales, 29/30, 53–75.
- Cardenas, S. (2010). Human rights in Latin America: A politics of terror and hope. University of Pennsylvania Press. Retrieved from http://www.jstor.org/stable/j.ctt3fhm05
- Centro de Investigaciones para el Desarrollo CID. (2006). Bien-estar y Macroeconomía 2002–2006, Crecimiento insuficiente, inequitativo e insostenible (p. 125). Bogotá: Universidad Nacional de Colombia.
- Couriel, A. (1984). Pobreza y subempleo en América Latina. Revista de La Cepal, 24, 39–62.
- Cruces, G., & Ham, A. (2010). La flexibilidad laboral en América Latina: las reformas pasadas y las perspectivas futuras (Colección documentos de proyectos) (p. 132). Santiago de Chile: CEPAL.
- DANE. (2014). Manual de recolección y conceptos básicos: Gran Encuesta Integrada de Hogares.
- DANE. (2018). Principales indicadores del mercado laboral. Marzo de 2018 (Boletín Técnico Gran Encuesta Integrada de Hogares) (p. 27). Bogotá.
- De la Garza, E. (2000). La flexibilidad del trabajo en América Latina. In E. (Coordinador) De la Garza (Ed.), Tratado latinoamerica de sociología del trabajo (1st ed.). México: COLMEX, FLACSO, UAM, Fondo de Cultura Económica.
- Duque Naranjo, C., & Mora Díaz, ÍI. (2012). La representación de la epidemiología de la caries en el mundo a través de mapas. Universitas Odontológica, 31(66), 39–48.
- Elbert, R. (2015). Informalidad en la estructura de clases de Argentina: ¿Es el proletariado informal una nueva clase social? Revisa Pilquen - Seccin Ciencias Sociales, 18(3), 50–65.
- Erikson, S. L. (2012). Global health business: The production and performativity of statistics in Sierra Leone and Germany. Medical Anthropology, 31, 367–384. doi: 10.1080/01459740.2011.621908
- Everitt, B., Landau, S., Leese, M., & Stahl, D. (2011). Cluster analysis. London: Wiley.
- Franco Agudelo, S. (2003). Para que la salud sea pública: Algunas lecciones de la reforma de salud y seguridad social en Colombia. Revista Gerencia y Politicas de Salud, 4, 59–69.
- Franco, A. M., & Ochoa, E. (2012). Caries dental e inequidades sociales: resultados de un estudio exploratorio en escolares de la comuna tres de Medellin.
- Fraser, N. (2016). Contradictions of capital and care. New Left Review, 100, 99–117.
- Fresneda, O. (2014). Clases sociales, modo de desarrollo y desigualdad: lineamientos para su análisis. Bogotá: Universidad Nacional de Colombia.
- Fresneda, Ó. (2016). Regímenes de acumulación, estructura de clases sociales y desigualdad en Colombia-1810-2010. Tesis Doctoral. Facultad de Ciencias (Tesis doctoral). Facultad de Ciencias Económicas, Universidad Nacional de Colombia, Bogotá.
- Garay, L. J. (1998). Colombia: Estructura Industrial e Internacionalización 1967–1996. Santafé de Bogotá: Departamento Nacional de Planeación y Colciencias.
- Hernández, M. (2002a). El debate sobre la ley 100 de 1993: antes, durante y después. In S. Franco (Ed.), La Salud Pública Hoy. Enfoques, y Dilemas Contemporáneos en Salud Pública. Memorias de la Cátedra Manuel Ancízar - I semestre 2002 (pp. 463–479). Bogotá: Universidad Nacional de Colombia.
- Hernández, M. (2002b). Reforma sanitaria, equidad y derecho a la salud en Colombia. Cadernos de Saúde Pública, 18(4), 991–1001. doi: 10.1590/S0102-311X2002000400007
- Instituto Nacional de Salud, & Observatorio Nacional de Salud. (2016). Clase Social y Salud (Octavo Informe Técnico) (p. 181). Bogotá: Observatorio Nacional de Salud.
- Iriart, C., Elías, E., & Waitzkin, H. (2001). Managed care in Latin America: The new common sense in health policy reform. Social Science and Medicine, 52, 1243–1253. doi: 10.1016/S0277-9536(00)00243-4
- Iriart, C., & Emerson-Elias, M. (2017). Disputas inter-capitalistas, biomedicalización y modelo médico hegemónico. Interface - Comunicação, Saúde, Educação, 21(63), 1005–1016. doi: 10.1590/1807-57622016.0808
- Johnson, D. E. (2000). Métodos multivariados aplicados al análisis de datos. México: International Thomson Editores.
- Jonna, R. J., & Bellamy Foster, J. (2016). Marx's theory of working-class precariousness: Its relevance today. Monthly Review, 67(11), 1. Retrieved from https://monthlyreview.org/2016/04/01/marxs-theory-of-working-class-precariousness/ doi: 10.14452/MR-067-11-2016-04_1
- Klein, H., Palmer, C. E., & Knutson, J. W. (1938). Studies on dental caries: I. Dental status and dental needs of elementary school children. Public Health Reports (1896–1970), 53, 751–765. doi:10.2307/4582532.
- Klein, N. (2007). The shock doctrine. The rise of disaster capitalism. New York: Metropolitan Books.
- Laurell, A. C. (1982). La salud-enfermedad como proceso social. Cuadernos Médico Sociales, 19, 1–11.
- Lenin, V. I. (1919). The great initiative, including the story of “communist saturdays”. Glasgow: Socialist Labour Press.
- López, O. (2013). Determinación social de la salud. Desafíos y agendas posibles. Divulgação Em Saúde Para Debate, 49, 144–150.
- Medina-Solís, C. E., Maupomé, G., Pelcastre-Villafuerte, B., Avila-Burgos, L., Vallejos-Sánchez, A. A., & Casanova-Rosado, A. J. (2006). Desigualdades socioeconómicas en salud bucal: caries dental en niños de seis a 12 años de edad. Revista de Investigación Clínica, 58, 296–304.
- Ministerio de Salud y Protección social. (2014a). IV estudio Nacional de Salud Bucal - ENSAB IV: Metodología y Determinación Social de la Salud Bucal (p. 195). Bogotá: Ministerio de Salud y Protección social.
- Ministerio de Salud y Protección Social. (2014b). IV estudio Nacional de Salud Bucal - ENSAB IV: Situación en Salud Bucal (p. 381). Bogotá: Ministerio de Salud y Protección Social.
- Mintz, S. W. (1985). Sweetness and power: The place of sugar in modern history. New York, NY: Viking.
- Misas Arango, G. (2002). La ruptura de los 90: del gradualismo al colapso. Bogotá: Facultad de Ciencias Económicas, Universidad Nacional de Colombia.
- Morón, A., & Córdova, M. (2008). Perfil epidemiológico bucal de las etnias venezolanas. Primer reporte nacional. Ciencia Odontológica, 5, 1–126.
- Muntaner, C., Borrell, C., Vanroelen, C., Chung, H., Benach, J., Kim, I. H., & Ng, E. (2010). Employment relations, social class and health: A review and analysis of conceptual and measurement alternatives. Social Science & Medicine, 71, 2130–2140. doi: 10.1016/j.socscimed.2010.09.038
- Muntaner, C., Rocha, K. B., Borrell, C., Vallebuona, C., Ibáñez, C., Benach, J., & Sollar, O. (2012). Clase social y salud en América Latina. Social Class and Health in Latin America, 31, 166–175.
- Navarro, V. (1976). Medicine under capitalism (1st ed.). New York: Prodist.
- Navarro, V. (Ed.). (2007). Neoliberalism, globalization, and inequalities: Consequences for health and quality of life. Amityville, NY: Baywood Pub.
- Naveda, A. (2014). Latinoamérica en el siglo XXI: clases y lucha de clases. Theomai, 29. Retrieved from http://www.redalyc.org/resumen.oa?id=12431432008
- Ogliastri, E., & Guerra, E. (1980). Fracciones de clase en la burguesía de ciudades intermedias de Colombia: un estudio sociológico. Revista Mexicana de Sociología, 42(4), 1631–1661. doi: 10.2307/3539964
- Ospina Vásquez, L. (1979). Industria y protección en Colombia, 1810–1930 (3ra ed.). Medellín: Biblioteca colombiana de ciencias sociales FAES.
- Petersen, P. E., Bourgeois, D., Ogawa, H., Estupinan-Day, S., & Ndiaye, C. (2005). The global burden of oral diseases and risks to oral health. Bulletin of the World Health Organization, 83, 661–669.
- Portes, A., & Hoffman, K. (2003). Las estructuras de clase en América Latina: composición y cambios durante la época neoliberal (Políticas sociales) (p. 51). Santiago de Chile: CEPAL.
- PREALC. (1991). Empleo y Equidad: El desafio de los 90. Santiago: OIT, Programa Mundial del Empleo.
- Restrepo, D. (2003). La falacia neoliberal: crítica y alternativas. Colombia: Universidad Nacional de Colombia.
- Rocha, K. B., Muntaner, C., Rodríguez, G., José, M., Baksai, P. B., Vallebuona, C., … Solar, O. (2013). Clase social, desigualdades en salud y conductas relacionadas con la salud de la población trabajadora en chile. Revista Panamericana de Salud Pública, 33, 340–348. doi: 10.1590/S1020-49892013000500005
- Safford, F., & Palacios, M. (2001). Colombia: Fragmented land, divided society. Bogotá: Norma.
- Samaja, J. (2004). Epistemología de la salud. Buenos Aires: Lugar Editorial.
- Sáenz Rovner, E. (2007). La ofensiva empresarial: industriales, políticos y violencia en los años 40 en Colombia. Bogotá: Universidad Nacional de Colombia. CES.
- StataCorp. (2013). Stata 13 base reference manual. College Station, TX: Stata Press.
- Vettore, M. V., Marques, R. A. d. A., & Peres, M. A. (2013). Desigualdades sociais e doença periodontal no estudo SBBrasil 2010: Abordagem multinível. Revista De Saúde Pública, 47(Suppl. 3), 29–39. doi:10.1590/S0034-8910.2013047004422
- Waitzkin, H. (2016). Medicine and public health at the End of empire (1st ed.). New York: Routledge.
- Waitzkin, H., & Working Group for Health Beyond Capitalism. (2018). Health care under the knife: Moving beyond capitalism for our health. Monthly Review Press. Retrieved from https://monthlyreview.org/product/health_care_under_the_knife/
- Waitzkin, H., & Jasso-Aguilar, R. (2015). Resisting the imperial order and building an alternative future in medicine and public health. Monthly Review, 67(3), Retrieved from https://monthlyreview.org/2015/07/01/resisting-the-imperial-order-and-building-an-alternative-future-in-medicine-and-public-health/ doi: 10.14452/MR-067-03-2015-07_8
- Wright, E. O. (1985). Clases. London: Verso.
- Wright, E. O. (2000). Class counts: Student edition. Cambridge: Cambridge University Press.
- Wright, E. O. (2015). Understanding class. London: Verso.
- Zurriaga, O., Martínez-Beneito, M. A., Abellán, J. J., & Carda, C. (2004). Assessing the social class of children from parental information to study possible social inequalities in health outcomes. Annals of Epidemiology, 14(6), 378–384. doi: 10.1016/j.annepidem.2003.06.001
