
ABSTRACT
Empowering women is presented as a key strategy to achieve several goals of the sustainable development (SDG) agenda, including child health. However, the literature on the subject shows mixed results and is limited regarding political empowerment. Responding to this gap, we explore whether women’s political empowerment is associated with positive health outcomes for children under 5 years of age. We use the V-Dem project’s ‘Women’s Political Empowerment Index’ (WPEI) in combination with selected SDG indicators of child health from the Institute for Health Metrics and Evaluation’s 2017 Global Burden of Disease, for 161 countries, between 1990 and 2016. We estimate fixed-effects regressions for the WPEI against child mortality, stunting and immunisation coverage, controlling for structural and socio-economic indicators from the SDGs and potential lagged effects. The WPEI is associated with improved nutrition and immunisation but its substantive effect is small. High-, low-income and least developed countries benefit more from the effect of women’s political empowerment on child mortality. The effect of women’s political empowerment on stunting is stronger in middle-income countries while its effect on immunisation is more relevant to low-income and least developed countries. Our study demonstrates the complexity of the relations between women’s political empowerment and child health.
Introduction
Ensuring a healthy start in life and promoting child health are essential to the health and wellbeing of future adults and of the next generation (Britto, Citation2017; Center on the Developing Child, Citation2010; Marmot et al., Citation2010; Wadsworth & Butterworth, Citation2005; Wang et al., Citation2017; Watkins, Citation2016). Children under 5 years of age are particularly vulnerable as their health and development rely heavily on their care-givers (Black et al., Citation2017), a role overwhelmingly undertaken by women (Duflo, Citation2012; Sen & Östlin, Citation2008). As a result, women’s status is likely to affect not only their own health and wellbeing but also their ability to fulfil their roles towards children. Hence, and aside from its own value, empowering women may improve women’s own health and also that of the next generation (UNICEF, Citation2015).
The World Health Organization (WHO) defines empowerment in health as ‘a social, cultural, psychological or political process through which individuals and social groups are able to express their needs, present their concerns, devise strategies for involvement in decision-making, and achieve political, social and cultural action to meet those needs’ (WHO, Citation1998, p. 6). Empowerment is not only a strategy to improve health in the long run and reduce health disparities, but also an outcome of health intervention itself. For example, there is evidence of the health effect of empowering initiatives as public health strategy (Sen & Östlin, Citation2008; Wallerstein, Citation2006; WHO, Citation1998). As they help address factors of inequities, improve programmes’ sensitivity to the community’s specificities or build community support, empowering strategies and citizen participation have been associated with improved effectiveness for specific development programmes, health services and services or programmes influencing health (e.g. education) (Wallerstein, Citation2006). Additionally, studies have directly linked empowerment and community participation with improved health outcomes such as child immunisation and utilisation of selected health services (Wallerstein, Citation2006).
In contrast, lack of empowerment is linked to poorer health through two mechanisms. First, exclusion, a lack of control or of agency are associated with social determinants of health, such as lower education, employment and access to services (Commission on Social Determinants of Health, Citation2008). Both aspects mutually reinforce each other, as being disenfranchised affects one’s capacity to access services and opportunities, while lower education, employment can affect one’s resources, agency and participation. Secondly, psychosocial factors resulting from disempowerment (e.g. financial insecurity, isolation) affect both physical and mental health. For example, prolonged stress caused by these factors has been associated with increased risks of cardio-vascular disease and obesity (Brunner & Marmot, Citation2005). In young children and pregnant women, exposure to toxic stress – which these factors of disempowerment can cause – affects a child’s brain development, exposing them to higher risk of poor mental and physical health later in life (Center on the Developing Child, Citation2010; Wadsworth & Butterworth, Citation2005).
There are ambitious expectations regarding the potential of empowering women to promote human development. Aside from being a desirable outcome in itself, women’s empowerment is presented as key to sustainable development (Duflo, Citation2012; Mason & King, Citation2001; United Nations, Citation2017). According to Sen and Östlin (Citation2008), gender power relations ‘are among the most influential social determinants of health’ as they determine one’s control over their health, the acknowledgement of their health needs and the realisation of their right to health. The 2030 Agenda for Sustainable Development, which all UN members have committed to, includes a goal (SDG) dedicated to achieving gender equality, with one target aiming to ‘ensure women’s full and effective participation and equal opportunities for leadership at all levels of decision-making in political, economic and public life’. The 2030 Agenda also highlights the contribution of women’s empowerment to achieve progress in and across the other goals (United Nations, Citation2017).
In this study, we explore whether a specific type of women’s empowerment − political empowerment − is associated with improving the health of children under the age of 5 years, a goal reflected in several targets of SDG 3. We address the following question: Is women’s political empowerment associated with positive child health outcomes?
First, in order to develop a conceptual framework that can guide our analysis, we review the potential mechanisms of action linking women’s empowerment – and political empowerment in particular – with health outcomes found in the empirical and theoretical literature. Then we detail the data and method used in this study. After presenting the results of our analysis, we further discuss these findings in relation to the wider context of the SDGs before highlighting key take-away messages from this empirical study.
Women’s political empowerment and child health: a review of empirical evidence
The concept of women’s empowerment
Women’s political empowerment is part of the wider concept of women’s empowerment, the complexity of which has led to inconsistencies in the way it has been defined and measured in the literature (Cunningham et al., Citation2015; Pratley, Citation2016; Sundström et al., Citation2017; Wallerstein, Citation2006). Some of the literature, such as the World Bank’s report on Engendering Development (Mason & King, Citation2001), focuses on the enablers and barriers of equality between men and women. In their report analysing women's contribution to human development, the World Bank highlights gender inequalities in ‘rights, resources and voices’ (Mason & King, Citation2001, p. 2). Other organisations and researchers have acknowledged the political dimension more directly when exploring the link between women’s empowerment and health. In their analysis of power inequalities, the WHO Commission on Social Determinants of health (CSDH) (Citation2008) identifies the political dimension as one of the four major fields where inequalities manifest themselves, alongside economic, social and cultural dimensions. In his systematic review, Pratley (Citation2016) identifies the political dimension as one of the five main dimensions of women’s empowerment, noting that the economic and social/cultural dimensions tend to be over-represented in the literature compared to the political, psychological and legal dimensions. Wallerstein’s (Citation2006) evidence review notes that most of the literature focuses on psychological empowerment, which encompasses political efficacy alongside collective efficacy, outcome efficacy, critical thinking ability and participatory behaviour. These differences in definitions affect the comparability and meta-analysis of studies exploring the impact of women’s empowerment on health (Cunningham et al., Citation2015; Pratley, Citation2016; Sundström et al., Citation2017; Wallerstein, Citation2006). They also make it harder to draw general conclusions as to the impact of women’s empowerment on specific outcomes, such as child health.
Limitations of the current evidence base on political empowerment and child health, and opportunities for research
Review of evidence
There is a growing body of literature looking at links between women’s empowerment and child health outcomes. Their findings are often mixed, with variations according to contexts or countries, aspects of child health and measures of women’s empowerment. Overall, markers of women’s social and economic empowerment such as women’s education or literacy, decision-making power and to a lesser extent, economic power or control over economic resources and assets are associated with improved child health outcomes (Carlson et al., Citation2015; Cunningham et al., Citation2015; Duflo, Citation2012; Hosseinpoor et al., Citation2018; Kuruvilla et al., Citation2014; Richards et al., Citation2013; Sen, Citation1999; Taukobong et al., Citation2016; Thorpe et al., Citation2016). The effect of political empowerment and participation has been far less studied (Pratley, Citation2016), also reflecting the wider lack of studies linking empowerment and citizens participation to health and healthcare outcomes (Wallerstein, Citation2006). This also reflects the proportionally fewer studies measuring the effect of women’s empowerment beyond the individual level (Pratley, Citation2016). However, the Success Factors for Women’s and Children’s Health studies on the Millennium Development Goals related to maternal and child health have highlighted the contribution of women’s political participation (a component of women’s political empowerment) as one of the structural factors linked to improved child and maternal heath in low- and middle-income countries (Kuruvilla et al., Citation2014).
Limitations and gaps in current research
As previously mentioned, the effect of women’s political empowerment remains under-researched as compared to the other dimensions of women’s empowerment. Secondly, most studies focus on the empowerment of mothers rather than women when exploring the link between empowerment and child health, thus ignoring the role of other female members in the family in child welfare or the broader role of women and girls in the community. Thirdly, the vast majority of the literature covers only selected low- and middle-income countries and has found significant variations in results from one context to the other (Carlson et al., Citation2015; Pratley, Citation2016; Richards et al., Citation2013; Taukobong et al., Citation2016; Thorpe et al., Citation2016). These studies also mainly study correlation, not causality, between women’s empowerment and child health or service utilisation outcomes (Taukobong et al., Citation2016). Finally, while several studies find promising results linking components of women’s empowerment, they also highlight the need for further research (Pratley, Citation2016; Richards et al., Citation2013; Taukobong et al., Citation2016; Wallerstein, Citation2006).
Contribution of the present study
The present study responds to that need both conceptually and empirically. Conceptually, the framework presented below describes the potential pathways through which women’s political empowerment, acting as a meta-determinant of health, may impact child health through the improvement of women’s status at different levels. Empirically, our analysis aims to fill several of the gaps identified in the literature. We focus on the link between women’s political empowerment and child health at the global level. Thus, our approach addresses the geographical gap previously observed and the comparative lack of research focusing specifically on political empowerment, beyond simple political participation. As described in the method section, our analysis also controls for and compare the actual effect size of structural determinants of child health, including markers of women’s social and economic empowerment, that have been associated with child health in previous research. While this approach does not allow us to conclusively prove or disprove causal relations between women’s political empowerment and child health, it enables us to isolate the specific effect of women’s political empowerment while controlling for other mechanisms at play.
Women’s political empowerment and child health: a conceptual framework
This section presents the theoretical and conceptual literature relevant to political empowerment and health, which has informed the development of our conceptual framework.
The political determinants of health: a review of theoretical and conceptual literature
The second half of the twentieth century has seen a growing number of epidemiological theories and frameworks highlighting the importance of political systems and politics as structural determinants of population health (Krieger, Citation2011). In their report on the determinants of health, the WHO CSDH highlights the pivotal role of political empowerment as ‘aspects of empowerment that underpin social well-being and equitable health’ (CSDH, Citation2008, p. 155). As a result, the CSDH considers interventions addressing the social determinants of health as intrinsically political, with changing power relations (and the shifting of powers in favour of disadvantaged groups) as a fundamental component in addressing health inequities. To operationalise its recommendations, the CSDH developed a framework (see ) based on three main epidemiological theories: social production of disease and political economy of health; psychosocial approaches; and ecosocial theory (Solar & Irwin, Citation2010). All of these theories consider health and diseases distribution as societally contextualised and health outcomes are socially patterned. Social production of disease and political economy of health theories emphasise the role of political and economic institutions in shaping society and the distribution of health within it. Psychosocial theories highlight the individual’s perception of social condition, status and interaction and how that perception, especially the psychosocial stress resulting from the social environment and hierarchy, can trigger biological response harming physical and mental health. Finally, while recognising the role of biological and social pathways in health, ecosocial theory focuses and the interaction between organisms, populations and their environment, highlighting the dynamic relationship between a person’s biology, society and environment over time, and how this relationship can affect their health (Krieger, Citation2011). While they emphasise different pathways and factors affecting one’s health, all these theories insist on the multiple layers of determinants affecting health (as the CSDH framework shows) and the crucial role of power and power relations between different groups in these processes (CSDH, Citation2008).
Figure 1. The CSDH conceptual framework (adapted from CSDH, Citation2008).
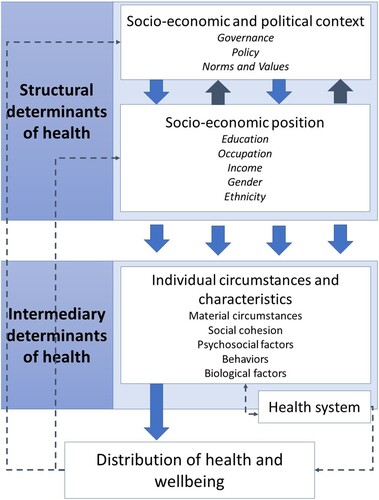
While not exclusively focused on political determinants, this framework does highlight the structural role that the political context and political decisions are likely to have on other determinants of health. Indeed, according to Amartya Sen (Citation1999), political rights (including political and social participation) are not only instrumental in making people’s voices heard and having political leaders address people’s needs, but also contribute to shaping a society’s values and priorities as well as making informed political choices. Based on this ‘constructive role’ of political rights, the political empowerment of women would allow the development of values and priorities that are beneficial to women’s agency, which Sen associates both with improved women’s wellbeing and improved child survival (Sen, Citation1999).
The role of political empowerment and participation in shaping health is also addressed by theories exploring the role of voters or supporters in influencing public policy. These theories look at survival strategies of political leaders, arguing that leaders stay in power by rewarding their supporters either financially or with policies that benefit or match the expectations and needs of this group (Bueno de Mesquita, Citation2011; Wigley & Akkoyunlu-Wigley, Citation2017). From this point of view, empowering women and making their voices more influential would encourage leaders to design and invest in policies that respond to women’s preferences, needs and concerns. These are seen as more family-friendly or oriented towards improving the status of women in the community and in the household (thus indirectly impacting the status of women as caregivers) (Duflo, Citation2012; Sen, Citation1999). Empowering women in political life and encouraging their participation may also impact leaders’ decision and policies through another pathway. Political leaders who rely on wider groups of supporters to stay in power are more likely to invest in public goods, including those influencing or improving health (Bueno de Mesquita, Citation2011; Wigley & Akkoyunlu-Wigley, Citation2017). As women make up half of the world population, empowering them and supporting their political participation increases the size of political leaders’ supporter group, thus making them more likely to invest in public goods.
Women’s political empowerment as a meta-structural determinant of child health: our conceptual framework
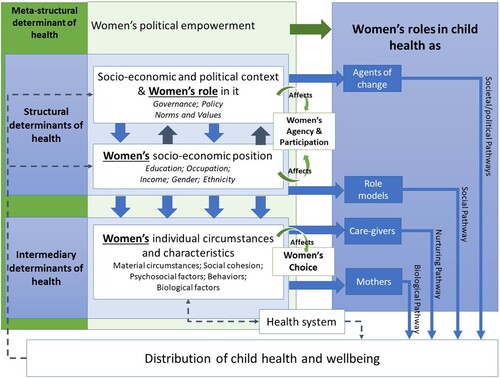
Building on these theories and the CSDH framework, we hypothesise that the political empowerment of women leads to empowerment in other dimensions (e.g. social, economic, psychological), thus allowing women to better fulfil roles critical to child health. As such, political empowerment would act as a meta-structural determinant of child health mediated through the status and roles of women. Our framework () illustrates how women’s political empowerment could lead to better child health. The left side reflects the determinants identified in the CSDH framework as applied to women. By acting on these different levels of determinants, the process of political empowerment would increase women’s choice (the ability to make decisions for themselves and their family), agency (the ability to define goals for themselves or their community) and participation (the ability to take part in political decision making and influence policy decision) (Sundström et al., Citation2017). Hence, this process would modify women’s status at the individual, community and structural levels, thus impacting their abilities to carry out key roles for ensuring children’s health: roles of mothers, care-givers, role models in their community and agents of change within society. Building on the three theories used by the CSDH framework, our framework highlights the biological, nurturing, social, societal/political pathways through which these key roles would affect child health. The biological pathway refers to how the health and well-being of the mother affect that of her child. The nurturing pathway reflects how a child’s environment and care as provided by care-givers, affect the child’s development and health. The social pathway covers the processes that shape the distribution of social factors (e.g. mother’s education and literacy, participation in the labour market, access to resources) through which women as role-models can set a path that promotes child health. Finally, the societal/political pathways reflect how women can lead to change in the priorities and political choices that shape not only health services and programme but also societal values and decisions (Wadsworth & Butterworth, Citation2005; World Health Organization, Citation2018). While these elements depend on more than women alone, the literature previously described illustrates how women’s unique roles in these different arenas could lead to improving child health, should women’s status be improved through political empowerment.
Figure 2. Women’s political empowerment as meta-structural determinant of child health: a conceptual framework.
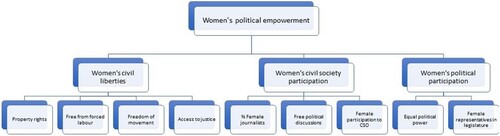
To test this hypothesis, we use the Women’s Political Empowerment Index (WPEI) developed by the Varieties of Democracy (V-Dem) project (Sundström et al., Citation2017) in combination with selected child health indicators from the Institute for Health Metrics and Evaluation’s (IHME) 2017 Global Burden of Disease (GBD) (Global Burden of Disease Collaborative Network, Citation2018a, Citation2018b) for 161 countries, covering the period from 1990 until 2016. We follow the definition of political empowerment given by the WPEI as ‘a process of increasing capacity for women, leading to greater choice, agency, and participation in societal decision-making’ (Sundström et al., Citation2017, p. 232). This index covers various components of women’s empowerment affecting structural determinants of health (): rights and liberties, participation in society and political participation and representation.
Figure 3. The components of the WPEI.
Material and method
Choice of variables and data sources
Child health outcomes
The dependent variables used to measure child health in this study – child mortality, stunting and immunisation (Global Burden of Disease Collaborative Network, Citation2018a, Citation2018b) (see Supplemental online material − Annex 1, Table S1) – cover various aspects of this concept and have been informed by current indicators included in the SDGs (United Nations, Citation2017). All the dependent variables were logged to reduce skewness. Covering a critical yet vulnerable period for child health and survival, the under-5 mortality rate is a widely used indicator of the state of child health in a country or globally. It is one of the indicators for SDG target 3.2 on ending preventable child deaths by 2030 (United Nations, Citation2017). Stunting is an indicator of poor nutrition, repeated infections and psychosocial risk factors (e.g. poverty or neglect), as well as a predictor of child development and future health (Onyango, Citation2014). It has been a major factor of the under-5 mortality reduction since 2000 and is one of the indicators for SDG target 2.2 on ending malnutrition by 2030 (United Nations, Citation2017; Watkins, Citation2016). The immunisation indicator used in this study – immunisation against diphtheria, pertussis and tetanus (DPT3) – not only reflects health service utilisation but also children’s protection from common infectious diseases, which has been a major factor in the decrease of under-5 mortality since 2000 (Watkins, Citation2016). Vaccine coverage is an indicator for SDG target 3.8 on universal health coverage (United Nations, Citation2017).
The choice for the IHME database was motivated by the quality and availability of data for all country-years covered in this study. As IHME generates and updates its health estimates on a yearly basis, the GBD 2017 provides cohesive panel data with annual estimates for each of the 195 countries and territories it includes, from 1990 to 2017 (Kyu et al., Citation2018; Lozano et al., Citation2018). As a result, it offers a more complete, balanced dataset than other international institutions like the World Bank, which rely on individual country’s reporting. However, the estimates used in this study remain highly consistent with those provided by international organisations such as the World Bank’s World Development Indicators (WDI) (Citation2018), with correlations coefficients over 0.95 for under-5 stunting and mortality rates and over 0.88 for DPT coverage between the IHME and WDI indicators.
Women’s political empowerment
The main independent variable, the WPEI, covers indices reflecting three key components of empowerment (see and Supplemental online material − Annex 1, Table S1): choice (reflected by the civil liberties index); agency (reflected by the civil society participation index) and participation (reflected by the political participation index) (Sundström et al., Citation2017). Unlike other indicators measuring women’s empowerment, the WPEI goes beyond political participation while focusing specifically on political empowerment as a process, both in terms of legal and effective rights. Its wide spatial and temporal coverage (Sundström et al., Citation2017) opens new opportunities for analysing the contribution of this process to sustainable development at the global level, as it offers a cohesive, complete and balanced dataset for a wide range of countries. Additionally, the V-Dem methodology allows us to capture the actual situation in a country rather than a government’s official position, while controlling for risks of individual or country biases from the expert respondents (Coppedge et al., Citation2018; Sundström et al., Citation2017). The WPEI has not yet been used to test the association of women’s political empowerment with child health outcomes within the context of global sustainable development.
Controlling for structural determinants of health
The effects of WPEI on child health was compared against a set of control variables related to specific SDGs and components of our framework (see Supplemental online material − Annex 1, Table S1). Our model was built in two steps, reflecting the two building blocks of structural determinants of health present in our framework. In our first step, we controlled for variables reflecting the socio-economic and political context. In our second step, we controlled for variables reflecting women’s socio-economic position, which are also markers of women’s socio-economic empowerment. Given our global focus and the causal relationship between structural and intermediary determinants of health in our framework (Solar & Irwin, Citation2010), we chose not to add individual-level variables representing intermediary determinants of health to our model.
Step 1: socio-economic and political context
Our first step included indicators covering structural, socio-economic and political contextual factors that may affect child health: countries’ economic growth, level of democratisation, population density and stability (Coppedge et al., Citation2018; Gleditsch et al., Citation2002; The World Bank, Citation2018b). To reduce skewness, two of these variables, economic growth and population density, were logged, since the broad level of these indicators for individual country-year mattered more than their actual individual value. Economic growth, a target of SDG 8 (United Nations, Citation2017), is associated with several health outcomes, including improved life expectancy and reduced infant mortality. This positive effect is particularly strong in poorer countries (CSDH, Citation2008; Wilkinson, Citation2005). Electoral democracy is thought to be beneficial to health by allowing citizens’ participation in decisions, which affects the allocation of resources and makes politicians more likely to invest in public goods and policies favourable to their population (Pieters et al., Citation2016; Sen, Citation1999; Welander et al., Citation2015). It is also thought to promote economic growth, thus indirectly benefiting health (Pieters et al., Citation2016). Democracy has been associated with child health outcomes such as improved nutrition and lower infant mortality (Welander et al., Citation2015). However, some studies have shown mixed results and great variation depending on the health outcome and regime considered (Pieters et al., Citation2016; Ross, Citation2006). Democratisation is not directly addressed by the SDGs, but several of its components are relevant to SDG 16 on inclusive institutions (United Nations, Citation2017). Population density has been associated with several health outcomes, although the relation between them is complex. At community level, high population density − and urban residence specifically − is associated with increased rates of violent deaths and injuries, selected chronic diseases, poor mental health and, when coupled with overcrowding and inadequate infrastructure, increased risks of infectious diseases. At country level, population density also seems to affect the population-level effect of selective preventative measures (Balk et al., Citation2004; Florey et al., Citation2007). On the other hand, living in urban areas is associated with increased access to information, infrastructure and health services. However, these benefits may be compromised when the population density exceeds service and infrastructure capacities (e.g. in slums) (Balk et al., Citation2004). Population density is not explicitly mentioned in the SDG targets but is directly related to a number of those included in SDG 11 on sustainable communities, including the targets on housing and equitable access to services (United Nations, Citation2017). Finally, countries’ stability indicators account for violence and wars’ long-lasting effect on young children’s physical and mental health (Calam, Citation2017; Wexler et al., Citation2006). These indicators are directly related to SDG 16 on peace, justice and strong institutions (United Nations, Citation2017). Children are disproportionally affected not only by the violence but also the long-term impact of conflicts such as malnutrition, epidemics, the destruction of health services, the increased vulnerability to abuse and the presence of unexploded devices like landmines (Pearn, Citation2003; Rieder & Choonara, Citation2012; Wexler et al., Citation2006). Controlling for these four elements allows us to assess the effect of women’s political empowerment on child health against key structural, socio-economic and political determinants over time.
Step two – women’s socio-economic position and empowerment
In the second step, we added non-political factors of women’s empowerment that have shown strong correlation with improved child health in the literature. They account for women’s socio-economic position determinants from our framework: maternal education and women’s labour participation (Global Burden of Disease Collaborative Network, Citation2018a; United Nations Development Programme, Citation2018). These indicators are also covered by SDG 4 on education and SDG 8 on decent work and economic growth (United Nations, Citation2017). As some countries rely on periodical national surveys to estimate female labour participation, the missing years for these countries have been linearly interpolated.
Comparing regression p values from both steps confirmed the relevance of the women’s socio-economic empowerment variables for the final model (see Supplemental online material – Annex 2, Tables S2a-c). As women’s political empowerment, women’s education and labour participation may be linked, we ran correlation tests between these three variables. The low correlations coefficients (all under 0.40) confirmed that these three elements of women’s empowerment remain, to a large extent, independent from one another (see the pairwise correlation matrix in Supplemental online material − Annex 3, Table S3).
Finally, to ensure that our model was sound, we tested for multicollinearity by calculating the variance inflation factors (VIF), which showed low to moderate multicollinearity (mean VIF of 2.48, VIF between 1.04 and 3.9),
Analysis
The analysis was performed using Stata 15.1. As the different datasets used do not necessarily cover the same number of countries and territories, we excluded countries and territories that are not currently members of the United Nations. To test for heteroskedasticity and address the complex correlation patterns associated with the use of cross-section, time series dataset, we performed a Wooldridge test for first order serial correlation and a Breusch–Pagan/Cook–Weisberg test for heteroskedasticity (Breusch & Pagan, Citation1979; Cook & Weisberg, Citation1983). As these tests failed to reject the null hypothesis, we used the Driscoll and Kraay method for estimating the standard errors to account for temporal and spatial correlations in our ordinary least squares regression analysis (Hoechle, Citation2007). Our initial regressions compared both the Newey-West and the Driscoll and Kraay methods (Supplemental online material – Annex 2, Tables S2a-c). We found that both methods returned very similar coefficients, although the results generated by the Driscoll and Kraay method tended to have slightly lower p values. Previous simulations reported that while the Driscoll and Kraay standard errors may be slightly optimistic with certain datasets, this method is more accurate when spatial dependence occurred (Hoechle, Citation2007). Hence, and following Sundström et al.’s (Citation2017) empirical analysis demonstrating the utility of the WPEI, only the regressions using the Driscoll and Kraay standard errors are reported in this article.
We first ran both random and country fixed-effects regressions. However, in line with the Hausman Test results, only the fixed-effects regressions were used for the subsequent regressions (initial random effect regressions are available from the author). As women’s empowerment is a long-term process and the impact of political changes may not be immediately reflected in health outcomes, we tested the hypothesis of a delayed effect of women’s political empowerment on child health outcomes. Thus, we tested the sensitivity of our findings to 2-year, 5-year and 10-year lags. Finally, we assessed whether our results were affected by outliers using Cook’s distance (Cook, Citation1977).
Calculating the substantive effects of women’s political empowerment on child health outcomes
When a correlation was found statistically significant and robust, we calculated its substantive effect to estimate the actual impact of the unlogged variable of interest. Substantive effect is obtained by multiplying the coefficient of the independent variable of interest by a standard deviation of the within variation of this variable, before dividing the product by a standard deviation of the within variation of the dependent variable studied in the model. This is then expressed as a percentage.
Assessing the women’s political empowerment – child health links by countries’ income and development levels
We wanted to further assess the effect difference of how various human and economic development thresholds at the global level shape the effect of women’s political empowerment on child health outcome. Hence, we added variables reflecting countries’ income and development categorisation. First, we ran our model with an interaction between the WPEI and a variable reflecting the World Bank’s historical classification of countries in three groups: high-, middle- and low-income (HIC, MIC and LIC respectively, see Supplemental online material – Annex 1, Table S1 for definitions). We used the historical classification at the beginning of our study period, 1990, or when countries first entered the World Bank’s classification (for countries founded after 1990) (The World Bank, Citation2018a). Then, we ran our initial model interacting the WPEI with a variable reflecting whether countries were ever defined by the United Nations as Least Developed Countries (LDC, see Supplemental online material – Annex 1, Table S1 for definitions) (United Nations Department of Economic and Social Affairs, Citation2010).
Robustness tests
To confirm the initial findings of our model, we added two control variables as part of a robustness test: governance and access to healthcare (Coppedge et al., Citation2018) (see Supplemental online material – Annex 1, Table S1). These indicators were chosen from the literature (Kuruvilla et al., Citation2014) to take into account how further structural and intermediary determinants of child health from our framework − the political context and health system governance − may affect the model or interfere with the effect of women’s political empowerment. We tested again for multicollinearity and outliers using the VIF and Cook’s distance tests, to assess how the additional variables affected the model in these regards.
Finally, in order to further explore potential causal relations between women’s political empowerment and child health outcomes, we ran Granger causality tests between the WPEI and each of the child health outcome variables (Granger, Citation1969). Besides providing further indications of a potential causal link between these phenomena, the Granger test also allows us to explore the risk of reverse-causality, where an improvement of child health could lead to women’s political empowerment. Indeed, reducing the burden and time women dedicate to child-bearing and child-rearing can reduce some of the constraints placed on them and open opportunities for active participation (Collins et al., Citation1993; Duflo, Citation2012). Hence, the Granger causality test allowed us to explore whether improved child health is driving women’s political empowerment.
Understanding the effects of WPEI components
The final stage of our analysis aimed to explore the mechanisms of actions of women’s political empowerment. To do so, we replaced the WPEI with each of its components: women’s civil liberties, civil society participation and political participation (see Supplemental online material – Annex 1, Table S1 for the definitions). This final step allowed us to test whether one dimension of women’s political empowerment (namely, choice, agency and participation) may be more influential than another on child health outcomes as compared to the process as a whole (as reflected by the WPEI).
A summary table of descriptive statistics covering the unlogged variables included in our models is included in Supplemental online material – Annex 4 (Table S4).
Results
Women’s political empowerment and child health outcomes at the global level
As shows, women’s political empowerment is associated with an improvement of two of the child health indicators: stunting and immunisation. The WPEI is negatively corelated with stunting prevalence and positively corelated with DPT3 coverage, both correlations being highly statistically significant. In this model, the association between WPEI and child mortality is not statistically significant.
Table 1. WPEI and child health outcomes, fixed effect regressions.
With regards to the structural factors reflecting the socio-economic and political context, our model confirms the positive association between child health and GDP per capita and the negative effect of civil war. It also confirms the complex links between child health and population density, which are associated with worsening mortality and stunting rates but improved immunisation coverage. Finally, the effect of democratisation is less clear.
As for women’s socio-economic empowerment markers, our model confirms the role of female education in child health. An increase in the mean level of maternal education is associated with a decrease in child mortality and stunting but also a decrease in immunisation coverage. In contrast, our model does not support an association between child health and women’s labour participation, as the associations are either not statistically significant (e.g. with child mortality or stunting) or the coefficient extremely small (with DPT3 coverage).
Substantive effect of women’s political empowerment on child health outcomes
The substantive effect of these variables shows a different picture. Increasing women’s political empowerment by one standard deviation would reduce stunting prevalence by 25.1% of a standard deviation but only increase DPT3 immunisation coverage by less than 1% of a standard deviation. As a comparison, the substantive effects of maternal education attainment and GDP per capita on stunting prevalence reduction are, respectively, over eight and three times superior to that of women’s political empowerment. However, their substantive effects on DPT3 immunisation are also very small.
Lagged effects of women’s political empowerment on child health outcomes
As women’s empowerment is a long-term process and the impact of political changes may not be immediately reflected in health outcomes, we tested the hypothesis of a lagged effect of women’s political empowerment on child health outcomes in the following 2, 5, and 10 years (see ). Most of the correlations remain unchanged compared to the previous regressions, confirming that the associations and effects previously described are unimpacted by the introduction of such time lags. However, a noticeable exception is child mortality; its negative correlation with women’s political empowerment becomes statistically significant when a 10-year lag is introduced. Substantively, an increase of women’s political empowerment by a standard deviation is associated with 2.6 fewer deaths per 1000 livebirths within 10 years. However, the substantive effect of women’s political empowerment on child mortality would still remain fairly small: over 15 times smaller than the one resulting from an increase of maternal education attainment and 13 times smaller than the one resulting from an increase in GDP per capita.
Table 2. WPEI and child health outcomes, fixed effect lagged regression.
As these results support a delayed effect of women’s political empowerment on at least one of the dependent variables, we continued to apply a 10-year lag alongside our main model in the subsequent regressions.
Women’s political empowerment and child health outcomes by countries’ income and development level
We tested how various human and economic development thresholds may shape the association between women’s political empowerment and child health outcomes.
Looking at these correlations by income groups (), we observe that high- and low-income countries benefit most from the effect of women’s political empowerment on child mortality. However, it is in middle-income countries where the effect of women’s political empowerment on reduced stunting is stronger, while its effect on DPT3 coverage is comparatively more important to low-income countries.
Table 3. WPEI and child health outcomes, fixed effect regressions by World Bank’s income groups.
When considering the case of LDCs (), we observe that women’s political empowerment in these countries has a comparatively strong effect on child mortality and immunisation coverage but not necessarily on stunting.
Table 4. WPEI and child health outcomes, fixed effect regressions for LDC and non-LDC countries.
Robustness tests
To confirm these findings, we added two control variables as part of a robustness test, to take into account how governance and access to healthcare may affect the model (, see also Supplemental online material – Annex 5, Tables S5a-b for robustness tests’ results by countries’ income and development levels). Adding these elements to the model reduces the correlation coefficients for most of the independent variables and thus, their substantive effect. However, this robustness test confirms the findings previously observed regarding women’s political empowerment being associated with reduced malnutrition and improved immunisation coverage. It also confirms that women’s social empowerment factors such as education have a larger substantive effect on these outcomes than political empowerment.
Table 5. WPEI and child health outcomes: robustness test with additional variables, fixed effect regressions.
We do note that under this model, the association between women’s political empowerment on child mortality is not statistically significant, even when accounting for a potential lagged effect of the empowerment process. This would suggest that other hidden factors may have been at play in the lagged association previously observed.
The Cook’s distance test allows to better understand the association between women’s political empowerment and child mortality, as it reveals that this association may be affected by outliers. Removing these outliers, we see that women’s political empowerment is associated with a statistically significant reduction of child mortality, with a slightly larger substantive effect (see ). Removing outliers do not affect the results of our model regarding stunting and immunisation coverage (results available from the author). The VIF for each independent variable in this latest model showed low to moderate multicollinearity (mean VIF of 2.81, VIF between 1.06 and 4.5), confirming the robustness of our initial findings.
Table 6. WPEI and child mortality, fixed effect lagged regression after removing outliers (Cook’s distance <4/N).
Granger-causality
While the Granger tests’ coefficients between the WPEI and stunting or child mortality are statistically significant, the F values are too low to conclude that these phenomena Granger-cause each other. Hence, this test does not allow us to support a causal relation between women’s political empowerment and any of the child health outcomes covered in our study. However, these tests do not indicate reverse causality between child health and women’s political empowerment either.
Understanding the effects of WPEI components
In line with the literature which suggests that child health may be affected differently by various components of empowerment, we tested whether one dimension of the WPEI (choice, agency and participation) was more relevant than another to improve child health outcomes. We used the same augmented list of control variables as in the robustness tests. Due to high correlation between the three indices, each regression was run separately. presents a summary of the correlation for each of the WPEI components, while the full tables are available in Supplemental online material – Annex 6 (Tables S6a-b).
Table 7. WPEI components and child health outcomes summary table: robustness test with additional variables, fixed effect regressions.
These models show that improving women’s choice and participation is associated with reduced mortality and improved immunisation coverage, especially in the long term (within 10 years). However, their substantive effect remains small and similar to those observed for the WPEI as a whole.
Under this model, improving women’s civil society participation – or agency – is not associated with improved child health outcomes.
Discussion
Contribution of this work to the field
Previous studies tended to focus on exploring the effect of women’s empowerment on child health at the individual level, with a particular emphasis on socio-economic empowerment. Our analysis complements these findings by studying women’s political empowerment as a structural determinant of child health, both conceptually and empirically. Therefore, our results respond to a critical gap in the literature, addressing the role of women’s political empowerment beyond simple representation. The Success Factors studies had already identified ‘good governance and women’s political and socioeconomic participation’ as ‘key enablers’ of the progress achieved in maternal and child health in low- and middle-income countries (Kuruvilla et al., Citation2014, p. 536). Building on these findings, we conclude that despite the variations observed, women’s political empowerment as a whole is relevant to improving child health across the globe, independently from markers of women’s socio-economic position.
Our results find a robust, positive association between progress in women’s political empowerment and two child health outcomes covered by the SDG targets: nutrition and DPT3 coverage. The association between women’s political empowerment and a reduction of child mortality is more complex. The correlation weakens once further factors such as governance and access to healthcare are added to the model, even when accounting for a possible lagged effect of empowerment. Yet, some of our tests suggest that such a robust link does exist once outliers have been removed from the model. Given the number of factors impacting child survival, our findings may reflect the role of other country-specific factors affecting the relation between women’s political empowerment and child mortality.
While the Granger tests does not allow us to further support the potential causal link between women’s political empowerment and child health outcomes described in our framework, it also does not indicate reverse causality. However, the use of fixed effect models controlling for several structural determinants of health in our study limits some of the risk of endogeneity. Hence, this study supports the opportunity for further research to explore potential causality between the women’s political empowerment process and improving child health.
As regards to structural determinants of health, our study confirms the findings from both the empirical literature on women’s empowerment at the individual level and the theoretical literature on political determinants of health. Indeed, our models have highlighted the positive association between child health and several structural determinants of child health from our framework – such as maternal education or GDP per capita, while confirming the complex relations between these health outcomes and population density. One marker of instability – the occurrence of civil war – is also strongly associated with worsening child health.
Looking at regional or national variations, we found that women’s political empowerment may have had more impact in LDCs or low-income countries when it came to improving immunisation coverage and child survival. Additionally, our results also suggest that even in high-income countries, which tend to have better child health outcomes and higher WPEI scores, women’s political empowerment remains relevant for improving child survival. As for middle-income countries, women’s political empowerment seems to be particularly relevant for the improvement of child nutritional status. These results complement the findings from previous empirical studies on women’s socio-economic empowerment, which pointed out that its effect on child health differed according to contexts and the outcome of interest. As a result, future research should further consider the regional or country-specific factors that may or may not make women’s political empowerment a suitable strategy for improving child health in their specific context.
Finally, our analysis found that components of women’s political empowerment may not all be relevant to improving child health. Our final test shows that rights and processes improving women’s choice or freedoms (e.g. intermediary determinants of child health in our framework) and women’s political participation into societal decision-making may have more impact than those improving women’s agency. Along with our findings regarding the role of women’s socio-economic empowerment, these findings call for further exploring if and how empowering women in different fields or investing in women’s different abilities and freedoms may offer a viable strategy for improving child health.
Women’s political empowerment and structural determinants of health: analysis of the substantive effects
A unique contribution of our work to this field is the comparison of actual effect sizes of different determinants of child health. We find that while the correlations between women’s political empowerment and selected child health outcomes are robust, the substantive effect of women’s political empowerment on child health outcomes is actually fairly small in comparison to other structural determinants of child health.
For stunting prevalence, the substantive effect is much smaller than those offered by other structural determinants, including markers of women’s socio-economic empowerment. This suggests that while women’s political empowerment may contribute to improving child health, women’s socio-economic position or the political and economic context determinants in our framework may offer stronger avenues to better health for young children. Future research should further explore the potential of these factors to improve child health, as well as their potential interactions.
As for improving immunisation coverage, while women’s political empowerment, education and other structural factors are strongly correlated with this outcome, all of them return a very small substantive effect. This suggests that other factors may offer better leverage to improve the coverage of these essential child health services. Looking back at our theoretical framework, the mediation of health systems in particular should be further researched when looking at the pathway through which structural determinants of health may affect child health services outcomes.
Strength and limitations
Our approach attempts to isolate the effect of women’s political empowerment on child health by controlling for other structural determinants of child health identified in the literature and by adopting fixed-effect models while also testing for a possible lagged effect of the process of interest. Our approach does not allow us to conclusively prove or disprove causal relations between women’s political empowerment and child health. However, the strong theoretical base supporting our hypothesis, the robust correlations observed and the steps taken to control for potential interfering phenomena warrant for causal relations between women’s political empowerment and child health to be explored further in future work. Additionally, to further inform policy and identify the most impactful level of intervention, future research should consider exploring the causal pathways through which these meta-structural processes may be mediated by, or directly impact, the individual level’s markers of empowerments that previous research has linked to child health outcomes.
Our analysis was constrained by data availability over time and globally. As a result, some of the transgenerational effects of women’s empowerment on child health or the dynamics in territories not internationally recognised as nations, could not be captured. Although our regressions were designed to control for both time and spatial dependence as well as country fixed effects, the global lens adopted in this analysis may also fail to fully capture the role of context in the child health outcomes covered. These elements may affect the relevance of our findings for individual countries and should therefore be considered alongside the literature previously highlighted, which explored the effect of women’s choice and agency at the individual level. Nevertheless, our results highlight general trends on the role of women’s political empowerment on child health, which could be of interest at the regional level, especially in the global South.
Our results do not dispute the value of women’s political empowerment in its own right, nor do they challenge its potential effect on other important elements of sustainable development − both of which being beyond the scope of this study. They rather point out the complexity of the relation and the need for careful evaluation of the role of different empowerment processes and structural factors when trying to improve child health. By adopting an inclusive definition of women’s political empowerment and focusing on the political condition of women as a whole, our study contributes to a better understanding of the societal impact of different dimensions of women’s status on specific child health outcomes. Therefore, unlike previous literature that focused exclusively on mothers, our findings provide a more inclusive overview of the complex interactions between women’s status and role in society and child health outcomes within the broader context of the SDGs.
Conclusion
While showing encouraging results, our study demonstrates the complexity of the relations between women’s political empowerment and child health. Our findings highlight the positive link between women’s political empowerment and selected child health outcomes such as nutrition and immunisation. However, they also show that their effect is rather small, especially in comparison to other structural determinants of child health. Secondly, our findings point out the differentiated effects of women’s political empowerment according to the WPEI components, the countries’ income and development level, and the individual child health outcomes considered.
Further research is needed to disentangle potential causal pathways in the associations found in our models. However, these findings suggest that women’s political empowerment can be an interesting process to explore at the global and regional levels to improve child health. Yet, they also suggest that women’s socio-economic empowerment or structural political or economic changes, may offer stronger leverage as structural determinants of child. With regards to the SDGs, these findings would further support integrating women’s empowerment into the goals on education, economic growth or strong institutions to achieve the SDGs’ child health and nutrition targets.
Supplemental Material
Download MS Word (131.4 KB)Acknowledgements
The author would like to thank Prof. Indra de Soysa for his guidance, help and comments in the development of this research and manuscript. I also would like to thank Prof. Nancy Lea Eik-Nes for reviewing and proofreading this manuscript. Finally, I would like to thank Prof. Terje Andreas Eikemo for his comments and feedback on early versions of this article.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Balk, D., Pullum, T., Storeygard, A., Greenwell, F., & Neuman, M. (2004). A spatial analysis of childhood mortality in West Africa. Population, Space and Place, 10(3), 175–216. https://doi.org/10.1002/psp.328
- Black, M. M., Walker, S. P., Fernald, L. C. H., Andersen, C. T., DiGirolamo, A. M., Lu, C., McCoy, D. C., Fink, G., Shawar, Y. R., Shiffman, J., Devercelli, A. E., Wodon, Q. T., Vargas-Barón, E., & Grantham-McGregor, S. (2017). Early childhood development coming of age: Science through the life course. The Lancet, 389(10064), 77–90. https://doi.org/10.1016/S0140-6736(16)31389-7
- Breusch, T. S., & Pagan, A. R. (1979). A simple test for heteroscedasticity and random coefficient variation. Econometrica, 47(5), 1287–1294. https://doi.org/10.2307/1911963
- Britto, P. R. (2017). Early moments matter for every child. UNICEF. https://www.unicef.org/publications/index_100862.html
- Brunner, E., & Marmot, M. (2005). Social organization, stress and health. In M. Marmot & R. Wilkinson (Eds.), Social determinants of health (2nd ed.). Oxford University Press. https://global.oup.com/academic/product/social-determinants-of-health-9780198565895?q=Social%20Determinants%20of%20Health%20wilkinson%20marmot%202nd%20ed&lang=en&cc=no
- Bueno de Mesquita, B. (2011). The dictator’s handbook: Why bad behavior is almost always good politics. Public Affairs.
- Calam, R. (2017). Public health implications and risks for children and families resettled after exposure to armed conflict and displacement. Scandinavian Journal of Public Health, 45(3), 209–211. https://doi.org/10.1177/1403494816675776
- Carlson, G. J., Kordas, K., & Murray-Kolb, L. E. (2015). Associations between women’s autonomy and child nutritional status: A review of the literature. Maternal & Child Nutrition, 11(4), 452–482. https://doi.org/10.1111/mcn.12113
- Center on the Developing Child. (2010). The foundations of lifelong health are built in early childhood. www.developingchild.harvard.edu
- Collins, R., Chafetz, J. S., Blumberg, R. L., Coltrane, S., & Turner, J. H. (1993). Toward an integrated theory of gender stratification. Sociological Perspectives, 36(3), 185–216. https://doi.org/10.2307/1389242
- Commission on Social Determinants of Health. (2008). Closing the gap in a generation: Health equity through action on the social determinants of health. WHO. https://www.who.int/social_determinants/thecommission/finalreport/en/
- Cook, R. D. (1977). Detection of influential observation in linear regression. Technometrics, 19(1), 15–18. https://doi.org/10.1080/00401706.1977.10489493
- Cook, R. D., & Weisberg, S. (1983). Diagnostics for heteroscedasticity in regression. Biometrika, 70(1), 1–10. https://doi.org/10.2307/2335938
- Coppedge, M., Gerring, J., Knutsen, C. H., Lindberg, S. I., Skaaning, S.-E., Teorell, J., Altman, D., Bernhard, M., Fish, M. S., Cornell, A., Dahlum, S., Gjerløw, H., Glynn, A., Hicken, A., Krusell, J., Lührmann, A., Marquardt, K. L., McMann, K., Mechkova, V., … Ziblatt, D. (2018). V-Dem Dataset - Version 8. [Datatset] Varieties of Democracy (V-Dem). https://doi.org/10.23696/vdemcy18
- Cunningham, K., Ruel, M., Ferguson, E., & Uauy, R. (2015). Women’s empowerment and child nutritional status in South Asia: A synthesis of the literature. Maternal & Child Nutrition, 11(1), 1–19. https://doi.org/10.1111/mcn.12125
- Duflo, E. (2012). Women empowerment and economic development. Journal of Economic Literature, 50(4), 1051–1079. https://doi.org/10.1257/jel.50.4.1051
- Florey, L. S., Galea, S., & Wilson, M. L. (2007). Macrosocial determinants of population health in the context of globalization. In Macrosocial determinants of population health (pp. 15–51). Scopus. https://doi.org/10.1007/978-0-387-70812-6_2
- Gleditsch, N. P., Wallensteen, P., Eriksson, M., Sollenberg, M., & Strand, H. (2002). Armed conflict 1946–2001: A new dataset. Journal of Peace Research, 39(5), 615–637. https://doi.org/10.1177/0022343302039005007
- Global Burden of Disease Collaborative Network. (2018a). Global Burden of Disease Study 2017 (GBD 2017) Covariates 1980–2017 [Dataset]. Institute for Health Metrics and Evaluation (IHME). http://ghdx.healthdata.org/record/ihme-data/gbd-2017-health-related-sdgs-1990-2030
- Global Burden of Disease Collaborative Network. (2018b). Global Burden of Disease Study 2017 (GBD 2017) Health-related Sustainable Development Goals (SDG) Indicators 1990–2030 [Dataset]. Institute for Health Metrics and Evaluation (IHME). http://ghdx.healthdata.org/record/ihme-data/gbd-2017-health-related-sdgs-1990-2030
- Granger, C. W. J. (1969). Investigating causal relations by econometric models and cross-spectral methods. Econometrica, 37(3), 424–438. https://doi.org/10.2307/1912791
- Hoechle, D. (2007). Robust standard errors for panel regressions with cross–sectional dependence. The Stata Journal, 7(3), 281–312. https://doi.org/10.1177/1536867X0700700301
- Hosseinpoor, A. R., Bergen, N., Schlotheuber, A., & Grove, J. (2018). Measuring health inequalities in the context of sustainable development goals. Bulletin of the World Health Organization, 96(9), 654–659. https://doi.org/10.2471/BLT.18.210401
- Krieger, N. (2011). Epidemiology and the people’s health: Theory and context. Oxford University Press.
- Kuruvilla, S., Schweitzer, J., Bishai, D., Chowdhury, S., Caramani, D., Frost, L., Cortez, R., Daelmans, B., de Francisco, A., Adam, T., Cohen, R., Alfonso, Y. N., Franz-Vasdeki, J., Saadat, S., Pratt, B. A., Eugster, B., Bandali, S., Venkatachalam, P., Hinton, R., … Bustreo, F. (2014). Success factors for reducing maternal and child mortality. Bulletin of the World Health Organization, 92(7), 533–544. https://doi.org/10.2471/BLT.14.138131
- Kyu, H. H., Abate, D., Abate, K. H., Abay, S. M., Abbafati, C., Abbasi, N., Abbastabar, H., Abd-Allah, F., Abdela, J., Abdelalim, A., Abdollahpour, I., Abdulkader, R. S., Abebe, M., Abebe, Z., Abil, O. Z., Aboyans, V., Abrham, A. R., Abu-Raddad, L. J., Abu-Rmeileh, N. M. E., … Murray, C. J. L. (2018). Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 392(10159), 1859–1922. https://doi.org/10.1016/S0140-6736(18)32335-3
- Lozano, R., Fullman, N., Abate, D., Abay, S. M., Abbafati, C., Abbasi, N., Abbastabar, H., Abd-Allah, F., Abdela, J., Abdelalim, A., Abdel-Rahman, O., Abdi, A., Abdollahpour, I., Abdulkader, R. S., Abebe, N. D., Abebe, Z., Abejie, A. N., Abera, S. F., Abil, O. Z., … Murray, C. J. L. (2018). Measuring progress from 1990 to 2017 and projecting attainment to 2030 of the health-related sustainable development goals for 195 countries and territories: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 392(10159), 2091–2138. https://doi.org/10.1016/S0140-6736(18)32281-5
- Marmot, M., Allen, J., Goldblatt, P., Boyce, T., McNeish, D., Grady, M., & Geddes, I. (2010). Fair society, healthy lives: The Marmot Review. UCL Institute of Health Equity. http://www.instituteofhealthequity.org/resources-reports/fair-society-healthy-lives-the-marmot-review/
- Mason, A. D., & King, E. M. (2001). Engendering development through gender equality in rights, resources, and voice (English) (A World Bank Policy Research Report.). World Bank. http://documents.worldbank.org/curated/en/512911468327401785/Engendering-development-through-gender-equality-in-rights-resources-and-voice
- Onyango, A. W. (2014). Global nutrition targets 2025 stunting policy brief (WHO/NMH/NHD/14.3). WHO. http://apps.who.int/iris/bitstream/handle/10665/149019/WHO_NMH_NHD_14.3_eng.pdf?ua=1
- Pearn, J. (2003). Children and war. Journal of Paediatrics and Child Health, 39(3), 166–172. https://doi.org/10.1046/j.1440-1754.2003.00124.x
- Pieters, H., Curzi, D., Olper, A., & Swinnen, J. (2016). Effect of democratic reforms on child mortality: A synthetic control analysis. The Lancet Global Health, 4(9), e627–e632. https://doi.org/10.1016/S2214-109X(16)30104-8
- Pratley, P. (2016). Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: A systematic review of evidence from the developing world. Social Science & Medicine, 169, 119–131. https://doi.org/10.1016/j.socscimed.2016.08.001
- Richards, E., Theobald, S., George, A., Kim, J. C., Rudert, C., Jehan, K., & Tolhurst, R. (2013). Going beyond the surface: Gendered intra-household bargaining as a social determinant of child health and nutrition in low and middle income countries. Social Science & Medicine, 95, 24–33. https://doi.org/10.1016/j.socscimed.2012.06.015
- Rieder, M., & Choonara, I. (2012). Armed conflict and child health. Archives of Disease in Childhood, 97(1), 59–62. https://doi.org/10.1136/adc.2009.178186
- Ross, M. (2006). Is democracy good for the poor? American Journal of Political Science, 50(4), 860–874. https://doi.org/10.1111/j.1540-5907.2006.00220.x
- Sen, A. (1999). Development as freedom. Oxford University Press.
- Sen, G., & Östlin, P. (2008). Gender inequity in health: Why it exists and how we can change it. Global Public Health, 3(sup1), 1–12. https://doi.org/10.1080/17441690801900795
- Solar, O., & Irwin, A. (2010). A conceptual framework for action on the social determinants of health (Social Determinants of Health Discussion Paper 2; Policy and Practice No. 2). WHO. https://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdf
- Sundström, A., Paxton, P., Wang, Y.-T., & Lindberg, S. I. (2017). Women’s political empowerment: A new global index, 1900–2012. World Development, 94, 321–335. https://doi.org/10.1016/j.worlddev.2017.01.016
- Taukobong, H. F. G., Kincaid, M. M., Levy, J. K., Bloom, S. S., Platt, J. L., Henry, S. K., & Darmstadt, G. L. (2016). Does addressing gender inequalities and empowering women and girls improve health and development programme outcomes? Health Policy and Planning, 31(10), 1492–1514. https://doi.org/10.1093/heapol/czw074
- Thorpe, S., VanderEnde, K., Peters, C., Bardin, L., & Yount, K. M. (2016). The influence of women’s empowerment on child immunization coverage in low, lower-middle, and upper-middle income countries: A systematic review of the literature. Maternal and Child Health Journal, 20(1), 172–186. https://doi.org/10.1007/s10995-015-1817-8
- UNICEF. (2015). Achieving Women’s economic empowerment and early childhood care and development as mutually reinforcing objectives toward an integrated vision of early childcare programming. A Technical note. https://www.unicef.org/earlychildhood/files/Technical_NoteAchieving_Womens_Economic_and_ECD.pdf
- United Nations. (2017). Transforming our world: The 2030 agenda for sustainable development. https://sustainabledevelopment.un.org/post2015/transformingourworld/publication
- United Nations Department of Economic and Social Affairs. (2010, September 23). Least Developed Countries (LDCs). Economic Analysis & Policy Division | Dept of Economic & Social Affairs | United Nations. Retrieved October 10, 2019, from https://www.un.org/development/desa/dpad/least-developed-country-category.html
- United Nations Development Programme. (2018). Human Development Data (1990-2017), Human Development Reports. http://hdr.undp.org/en/data
- Wadsworth, M., & Butterworth, S. (2005). Early life. In M. Marmot & R. Wilkinson (Eds.), Social determinants of health (2nd ed.). Oxford University Press. https://global.oup.com/academic/product/social-determinants-of-health-9780198565895?q=Social%20Determinants%20of%20Health%20wilkinson%20marmot%202nd%20ed&lang=en&cc=no
- Wallerstein, N. (2006). What is the evidence on effectiveness of empowerment to improve health? (Health Evidence Network Report). WHO EURO. http://www.euro.who.int/__data/assets/pdf_file/0010/74656/E88086.pdf?ua=1
- Wang, H., Abajobir, A. A., Abate, K. H., Abbafati, C., Abbas, K. M., Abd-Allah, F., Abera, S. F., Abraha, H. N., Abu-Raddad, L. J., Abu-Rmeileh, N. M. E., Adedeji, I. A., Adedoyin, R. A., Adetifa, I. M. O., Adetokunboh, O., Afshin, A., Aggarwal, R., Agrawal, A., Agrawal, S., Kiadaliri, A. A., … Murray, C. J. L. (2017). Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: A systematic analysis for the Global Burden of Disease Study 2016. The Lancet, 390(10100), 1084–1150. https://doi.org/10.1016/S0140-6736(17)31833-0
- Watkins, K. (2016). A fair chance for every child (No. 978-92-806-4838–6). UNICEF. https://www.unicef.org/publications/index_91711.html
- Welander, A., Lyttkens, C. H., & Nilsson, T. (2015). Globalization, democracy, and child health in developing countries. Social Science & Medicine, 136–137, 52–63. https://doi.org/10.1016/j.socscimed.2015.05.006
- Wexler, I. D., Branski, D., & Kerem, E. (2006). War and children. JAMA, 296(5), 579–581. https://doi.org/10.1001/jama.296.5.579
- WHO. (1998). Health promotion glossary. http://www.who.int/healthpromotion/about/HPR%20Glossary%201998.pdf
- Wigley, S., & Akkoyunlu-Wigley, A. (2017). The impact of democracy and media freedom on under-5 mortality, 1961–2011. Social Science & Medicine, 190, 237–246. https://doi.org/10.1016/j.socscimed.2017.08.023
- Wilkinson, R. (2005). Ourselves and others – for better or worse: Social vulnerability and inequality. In M. Marmot & R. Wilkinson (Eds.), Social determinants of health (2nd ed.). Oxford University Press. https://global.oup.com/academic/product/social-determinants-of-health-9780198565895?q=Social%20Determinants%20of%20Health%20wilkinson%20marmot%202nd%20ed&lang=en&cc=no
- The World Bank. (2018a). World Bank country and lending groups. Retrieved March 1, 2019, from https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups
- The World Bank. (2018b). World Development Indicators [Dataset]. World Bank. https://databank.worldbank.org/data/reports.aspx?source=World-Development-Indicators
- World Health Organization. (2018). Nurturing care for early childhood development: A framework for helping children survive and thrive to transform health and human potential. https://www.who.int/maternal_child_adolescent/child/nurturing-care-framework/en/