
ABSTRACT
Orphans are at higher risk of HIV infection and several important HIV risk factors than non-orphans; however, this may be due to a combination of related social, psychological, and economic factors, as well as care environment, rather than orphan status alone. Understanding these complex relationships may aid policy makers in supporting evidence-based, cost-effective programming for this vulnerable population. This longitudinal study uses a causal effect model to examine, through decomposition, the relationship between care environment and HIV risk factors in orphaned and separated adolescents and youths (OSAY) in Uasin Gishu County, Kenya; considering resilience, social, peer, or family support, volunteering, or having one's material needs met as potential mediators. We analysed survey responses from 1105 OSAY age 10–26 living in Charitable Children's Institutions (CCI) (orphanages) and family-based care settings (FBS). Follow-up time was 7–36 months. Care in CCIs (vs. FBS) was associated with a decreased likelihood of engaging in forced, exchange, and consensual sex. Excess relative risks (ERR) attributable to the indirect pathway, mediation, or interaction were not significant in any model. Care environment was not statistically associated with differences in substance use. Our findings support the direct, unmediated, association between institutional care and HIV risk factors.
ABBREVIATIONS
| 95%CI | = | – 95% Confidence interval |
| AMPATH | = | – Academic Model Providing Access to Healthcare |
| CASSS | = | – Child and Adolescent Social Support Scale |
| CCI | = | – Charitable Children's Institutions |
| CDE | = | – Controlled Direct Effect |
| CTQ | = | – Childhood Trauma Questionnaire |
| ERR | = | – Excess Relative Risk |
| FBS | = | – Family-based setting |
| ICAST-CH | = | – ISPCAN Child Abuse Screening Tool for Children a Home |
| ISPCAN | = | – International Society for the Prevention of Child Abuse and Neglect |
| INTmed | = | – Mediated Interaction Effect |
| INTref | = | – Reference Interaction Effect |
| MSPSS | = | – Multidimensional Scale of Perceived Social Support |
| OSAY | = | – Orphaned and separated adolescents and youths |
| OSCAR | = | – Orphaned and Separated Children's Assessments Related to Their Health and Well-Being Study |
| PIE | = | – Pure Indirect Effect |
| RS14 | = | – Resilience Scale |
| SD | = | – Standard deviation |
| SDQ | = | – Strengths and Difficulties Questionnaire |
| TE | = | – Total Effect |
| UNICEF | = | – United Nations Children's Fund |
Introduction
Millions of orphaned and separated adolescents and youths (OSAY) in sub-Saharan Africa are at a disproportionately higher risk of many adverse health outcomes, including HIV and associated risk factors, as compared to their non-orphaned peers (Operario et al., Citation2011; World Health Organization, Citation2013). This increased vulnerability may be due more to a combination of environmental, social, and psychological factors than orphan status alone (Juma et al., Citation2013a, Citation2013b; Kataoka et al., Citation2012; Mistry et al., Citation2009; Puffer et al., Citation2012a). Care environment has been linked to differences in physical and mental health as well as risk behaviours in this population; however, the mechanisms underlying these relationships are not well understood (Embleton et al., Citation2014, Citation2017; Sutherland et al., Citation2022).
In 2019, sub-Saharan Africa was home to approximately 53 million children who had lost one or both parents, nearly 20% due to HIV/AIDS. In Kenya alone, there are approximately 2,080,000 orphans, 32% due to HIV/AIDS (UNICEF, Citation2021). In 2017, nearly 49% of new HIV cases in Kenya occurred in individuals ≤24 years of age (National AIDS Control Council, Citation2018). Sexual transmission, through consensual sexual activity and sexual exploitation, as well as substance use are leading causes of HIV transmission in this population (National AIDS Control Council, Citation2018; Operario et al., Citation2011; World Health Organization, Citation2013). Substance use is linked to increased HIV risk both directly, through injection drug use, and indirectly, through participation in high-risk sexual practices including unprotected sex and increased vulnerability to sexual exploitation (Embleton et al., Citation2017; World Health Organization, Citation2013).
Orphans are at higher risk of HIV infection than non-orphans (World Health Organization, Citation2013). Orphan status has also been linked to risk factors for HIV including sexual exploitation, sexual abuse, substance use, early sexual debut, and having multiple sexual partners (Operario et al., Citation2011; World Health Organization, Citation2013). However, several studies have found that orphan status alone was not related to increases in sexual risk behaviours (Juma et al., Citation2013b; Puffer et al., Citation2012a). Instead, a combination of social, psychological, economic, and contextual factors may play a larger role in increased vulnerability and sexual risk-taking behaviours in this group (Juma et al., Citation2013a, Citation2013b; Kataoka et al., Citation2012; Mistry et al., Citation2009; Puffer et al., Citation2012a). These include protective factors such as positive relationships with peers and caregivers as well as involvement in one's community that may decrease an individual's likelihood of early sexual debut and sexual risk-taking as a means of facilitating social connection, psychological characteristics including resilience that may minimise an individual's vulnerability to participation in high-risk behaviours and sexual coercion, and economic factors that prevent OSAY from feeling pressured to engage in exchange sex as a survival strategy in order to meet their basic needs (Mmari, Citation2011; Perrino et al., Citation2000; Phillips et al., Citation2019; Puffer et al., Citation2012b; World Health Organization, Citation2013).
Care environment may also play an important role in risk behaviour. While the majority of orphaned and separated children and adolescents in sub-Saharan Africa are cared for by extended family (family-based settings, FBS), HIV/AIDS, poverty, and urbanisation have left many families unable to care for OSAY and led to the emergence of alternative models of care (Embleton et al., Citation2014). Despite strong cultural preferences for family-based care in the community, with institutional care often viewed as a damaging and inadequate response to child protection needs, a 2017 study estimated that 286,000 children age 0–17 in eastern and southern Africa live in residential care (Berens & Nelson, Citation2015; Embleton et al., Citation2014; Petrowski et al., Citation2017). In Kenya, common alternative models of care include Charitable Children's Institutions (CCI) (orphanages and rescue centres caring for ≥20 OSAY) and community-based supports by non-governmental organisations (Embleton et al., Citation2014). Some studies have concluded that institutional care is detrimental to child development (Berens & Nelson, Citation2015). Combined with strong cultural preferences for FBS care environments and historic examples of abuse and neglect this has led to global calls for the deinstitutionalisation of OSAY (Berens & Nelson, Citation2015; Gulaid, Citation2004; Save the Children UK, Citation2003; UNICEF, Citation2004). However, in countries with weak infrastructure, there is often greater heterogeneity in well-being within care environments than between them (Atwoli et al., Citation2014; Braitstein et al., Citation2013; Embleton et al., Citation2017; Gayapersad et al., Citation2019; Williamson et al., Citation2017).
Previous studies have found that Kenyan OSAY living in CCIs (vs. FBS) had lower prevalence of risk factors for HIV including having ever exchanged sex or experienced forced sex (Embleton et al., Citation2017). These benefits may partially stem from increased levels of protective social, psychological, and economic factors (Embleton et al., Citation2014; Sutherland et al., Citation2022). A 2014 study found that in this population CCIs met the basic material needs of OSAY 95% of the time, compared to 17% in FBS (Embleton et al., Citation2014). Previous analyses found that OSAY in CCIs had higher average levels of resilience, social support, peer support, and volunteering as compared to those in FBS (Sutherland et al., Citation2022). However, the cross-sectional nature of these studies was a primary limitation; as associations were demonstrated but causality was unable to be determined. There is a need for longitudinal investigation of the relationships and mechanisms of action between care environment, HIV risk factors, and associated social, psychological, and physical factors.
VanderWeele (Citation2014) developed a method of ‘decomposing’ the relationship between an exposure and an outcome into four components reflecting the effects of the exposure in the absence of the mediator, the interactive effect of the mediator at its natural level in the absence of the exposure, the mediated interaction, and the pure mediated effect. Combinations of components provide insight into how much of an effect is due to mediation, interaction, both, or neither (VanderWeele, Citation2014). This method overcomes limitations of traditional analyses that assess either mediation or interaction but not both simultaneously.
Insight into the drivers of HIV risk in vulnerable populations is of particular importance in lower and middle income countries where the burden of HIV is high and resources may be limited (National AIDS Control Council, Citation2018). The aim of the present study was to characterise the direct and indirect effects of care environment on HIV risk factors in the Kenyan OSAY population using VanderWeele's decomposition method and to assess the potential mediating effects of resilience, peer, social, and family support, volunteering, and having one's basic material needs met. We hypothesised that care in CCIs would be associated with reduced incidence of HIV risk factors and that this relationship would be mediated by resilience, as previous work has also shown that resilience is on average higher among OSAY in institutions compared to FBS (Sutherland et al., Citation2022). Understanding these complex relationships is important as it may help policy makers to support evidence-based, cost-effective programming that minimises the burden of HIV in this group and encourages the health, well-being, and social and economic potential of OSAY in any care environment.
Materials and methods
Study setting
This study occurred in Uasin Gishu County, Kenya. Its capital, Eldoret, is home to Moi University, Moi Teaching and Referral Hospital, and the Academic Model Providing Access to Healthcare (AMPATH) programme, a collaboration between Moi Teaching and Referral Hospital, Moi University, and a consortium of universities from North America (Einterz et al., Citation2007). In 2019, the population of Eldoret was 476,000 while Uasin Gishu County was home to approximately 1,153,000 individuals from 305,000 households; 37% aged ≤14 years (Kenya National Bureau of Statistics, Citation2019, Citation2020a, Citation2020b). In 2016, approximately 37% of individuals in Uasin Gishu County aged <18 years were living in multidimensional poverty as defined by UNICEF's Multiple Overlapping Deprivation Analysis (Kenya National Bureau of Statistics, Citation2020c).
Procedures and participants
This study uses data from Phase II of the Orphaned and Separated Children's Assessments Related to Their Health and Well-Being (OSCAR) longitudinal cohort study. The study began in 2010, with near universal inclusion of CCIs and a random representative sample of FBS households. It used annual surveys and medical assessments to investigate the effects of care environment on the physical and mental health of OSAY, ≤18 years old at baseline, in Uasin Gishu County, Kenya. Phase I found that contrary to expectations, OSAY in institutional environments largely fared better than their counterparts in FBS when measuring nutrition, mental, and sexual health outcomes (Atwoli et al., Citation2014; Braitstein et al., Citation2013; Embleton et al., Citation2017). Phase II, begun in 2016, sought to explain the results of Phase I, with a focus on individual and interpersonal factors that may promote well-being within and between care environments (Embleton et al., Citation2017). The OSCAR study has been described in detail previously (Embleton et al., Citation2014; Kamanda et al., Citation2013).
This analysis uses longitudinal data from 1105 of 1134 participants with two or more Phase II captures at least 6 months apart. The first data capture of Phase II, time 1, established baseline. Time 2, an individual's latest capture within the follow-up period, provided outcome measures. These ranged 7–36 months post-baseline. Exclusions were based upon age, as psychological assessments were not administered to OSAY aged <10 (n = 4), and incomplete data (n = 25). Individuals with limited missing data, including ‘refuse to answer’, were only excluded from analyses using the affected variables. Data cleaning occurred first in the field and discrepancies or missing information were verified with the participant on site (Kamanda et al., Citation2013).
Human subjects protections
Protocols for this and the parent OSCAR study were approved by the Institutional Research Ethics Committees of Moi University College of Health Sciences and Moi Teaching and Referral Hospital, the Research Ethics Board of the University of Toronto, and Indiana University's Institutional Review Board. All participants provided written assent or fingerprints in cases where they were unable to sign their names. Heads of FBS households and the Director of each CCI provided informed consent. A project psychologist reviewed psychological assessments for red flags, including suicidality, markers of active abuse, and posing likely harm to oneself or others, and cases were followed up by OSCAR study staff.
Instruments
The 14-item Resilience Scale (RS14) with a 7-point response measured resilience (Wagnild, Citation2009). The 12-item Multidimensional Scale of Perceived Social Support (MSPSS) using a 5-point response measured social support (Zimet et al., Citation1988). The 10-item Parent subscale of the Child and Adolescent Social Support Scale (CASSS) with a 4-point adaptation of the frequency response measured Family Support (Kerres Malecki & Kilpatrick Demary, Citation2002). The 5-item Peer Problems subscale of the Strengths and Difficulties Questionnaire (SDQ) with a 3-point response measured peer support (Escueta et al., Citation2014). The ISPCAN Child Abuse Screening Tool for Children at Home (ICAST-CH) measured a history of abuse in OSAY <18 years of age (Zolotor et al., Citation2009). The Childhood Trauma Questionnaire (CTQ) measured history of abuse for OSAY age ≥18 (Bernstein, Citation1998). Abuse was considered binary with any score of ‘moderate’ or ‘severe’ in any of the emotional, sexual, or physical abuse subscales considered positive for abuse. Additional instrument information can be found in Supplementary Table 1.
Variables
Data collection included standardised clinical and psychosocial encounters. Psychosocial instruments were self-administered with assistance from a psychologist available when necessary.
The exposure variable was care environment (CCI vs. FBS). Four potentially mediating variables were continuous – resilience, social support, family support, and peer relationships. Two were binary – involvement in volunteering and having one's basic material needs met, the latter defined as a child having at least one blanket, a pair of shoes, and two sets of non-school uniform clothing (UNICEF, Citation2006).
Outcome variables were incident HIV risk factors during the follow-up time, operationalised as binary (yes/no) with prevalent cases at baseline excluded from each analysis. These included alcohol or drug use (‘Have you ever used any of the following substances’; ‘yes’ if ever yes for any kind of drugs or alcohol), consensual sex (‘Have you ever willingly had sex with anyone’; ‘yes’ if ever experienced consensual sex), forced sex (‘Has anyone … tried or forced you to have sex when you did not want them to’; ‘yes’ if ever experienced forced sex), and exchange sex (‘Have you ever exchanged sex for money, shelter, food, protection, or anything else’ and ‘In the past 12 months have you had sex or been sexually involved with anyone because he/she gave you or told you he/she would give you gifts, cash, or anything else?’; ‘yes’ if yes to either question).
Model adjustment variables include age (continuous), sex (female/male), orphaned/separated status (maternal/paternal/double/non-orphan), HIV status (positive/negative), and history of abuse (yes/no). Sub-group analysis variables include sex and age (<18/≥18 years of age).
Statistical analysis
Descriptive analysis included frequencies, means, and standard deviations (SD). Data on participation in volunteering was only collected from OSAY <18 years of age.
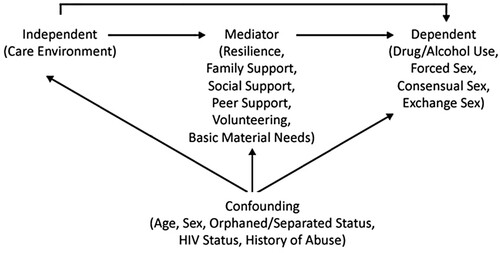
Our analyses were guided by a theoretical causal framework () that hypothesises that resilience, social, and physical factors mediate the effect of care environment on HIV risk factors. Potentially confounding factors were adjusted for in all analyses. These were collected at baseline and include age, sex, HIV status, orphan status, and history of abuse. Models accounted for the possibility of clustering by household or institute (i.e. similarities among individuals from the same household or institute due to common unmeasured factors) (239 clusters). All models were tested for age and gender effects. Stratified sub-group analyses were run by sex and age (<18 or ≥18) and differences were investigated. For each analysis, OSAY with the outcome at baseline were excluded as they were not at risk of developing the outcome.
Figure 1. Causal diagram of the mediation hypothesis.
Note: A causal diagram of the effect of care environment on HIV risk factors. All confounding variables are adjusted for in all models.
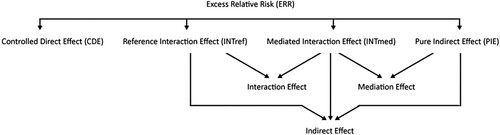
An adapted version of VanderWeele's method was used to decompose the effect of care environment on HIV risk factors into direct and indirect pathways, accounting for the raw excess relative risk (ERR) and portion of Total Effect (TE) due to mediation and interaction (). This method decomposes the TE into four parts: Controlled Direct Effect (CDE), Reference Interaction Effect (INTref), Mediated Interaction Effect (INTmed), and Pure Indirect Effect (PIE). TE is the sum of all four components. Every exposure-mediator pair has a unique set of effects (VanderWeele, Citation2014). The direct effect consists of the CDE, quantifying the causal effect of the exposure not attributable to the mediator currently under consideration. This ‘direct effect’ is potentially mediated by other variables outside the causal pathway of interest. The indirect effects are mediated by the current mediator, describe the effect due to interaction, mediation, or both, and consist of the INTref, INTmed, and PIE. PIE quantifies the causal effect of the mediator when the exposure is fixed. The TE due to mediation is the sum of PIE and INTmed. The TE due to interaction is the sum of INTmed and INTref (VanderWeele, Citation2014).
Figure 2. Mediation and interaction decomposition.
Note: The decomposition of the ERR into four components: CDE, INTref, INTmed, PIE as described in VanderWeele (Citation2014). In a mediation analysis, CDE forms the direct pathway. INTref and INTmed sum to create the interaction effect. INTmed and PIE sum to create the mediation effect. INTref, INTmed, and PIE sum to create the indirect pathway.
ERR between CCI and FBS (i.e. risk ratio – 1) was used as the effect measure and decomposed into contributions due to the direct effect, indirect effect, mediation, and interaction of each mediator-outcome pair. Conclusions were based on significance testing. To account for multiple comparisons, false discovery rate was controlled at 5% for each effect measure separately, across different mediator-outcome combinations. presents unadjusted results. All analyses used two-tailed tests and were conducted using SAS 9.1 (SAS Institute Inc., Citation2002).
Table 1. The effect of care environment on HIV risk factors including alcohol or drug use, forced sex, consensual sex, and exchange sex due to mediation and interaction with resilience, social, and physical factors in OSAY in Western Kenya.
Results
The sample consisted of 1105 OSAY; 553 females and 552 males. Ages at baseline ranged from 10 to 27 and 57% were <18 years of age. Most OSAY lived in FBS (73%) while 27% lived in CCIs (). OSAY in CCIs were on average younger, with 75% <18 years compared to 50% in FBS, and more likely to be male (55% vs. 48%).
Table 2. Sample characteristics of OSAY (ages 10–26) in Western Kenya.
At baseline, 89% participated in volunteering. Basic material needs were met in 62% of OSAY <18 years old and 71% age ≥18. Resilience scores ranged from 14 to 98 (mean = 65; SD = 20) (Wagnild, Citation2009). Social support scores ranged from 1 to 5 (mean = 4.2; SD = 0.8) (Zimet, Citation2016). Family support scores ranged from 10 to 40 (mean = 27; SD = 8). Peer support scores ranged from 6 to 15 (mean = 12; SD = 2) (Escueta et al., Citation2014). Participation in volunteering, having one's basic material needs met, and levels of resilience, social, family, and peer support did not vary by sex. OSAY ≥18 years of age had higher average levels of resilience (mean = 67 vs. 63) and family support (mean = 28 vs. 27) than those age <18. Peer and social support did not vary by age. Follow-up time ranged from 7 to 36 months (mean = 20; SD = 5) and did not vary by care environment. The percentage of individuals eligible for follow-up due to not being positive for the outcome at baseline ranged from 77% (consensual sex) to 96% (drug/alcohol) ().
Table 3. Outcome measures at time 1 and time 2 by care environment.
Compared to their older peers, OSAY <18 years of age had a higher prevalence of having experienced forced (20% vs. 8%) or exchange (20% vs. 10%) sex, and were less likely to have used drugs/alcohol (5% vs. 9%), or participated in consensual sex (16% vs. 54%) by time 2. Females were less likely than males to have used drugs/alcohol (4% vs. 9%). The prevalence of outcomes at baseline and incidence during follow-up time are presented in .
Decomposition of the total effects of care environment on HIV risk factors into ERR and components attributable to direct effects and indirect effects, including mediation and interaction, is presented in with detailed intermediate results available in Supplemental Table 2. Due to the exclusion of individuals with incomplete mediator data, the population eligible for each exposure-mediator pairing differed slightly, resulting in small differences in ERR within outcome measures. This section presents the range of significant ERRs for each outcome variable, with exposure-mediator specific breakdowns and 95% confidence intervals (95%CI) presented in .
After adjusting for potential confounding factors and intra-household clustering, care in CCIs (vs. FBS) was associated with lower incidence of all sexual health outcomes. During the follow-up period, OSAY in CCIs were 65–80% less likely to have experienced forced sex, 63–78% less likely to have engaged in exchange sex, and 64–77% less likely to have participated in consensual sex than those in FBS. ERR attributable to the direct pathway was significant in most models, while ERR due to the indirect pathway, mediation, or interaction was only significant in one unadjusted model and was not statistically significant once the false discovery rate was controlled at 5% (). Care environment was not statistically associated with differences in drug/alcohol use.
Sub-group analyses stratified by sex and age were generally underpowered due to rare events; however, the results were similar in direction and magnitude to the original analyses. Differences were investigated and no significant interaction with age or sex was identified.
Discussion
This study suggests that institutional care in this setting has a direct protective effect against sexual risk behaviours or experiences including consensual, exchange, and forced sex and that these relationships are not strongly mediated by any of resilience, family, peer, or social support, volunteering, or having one's material needs met. The single exception was consensual sex which was mediated exclusively by having one's material needs met in the unadjusted model; however, these relationships were not significant once false discovery rate was controlled for. Care environment was not associated with the likelihood of engaging in drug/alcohol use.
A previous cross-sectional study found that CCIs were associated with lower prevalence of sexual exploitation than FBS, including forced and exchange sex, but found no significant heterogeneity between care environments with consensual sex (Embleton et al., Citation2017). In our study, at time 1, forced, consensual, and exchange sex were already higher in FBS, resulting in lower proportions of OSAY at risk of developing the outcome of interest by time 2. Despite this, between time 1 and time 2, OSAY in CCIs were still less likely to experience any of the sexual health outcomes than their peers in FBS, demonstrating a direct relationship between these outcomes and care environment. The protective effects of care in CCIs maintained significance in all but two adjusted models.
Beyond simply demonstrating these relationships, our analysis investigated whether the effects of care environment on sexual health outcomes may have been mediated by previously identified protective factors. Feeling supported by, connected to, and involved with one's community may increase access to positive role models and encourage prosocial behaviours while decreasing the likelihood of engaging in risky sexual activities as a means of facilitating social connection (Mmari, Citation2011; Perrino et al., Citation2000). Likewise, strong perceived social and family support, including increased caregiver communication and monitoring, have been linked to decreased risk-taking behaviours in adolescents (Kabiru et al., Citation2010). OSAY in CCIs in Kenya have demonstrated higher average levels of peer and social support than those in FBS (Sutherland et al., Citation2022). For this reason, peer, family, and social support along with volunteering in one's community were considered as potential mediators in this study. Likewise, higher psychological resilience has been linked to lower sexual risk-taking behaviours in adolescents, mitigating the increase in risk associated with adverse childhood experiences even after adjusting for social and family support. It is theorised that higher levels of resilience may minimise the risk of sexual transmission of HIV infection through decreasing an individual's vulnerability to sexual coercion or exploitation (Phillips et al., Citation2019). OSAY in CCIs in Kenya have also demonstrated higher average resilience compared to those in FBS, leading to its inclusion (Sutherland et al., Citation2022). Lastly, poverty is a known driver of sexual risk behaviour in adolescents; both directly through increasing vulnerability to transactional sex as a survival strategy and indirectly through exposure to work environments that predispose OSAY to sexual risks and exploitation. For adolescents in Kenya, work outside of the home has been linked with increased sexual risk factors for HIV infection including multiple sexual partners, exchange sex, and coerced or forced sex, often with older partners with whom there is a power dynamic that reduces the adolescent's ability to negotiate safe sex (Juma et al., Citation2013a). Kenyan OSAY in CCIs are more likely to have their basic material needs met, potentially mitigating the motivation to engage in transactional sex, as compared to those in FBS (Embleton et al., Citation2014). For this reason, having basic material possessions was investigated as a potential mediator.
Despite their theoretical impact on the relationship between care environment and HIV risk factors, the amount of excess risk explained by the indirect pathway, mediation, or interaction alone were non-significant in nearly all models. In one exception, in the unadjusted model the direct protective effect of care in CCIs on engaging in consensual sex was mitigated by the increased likelihood of OSAY in CCIs of having their basic material needs met. While the PIE also decreased the ERR, in line with studies linking material deprivation to increased sexual risk behaviour, these protective effects were not additive and both components of the interaction (INTref & INTmed) reversed the direction of the effect in the resulting indirect pathway, mediation, and interaction summary measures (Jean-Robert, Citation2003; Jennings et al., Citation2017).
We did not find evidence of significant mediation with the investigated mediators which suggests that the mechanisms through which care environment affects HIV risk factors likely involve alternative mediators or confounding factors, such as quality of care, not measured in this study (or maybe lack of power). While having one's basic material needs met was only a significant mediator in one unadjusted analysis, alternate socioeconomic factors including lack of food security or participating in income generating activities such as domestic labour outside the home, which may be more common outside of institutional care, have also been linked to increased rates of exchange sex in Kenyan adolescents (Juma et al., Citation2013a). Access to external support and resources may also be important as poverty among OSAY has been linked to increased sexual risk-taking as a survival strategy (Juma et al., Citation2013a). In a 2014 study, 100% of CCIs in Eldoret reported some form of external financial or alternative support, primarily through individual donors, while 36% of FBS households caring for OSAY reported no external support of any kind (Embleton et al., Citation2014). While family support was not a strong mediator in this study, increased structure and caregiver supervision has been linked to lower rates of forced and exchange sex (Embleton et al., Citation2017). Fear of repercussions for engaging in sexual risk behaviours may also act as a deterrent in institutional settings (Embleton et al., Citation2017).
Unlike sexual risk outcomes, care environment was not related to drug/alcohol use. Similar proportions of OSAY in CCIs and FBS had engaged in drug/alcohol use at time 1 (5% vs. 4%); however, eligible OSAY in CCIs were more likely to begin using drugs/alcohol during the follow-up time (5% vs. 2%). This relationship became non-significant when adjusted for age, sex, orphan status, HIV status, and history of abuse. This differs from a 2017 study in the OSAY population that found substance use to be higher in CCIs vs. FBS; however, that was a descriptive, cross-sectional, unadjusted measure (Embleton et al., Citation2017).
The study's relatively large sample size provides sufficient power to detect true relationships while the sampling frame, with near universal inclusion of CCIs and a representative, random sample of FBS households, minimises the potential for selection bias, increasing confidence in the generalizability of findings. While most OSAY studies have focussed on either orphans vs. non-orphans or CCIs without an FBS comparison group, this study includes detailed information on care environment, day-to-day activities, and social, psychological, and physical factors. While previous analyses of this population have been primarily cross-sectional, this study is longitudinal; minimising the potential for reverse-causality. Though full temporality is not achieved as exposure and mediator variables are collected at baseline, all OSAY had been in the same care environment for over 5 years at data collection while mediators were a reflection of the individual's current state. There was no cross-over between exposure groups.
VanderWeele (Citation2014)’s four-way decomposition differs from the more commonly presented ‘natural’ direct and indirect effect models. However, VanderWeele's method offers the benefit of simultaneously distinguishing effects due to mediation and interaction in a single unified framework, which is lacking in traditional models (VanderWeele, Citation2014).
The four-way decomposition method assumes that there are no unmeasured confounders and that confounders to the mediator-outcome relationship are not affected by the exposure (VanderWeele, Citation2014). If this is incorrect, these confounders would lie on both the direct and indirect pathways. As the indirect effects of care environment on HIV risk factors via the potential mediators were rarely statistically significant, it is unlikely that any were highly influential confounders for other mediator-outcome pairs.
This study also has limitations. The incidence of outcomes of interest was relatively rare. A longer follow-up time may have increased outcome incidence rates and provided additional analytical power. Rare outcomes also limited sub-group analyses. Future longitudinal analyses with longer follow-up time will allow stronger exploration of age- and sex-related heterogeneity as well as additional risk factors such as multiple sexual partners or sexual debut.
Measurement error with theoretical constructs is unavoidable with tools measuring psychological factors. The associated risks were minimised using age-appropriate, English-language tools, validated in the OSCAR or similar samples with only minor modifications (Supplementary Table 1) (Hoosen et al., Citation2018; Sutherland et al., Citation2020). The same tools were used in both care environments to minimise the potential for measurement variance. Outcomes were measured with a single item and the term ‘sex’ was not explicitly defined. OSAY may have interpreted the meaning of ‘sex’ differently based on age and knowledge, reducing reliability.
Missing data may be non-random. Outcome measures were self-reported and may be subject to non-response or social desirability bias due to the sensitive nature of adolescent substance use and sexual behaviour. This may have led to underreporting, particularly for OSAY in institutionalised care due to fear of repercussions, potentially affecting internal and external validity. To minimise this potential source of bias, questionnaires were self-administered, with a clinical psychologist available to assist with question clarification. Privacy and confidentiality were assured. Completeness was confirmed on site with immediate follow-up on incomplete questions. Missing data was rare. All variables with >5% missingness were investigated; no factors predictive of missingness were found.
This study is among the first to assess the longitudinal impact of care environment on HIV risk factors in the Kenyan OSAY population. Consistent with the primary hypothesis, it demonstrates strong protective effects of care in CCIs on likelihood of experiencing consensual, forced, or exchange sex; however, with a single exception, resilience, peer, family, and social support, volunteering, and having one's material needs met were not strong mediators of this effect. For initiatives looking to minimise the incidence of HIV risk factors, this study indicates that research into the causal pathways related to care environment might be a good place to start. While these relationships were not explained by factors explored in this study, alternate causal mechanisms including mediators such as poverty, external support, engaging in income generating activities, and the role of caregivers should be explored in order to identify potential targets for initiatives to minimise risk behaviours in this vulnerable population. Understanding this complex issue is crucial to the creation and support of evidence-based, cost-effective programming to encourage the welfare, health, and potential of OSAY in any care environment.
Implications and contribution
The causal mechanisms of care environment on HIV risk factors in OSAY in Western Kenya have not been previously investigated. Through better understanding of this complex issue, policy makers may be able to support evidence-based, cost-effective programming that encourages the health, well-being, and social and economic potential of OSAY in any care environment. This study found a strong, unmediated effect between care environment and most outcomes. These data suggest that the causal mechanisms of these effects are likely due to unmeasured mediators or confounding factors.
Supplemental Material
Download MS Word (19.6 KB)Supplemental Material
Download MS Word (66.3 KB)Acknowledgements
We wish to gratefully acknowledge the Chiefs, Assistant Chiefs, and Village Elders of the Locations of Pioneer, Kapsoya, Koisagat, Ol’Lenguse, Olare, Tarakwa, Kipsinende and Kapyemit for their support and leadership. We also wish to acknowledge all the residents of these locations and in particular the many households caring for vulnerable members of their community, notably orphaned and separated children, children with physical and mental disabilities, and the elderly. We particularly want to acknowledge the County and District Children's Officers for their dedication to protecting the children of Uasin Gishu County, as well as the Uasin Gishu Children's Services Forum. This study would not have been possible without the willing participation of the children and youth participants and their guardians and we would like to acknowledge and thank them. The enthusiasm and commitment of the staff and volunteers of the OSCAR study have not gone unnoticed and we the authors wish to thank them for their efforts and engagement with this project.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Atwoli, L., Ayuku, D., Hogan, J., Koech, J., Vreeman, R., Ayaya, S., & Braitstein, P. (2014). Impact of domestic care environment on trauma and posttraumatic stress disorder among orphans in Western Kenya. PLoS ONE, 9(3), e89937. https://doi.org/10.1371/journal.pone.0089937
- Berens, A., & Nelson, C. (2015). The science of early adversity: Is there a role for large institutions in the care of vulnerable children? The Lancet, 386(9991), 388–398. https://doi.org/10.1016/S0140-6736(14)61131-4
- Bernstein, D. P. (1998). Childhood trauma questionnaire: A retrospective self-report: Manual. Psychological Corporation.
- Braitstein, P., Ayaya, S., Nyandiko, W., Kamanda, A., Koech, J., Gisore, P., Atwoli, L., Vreeman, R., Duefield, C., & Ayuku, D. (2013). Nutritional status of orphaned and separated children and adolescents living in community and institutional environments in Uasin Gishu County, Kenya. PLoS ONE, 8(7), e70054. https://doi.org/10.1371/journal.pone.0070054
- Einterz, R., Kimaiyo, S., Mengech, H., Khwa-Otsyula, B., Esamai, F., Quigley, F., & Mamlin, J. (2007). Responding to the HIV pandemic: The power of an academic medical partnership. Academic Medicine, 82(8), 812–818. https://doi.org/10.1097/ACM.0b013e3180cc29f1
- Embleton, L., Ayuku, D., Kamanda, A., Atwoli, L., Ayaya, S., Vreeman, R., Nyandiko, W., Gisore, P., Koech, J., & Braitstein, P. (2014). Models of care for orphaned and separated children and upholding children’s rights: Cross-sectional evidence from Western Kenya. BMC International Health and Human Rights, 14(9), 1–18. https://doi.org/10.1186/1472-698X-14-9
- Embleton, L., Nyandat, J., Ayuku, D., Sang, E., Kamanda, A., Ayaya, S., Nyandiko, W., Gisore, P., Vreeman, R., Atwoli, L., Galarraga, O., Ott, M. A., & Braitstein, P. (2017). Sexual behavior among orphaned adolescents in Western Kenya: A comparison of institutional- and family-based care settings. Journal of Adolescent Health, 60(4), 417–424. https://doi.org/10.1016/j.jadohealth.2016.11.015
- Escueta, M., Whetten, K., Ostermann, J., O’Donnell, K., & The Positive Outcomes for Orphans (POFO) Research Team. (2014). Adverse childhood experiences, psychosocial well-being and cognitive development among orphans and abandoned children in five low income countries. BMC International Health and Human Rights, 14(6), 1–13. https://doi.org/10.1186/1472-698X-14-6
- Gayapersad, A., Ombok, C., Kamanda, A., Tarus, C., Ayuku, D., & Braitstein, P. (2019). The production and reproduction of kinship in charitable children’s institutions in Uasin Gishu County, Kenya. Child & Youth Care Forum, 48(6), 797–828. https://doi.org/10.1007/s10566-019-09506-8
- Gulaid, L. (2004). The framework for the protection, care and support of orphans and vulnerable children living in a world with HIV and AIDS. UNICEF.
- Hoosen, N., Davids, E. L., de Vries, P. J., & Shung-King, M. (2018). The strengths and difficulties questionnaire (SDQ) in Africa: A scoping review of its application and validation. Child and Adolescent Psychiatry and Mental Health, 12(1), 6. https://doi.org/10.1186/s13034-017-0212-1
- Jean-Robert, R. (2003). Poverty and sexual risk behaviour among young people in Bamenda, Cameroon. African Population Studies, 18(2), 91–104.
- Jennings, L., Mathai, M., Linnemayr, S., Trujillo, A., Mak’anyengo, M., Montgomery, B. E. E., & Kerrigan, D. L. (2017). Economic context and HIV vulnerability in adolescents and young adults living in urban slums in Kenya: A qualitative analysis based on scarcity theory. AIDS and Behavior, 21(9), 2784–2798. https://doi.org/10.1007/s10461-017-1676-y
- Juma, M., Alaii, J., Bartholomew, L. K., Askew, I., & Van den Born, B. (2013a). Understanding orphan and non-orphan adolescents’ sexual risks in the context of poverty: A qualitative study in Nyanza Province, Kenya. BMC International Health and Human Rights, 13(1), 32. https://doi.org/10.1186/1472-698X-13-32
- Juma, M., Alaii, J., Bartholomew, L. K., Askew, I., & Van den Borne, B. (2013b). Risky sexual behavior among orphan and non-orphan adolescents in Nyanza Province, Western Kenya. AIDS and Behavior, 17(3), 951–960. https://doi.org/10.1007/s10461-012-0336-5
- Kabiru, C. W., Beguy, D., Undie, C.-C., Zulu, E. M., & Ezeh, A. C. (2010). Transition into first sex among adolescents in slum and non-slum communities in Nairobi, Kenya. Journal of Youth Studies, 13(4), 453–471. https://doi.org/10.1080/13676261003801754
- Kamanda, A., Embleton, L., Ayuku, D., Atwoli, L., Gisore, P., Ayaya, S., Vreeman, R., & Braitstein, P. (2013). Harnessing the power of the grassroots to conduct public health research in Sub-Saharan Africa: A case study from Western Kenya in the adaptation of community-based participatory research (CBPR) approaches. BMC Public Health, 13(1), 91. https://doi.org/10.1186/1471-2458-13-91
- Kataoka, C., Nozu, Y., Kawahara, S., Kuroiwa, H., Kudo, M., Sato, Y., Kubo, M., & Watanabe, M. (2012). Relationships of youth risk behaviors with norm-consciousness and resilience among Japanese high school students. Open Journal of Preventive Medicine, 02(03), 306–311. https://doi.org/10.4236/ojpm.2012.23044
- Kenya National Bureau of Statistics. (2019). 2019 Kenya population and housing census volume I: Population by county and sub-county (p. 49). https://www.knbs.or.ke/?wpdmpro=2019-kenya-population-and-housing-census-volume-i-population-by-county-and-sub-county
- Kenya National Bureau of Statistics. (2020a). 2019 Kenya population and housing census volume II: Distribution of population by administrative units (p. 270). https://www.knbs.or.ke/?wpdmpro=2019-kenya-population-and-housing-census-volume-ii-distribution-of-population-by-administrative-units
- Kenya National Bureau of Statistics. (2020b). 2019 Kenya population and housing census volume III: Distribution of population by age, sex and administrative units (p. 526). https://www.knbs.or.ke/?wpdmpro=2019-kenya-population-and-housing-census-volume-iii-distribution-of-population-by-age-sex-and-administrative-units
- Kenya National Bureau of Statistics. (2020c). Comprehensive poverty report (p. 151). https://www.genderinkenya.org/publication/comprehensive-poverty-report/
- Kerres Malecki, C., & Kilpatrick Demary, M. (2002). Measuring perceived social support: Development of the child and adolescent social support scale (CASSS). Psychology in the Schools, 39(1), 1–18. https://doi.org/10.1002/pits.10004
- Mistry, R., McCarthy, W. J., Yancey, A. K., Lu, Y., & Patel, M. (2009). Resilience and patterns of health risk behaviors in California adolescents. Preventive Medicine, 48(3), 291–297. https://doi.org/10.1016/j.ypmed.2008.12.013
- Mmari, K. (2011). Exploring the relationship between caregiving and health: Perceptions among orphaned and non-orphaned adolescents in Tanzania. Journal of Adolescence, 34(2), 301–309. https://doi.org/10.1016/j.adolescence.2010.05.001
- National AIDS Control Council. (2018). Kenya AIDS response progress report 2018.
- Operario, D., Underhill, K., Chuong, C., & Cluver, L. (2011). HIV infection and sexual risk behaviour among youth who have experienced orphanhood: Systematic review and meta-analysis. Journal of the International AIDS Society, 14(1), 25. https://doi.org/10.1186/1758-2652-14-25
- Perrino, T., González-Soldevilla, A., Pantin, H., & Szapocznik, J. (2000). The role of families in adolescent HIV prevention: A review. Clinical Child and Family Psychology Review, 3(2), 81–96. https://doi.org/10.1023/A:1009571518900
- Petrowski, N., Cappa, C., & Gross, P. (2017). Estimating the number of children in formal alternative care: Challenges and results. Child Abuse & Neglect, 70, 388–398. https://doi.org/10.1016/j.chiabu.2016.11.026
- Phillips, S. P., King, N., Michaelson, V., & Pickett, W. (2019). Sex, drugs, risk and resilience: Analysis of data from the Canadian health behaviour in school-aged children (HBSC) study. European Journal of Public Health, 29(1), 38–43. https://doi.org/10.1093/eurpub/cky169
- Puffer, E. S., Drabkin, A. S., Stashko, A. L., Broverman, S. A., Ogwang-Odhiambo, R. A., & Sikkema, K. J. (2012a). Orphan status, HIV risk behavior, and mental health among adolescents in rural Kenya. Journal of Pediatric Psychology, 37(8), 868–878. https://doi.org/10.1093/jpepsy/jss077
- Puffer, E. S., Watt, M. H., Sikkema, K. J., Ogwang-Odhiambo, R. A., & Broverman, S. A. (2012b). The protective role of religious coping in adolescents’ responses to poverty and sexual decision-making in Rural Kenya. Journal of Research on Adolescence, 22(1), 1–7. https://doi.org/10.1111/j.1532-7795.2011.00760.x
- SAS Institute Inc. (2002). SAS 9.1.3 help and documentation. SAS Institute Inc.
- Save the Children UK. (2003). A last resort: The growing concern about children in residential care. International Save the Children Alliance.
- Spies, G., Kidd, M., & Seedat, S. (2019). A factor analytic study of the childhood trauma questionnaire-short form in an all-female South African sample with and without HIV infection. Child Abuse & Neglect, 92, 157–166. https://doi.org/10.1016/j.chiabu.2019.04.002
- Sutherland, S. C., Shannon, H. S., Ayuku, D., Streiner, D. L., Saarela, O., Atwoli, L., & Braitstein, P. (2020). Reliability and validity of the RS14 in orphaned and separated adolescents and youths in Western Kenya. PLoS ONE, 15(11), e0241699. https://doi.org/10.1371/journal.pone.0241699
- Sutherland, S. C., Shannon, H. S., Ayuku, D., Streiner, D. L., Saarela, O., Atwoli, L., & Braitstein, P. (2022). The relationships between resilience, care environment, and social-psychological factors in orphaned and separated adolescents in Western Kenya. Vulnerable Children and Youth Studies, 17(2), 165–179. https://doi.org/10.1080/17450128.2022.2067381
- UNICEF. (2004). Children in residential care: The Zimbabwean experience. https://bettercarenetwork.org/library/the-continuum-of-care/residential-care/children-in-residential-care-the-zimbabwean-experience
- UNICEF. (2006). Africa’s orphaned and vulnerable generations: Children affected by AIDS. UNICEF.
- UNICEF. (2021). Data warehouse. UNICEF Data Warehouse. https://data.unicef.org/resources/data_explorer/unicef_f/
- VanderWeele, T. J. (2014). A unification of mediation and interaction: A 4-way decomposition. Epidemiology, 25(5), 749–761. https://doi.org/10.1097/EDE.0000000000000121
- Wagnild, G. (2009). The resilience scale user’s guide for the US English version of the resilience scale and the 14-item resilience scale (RS-14). Resilience Center.
- Williamson, K., Landis, D., Shannon, H., Priya, G., & Gillespie, L.-A. (2017). The impact of protection interventions on unaccompanied and separated children in humanitarian crises. Oxfam; Feinstein International Center; UKAID.
- World Health Organization. (2013). HIV and adolescents: Guidance for HIV testing and counselling and care for adolescents living with HIV: Recommendations for a public health approach and considerations for policy-makers and managers. World Health Organization.
- Zimet, G. (2016). Multidimensional scale of perceived social support (MSPSS)—Scale items and scoring information. https://www.researchgate.net/publication/311534896_Multidimensional_Scale_of_Perceived_Social_Support_MSPSS_Scale_Items_and_Scoring_Information#:~:text=The%20Zimet%20Multidimensional%20Scale%20of,Very%20Strongly%20Agree.%20.
- Zimet, G., Dahlem, N., Zimet, S., & Farley, G. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2
- Zolotor, A. J., Runyan, D. K., Dunne, M. P., Jain, D., Péturs, H. R., Ramirez, C., Volkova, E., Deb, S., Lidchi, V., Muhammad, T., & Isaeva, O. (2009). ISPCAN child abuse screening tool children’s version (ICAST-C): Instrument development and multi-national pilot testing. Child Abuse & Neglect, 33(11), 833–841. https://doi.org/10.1016/j.chiabu.2009.09.004
