
ABSTRACT
Maternal depression remains under characterised in many low- and middle-income countries, especially in rural settings. We aimed to describe maternal depression and anxiety symptoms in rural and urban communities in northern Ecuador and to identify socioeconomic and demographic factors associated with these symptoms. Data from 508 mothers participating in a longitudinal cohort study were included. Depression and anxiety symptoms were assessed using the Hopkins Symptom Checklist (HSCL-25), and maternal psychological functioning was assessed using a checklist of daily activities. Tobit regression models were used to examine associations with sociodemographic variables and urbanicity. The median HSCL-25 score was 1.2 (IQR: 0.4) and 14% of women scored above the threshold for clinically relevant symptoms. Rural women reported similar food insecurity, less education, younger age of first pregnancy, and lower socio-economic status compared to their urban counterparts. After adjusting for these factors, rural women reported lower HSCL-25 scores compared to women lin urban areas (β = −0.48, 95%CI:0.65, −0.31). Rural residence was also associated with lower depression and anxiety HSCL-25 sub-scale scores, and similar levels of maternal functioning, compared to urban residence. Our results suggest that both household and community-level factors are risk factors for maternal depression and anxiety in this context.
Introduction
Depression among women of childbearing age is the single largest contributor to the substantial global burden of mental health disorders (Rieder et al., Citation2019). Poor maternal mental health has negative outcomes for both mothers and children (Muzik & Borovska, Citation2011). Specifically, it is well documented that poorer maternal mental health often leads to an increased risk of mortality, poorer growth, and behavioural and emotional issues for children (Leis et al., Citation2014; Boivin et al., Citation2018; Surkan, Citationn.d; Thompson et al., Citation2022).
For women living in low- and middle-income countries (LMICs), mood and anxiety disorders, including depression, may be more common than in high-income countries (HICs), with systematic reviews estimating a prevalence of depression at 31% during the antenatal period (Yin et al., Citation2021) and 26% during the postnatal period (Dadi et al., Citation2020). More recent research is directing attention to perinatal depression, which considers depressive symptomatology arising during pregnancy and up to a year after delivery. A 2018 systematic review and meta-regression estimated the global prevalence of perinatal depression at 11.9%, although with significant differences between HICs and LMICs (Shorey et al., Citation2018). Depression is more common among poorer women exposed to gender-based risks (e.g. intimate partner violence, role restrictions around infant care and household work), circumstances that tend to be more common in LMICs (Fisher et al., Citation2012).
Despite the fact that maternal depression is prevalent and has adverse impacts on mother and baby, it remains under-characterised in many LMIC contexts (Fisher et al., Citation2012). Much of the literature on maternal depression in LMICs derives from health-facility based, rather than community-based studies (Atif et al., Citation2015), which may over-represent on women of higher socioeconomic status (SES) (Fisher et al., Citation2012) and women in urban areas with relatively greater health system access. Relatively less is known about maternal depression in rural settings in LMICs. Evidence from HICs on the prevalence of rural versus urban depression is conflicting (Ginja et al., Citationn.d; Nidey et al., Citation2020; Weaver et al., Citation2015). Compared to their urban counterparts, some studies have found that rural women are at an increased risk of depression (Ginja et al., Citationn.d), (Nidey et al., Citation2020), as well as at increased risk of untreated mental health disorders, and the downstream complications resulting from these disorders (Muzik & Borovska, Citation2011). In other reports, women residing in rural settings were at decreased risk compared to their urban counterparts (Weaver et al., Citation2015). The underlying factors that may drive these differences has not been fully characterised, either in HICs or in LMICs. However, socioeconomic status, marital status, social support, and access to services are among other recognised risk factors for maternal depression that may vary between rural and urban settings (Beck, Citation2001; Eastwood et al., Citation2015; Vigod et al., Citation2013).
High rates of maternal depression have been reported in many parts of urban Latin America (Santos et al., Citation2011) and in some parts of Ecuador (Thompson et al., Citation2022). A recent analysis of national health surveillance data found that unplanned pregnancy, and living in an urban versus a rural area, were associated with an increased risk of a postpartum depressive episode (Parra-parra et al., Citation2022).
The province of Esmeraldas is in north-western Ecuador, along the border with Colombia. Our group has previously observed that rural and urban communities in this context tend to vary along several axes that might act as causes of maternal stress or help to protect against it. For instance, more remote riverine communities without road access tend to have the highest rates of food insecurity (Go et al., Citation2021), but also greater social connectedness (Trostle et al., Citation2008; Zelner et al., Citation2013).
The aim of this study was to identify sociodemographic factors associated with depression and anxiety symptoms among women in the perinatal period across an urban-rural gradient in northern Ecuador. In doing so, we aim to increase the knowledge around maternal mental health and its risk factors, to ultimately inform interventions to optimise maternal and child health for women living in LMIC settings.
Methods
Study design and location
The Enteropatógenos, Crecimiento, Microbioma, y Diarrea (EcoMiD) study (Lee et al., Citation2021) is a longitudinal birth cohort designed to investigate the effects of enteric infections on the development of the gut microbiome, as well as child health outcomes, including diarrhea and growth. We leveraged this cohort to implement a sub-study amongst mothers in the cohort to better understand maternal depression, mother–child interactions, and child neurodevelopment. The EcoMiD cohort began enrolment in May 2019, and the sub-study was implemented in February 2021.
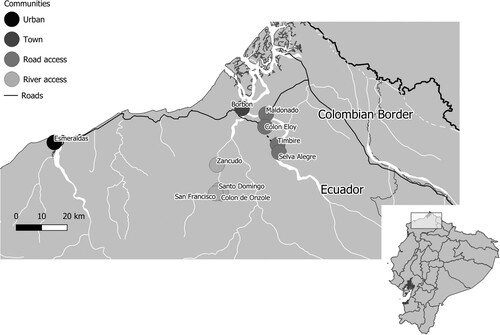
The study catchment area encompasses communities that can be broadly classified into four categories along an urban-rural gradient (): (a) The urban city of Esmeraldas, Ecuador, the 13th largest city in Ecuador, with a population of 161,868 (Instituto Nacional de Estadística y Censos, Citation2010); (b) Borbón, a large town of approximately 1,800 households and 5,000 individuals, located at the confluence of the Cayapas, Santiago, and Onzole rivers (Eisenberg et al., Citation2006); (c) 4 road-accessible rural communities near Borbón, including the towns of Timbire, Selva Alegre, Colon Eloy and Maldonado (populations ∼400–920); (d) 3 communities that were only accessible by river, including Santo Domingo, Zancudo, and Colon de Onzole, and one community, San Francisco, with limited road access (populations ∼200–700) (). Women are recruited and enrolled into the study through a combination of strategies, including recruitment of women attending prenatal services at the local health centre, snowball sampling (participating mothers nominating their acquaintances) and radio announcements that are broadcast throughout the study area. After potential participants are identified, field staff contact the pregnant woman to confirm eligibility and invite them to participate in the study via the informed consent process.
Figure 1. Map of the study area in Northern Ecuador with communities highlighted by urban-rural gradient.
Among the 521 women enrolled in EcoMiD cohort study, six women could not be contacted to participate in the sub-study because they moved from the study catchment area before the sub-study was implemented and two women did not participate because their child had passed away. Of the remaining 513, 5 women declined to participate in the sub-study. In total, therefore, 508 women participated in the sub-study. After providing written informed consent for both the EcoMiD cohort study and the sub-study, participants responded to questionnaires administered by trained Ecuadorian research assistants in Spanish in a private setting, usually the participant’s home. Sixteen data collectors were involved in data collection, and all but one of these were female. The Institutional Review Boards of Emory University and the Universidad San Francisco de Quito each approved the study protocols (Approval numbers CR002-IRB00101202; and MOD0014-IRB00101202 at Emory and 2018-022M and 2020-074M at the Universidad San Francisco de Quito).
Data collection
Women’s sociodemographic factors and depression and anxiety symptoms, and psychological functioning data were collected at 37 weeks pregnancy. The sub-study was begun in February 2021, mid-way through study enrolment, and then continued on a rolling basis through the end of study enrolment, in December 2022. As a result, 110 women had already given birth and were assessed in catch-up visits when their children were between 0 and 2 years old (i.e. postnatally), all in early 2021. The remaining 398 women were assessed at 37 weeks of pregnancy, between February 2021 and December 2022.
Demographic information including age, years of education, marital status, number of pregnancies, number of children and age of first pregnancy was collected using survey instruments. We also assessed socioeconomic status (SES) by constructing a wealth index from a checklist of 15 material possessions (shoes, radio, mattress, blanket, bicycle, motorcycle, cows, and goats) and whether participants owned their own house and/or agricultural land. Respondents reported the presence or absence of each of these assets in their households. Scores were created using a multiple correspondence (MCA) analysis. The final asset-based SES score had a mean of 0.0 and a standard deviation of 1.0. Food security was also measured using the Household Food Insecurity Access Scale (HFIAS) (Coates et al., Citation2006), a nine-item that queries about three aspects of food insecurity: anxiety and uncertainty, insufficient quality, and insufficient food intake. This data was used to assign each household to one of four categories (food secure, and mildly, moderately, and severely food insecure) following the standard scoring method (Coates et al., Citation2007), and then further reduced to two categories of food secure (food secure) or food insecure (mildly, moderately, and severely food secure).
All maternal depression, anxiety and psychological functioning assessments were conducted in Spanish, after translation and back-translation by members of the field study staff. Final translations were discussed among bilingual members of the study team. After the assessments had been implemented for two months, cognitive interviews were conducted with six members of the field team from all four community types to evaluate how the assessments were received and understood by study participants and further revise translations.
Depressive and anxiety symptoms were assessed using the Hopkins Symptom Checklist-25 (HSCL-25) (Hesbacher et al., Citation1980; Winokur et al., Citation1984), with each symptom being reported for the prior 4 weeks using a 4-point Likert scale ranging from 1 (not at all) to 4 (all the time). The HSCL-25 is a widely used scale in many LMIC contexts (Bolton et al., Citation2003; Kaida et al., Citation2014; Nabbe et al., Citation2018). Average scores were generated for depression (15 item) and anxiety (10 item) subscales; higher scores indicating greater severity. Following the literature (Kinyanda et al., Citation2011; Tsai et al., Citation2016) we used the cut-off score of 1.75 or higher to suggest clinical relevancy of symptoms (calculated as the average of the 25 items).
Maternal psychological functioning was assessed using a list of daily activities (Boivin et al., Citation2013). This questionnaire uses 16 items that relate to tasks women regularly do to take care for themselves, their family, their community, and their young child. Women indicate how much difficulty they have completing each task, using a Likert scale from 0 (no difficulty) to 4 (cannot complete). A functionality score was obtained by averaging item responses.
Spearman correlation coefficients were used to assess the correlation between the HSCL-25 depression, anxiety and overall scores and the psychological functioning score. Tobit regression models were used to assess bivariate associations between the demographics, wealth, and the depression and anxiety outcomes. Tobit models yield unbiased estimates when the dependent variable is truncated (Hsiao, Citation2003), as is the case here. Overall HSCL-25 scores, as well as depression and anxiety subscales, were truncated below 1 and above 4, while maternal functioning scores were truncated below 0 and above 4. Tobit models were also used to assess bivariate associations between socio-demographic factors and overall HSCL-25 scores. Multivariable models were then constructed to assess whether associations between urbanicity and depression and anxiety symptoms were modified by any sociodemographic factor. The multivariable model was based on inclusion of all theoretically justifiable variables, and then a final reduced multivariable model was constructed with non-significant descriptors and characteristics excluded. Urbanicity was treated as a categorical variable, with the most urban site of Esmeraldas used as reference. Because risk factors for antenatal versus postnatal depression may be interrelated but distinct (Leigh & Milgrom, Citation2008), we also considered the timing of the assessment (pre- versus postnatal).
All analyses were done using R software version 4.0.3 (CitationR Core Team, n.d).
Results
Reliability and validity. The internal consistency (Cronbach’s alpha) of the HSCL-25 was 0.86 and 0.87 for the depression and anxiety subscales, respectively. The internal consistency of the maternal functioning score was 0.92. The overall Spearman correlation between the HSCL-25 and the maternal functioning score was 0.31 (), demonstrating convergent validity.
Table 1. Spearman correlations between the Hopkins’ and maternal functioning scales.
Maternal characteristics. Demographic variables of study participants are described in . Women were on average 26 years old, mostly married, and in their second pregnancy. The median overall HSCL-25 was 1.2 (IQR: 0.44), the median depression subscale was 1.26 (IQR: 0.53). and the median anxiety score was 1.1 (IQR:0.40). The median maternal functioning score was 1.0 (IQR: 0.31). A total of 74 women (14.6%) had HSCL-25 above the 1.75 threshold for clinically relevant symptoms. Eight women (1.6%) endorsed suicidality items. These women received immediate psychiatric referral. There were few differences in women assessed prenatally versus postnatally, other than the timing of assessment (postnatal women were assessed earlier in the study period due to the pandemic pause in data collection), number of children prior to their current child, and ethnicity (Supplemental Table 1).
Table 2. Descriptive statistics by community, n = 508.
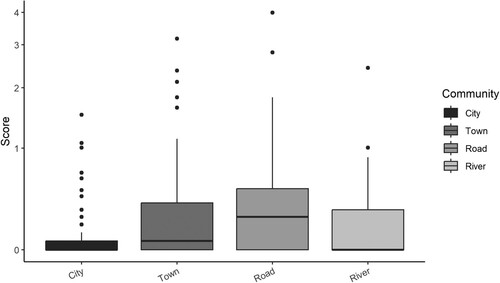
Associations between sociodemographic factors and depression and anxiety symptoms. Across the urban rural gradient there were significant differences in the HSCL-25 scores, depression subscale scores, and anxiety scores, with higher scores observed in urban and large town communities ( & Supplemental Table 2). Maternal psychological functioning scores were higher among rural communities (). There were no statistically significant differences (median overall HSCL scores 1.20 for those assessed during pregnancy versus 1.28 for those assessed when their children were older, Mann–Whitney p = 0.067).
Figure 2. Bar graph of HSCL scores by community.* Possible range 1–4.
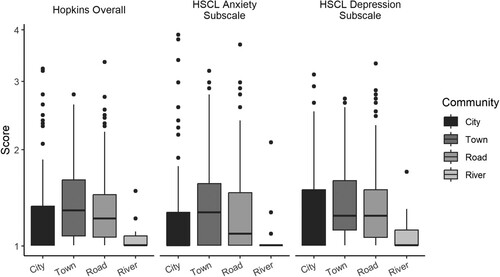
Figure 3. Bar graph of maternal functioning scores by community. * Possible range 0–4.
Bivariate linear regression models were constructed to assess the association of depression and anxiety HSCL subscales and maternal functioning with demographic variables and urbanicity. The results of the regression indicated that food insecurity was significantly associated with depression (β = 0.19, 95%CI: 0.09, 0.29), anxiety (β = 0.27, 95%CI: 0.01, 0.39), and maternal functioning (β = 0.17 95%CI: 0.02, 0.31) scores. A statistically significant relationship was also observed between community type and depression, anxiety, and maternal functioning scores. Riverine community residence was inversely associated with both depression (β = −0.54, 95%CI: −0.73, −0.35) and anxiety (β = −0.74 95%CI: −1.07, −0.42) (). In the bivariate analyses, only the timing of the survey relative to the COVID-19 pandemic (late-pandemic versus mid-pandemic) (β = −0.21 95%CI: −0.30. −0.12), single (versus partnered) marital status (β = 0.12, 95%CI: 0.01, 0.24), food insecurity (β = 0.16, 95%CI: 0.07, 0.25), and town residence (versus city) (β = 0.60 95%CI: 0.01, 0.24) were associated with higher overall HSCL-25 scores, while riverine residence (β = −0.48, 95%CI: −0.65, −0.30) was associated with lower overall HSCL-25 scores. In multivariate analysis, survey timing relative to the COVID-19 pandemic (β = −0.20, 95%CI: 0.29, −0.11) food insecurity (β = 0.13, 95%CI: 0.04, 0.22), town residence (β = 0.13, 95%CI: 0.01, 0.24) and river-accessible community residence (β = −0.48, 95%CI: −0.65, −0.31) retained statistical significance ().
Table 3. Bivariate tobit regression models of HSCL subscales, maternal functioning, and risk factors.
Table 4. Bivariate and multivariate linear regression of overall HSCL-25 scores and risk factors for maternal depression and anxiety.
Discussion
Fourteen percent of women in our sample could be classified as having were above the threshold for clinically relevant symptoms of depression, slightly below the 19% prevalence of postpartum depression estimated by a 2018 systematic review across Latin America (Shorey et al., Citation2018), although well above the estimated depression prevalence in Ecuador in 2017 (4.6%) (World Health Organization, Citation2017), and higher than the median lifetime prevalence rate of several epidemiological studies from the Latin American region (9.7%) (Kohn & Rodríguez, Citation2009). Although the reasons for these high rates are likely complex and multifactorial, it is generally accepted that women living in Latin American countries frequently face restriction and devaluation of opportunities, and poverty, contributing to poorer mental health (Gaviria & Rondon, Citation2010). These challenges are uniquely experienced by Afro-Ecuadorian women: a population that some researchers have found to be at higher risk of reported depressive symptoms compared to the majority mestizo group (Parra-parra et al., Citation2022; Sisa & Vega, Citation2021).
We observed that women in relatively isolated rural communities without road access reported fewer depression and anxiety symptoms – and higher levels of functioning – compared to women in cities and larger towns in Northern Ecuador. Interestingly, this relationship held even though households in these more isolated rural communities had, on average, lower socioeconomic status, and similar rates of food insecurity – both known risk factors for maternal depressive symptoms in Ecuador (Weigel et al., Citation2016) and elsewhere (Goyal et al., Citation2010; Hadley & Patil, Citation2006) compared to more urban sites. This result adds to a body of research on depression rates across rural-urban gradients that have produced conflicting results across diverse global settings (Sampson et al., Citation2020; McCall-Hosenfeld et al., Citation2014; Arvind et al., Citation2019; Bui et al., Citation2018). Nationally, our regional results align with findings from the country-wide 2018 Health and Nutrition Survey (ENSANUT) survey, which found that Ecuadorian women residing in urban areas were at increased risk for postpartum depression compared to rural women (Parra-parra et al., Citation2022). While the reasons for this association between depression and urbanicity are not fully understood, other studies have posited that women living in urban settings may be more exposed to daily stressors in their environment compared to their rural counterparts (Vigod et al., Citation2013), and that urban woman may struggle more with the transition into motherhood specifically due to the tensions between traditional and modern values (Schwank et al., Citation2020). Although we did not measure relative social support, which may play a large role in perinatal depression and anxiety (Fisher et al., Citation2012; Hagaman et al., Citation2021), in prior studies by our group we have also found that more rural and relatively isolated communities tended to report stronger intra-community social networks, as well as a higher degree of community trust and cohesion (Hegde et al., Citation2022).
An additional factor that may have impacted on our results is exposure to urban violence and violence driven by organised criminal activity, which, although not new (Capella et al., Citation2020) increased sharply throughout the province, and most dramatically in the city of Esmeraldas during the period of data collection (February 21 to December 2022) (Bargent, Citation2019; Primicias, Citation2019). The acute challenges posed by the highly violence environment may have impacted study enrollment, as women living in the most unsafe neighbourhoods were screened out early in the recruitment process. Unfortunately, we did not collect data estimate the number of women who were not invited to participate in the study for this reason. Moreover, under or overreporting of depression symptoms due to the pervasive levels of community violence and the potential fear and stigma associated with mental health issues in such settings is a significant concern, as the sample population’s ability to freely express their psychological distress may be hindered by the prevailing atmosphere of insecurity. However, violence in Central and South American, partially associated with organised crime, is escalating and negatively impacts the socio-political landscape. Exposure to urban violence is a recognised risk factor for depressive symptoms and other mental health disorders (Smith et al., Citation2020; Pupo et al., Citation2011), and the role of violence on mental health outcomes in Ecuador has also previously been documented (Cruza-Guet et al., Citation2009). The profound implications on public health and safety are likely to continue.
Our study had several limitations. Our recruitment strategy effectively led to all eligible and interested women in the community enrolled in rural communities and in the town of Borbon, however, in the city of Esmeraldas, recruitment through health centers may have resulted in participants who were not representative of their communities. Thus, care should be taken in extrapolating the results to other urban groups. We relied on self-report of depression and anxiety symptoms that may have resulted in response bias, as well as the potential of social desirability bias. Similarly, the questionnaires included sensitive questions and it is possible that women under-reported depression and/or anxiety symptoms. The Spanish-language version of the HSCL-25 has been validated against the DSM-V criteria (Rodríguez-Barragán et al., Citation2021) that performs well in diverse LMIC populations, including an Afro-Colombian population (Haroz et al., Citation2016) with some similarities to the Afro-Ecuadorian group we describe here. Nevertheless, it is possible that differential functioning of items in this setting may have influenced our prevalence estimates. We were, however, able to assess convergent validity of the maternal health tools. Reported depression and anxiety symptoms were correlated with greater reported challenges in completing daily tasks, which suggests that these symptoms negatively interfered with study participants’ quality of life. Thirdly, due to the delayed implementation of the HSCL caused by the COVID-19 pandemic, some women were not surveyed during pregnancy, but instead either in pregnancy or after their children were born. Although we did not assess the impacts of the COVID-19 pandemic on the mental health of these women directly, we observed a statistically significant increase in the prevalence of symptoms based on the timing of data collection, with more frequent symptoms reported earlier in the pandemic (i.e. early 2022) as opposed to later (late 2022 and throughout 2023). Systematic reviews have demonstrated higher anxiety and depression symptomatology during pregnancy and perinatal period during the COVID-19 pandemic (Hessami et al., Citation2020). There is also evidence of similar adverse perinatal mental health outcomes in comparable scenarios, such as natural disasters and following other stressful life-events (O’Connor et al., Citation2019). ‘Catch-up’ visits were conducted in early 2022 to assess women who could not be assessed prepartum due to the pandemic, and these women reported higher anxiety scores compared to women assessed prepartum. The cross-sectional nature of this study also limits our ability to compare between prepartum and postpartum risk factors, or to establish causality between risk factors and reported symptoms. Future work will investigate the trajectory of reported symptoms among the same population as their children grow.
Mental health care in Ecuador has recently been described as ‘shifting from historical neglect to state recognition’ (Capella et al., Citation2020). The recent COVID-19 pandemic may have accelerated this transition, as the pandemic led to a wave of scientific articles documenting the burden of mental health problems in diverse Ecuadorian populations (Paz et al., Citation2020; Paz et al., Citation2020; Asanov et al., Citation2021; Hidalgo-Andrade et al., Citation2021; Mautong et al., Citation2021), as well as, anecdotally, an expansion of mental health outreach and services by both the public and the private sector. While these activities, as well as the government’s commitment to community-based model of mental health, evidenced by the 2014 strategic plan (MSP, Citation2015), suggest the potential for further action to support maternal mental health, insufficient funding, a lack of trained mental health professionals, and a need for continuing medical education in this space have been identified as key challenges (Vc, Citation2018). In addressing these gaps, researchers have highlighted the need for a medical curriculum that provides historical context for the unique social and political challenges of the Afro-Ecuadorian population of Esmeraldas (Capella et al., Citation2020). For historically marginalised communities and rural communities, culture-centered approaches that include community strengths, resilience, and localised interpretations of mental well-being, have also been promoted (Bates et al., Citation2019).
The present study adds to this discussion by providing a comparative analysis across a rural urban gradient. Our results suggest that both individual-level and household and community-level factors were associated with the risk of depression. Further work should aim to contextualise these results by qualitatively investigating how women in these areas experience and interpret reported symptomatology, as well as factors that may help to support mental health among relatively impoverished and food insecure rural women.
Supplemental Material
Download MS Word (36 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Arvind, B. A., Gururaj, G., Loganathan, S., et al. (2019). Prevalence and socioeconomic impact of depressive disorders in India: Multisite population-based cross-sectional study. BMJ Open, 9, DOI:10.1136/bmjopen-2018-027250
- Asanov, I., Flores, F., McKenzie, D., Mensmann, M., & Schulte, M. (2021). Remote-learning, time-use, and mental health of Ecuadorian high-school students during the COVID-19 quarantine. World Development, 138, 105225.
- Atif, N., Lovell, K., & Rahman, A. (2015). Maternal mental health: The missing ‘m’ in the global maternal and child health agenda. Seminars in Perinatology, 39, 345–352.
- Bargent, J. (2019). Esmeraldas: An Ecuador province gripped by drug conflict. InSight Crime; published online Nov 5. https://insightcrime.org/news/analysis/esmeraldas-an-ecuador-province-gripped-by-drug-conflict/.
- Bates, B. R., Marvel, D. L., Nieto-Sanchez, C., & Grijalva, M. J. (2019). Painting a community-based definition of health: A culture-centered approach to listening to rural voice in Chaquizhca, Ecuador. Frontiers in Communications, 4, 1–13.
- Beck, C. T. (2001). Predictors of postpartum depression: An update. Nursing Research, 50. https://journals.lww.com/nursingresearchonline/Fulltext/2001/09000/Predictors_of_Postpartum_Depression__An_Update.4.aspx.
- Boivin, M., Bangirana, P., Nakasujja, N., et al. (2013). A year-long caregiver training program to improve neurocognition in preschool Ugandan HIV-exposed children. Journal of Developmental & Behavioral Pediatrics, 34, 269–278.
- Boivin, M. J., Nakasujja, N., Familiar, I., et al. (2018). Effect of caregiver training on neurodevelopment of HIV-exposed uninfected children and caregiver mental health: A Ugandan cluster randomized controlled trial. Journal of Developmental & Behavioral Pediatrics, 38, 753–764.
- Bolton, P., Bass, J., Verdeli, H., Clougherty, K. F., & Ndogoni, L. (2003). Group interpersonal psychotherapy for depression in rural Uganda. Jama, 289, 3117–3124.
- Bui, Q. T. T., Vu, L. T. H., & Tran, D. M. (2018). Trajectories of depression in adolescents and young adults in Vietnam during rapid urbanisation: Evidence from a longitudinal study. Journal of Child and Adolescent Mental Health, 30, 51–59.
- Capella, M., Jadhav, S., & Moncrieff, J. (2020). History, violence and collective memory: Implications for mental health in Ecuador. Transcultural Psychiatry, 57, 32–43.
- Coates, J., Swindale, A., & Bilinsky, P. (2006). Household food insecurity access scale (HFIAS) for measurement of food access. Indicator Guide.
- Coates, J., Swindale, A., & Bilinsky, P. (2007). Household food insecurity access scale (HFIAS) for measurement of food access. Indicator Guide.
- Cruza-Guet, M.-C., Spokane, A. R., Leon-Andrade, C., & Borja, T. (2009). Diversity, hegemony, poverty, and the emergence of counseling psychology in Ecuador. Int Handb Cross-Cultural Couns Cult Assumptions Pract Worldwide, 393–401.
- Dadi, A. F., Miller, E. R., & Mwanri, L. (2020). Postnatal depression and its association with adverse infant health outcomes in low-and middle-income countries: A systematic review and meta-analysis. BMC Pregnancy and Childbirth, 20, 1–15.
- Eastwood, J. G., Kemp, L. A., & Jalaludin, B. B. (2015). Being alone and expectations lost: A critical realist study of maternal depression in South Western Sydney. Springerplus, 4(700).
- Eisenberg, J. N., Cevallos, W., Ponce, K., et al. (2006). Environmental change and infectious disease: How new roads affect the transmission of diarrheal pathogens in rural Ecuador. Proceedings of the National Academy of Sciences of USA, 103, 19460–19465. PMCID: PMC1693477.
- Fisher, J., de Mello, M. C., Patel, V., et al. (2012). Prevalence and determinants of common perinatal mental disorders in women in low-and lower-middle-income countries: A systematic review. Bulletin of the World Health Organization, 90, 139–149.
- Gaviria, S. L., & Rondon, M. B. (2010). Some considerations on women’s mental health in Latin America and the Caribbean. International Review of Psychiatry, 22, 363–369.
- Ginja, S., Jackson, K., Newham, J. J., Henderson, E. J., Smart, D., & Lingam, R. (n.d). Rural-urban differences in the mental health of perinatal women: A UK-based cross-sectional study. DOI:10.1186/s12884-020-03132-2
- Go, L., W, C., J, U., et al. (2021). Research response to the COVID-19 pandemic and food insecurity in northern, coastal Ecuador. In American society for tropical medicine and hygiene.
- Goyal, D., Gay, C., & Lee, K. A. (2010). How much does low socioeconomic status increase the risk of prenatal and postpartum depressive symptoms in first-time mothers? Women’s Heal Issues, 20, 96–104.
- Hadley, C., & Patil, C. L. (2006). Food insecurity in rural Tanzania is associated with maternal anxiety and depression. American Journal of Human Biology, 18, 359–368.
- Hagaman, A., Lemasters, K., Zivich, P. N., et al. (2021). Longitudinal effects of perinatal social support on maternal depression: A marginal structural modelling approach. Journal of Epidemiology and Community Health, 75, 936–943.
- Haroz, E. E., Bolton, P., Gross, A., Chan, K. S., Michalopoulos, L., & Bass, J. (2016). Depression symptoms across cultures: An IRT analysis of standard depression symptoms using data from eight countries. Social Psychiatry and Psychiatric Epidemiology, 51, 981–991.
- Hegde, S. T., Trostle, J. A., Mukherjee, B., & Eisenberg, J. N. S. (2022). The importance of community during rapid development: The influence of social networks on acute gastrointestinal illness in rural Ecuador. SSM – Population Health, 19, 101159.
- Hesbacher, P. T., Rickels, K., Morris, R. J., Newman, H., & Rosenfeld, H. (1980). Psychiatric illness in family practice. Journal of Clinical Psychiatry, 41.
- Hessami, K., Romanelli, C., Chiurazzi, M., & Cozzolino, M. (2020). COVID-19 pandemic and maternal mental health: A systematic review and meta-analysis. The Journal of Maternal-Fetal & Neonatal Medicine, 0, 1–8.
- Hidalgo-Andrade, P., Hermosa-Bosano, C., & Paz, C. (2021). Teachers’ mental health and self-reported coping strategies during the covid-19 pandemic in Ecuador: A mixed-methods study. Psychology Research and Behavior Management, 14, 933–944.
- Hsiao, C. (2003). Analysis of panel data (2nd ed.). Cambridge University Press.
- Instituto Nacional de Estadística y Censos. (2010). Censo de Población y Vivienda.
- Kaida, A., Matthews, L. T., Ashaba, S., et al. (2014). Depression during pregnancy and the postpartum Among HIV-infected women on antiretroviral therapy in Uganda. JAIDS Journal of Acquired Immune Deficiency Syndromes, 67), DOI:10.1097/QAI.0000000000000370
- Kinyanda, E., Hoskins, S., Nakku, J., Nawaz, S., & Patel, V. (2011). Prevalence and risk factors of major depressive disorder in HIV/AIDS as seen in semi-urban Entebbe district, Uganda. DOI:10.1186/1471-244X-11-205
- Kohn, R., & Rodríguez, J. (2009). Prevalencia y carga de los trastornos mentales en la población adulta de América Latina y el Caribe. In Epidemiología de los trastornos mentales en América Latina y el Caribe.
- Lee, G. O., Eisenberg, J. N., Uruchima, J., Vasco, G., Smith, S. M., Van Engen, A., Victor, C., Reynolds, E., Mackay, R., Jesser, K. J., & Castro, N. (2021). Gut microbiome, enteric infections and child growth across a rural-urban gradient: Protocol for the ECoMiD prospective cohort study. BMJ Open, 11(10), e046241.
- Leigh, B., & Milgrom, J. (2008). Risk factors for antenatal depression, postnatal depression and parenting stress. BMC Psychiatry, 8, 1–11.
- Leis, J. A., Heron, J., Stuart, E. A., & Mendelson, T. (2014). Associations between maternal mental health and child emotional and behavioral problems: Does prenatal mental health matter? Journal of Abnormal Child Psychology, 42, 161–171.
- Mautong, H., Gallardo-Rumbea, J. A., Alvarado-Villa, G. E., et al. (2021). Assessment of depression, anxiety and stress levels in the Ecuadorian general population during social isolation due to the COVID-19 outbreak: A cross-sectional study. BMC Psychiatry, 21, 1–15.
- McCall-Hosenfeld, J. S., Mukherjee, S., & Lehman, E. B. (2014). The prevalence and correlates of lifetime psychiatric disorders and trauma exposures in urban and rural settings: Results from the national comorbidity survey replication (NCS-R). PLoS One, 9), DOI:10.1371/journal.pone.0112416
- MSP. (2015). Plan Nacional De Salud Mental. Plan Nac Salud Ment, 92.
- Muzik, M., & Borovska, S. (2011). Perinatal depression: Implications for child mental health. Mental Health in Family Medicine, 7, 239–247.
- Nabbe, P., Le Reste, J. Y., Guillou-Landreat, M., et al. (2018). One consensual depression diagnosis tool to serve many countries: A challenge! A RAND/UCLA methodology. BMC Research Notes, 11), DOI:10.1186/s13104-017-3111-x
- Nidey, N., Tabb, K. M., Carter, K. D., et al. (2020). Rurality and risk of perinatal depression among women in the United States. The Journal of Rural Health, 36, 9–16.
- O’Connor, E., Senger, C. A., Henninger, M. L., Coppola, E., & Gaynes, B. N. (2019). Interventions to prevent perinatal depression: Evidence report and systematic review for the US preventive services task force. JAMA – The Journal of the American Medical Association, 321, 588–601.
- Parra-parra, P., Perugachi-p, A., Juan, S., Alem, C., & Chilito-osorio, V. (2022). What factors predispose to postpartum depression in Ecuadorian women ? A cross-sectional analysis. IOSR Journal of Nursing and Health Sciences, 11, 29–40.
- Paz, C., Mascialino, G., Adana-Díaz, L., et al. (2020a). Anxiety and depression in patients with confirmed and suspected COVID-19 in Ecuador. Psychiatry and Clinical Neurosciences, 74, 554–555.
- Paz, C., Mascialino, G., Adana-Díaz, L., et al. (2020b). Behavioral and sociodemographic predictors of anxiety and depression in patients under epidemiological surveillance for COVID-19 in Ecuador. PLoS One, 15, 1–14.
- Primicias, R. (2019). Presidente decreta estado de excepción en Guayas, Manabí y Esmeraldas, ante inseguridad Para hacer uso de este contenido cite la fuente y haga un enlace a la nota original en Primicias.ec: https://www.primicias.ec/noticias/politica/estado-excepcion-parroq. Primicias. https://www.primicias.ec/noticias/politica/estado-excepcion-parroquias-guayas-manabi-esmeraldas/.
- Pupo, M. C., Jorge, M. R., Schoedl, A. F., et al. (2011). The accuracy of the clinician-administered PTSD scale (CAPS) to identify PTSD cases in victims of urban violence. Psychiatry Research, 185, 157–160.
- R Core Team. (n.d). R: A language and environment for statistical computing. 2017. https://www.r-project.org/.%0A.
- Rieder, A. D., Roth, S. L., Musyimi, C., et al. (2019). Impact of maternal adverse childhood experiences on child socioemotional function in rural Kenya : Mediating role of maternal mental health. DOI:10.1111/desc.12833
- Rodríguez-Barragán, M., Fernández-San-martín, M. I., Clavería-Fontán, A., et al. (2021). Validation and psychometric properties of the spanish version of the hopkins symptom checklist-25 scale for depression detection in primary care. International Journal of Environmental Research & Public Health, 18, 1–15.
- Sampson, L., Ettman, C. K., & Galea, S. (2020). Urbanization, urbanicity, and depression: A review of the recent global literature. Current Opinion in Psychiatry, 33, 233–244.
- Santos, D. S., Santos, D. N., De Cássia Ribeiro Silva, R., Hasselmann, M. H., & Barreto, M. L. (2011). Maternal common mental disorders and alnutrition in children: A case-control study. Social Psychiatry and Psychiatric Epidemiology, 46, 543–548.
- Schwank, S., Lindgren, H., Wickberg, B., Fu, S.-C., Yan, D., & Andersson, E. (2020). When a new mother becomes mentally unhealthy, it is everyone’s problem: Shanghai women’s perceptions of perinatal mental health problems. Women's Reproductive Health, 7, 190–204.
- Shorey, S., Chee, C. Y. I., Ng, E. D., Chan, Y. H., Tam, W. W. S., & Chong, Y. S. (2018). Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. Journal of Psychiatric Research, 104, 235–248.
- Sisa, I., & Vega, R. (2021). Prevalence of depression in older adults living in Ecuador and contributing factors: A population-based study. Revista de Saúde Pública, 23, 1–10.
- Smith, M. E., Sharpe, T. L., Richardson, J., Pahwa, R., Smith, D., & DeVylder, J. (2020). The impact of exposure to gun violence fatality on mental health outcomes in four urban U.S. Settings. Social Science & Medicine (1982), 246, 112587.
- Surkan, P. J. (n.d). Early maternal depressive symptoms and child growth trajectories : A longitudinal analysis of a nationally representative US birth cohort.
- Thompson, A. L., Jahnke, J. R., Teran, E., & Bentley, M. E. (2022). Pathways linking maternal mental health and child health in a dual burden context: Evidence from Galapagos, Ecuador. Social Science & Medicine (1982), 305, 115043.
- Trostle, J. A., Hubbard, A., Scott, J., Cevallos, W., Bates, S. J., & Eisenberg, J. N. S. (2008). Raising the level of analysis of food-borne outbreaks. Epidemiology, 19), DOI:10.1097/EDE.0b013e31816a9db0
- Tsai, A. C., Wolfe, W. R., Kumbakumba, E., et al. (2016). Prospective study of the mental health consequences of sexual violence among women living with HIV in rural Uganda. Journal of Interpersonal Violence, 31, DOI:10.1177/0886260514567966
- Vc, B. (2018). Community mental health, primary health care and health promoting universities in Ecuador. Revista Panamericana de Salud Publica, 42.
- Vigod, S. N., Tarasoff, L. A., RM, B. B., Dennis, C.-L., Yudin, M. H., & Ross, L. E. (2013). Relation between place of residence and postpartum depression. Canadian Medical Association Journal, 185, 1115.
- Weaver, A., Himle, J. A., Taylor, R. J., Matusko, N. N., & Abelson, J. M. (2015). Urban vs rural residence and the prevalence of depression and mood disorder among African American women and non-hispanic white women. JAMA Psychiatry, 72, 576–583.
- Weigel, M. M., Armijos, R. X., Racines, M., Cevallos, W., & Castro, N. P. (2016). Association of household food insecurity with the mental and physical health of Low-income urban Ecuadorian women with children. Journal of Environmental and Public Health, 2016, DOI:10.1155/2016/5256084
- Winokur, A., Winokur, D. F., Rickels, K., & Cox, D. S. (1984). Symptoms of emotional distress in a family planning service: Stability over a four-week period. British Journal of Psychiatry, 144), DOI:10.1192/bjp.144.4.395
- World Health Organization. (2017). Depression and other common mental disorders: Global health estimates. Geneva, Switzerland.
- Yin, X., Sun, N., Jiang, N., et al. (2021). Prevalence and associated factors of antenatal depression: Systematic reviews and meta-analyses. Clinical Psychology Review, 83, 101932.
- Zelner, J. L., Trostle, J., Goldstick, J. E., Cevallos, W., House, J. S., & Eisenberg, J. N. (2013). Social connectedness can inhibit disease transmission: Social organization, cohesion, village context and infection risk in rural Ecuador. American Journal of Public Health, 102, 2233–2239. PMCID: PMC3519324.
