
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Bangladesh, one of the world’s poorest countries, has experienced a dramatic decline in fertility since 1985, with a decline in the total fertility rate from 5.5–2.1. International researchers have debated the reasons for this rapid decline, with some studies attributing it primarily to family planning programmes and others pointing at the simultaneous increase in the education of women and other socioeconomic factors. Using data from seven-rounds of the Bangladesh Demographic Health Survey (BDHS), we comprehensively review fertility trends by reconstructing cohort and period fertility indicators by educational attainment. Multilevel regression shows a robust negative association between fertility and educational attainment at the individual and community levels. Pathway’s analysis reveals that female education has a significant effect on declining fertility desires dominating all other effects. Increased women's education and the associated diffusion of smaller desired family size might be the primary factor driving the impressive fertility decline in Bangladesh.
1. Introduction
Bangladesh is a prominent country of study for demographers wanting to demonstrate the effectiveness of family planning programmes. One of the world’s poorest countries, it has experienced a steep decline in fertility; from a total fertility rate (TFR) of 5.5 in 1985, to 3.7 in 1995, to 2.1 in 2017 (The World Bank, Citation2019). Given the concentrated efforts at family planning and the low economic development over these years, studying Bangladesh seems like a sort of natural experiment that can help isolate the effects of these two possible drivers of the decline in fertility, which in many other countries tend to change together. A recent prominent paper on population growth and climate change (Bongaarts & O’Neill, Citation2018) singled out Bangladesh as an example that family planning programmes work and are effective at kerbing population growth.
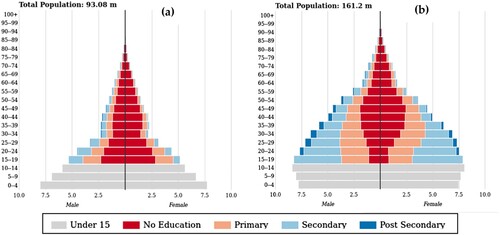
However, a closer look at the available data and in-depth studies of the drivers of the decline in fertility in Bangladesh reveals that the evidence for this strong claim is surprisingly fragmentary. In particular, the educational attainment of women of reproductive age has increased roughly in parallel with a decline in the birth rate. illustrates this with age and education pyramids for the years 1985 and 2015. The figure shows the change from a very large proportion of children together with the majority of women of reproductive age having no education at all (dark red) to the majority of women having a primary education or higher at the bottom of the pyramid. More than half of the youngest cohorts even have a secondary education, as we discuss later. Many other studies also point to the important role of education in the decline in fertility in Bangladesh.
Figure 1. Population pyramids (in millions) with medium SSP2 scenario by education for (a) 1985 and (b) 2015, Bangladesh Source: Wittgenstein Centre (Citation2018)
Note: The population component of SSP2 is a middle-of-the-road scenario that can be seen as the most likely path for a country. It combines medium fertility with medium mortality, medium migration, and the Global Education Trend education scenario.
In this context, we comprehensively assess fertility trends by merging data from seven rounds of BDHS between 1993 and 2014 and constructing cohort histories and period rates by education level. Using multilevel analysis, we also re-examine the relative effects of changes in education and different family planning efforts and usage indicators after controlling for other factors. The advantage of using a multilevel approach is that it considers the direct compositional effect of improving educational attainment and addresses spill-over and diffusion effects at the local level.
This study contributes to a long-standing debate among demographers and health researchers about whether the education of females or family planning programmes is the main factor driving declines in fertility and thus should receive priority when the goal is to kerb rapid population growth. A long tradition of research has highlighted the impact of educating females on bringing fertility within the calculus of conscious choice (Coale, Citation1973), enhancing the numeracy in desired family size (Van van de Walle, Citation1992), increasing the mean age at marriage, empowering women to pursue their desire for a smaller family vis-à-vis their husbands, and increasing the opportunity cost of children (Basu, Citation2002; Bongaarts, Citation2010; Cleland, Citation2002; Jejeebhoy, Citation1996; Kravdal, Citation2002; Lutz & Skirbekk, Citation2013; Martin & Juarez, Citation1995). However, it has also been argued that family planning programmes have been highly effective by providing easier access to contraception, promoting the advantages of smaller families, or often doing both. These studies mostly point to Asian countries that have experienced accelerated declines in fertility in a short period, such as Bangladesh, Indonesia, and Iran (Angeles et al., Citation2005; Carty et al., Citation1993; Cleland et al., Citation1994; Erfani & McQuillan, Citation2008; Gertler & Molyneaux, Citation1994). Of course, the two approaches—educating females and family planning—are not mutually exclusive, and it has also been argued that they reinforce each other (Bongaarts, Citation2017; Lutz, Citation2014).
We first briefly discuss fertility in Bangladesh and summarise previous studies on the topic. Next, we describe the data and the methods used to sequence seven rounds of the surveys to identify trends in age- and education-specific fertility by cohort and period. Then we discuss data and evidence for available family planning efforts and outcome indicators over time. Finally, we define the multilevel statistical model and apply it to individual round of BDHS and a merged data set. We conclude with a summary of our findings and some discussion.
2. Fertility trends in Bangladesh
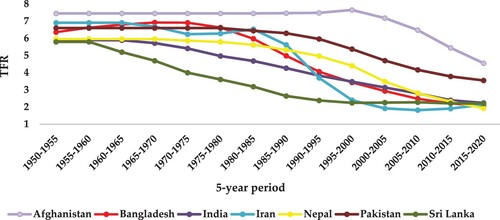
The rapid decline in fertility in Bangladesh since 1980 has caught the attention of international researchers and policymakers for several reasons. First, Bangladesh was one of the world’s poorest countries when it experienced the steep decline in TFR. Until 1980, Bangladesh had a higher fertility rate than most other countries in South Asia (see ), but after that it experienced a more rapid decline than the other countries. Second, as a rare exception in the history of fertility transitions worldwide, the decline in fertility in Bangladesh began at a relatively high level of under-5 mortality. It was still above 200 per 1,000 births in 1975–1980, which means that 1 out of 5 children died before reaching age 5. Finally, Bangladesh underwent a substantial socioeconomic transformation when fertility started falling, triggering efforts by researchers to disentangle the drivers of and better understand the demographic transition, to ultimately apply their findings in high-fertility countries.
Figure 2. Trends in fertility estimates for South Asian countries according to UN-WPP Source: United Nations (Citation2019).
In Bangladesh, family planning activities were carried out in three distinct phases. In phase I in the early 1950s, activities were mostly voluntary. In phase II in the 1960s, the government took broader steps to check population growth. Population control was officially adopted in Pakistan’s First Five-Year Plan (1960–1965). During these two phases, Bangladesh was a part of Pakistan. In phase III, after Bangladesh achieved independence in 1971, the first Five-Year Plan of Bangladesh was launched with the clear priorities of population control and food production. Phase III also marked the beginning of a comprehensive multi-sector, broad-based population control and family planning programme (Khuda & Barkat, Citation2012).
2.1. The impact of family planning on the decline in fertility in Bangladesh
There is an unresolved debate over the impact of family planning on fertility in Bangladesh. Until the mid-1980s, government family planning programmes had little success, despite expending considerable effort and money to reduce fertility. According to an analysis of data from the Poverty and Fertility Survey conducted in 1977 in four rural areas of the country, the modest increase in the use of contraceptives in Bangladesh had no significant impact on fertility (Amin et al., Citation1985). This study found that child mortality and the use of contraceptives were positively related to the number of children born. The positive correlation between the use of contraceptives and the number of children born can be explained by the fact that the use of contraceptives usually began late in a couple’s reproductive life. This implies that although contraceptives play some role in depressing fertility at higher parities, high child and infant mortality and secondary sterility (at higher ages) dominated the fertility pattern in Bangladesh in the study period. Many other studies in this period confirmed that at the family level, the benefits of practising contraception were minimal (Arthur & McNicoll, Citation1978; Cain, Citation1981, Citation1983; Demeny, Citation1975; Khuda, Citation1978). Analysing trends in the use of contraceptives between 1969 and 1983, Amin et al. (Citation1987) found a steady increase in conception among all women of all subgroups, irrespective of place of residence, education, or parity. However, women of high parity, women with more education, and those living in urban areas were more likely to use contraceptives (Amin et al., Citation1987). Comparing trends in family size preferences and the use of contraceptives in treatment and comparison areas in Matlab, Bangladesh, Koenig et al. (Citation1987) inferred that although education, modernising influences, and growing diversity contributed to changes in reproductive preferences, maternal child health and family planning programmes were successful in addressing reproductive preferences in the treatment area.
The debate over fertility in Bangladesh intensified with the publication of studies (Carty et al., Citation1993; Cleland et al., Citation1994) that attributed the decline in fertility to increased use of contraceptives. Cleland et al. (Citation1994) concluded, that it is unnecessary and indeed implausible to invoke economic change and shifts in the utility of the children as the central determinant. Carty et al. (Citation1993) concluded that no change was needed in economic development, urbanisation, the employment of women, or education for family planning to succeed. They pointed to the critical importance of sustained political commitment to an effective family planning programme adopted and pursued at the highest government levels (as stated in Caldwell et al., Citation1999). Arends-Kuenning (Citation2001) demonstrated that visits from family planning workers affected women’s contraceptive behaviour by decreasing contraception costs. Women from programme villages experienced long-term consequences of outreach programmes in terms of increased birth spacing, lower child mortality, improved health, and greater use of preventive health inputs (Joshi & Schultz, Citation2013).
Another feature specific to Bangladesh is the long series of data from in-depth studies in the Matlab project. Sinha (Citation2005) found that women exposed to intensive family planning programmes in the Matlab area had a 14 per cent reduction in lifetime fertility. That study concluded that family planning programmes were highly successful at reducing fertility. Using data from the 1991 Contraceptive Prevalence Survey of 11,065 women, researchers found that the most significant determinant of using modern contraceptive methods in a rural area was a visit by a Family Welfare Assistant within the past 3 months. After the Family Welfare Assistant visit, the odds of use for rural women increased 8 times, whereas the odds of use for urban women increased 2.6 times (Kamal & Sloggett, Citation1996). A study of 141 villages in Matlab from 1974 to 1996 confirmed a decline in fertility of about 15 per cent in programme villages (which received door-to-door outreach family planning and maternal/child health programmes) compared to control villages (Schultz, Citation2009).
It is interesting that a more recent study assessing the achievements and limitations of the Bangladesh Family Planning Programme concluded that the programme achieved commendable success until the mid-1990s, then slowed, resulting in a stalling or near stagnation in fertility in recent years (Khuda & Barkat, Citation2012). It suggested that an erosion in political will and government commitment after the mid-1990s together with high adolescent fertility and sharp differences in fertility by socioeconomic status led to a plateau in fertility.
2.2. The impact of education and other factors on the decline in fertility in Bangladesh
According to Caldwell et al. (Citation1999), Bangladesh has undergone a great transformation as a result of urbanisation (which increased from 6 per cent in 1965–20 per cent in 1997), improvements in the Human Development Index (which saw about a 45.5 per cent increase between 1960 and 1980), a massive increase in the number of girls attending primary school and high school (70 per cent and 60 per cent, respectively, between 1973 and 1986), and improvements in many other indicators (e.g., the number of villages with electricity, the number of doctors and nurses). These researchers strongly refuted the notion that family planning programmes alone were responsible for the decline in fertility. However, they may have impacted the timing of the onset of the decline in fertility and the pace of the decline.
Some qualitative studies have also concluded that family planning programmes were not successful. In-depth interviews of 104 women and 92 men (including 85 couples) as part of an ethnographic study in rural Bangladesh, suggested that despite their success increasing the prevalence of contraception, such programmes often failed to provide adequate information or support users of contraceptives (Schuler et al., Citation1995). Some other studies in the late 1990s claimed that the faster decline in fertility in Bangladesh resulted from a combination of socioeconomic changes, with substantial input from family planning programmes. A qualitative study by Caldwell and Khuda (Citation2000) suggested that family planning programmes have played an essential role in reducing family size. Still, economic and social changes and growing aspirations have made couples more receptive to family planning.
More recent studies have also documented that the reduction in fertility in Bangladesh is the result of the education of women, economic status, access to mass media, urbanisation, and the efforts of family planning programmes (Amin et al., Citation1996; Amin, Hill, et al., Citation1995; Hahn et al., Citation2018; Khuda et al., Citation2000, Citation2018; Khuda & Hossain, Citation1996). Some other studies have found striking similarities in reproductive behaviour in Western divisions of Bangladesh and West Bengal in India (Amin et al., Citation2002; Das et al., Citation2020). It has been argued that the education and modernisation processes started among the elites of greater Bengal (current Bangladesh and the state of West Bengal in India) with a strong allegiance to the Bengali language. Later this strong sense of language identity facilitated and reinforced modern ideas both within and between the two Bengali-speaking regions (Basu & Amin, Citation2000). Fertility behaviour in Bangladesh and the border divisions of West Bengal indicates cross-border diffusion of fertility practices (Das et al., Citation2020).
Schooling has had a large and statistically significant effect on the use of traditional and modern reversible contraceptives (Cleland et al., Citation1996; Hoque & Murdock, Citation1997). Participation in income-generating projects or accessing of credit programmes by poor rural women is associated with delayed marriage and childbirth, increased use of contraceptives, decreased fertility, and an increased desire for no more children (Amin, Cleland, et al., Citation1995; Heath & Mobarak, Citation2015; Schuler et al., Citation1997). The education of women is always a significant determinant of the use of contraceptives: Modern and traditional teenage girls who had no education had 2.76 times higher odds of becoming mothers as adolescents than their counterparts with more than a secondary education (Islam et al., Citation2017). The education of women is a significant positive predictor of the use of contraceptives among employed and unemployed women in Bangladesh (Islam et al., Citation2016).
Recently some authors have claimed that Bangladesh experienced two episodes of fertility stall: in 1996–2000 and in 2011–2014. Whereas the first stall occurred at 3.3 births per woman, the second stall occurred at 2.3 births per woman (Khuda & Barkat, Citation2012; Rahman, Citation2018). Rahman argued that decrease in family planning services was strongly associated with both stalls. Moreover, a decline in labour force participation among women was closely associated with the first stall, whereas not having any education, living in a rural area, and being Muslim were associated with the second (Rahman, Citation2018).
This literature review on the drivers of fertility trends in Bangladesh clearly shows that this has been a highly controversial issue for decades, and no consensus seems to be on the horizon. Here we revisit these issues using the broadest possible data set by merging data from seven rounds of the nationally representative BDHS through the pooling of birth histories.
3. Data and methods
We used data from seven rounds of the BDHS: 1993–1994, 1996–1997, 1999–2000, 2004, 2007, 2011, and 2014. The BDHS is a nationally representative survey conducted under the authority of the National Institute for Population Research and Training of the Ministry of Health and Family Welfare, Government of Bangladesh, and implemented by Mitra and Associates of Dhaka. It is part of the worldwide Demographic and Health Surveys (DHS) programme designed to collect data on fertility, family planning, and maternal and child health. We present data on the sample for different rounds of the BDHS in .
Table 1. Sample coverage of the Bangladesh Demographic Health Survey in 1993–2014, Bangladesh.
Details on the sample design and survey methodology can be found in respective reports on the BDHS. Individual-level data are available from the DHS data repository and accessible on request.
We used the tfr2 Stata module, developed by Schoumaker (Citation2013), to compute fertility rates from birth histories and estimate trends in TFR across all rounds of the BDHS data. Bivariate and multilevel analyses were performed. At the bivariate level, cross-tabulation was performed to determine the percent distribution of women’s characteristics by BDHS survey rounds. A three-level mixed-effects linear regression model was run to examine the association between fertility and selected predictors.
4. Trends in pooled BDHS data
To address apparent inconsistencies in fertility rates for the same cohorts derived from different rounds of the BDHS, we reconstructed the fertility trends by pooling birth histories from successive surveys. We applied the adjustment procedures discussed by Schoumaker (Citation2014). We distinguished among women with four levels of educational attainment: no education, primary education, secondary education, and higher education as defined by the BDHS. As the DHS is a representative sample survey, the information collected at different time points for the same cohorts of women is not necessarily the same. The ‘figure in Appendix 1’ shows cohort fertility rates for Bangladeshi women without any formal education derived from different rounds of surveys. It shows different cohort fertility rates for the same cohorts interviewed at different times, in particular for earlier cohorts. Thus, reconstructing fertility trends by merely pooling birth histories from different surveys would be not meaningful. Therefore, we followed the strategy described below to reconstruct TFRs.
We estimated age-specific fertility rates for women of the same age for the same cohorts. To do this, we used a weighted average of the different surveys. First, for each survey, we computed birth events and exposures by age, birth year, and education. Second, we computed the weighted average of events and exposures of different surveys by age, birth cohort, and education. Third, we smoothed the age- and education-specific averaged events and exposures using spline functions across ages and birth cohorts. Finally, we computed age- and education-specific cohort fertility rates from the smoothed weighted average of events and exposures.
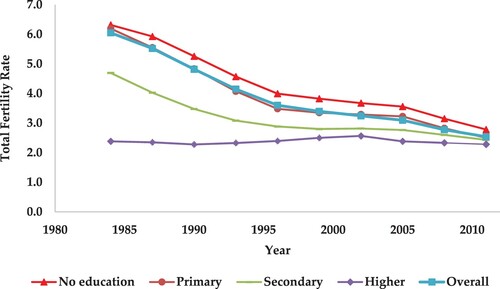
presents reconstructed TFRs for Bangladesh for the period 1984–2011 based on successive rounds of the BDHS. It reveals that after an initial sharp decline in TFR from 1987 to the mid-1990s, Bangladesh experienced some stall in TFR between 1996–2004. After that, fertility continued to decline until 2011. The reconstructed TFRs did not exhibit the aforementioned second stall in 2011–2014. The trends in TFR by educational attainment show a striking pattern (). The TFRs for women with secondary education and higher education are substantially lower than those of women with no education or a primary education, which converge in the most recent period. Whereas women with no education or a primary education experienced a similar decline in fertility or stall compared to all women over time, women with secondary education or higher education followed a different trajectory. Women with secondary education experienced a decline in fertility from a TFR of 4.7 in 1984–3.1 in 1993, then experienced a stall for an extended period between 1996 and 2005. The TFR for women with higher education was almost constant, from 2.4 in 1984–2.3 in 2011.
Figure 3. Period total fertility rate (3-year moving average) by education, 1984–2011, Bangladesh Source: Authors’ own calculation from various waves of the BDHS, 1993–1994–2014.
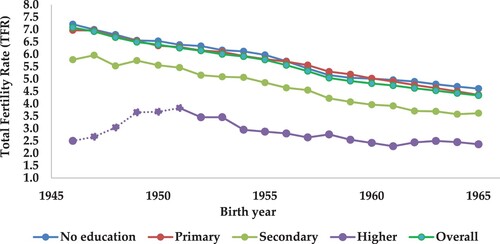
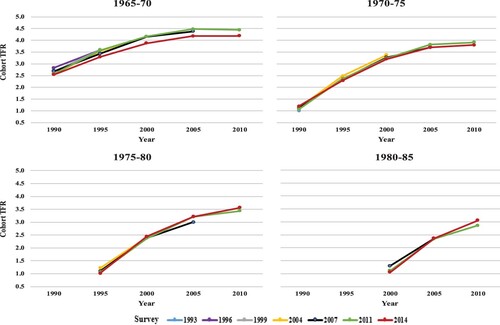
presents TFRs by birth cohort and education. Aside from the very small group of women with higher education born before 1955, there was a continuous decline in overall TFR for each consecutive birth cohort at each level of education. This remarkably consistent picture also does not show any stalls in TFR. Although the trends for women with no education or a primary education and the national average are very similar, the difference for women with secondary education is roughly one child and is surprisingly constant over time. Women with higher education have the lowest fertility rates, although trends have to be interpreted with caution due to small numbers.
Figure 4. Total fertility rate by birth cohort (3-year moving average) and education among women ages 15–49, Bangladesh Source: Authors’ own calculation from various waves of the Bangladesh Demographic Health Survey, 1993–1994–2014
Note: Dotted lines indicate a small number of cases.
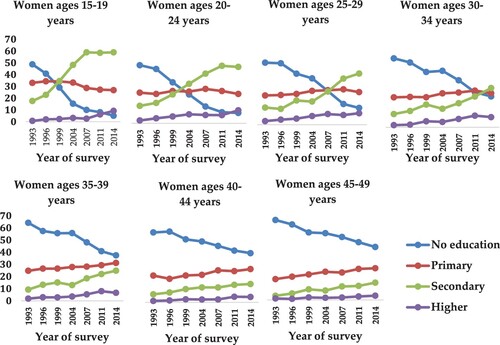
To put these trends in education-specific fertility into context, shows trends in educational attainment for women by 5-year age groups for the period 1993–2014. reveals a sharp increase in the proportion of women ages 15–34 with secondary education since the mid-1990s. In contrast, the percentage of women with a primary education either remained stagnant or decreased. At the same time, there was a sharp decline in the percentage of women with no education. The per cent share of women with higher education increased from 0 per cent to about 10 per cent for women ages 15–34.
Figure 5. Trends in women’s level of education by 5-year age group in the BDHS, 1993–2014, Bangladesh.
5. Trends in indicators of family planning programs
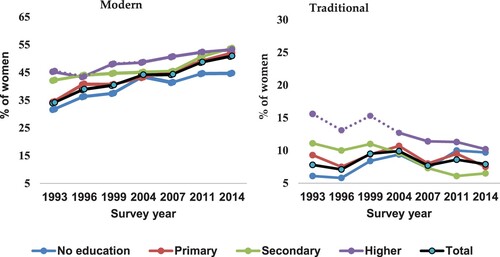
shows trends in contraceptive use (modern and traditional method) by women’s (aged 15–49) by the level of education, Bangladesh. In the BDHS, the use of contraception is defined as the use of a family planning method by a currently married woman at the time of the survey. Modern methods include female sterilisation, male sterilisation, the pill, intrauterine devices, injectables, implants, and male condoms. Traditional methods include periodic abstinence, withdrawal, and other traditional methods. As expected, the percentage of women using contraception was lower among women without education than among women with some education (women with no education: 44.8 per cent vs. women with higher education: 53.3 per cent). Over time, all education groups showed increased of use of modern contraceptive methods, with the most recent years showing stagnation among uneducated women. The use of traditional methods was roughly constant over time, with a temporary increase around 2000–2005. It is interesting to note that women with the highest education also had the highest use of traditional methods, although this declined over time. They also had the highest use of modern contraception, which implies that they generally had a greater desire to avoid pregnancy by any method. Analyses of DHS data from other countries on obstacles to meeting the unmet need for contraception suggest that this could also be explained by a greater fear of side effects among more educated women who do want to conceive but have more access to information about possible side effects (Lutz, Citation2014).
Figure 6. Trends in contraceptive use (modern and traditional method) by women's (aged 15-49) by the level of education, Bangladesh
Note: Dotted lines indicate a small number of cases.
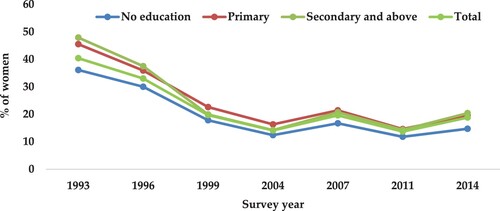
presents trends in visits by family planning field workers (FPFWs) to women in the past 6 months by education. In 1993, FPFWs visited 40.4 per cent of all women of reproductive age. The percentage of women visited by FPFWs was higher among women with secondary education or above (47.9 per cent) than women without education (36.1 per cent). Overall, the percentage of women visited by FPFWs declined sharply from 40.4 per cent in 1993–19.7 per cent in 1999 and remained within a range of 19.6 per cent to 13.7 per cent in the following years. In all DHS rounds, women without education had less access to FPFWs than educated women, although the difference between these two groups was not substantial.
Figure 7. Trends in visits by family planning field workers (FPFWs) to women ages 15–49 in the past 6 months by education.
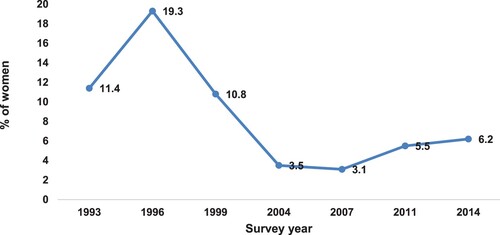
presents trends in the percentage of women who received family planning support at a satellite clinic in the local area in the 3 months before the survey. Only a small percentage of women received such services, according to DHS data.
Figure 8. Percentage of women ages 15–49 who received family planning support at a satellite clinic in the local area during the past 3 months, 1993–2014, Bangladesh.
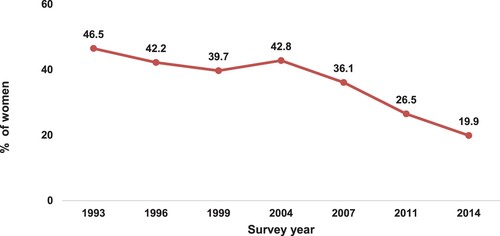
We also investigated the possible role of media in awareness of family planning programmes among women in Bangladesh. presents trends in the percentage of women reporting having been exposed to messages about family planning programmes in mass media. Respondents were asked whether in the past month they had heard about family planning a) on the radio, b) on the television, c) in a newspaper or magazine, or d) from a poster or billboard or leaflet. In our analysis, we considered women to have been exposed to media if they had heard, read, or seen about family planning programme messages on radio, television, newspapers/magazines, posters, brochures, or billboards last month before the survey. From 1993 to 2004, more than 40 per cent of women were exposed to family planning messages in mass media; this percentage decreased to 19.9 per cent by 2014.
Figure 9. Percentage of women ages 15–49 who were exposed to (heard, saw, or read) family planning messages in mass media in the past month, 1993–2014, Bangladesh.
6. Multilevel analysis
The aforementioned trends of convergence in the fertility levels of different education groups—at least for recent TFRs—together with a general decline in the indicators of family planning efforts and utilisation of services looks somewhat puzzling at first sight. What were the forces decreasing fertility and increasing the use of contraceptives in the less educated groups under weakening family planning efforts and services? The most plausible explanation is strong diffusion of the ideal of a smaller family size and the use of contraception from more educated to less educated women. Because such diffusion tends to happen at the local and community levels, a natural way of studying it would be to run multilevel statistical models that consider education and family planning indicators at the individual and community levels. We thus ran models that controlled for household wealth, religion, urban/rural residence, female empowerment, gender preference, and region in each DHS round separately and in a merged data set of all seven rounds.
We use the number of children born in the past 5 years to women ages 15–49 as the dependent variable. We also included age group as a control variable in the model to capture additional births after age 35 and possibly inter-cohort changes.
Following the literature and the available data, we selected independent variables at two levels: the individual and the community. Individual-level predictors were the age of the woman in years (15–24, 25–34, 35–44, 45–49); women’s level of education (no education, primary, secondary or higher); religion (Islam, other); place of residence (urban, rural); wealth index (poorest, poorer, middle, richer, richest); FPFW visit to the respondent’s house in the past 6 months (no, yes); and division of residence (Barisal, Chittagong, Dhaka, Khulna, Rajshahi, Rangpur, Sylhet). Community-level predictors were the proportion of educated women in the community (sample cluster) and the proportion of women visited by health workers in each community. We generated the community-level variables by aggregating individual women’s responses within their clusters. We computed the aggregates for clusters using the mean proportion in each category of a given variable.
Mixed-effects models, which contain both fixed effects and random effects, are essential in multilevel analyses and were used to interpret the results.
The fact that the DHS data are hierarchical, that is, women at the individual level (i), nested within clusters (j), nested within divisions (k), allowed us to use multilevel modelling. A three-level mixed-effects model was written as.
where outcome yijk is the number of children born in the past 5 years of ith women of jth community from kth division; xpijk is the pth independent variable at the individual (level 1), community (level 2), and division (level 3) levels;
is the corresponding regression coefficient;
is the random effect of division assumed to be normally distributed with N (0,
);
is the random effect of community assumed to be normally distributed with N (0,
); and
is the random error assumed to be normally distributed with N (0,
) and independent of the random effects at both level 2 and level 3.
presents sample characteristics of women ages 15–49 for the individual and pooled BDHS. Over the study period, the mean number of children born in the past 5 years declined from 0.74 in 1993–1994–0.44 in 2014. The percentage of women with no education declined by 58.4 per cent (from 56.5 per cent in 1993–1994–23.5 per cent in 2014). The percentage of women with secondary or higher education increased from 15.8 per cent to 47.2 per cent. In all rounds, more than 85 per cent of women reported practising Islam. The percentage of women living in urban areas increased substantially (from 15.3 per cent to 34.5 per cent). Finally, the proportion of educated women in the community increased, whereas the proportion of women in the community visited by FPFWs either declined or remained stagnant.
Table 2. Selected characteristics of women ages 15–49 years for regression analyses of BDHS data, 1993–1994, 2004, 2014, and 1993–2014, Bangladesh.
Results of multilevel regression modelling of pooled data for women ages 15–49 years are presented in . We ran three stepwise models for . Model 1 shows regression coefficients for all socio-economic determinants. Model 2 presents regression coefficients for family planning and proximate determinants, and Model 3 presents regression coefficients for all socio-economic, family planning and proximate determinants.
Table 3. Results of multilevel regression modelling of births in the past 5 years to women ages 15–49 with associated predictors, pooled data, Bangladesh.
The results of model 1 in shows that the variance in children born in the past 5 years was much higher at the individual level (variance = 0.385) than at the community (variance = 0.006) or division (variance = 0.009) levels. The intra-class correlation coefficients showed that when individual-level characteristics were adjusted, about 4 per cent of the variance in children born in the past 5 years was due to clustering at the community level. Compared to women with no education, women with primary (β = –0.02, SE: 0.01, p < 0.001) and secondary or higher (β = –0.03, SE: 0.01, p < 0.001) education had a lower likelihood of having had children born in the past 5 years. Women belonging to other religions had a lower likelihood of having more children (β = –0.06, SE: 0.01, p < 0.001). As expected, rural women (β = 0.02, SE: 0.01, p < 0.001) had a higher likelihood of having more children than urban women. Women belonging to households of the richest wealth index had a lower likelihood of having more children than the women belonging to households of the poorest wealth index. It was also observed that female empowerment and gender preference helping in lowering the fertility. The proportion of educated women in the community was also significantly inversely associated with children born in the past 5 years (β = –0.16, SE: 0.02, p < 0.001).
In model 2, which includes indicators of family planning efforts as well as the proximate determinant of contraceptive use, shows that family planning messages in mass media in the past month (β = –0.05, SE: 0.01, p < 0.001) had a negative association with children born in the past 5 years. It is interesting that women visited by a FPFW had a higher likelihood of having had more children than women who were not visited by a FPFW (β = 0.15, SE: 0.01, p < 0.001). This significant positive effect may indicate that visits by FPFWs may be associated more with pregnancies and maternal health than with efforts to prevent births. Other indicators such as modern contraceptive use and service received from temporary health clinic (family planning methods) had a significant positive association with the children born in the past 5 years. It is worth mentioning that the information on modern contraceptive use was at the time of survey whereas the dependent variable is the number of births in the past 5 years to women.
In the final model 3, which included all indicators, individual women’s education and the proportion of educated women in the community had a consistently significant negative effect. In contrast, all the family planning indicators except mass media had a positive significant association with fertility. Also, female empowerment and gender preference had significant adverse effects on births in the past 5 years. The effect of age on children born in the past 5 years was—as it should have been—very regular and highly significant, with the number of children born in the past 5 years decreasing with women’s age. In all the models the proportion of educated women in the community was also negative and significant on top of the individual-level effects. This points to a significant role of diffusion that further depresses fertility even among women with low education in an environment of better-educated women.
Further, we analysed four pathways (present in ) for modern contraceptive use, women empowerment, mass-media exposure and fertility desire through which women’s education might reduce fertility in Bangladesh. We used the same multi-level analysis approach, and substituted the pathway outcomes for the fertility indicator. Though it does not include a number of other possible pathways, partly due to data constraints, this analysis revealed the different pathways through which education would affect fertility decline in Bangladesh.
Table 4. The effect of women’s education on pathways through which formal education attainment may affect fertility (marginal effects are reported).
Results of a sensitivity test of the diffusion effects for the last two rounds of the survey (2004 and 2014) are presented in ‘Table in Appendix 2’. The higher proportion of women with secondary education or more corresponded to a significantly lower number of children (born in the past 5 years). However, the interaction terms for community education and individual education revealed that the impact of increasing community education was not the same across all education groups. Women with no education or a primary education tended to respond more strongly to the increasing number of educated women in the community. In contrast, the fertility of women with secondary education or more did not change significantly with the increasing number of women with similar education levels in the community (and even showed a tendency to increase). This suggests a positive spill-over effect of fertility and reproductive knowledge transmitted from better educated groups to women with no education or a primary education.
7. Discussion and conclusion
The various studies debating the relative roles of education and family planning programmes in driving the decline in fertility in Bangladesh are inconclusive. We addressed this question using the broadest possible set of available individual-level data. We merged individual data from seven rounds of the BDHS between 1993 and 2014, including more than 85,000 observations for almost 1,700 community groups and seven regional divisions.
In addition to merging these individual-level data, we made a considerable effort to reconstruct consistent trends over time in both period and cohort fertility by education, thus avoiding inconsistencies and adjusting for known problems with DHS birth history data. These problems include misreporting of dates of birth (age heaping, displacement of recent births, the Potter effect), underreporting of births (omitting distant or recent births), sample implementation (oversampling, under sampling), and misreporting of women’s age (Schoumaker, Citation2014). To address these issues, we reconstructed the trend in TFR using pooled birth histories from various rounds of the BDHS. Some of the new TFR estimates are higher than those in published reports of the BDHS. The reconstructed trend in TFR in this study is consistent with the trend presented by Schoumaker (Citation2014). It shows that Bangladesh experienced a steep decline in fertility, although at varying times. The country experienced a steep decline in TFR between 1980 and the early 1990s, followed by a fertility stall between 1996 and 2000. The TFR again began to decline continuously in 2000 without any evidence of a further stall in fertility. Thus, our findings contradict previous studies (Khuda & Barkat, Citation2012; Rahman, Citation2018), showing a different trend in TFR estimated directly from BDHS reports of individual rounds without adjustment of data across rounds. It is important to note that our reconstructed and consistent cohort data show an even smoother, almost linear decline in fertility among cohorts born around 1945 to around 1965. Even the education-specific cohort trends are almost linear, although at different levels. There is also no sign of stalls in the cohort fertility trends.
We performed simple trend analysis to see how fertility patterns were associated with women’s educational attainment, the use of contraceptives, and family planning indicators (visits by FPFWs, support for family planning from satellite clinics, family planning messages in mass media). Although uneducated women experienced the sharpest decline in fertility, family planning programme indicators over the same period either declined or remained at an already low level. In other words, the reduction in family planning programme indicators did not seem to lead to a corresponding stall in the decline in fertility. For instance, the percentage of women visited by FPFWs was relatively high (33–40 per cent) in 1993–1996 during the stall in period fertility, whereas it was much lower (13–20 per cent) after 2000 when there was a continued decline in fertility. Similarly, the decline in media exposure to family planning after 2007 did not lead to a corresponding stagnation in the decline in fertility. However, there was a massive improvement in the educational attainment of reproductive age between 1994 and 2014. This simple descriptive analysis of temporal changes in the aggregate level of fertility and different available family planning indicators suggests no prominent association that would imply that family planning efforts could be considered a significant driver of the decline in fertility. In contrast, a comparison of aggregate-level trends in the educational attainment of women of reproductive age and fertility suggests a strong association.
The results of multilevel regression analysis provide a much stronger and more weighty confirmation of the finding that the education of females is the most significant driver of the decline in fertility than the family planning indicators. The proportion of educated women in the community affected the decline of fertility in other education groups. This implies a diffusion effect in which women with lower education living in communities with a higher average education learn from the more educated women or are influenced by the local environment and cultural atmosphere in that community. This effect cannot be a function of the differential availability of family planning efforts in different communities because it was explicitly controlled for. Over time, this diffusion effect can also contribute to the declining trend in the fertility of less educated women. Also, the pathways analysis approach revealed that women’s education would more significantly affect the decline in fertility desires than the family planning and empowering indicators in Bangladesh.
Among the other explanatory variables considered in the model, other religion and living in an urban area were associated significantly with lower fertility. Concerning the wealth index, these results contribute to another on-going debate over the drivers of the decline in fertility, namely, whether income or education is more relevant (Colleran & Snopkowski, Citation2018). In the model applied to women of all ages (15–49), the wealth index was statistically related to lower fertility.
One advantage of our study compared to others on specific regions of Bangladesh is that we addressed the role of education in reducing fertility using data from all rounds of the BDHS. Because the BDHS is a nationally representative survey, our findings represent the entire country. But, although we reconstructed birth histories for different cohorts, these cross-sectional data cannot directly establish causality. To do this, a proper longitudinal survey using a case–control study design to evaluate the roles of education and family planning programmes would be more appropriate. This type of study could help separate out the effects of education and family planning on contraceptive use or age at marriage, which affect fertility outcomes. However, such a study design requires great effort and resources and could be on the agenda for future research.
In conclusion, this study’s findings indicate that the education of women was the driving factor behind the significant decline of fertility in Bangladesh from the 1980s (TFR above 6.0) to 2014 (TFR around 2.2). Urbanisation and higher household wealth were also associated with a lower number of births in the past 5 years. Regarding the family planning indicators for which data were available and considered in this study, neither a descriptive analysis of trends nor multilevel statistical analysis found significant effects. This does not necessarily imply that earlier studies focusing on specific regions or the very early phases of the decline in fertility, such as Carty et al., (Citation1993) or Cleland et al., (Citation1994), who found strong effects of family planning, were wrong. But for the overall picture of entire period from the 1980s to today, there is no indication of a significant role of government family planning efforts in the remarkable decline of fertility in Bangladesh. The statistical analyses presented here all point to increasing female education as the key driver of fertility decline.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Amin, R., Choudhuri, S. R., Mariam, A. G., & McCarthy, J. (1987). Family planning in Bangladesh, 1969-1983. International Family Planning Perspectives, 13(1), 16–20. https://doi.org/10.2307/2948103
- Amin, R., Hill, R. B., & Li, Y. (1995). Poor women's participation in credit-based self-employment: TheImpact on their empowerment, fertility, contraceptive Use, and FertilityDesire in rural bangladesh. The Pakistan Development Review, 34(2), 93–119. https://EconPapers.repec.org/RePEc:pid:journl:v:34:y:1995:i:2:p:93-119. https://doi.org/10.30541/v34i2pp.93-119
- Amin, R., Mariam, A. G., & Faruqee, R. (1985). Fertility contraceptive use and socioeconomic context in Bangladesh. Demography India, 14(1), 1–16.
- Amin, S., Basu, A. M., & Stephenson, R. (2002). Spatial variation in contraceptive use in Bangladesh: Looking beyond the borders. Demography, 39(2), 251–267. https://doi.org/10.1353/dem.2002.0014
- Amin, S., Cleland, J., Phillips, J. F., & Kamal, G. M. (1995). Socioeconomic change and the demand for children in rural Bangladesh. Research Division Working Paper, No. 70, The Population Council, New York.
- Amin, S., Diamond, I., & Steele, F. (1996). Contraception and religious practice in Bangladesh. In G. W. Jones, R. M. Douglas, J. C. Caldwell, & R. M. D’Souza (Eds.), The continuing Demographic transition (pp. 268–289). Clarendon Press.
- Angeles, G., Guilkey, D. K., & Mroz, T. A. (2005). The effects of education and family planning programs on fertility in Indonesia. Economic Development and Cultural Change, 54(1), 165–201. https://doi.org/10.1086/431261
- Arends-Kuenning, M. (2001). How do family planning workers’ visits affect women’s contraceptive behavior in Bangladesh? Demography, 38(4), 481–496. https://doi.org/10.1353/dem.2001.0032
- Arthur, W. B., & McNicoll, G. (1978). An analytical survey of population and development in Bangladesh. Population and Development Review, 4(1), 23–80. https://doi.org/10.2307/1972147
- Basu, A. M. (2002). Why does education lead to lower fertility? A critical review of some of the possibilities. World Development, 30(10), 1779–1790. https://doi.org/10.1016/S0305-750X(02)00072-4
- Basu, A. M., & Amin, S. (2000). Conditioning factors for fertility decline in bengal: History, language identity, and openness to innovations. Population and Development Review, 26(4), 761–794. https://doi.org/10.1111/j.1728-4457.2000.00761.x
- Bongaarts, J. (2010). The causes of educational differences in fertility in Sub-saharan Africa. Vienna Yearbook of Population Research, 8, 31–50. https://www.jstor.org/stable/23025509. https://doi.org/10.1553/populationyearbook2010s31
- Bongaarts, J. (2017). Africa’s unique fertility transition. Population and Development Review, 43(S1), 39–58. https://doi.org/10.1111/j.1728-4457.2016.00164.x
- Bongaarts, J., & O’Neill, B. C. (2018). Global warming policy: Is population left out in the cold? Science, 361(6403), 650–652. https://doi.org/10.1126/science.aat8680
- Cain, M. (1981). Risk and insurance: Perspectives on fertility and agrarian change in India and Bangladesh. Population and Development Review, 7(3), 435–474. https://doi.org/10.2307/1972559
- Cain, M. (1983). Fertility as an adjustment to risk. Population and Development Review, 9(4), 688–702. https://doi.org/10.2307/1973546
- Caldwell, B., & Khuda, B. E. (2000). The first generation to control family size: A microstudy of the causes of fertility decline in a rural area of Bangladesh. Studies in Family Planning, 31(3), 239–251. https://doi.org/10.1111/j.1728-4465.2000.00239.x
- Caldwell, J. C., Khuda, B. E., Caldwell, B., Pieris, I., & Caldwell, P. (1999). The Bangladesh fertility decline: An interpretation. Population and Development Review, 25(1), 67–84. https://doi.org/10.1111/j.1728-4457.1999.00067.x
- Carty, W. P., Yinger, N. V., & Rosov, A. (1993). Success in a challenging environment: Fertility decline in Bangladesh. Population Reference Bureau.
- Cleland, J. (2002). Education and future fertility trends, with special reference to mid-transitional countries. Completing the Fertility Transition, 26(4), 187–202. Available at: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/unpd_egm_200203_backgroundpaper_education_and_future_fertility_trends_cleland.pdf
- Cleland, J., Kamal, N., & Sloggett, A. (1996). Links between fertility regulation and the schooling and autonomy of women in Bangladesh. In R. Jeffrey & A. M. Basu (Eds.), Girls’ schooling, women's autonomy and fertility change in South Asia (pp. 218–234). Sage Publications.
- Cleland, J., Phillips, J. F., Amin, S., & Kamal, G. M. (1994). The determinants of reproductive change in Bangladesh: Success in a challenging environment (No. 13232) (p. 1). Washington, D.C.: The World Bank. http://documents.worldbank.org/curated/en/991321468768584526/The-determinants-of-reproductive-change-in-Bangladesh-success-in-a-challenging-environment Accessed 28 November 2019.
- Coale, A. (1973). The Demographic transition reconsidered (Vol. 1, pp. 53–72). Presented at the International Population conference, Liege, Liege: International union for the scientific study of Population.
- Colleran, H., & Snopkowski, K. (2018). Variation in wealth and educational drivers of fertility decline across 45 countries. Population Ecology, 60(1), 155–169. https://doi.org/10.1007/s10144-018-0626-5
- Das, P., Husain, Z., & Ghosh, S. (2020). Fertility behaviour in linguistic zones: Revisiting the diffusion hypothesis in greater bengal. Asian Population Studies, 16(1), 34–60. https://doi.org/10.1080/17441730.2019.1706300
- Demeny, P. (1975). Observations on population policy and population program in Bangladesh. Population and Development Review, 1(2), 307–321. https://doi.org/10.2307/1972227
- Erfani, A., & McQuillan, K. (2008). Rapid fertility decline in Iran: Analysis of intermediate variables. Journal of Biosocial Science, 40(3), 459–478. https://doi.org/10.1017/S002193200700243X
- Gertler, P. J., & Molyneaux, J. W. (1994). How economic development and family planning programs combined to reduce Indonesian fertility. Demography, 31(1), 33–63. https://doi.org/10.2307/2061907
- Hahn, Y., Islam, A., Nuzhat, K., Smyth, R., & Yang, H.-S. (2018). Education, marriage, and fertility: Long-term evidence from a female stipend program in Bangladesh. Economic Development and Cultural Change, 66(2), 383–415. https://doi.org/10.1086/694930
- Heath, R., & Mobarak, A. M. (2015). Manufacturing growth and the lives of Bangladeshi women. Journal of Development Economics, 115, 1–15. doi:10.1016/j.jdeveco.2015.01.006
- Hoque, M. N., & Murdock, S. H. (1997). Socioeconomic development, status of women, family planning, and fertility in Bangladesh: A district level analysis. Biodemography and Social Biology, 44(3-4), 179–197. https://doi.org/10.1080/19485565.1997.9988946
- Islam, A. Z., Mondal, M. N. I., Khatun, M. L., Rahman, M. M., Islam, M. R., Mostofa, M. G., & Hoque, M. N. (2016). Prevalence and determinants of contraceptive use among employed and unemployed women in Bangladesh. International Journal of MCH and AIDS (IJMA), 5(2), 92–102. https://doi.org/10.21106/ijma.83
- Islam, M. M., Islam, M. K., Hasan, M. S., & Hossain, M. B. (2017). Adolescent motherhood in Bangladesh: Trends and determinants. PLOS ONE, 12(11), e0188294. https://doi.org/10.1371/journal.pone.0188294
- Jejeebhoy, S. J. (1996). Women’s education, autonomy, and reproductive behaviour: Experience from developing countries. Oxford University Press.
- Joshi, S., & Schultz, T. P. (2013). Family planning and women’s and children’s health: Long-term consequences of an outreach program in matlab, Bangladesh. Demography, 50(1), 149–180. https://doi.org/10.1007/s13524-012-0172-2
- Kamal, N., & Sloggett, A. (1996). The effect of female family planning workers on the use of modern contraception in Bangladesh. Asia-Pacific Population Journal, 11(3), 1–7. https://doi.org/10.18356/15f50b99-en
- Khuda, B. E. (1978). Labor utilisation in a village economy in Bangladesh (Doctoral dissertation). The Australian National University, Canberra.
- Khuda, B.E., & Barkat, S. (2012). The Bangladesh family planning programme: Achievements, gaps and the way forward. In: Zaman, W, Masin, H, Loftus, J (Eds.), Family planning in Asia and the pacific: Addressing the challenges (pp. 103–125). International Council on Management of Population Programs/ UNFPA.
- Khuda, B. E., Haque, M. R., Hasan, M. S., Alam, N., & Barkat, S. (2018). Fertility preferences in Bangladesh. In S. Giettel-Basten, J. Casterline, & M. K. Choe (Eds.), Family Demography in Asia: A comparative analysis of fertility preferences (pp. 30–51). Edward Elgar Publishing Limited. https://www.elgaronline.com /view/ edcoll/978178 5363542/9781785363542.00008.xml. Accessed 28 November 2019.
- Khuda, B. E., & Hossain, M. B. (1996). Fertility decline in Bangladesh: Toward an understanding of major causes. Health Transition Review, Supplement 6, 155–167. https://www.jstor.org/stable/40652257
- Khuda, B. E., Roy, N. C., & Rahman, D. M. (2000). Family planning and fertility in Bangladesh. Asia-Pacific Population Journal, 15(1), 41–54. https://doi.org/10.18356/ca8a551b-en
- Koenig, M. A., Phillips, J. F., Simmons, R. S., & Khan, M. A. (1987). Trends in family size preferences and contraceptive use in matlab, Bangladesh. Studies in Family Planning, 18(3), 117–127. https://doi.org/10.2307/1966807
- Kravdal, Ø. (2002). Education and fertility in sub-saharan Africa: Individual and community effects. Demography, 39(2), 233–250. https://doi.org/10.1353/dem.2002.0017
- Lutz, W. (2014). A population policy rationale for the twenty-first century. Population and Development Review, 40(3), 527–544. https://doi.org/10.1111/j.1728-4457.2014.00696.x
- Lutz, W., & Skirbekk, V. (2013). How Education Drives Demography and Knowledge Informs Projections (IIASA Interim Report No. IR-13-016). Laxenburg, Austria: IIASA. http://pure.iiasa.ac.at/id/eprint/10744/. Accessed 28 November 2019
- Martin, T. C., & Juarez, F. (1995). The impact of women’s education on fertility in latin america: Searching for explanations. International Family Planning Perspectives, 21(2), 52–80. https://doi.org/10.2307/2133523
- Rahman, M. M. (2018). Fertility stalls in Bangladesh (Doctoral dissertation). University of Otago, Otago. https://otago.ourarchive.ac.nz/handle/10523/8337.
- Schoumaker, B. (2013). A Stata module for computing fertility rates and TFRs from birth histories: tfr2. Demographic Research, 28, 1093–1144. https://www.jstor.org/stable/26349981. https://doi.org/10.4054/DemRes.2013.28.38
- Schoumaker, B. (2014). Quality and consistency of DHS fertility estimates, 1990 to 2012 (DHS Methodological Reports No. 12). Rockville, Maryland, USA: ICF International.
- Schuler, S. R., Hashemi, S. M., & Jenkins, A. H. (1995). Bangladesh’s family planning success story: A gender perspective. International Family Planning Perspectives, 21(4), 132–166. https://doi.org/10.2307/2133319
- Schuler, S. R., Hashemi, S. M., & Riley, A. P. (1997). The influence of women’s changing roles and status in Bangladesh’s fertility transition: Evidence from a study of credit programs and contraceptive use. World Development, 25(4), 563–575. https://doi.org/10.1016/S0305-750X(96)00119-2
- Schultz, T. P. (2009). How does family planning promote development? Evidence from a social experiment in matlab, Bangladesh, 1977-1996. Yale University, Economic Growth Center.
- Sinha, N. (2005). Fertility, child work, and schooling consequences of family planning programs: Evidence from an experiment in rural Bangladesh. Economic Development and Cultural Change, 54(1), 97–128. https://doi.org/10.1086/431259
- The World Bank. (2019). Fertility rate, total (births per woman) - Bangladesh. https://data worldbank.org/indicator/SP.DYN.TFRT.IN?locations = BD.
- United Nations. (2019). World Population prospects 2019, online edition. United Nations, Department of Economic and Social Affairs, Population Division. https://population.un.org/ wpp/Download/Standard/Fertility/.
- van de Walle, E. (1992). Fertility transition, conscious choice, and numeracy. Demography, 29(4), 487–502. https://doi.org/10.2307/2061848
- Wittgenstein Centre. (2018). Wittgenstein Centre Data Explorer Version 2.0 (Beta). Vienna, Austria: Wittgenstein Centre for Demography and Global Human Capital (Univ.Vienna, IIASA, VID/OeAW). http://www.wittgensteincentre.org/dataexplorer.
Appendix 1
Cumulative total fertility rates by survey year and 5-year birth cohort for women with no formal education
Appendix 2. Sensitivity test: The differential impact of community education on fertility by individual education.