

ABSTRACT
Introduction
Obesity is a chronic, multifactorial condition with devastating health consequences. It was thought that obesity could be controlled with discipline and lifestyle changes, but we now know that the underlying pathophysiology is a dysregulation of the body’s energy balance system, controlled by a complex interplay of neural, hormonal, and metabolic pathways. Recognizing obesity as a chronic disease places a greater responsibility on all health care professionals to screen and identify patients at risk and develop long-term tailored treatment plans.
Areas covered
This narrative review describes the central and peripheral pathways regulating obesity, the factors contributing to its development and how to effectively manage this disease.
Expert opinion
Obesity is a disease with pathophysiologic mechanisms and should be treated accordingly to reduce the significant risk of morbidity and mortality. Lifestyle interventions remain the cornerstones of treatment; however, these measures alone are rarely enough for long-term maintenance of weight loss. Additional interventions, such as pharmacotherapy or bariatric surgery, are indicated for many patients and should be recommended. Treatment considerations should include assessment of comorbidities or risk factors, as many anti-obesity agents and bariatric surgeries also have beneficial effects on other weight-associated comorbidities.
Plain language summary: This plain language summary highlights information from a recent scientific article about obesity. Obesity is a disease that leads to excess accumulation of body fat that may negatively affect health. People can check if they have obesity by measuring their body mass index (BMI for short). The BMI is a screening tool to see if you are at risk of obesity. Obesity is defined as a BMI of 30 kg/m2 or higher with lower cut-offs in Asian populations. Obesity is a chronic health condition that leads to a shorter life span. People with obesity have a higher chance of having other health conditions, such as type 2 diabetes, fatty liver disease, heart disease, kidney problems, osteoarthritis, and some types of cancer. It can be hard for people with obesity to lose weight for various reasons. The aim of this article is to help doctors who treat people with obesity understand more about the causes for obesity, as well as the available treatment options, which include lifestyle changes, medicines, and for some people, weight loss surgery.

© 2021 Boehringer Ingelheim. Published by Informa UK Limited, trading as Taylor & Francis Group.
Article highlights
Obesity is a chronic disease with serious health consequences.
Its underlying pathophysiology is a dysregulation of the body’s energy balance system, which is controlled by a complex interplay of neural, hormonal, and metabolic pathways.
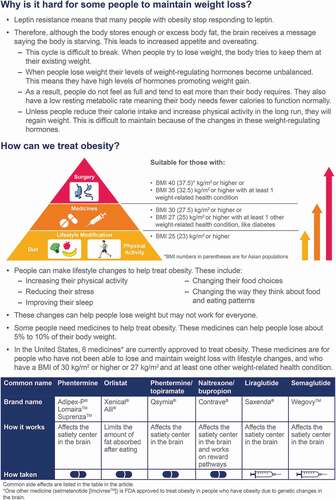
Lifestyle interventions remain the cornerstones of treatment; however, these measures alone are rarely enough for the long-term management of obesity.
Appropriate interventions, such as pharmacotherapy or bariatric surgery, are indicated for many patients and should be recommended.
Treatment considerations should include assessment of comorbidities or risk factors, as many anti-obesity agents and bariatric surgeries also have beneficial effects on weight-associated comorbidities.
Acknowledgments
Writing support was provided by Linda Merkel, PhD, of Elevate Medical Affairs, Envision Pharma Group Ltd, which was contracted and compensated by Boehringer Ingelheim Pharmaceuticals, Inc. (BIPI) for this service. BIPI was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations.
Financial and competing interests disclosure
RB Kumar is a speaker for Novo Nordisk and Janssen Pharmaceuticals, a consultant to Gelesis; and reports holding shares of Vivus, Myos Corp, and Zafgen. LJ Aronne reports receiving consulting fees from and/or serving on advisory boards for Jamieson Laboratories, Pfizer, Novo Nordisk, Eisai, Real Appeal, Janssen, and Gelesis; receiving research funding from Aspire Bariatrics, Allurion, Eisai, AstraZeneca, Gelesis, Janssen, and Novo Nordisk; having equity interests in BMIQ, ERX, Zafgen, Gelesis, MYOS, and Jamieson Laboratories; and serving on a board of directors for BMIQ, MYOS, and Jamieson Laboratories. G Srivastava reports advisory fees from RHYTHM and Novo Nordisk. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.