
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background
This study investigated the impact of the High Intensity Interval Resistance Training (HIIRT) protocol on hormonal changes in older women.
Research design and methods
Forty sarcopenic women were divided into an experimental group (EX = 30) and a control group (C = 10). The EX-group was further divided into Maintenance Training 1 (MT1 = 10), Maintenance Training 2 (MT2 = 10), and Detraining (DT = 10). The participants underwent 8 weeks of resistance training, consisting of hypertrophy and strength cycles. Following this, the EX-group had a 4-week period with no exercise or a reduced training volume. Measurements were taken at three time points.
Results
After 8 weeks, the EX-group showed significant improvements in Insulin Like Growth Factor-1 (IGF-1), Myostatin (MSTN), Follistatin (Fstn), Growth Hormone (GH) and Cortisol (Cort) compared to the control group. During the volume reduction period, there were no significant differences between MT1 and MT2 groups, but both groups saw increases in IGF-1, Fstn, GH, and decreases in MSTN and Cort compared to the DT group.
Conclusions
These findings suggest that performing at least one training session per week with the HIIRT protocol is crucial for maintaining hormonal adaptations in sarcopenic older women.
1. Introduction
As individuals age, preserving their health and skeletal muscle mass and function becomes crucial for improving their quality of life and increasing their life expectancy [Citation1]. This is because muscles play a vital role in metabolic health and protein metabolism [Citation2]. Disturbance in muscle homeostasis can lead to pathological conditions such as chronic inflammation, progressive reduction of muscle mass and function (sarcopenia) [Citation3], which is accepted as one of the syndromes of aging and a significant public health concern. Sarcopenia can cause functional decline, physical disability, falls, increased hospitalization and health care costs, poor quality of life, and even death [Citation4]. Therefore, maintaining muscle mass, performance, and strength is essential. Recent research has demonstrated that muscle strength reduction and myofibrillar protein loss are associated with the risk of functional disability, highlighting the importance of improving muscle strength and tissue for maintaining health [Citation5]. With aging, some anabolic factors, including serum insulin like growth factor-1 (IGF-1), Follistatin (Fstn) and Growth Hormone (GH) decrease, while some catabolic factors, including serum myostatin (MSTN) and Cortisol (Cort) increase. These factors are crucial biomarkers in diagnosing sarcopenia [Citation6,Citation7] Hence, providing strategies to prevent or manage sarcopenia can significantly impact improving the quality of life of older individuals. Historically, physical activity has been shown to be an effective, cost-free medicine for managing and treating multiple diseases [Citation8]. Various studies indicate that resistance exercises can have the greatest impact on improving the quality of life and muscles of the older [Citation8,Citation9]. Although resistance training is safe and easy, these exercises can lead to an increase in muscle mass due to increased muscle protein synthesis, activation and proliferation of satellite cells, production of anabolic hormones, and decreased activity of catabolic hormones [Citation10–15]. However, resistance training protocols for dramatic effects are still improving, and one of the rest-pause training protocols is an advanced technique that can provide optimal anabolic conditions for increasing muscle hypertrophy and strength, as well as increasing aerobic capacity [Citation16]. However, maintaining the gains from training, such as hypertrophy and strength, remains a challenge. According to research results, less than a fifth of people continue their training after a period of supervised resistance training, and a significant reduction in training volume or complete cessation of training causes the reversibility of adaptations and a decrease in muscle mass and strength [Citation17]. Therefore, reducing the volume and resistance training sessions to maintain the adaptations obtained in the strength and muscle mass of older individuals is crucial. The rest-pause technique or the High Intensity Interval Resistance Training (HIIRT) protocol is an advanced training technique performed with high intensity and load for a short period of time, which can be efficient in terms of time and create similar or greater adaptations in a shorter period of time compared to traditional exercises [Citation18]. However, research on the effect of this method on muscle adaptations is limited, and further investigation is necessary. The aim of this study was to compare two maintenance exercise protocols followed by the HIIRT protocol on the serum levels of IGF-1, MSTN, Fstn, GH, and Cort in sarcopenic older individuals. Therefore, this research aimed not only to investigate the effect of a high-intensity resistance training period on factors related to skeletal muscles but also to prescribe an appropriate training dose to maintain the benefits of this training period.
2. Methods
2.1. Study design
We conducted a randomized controlled trial (RCT) of a one-month HIIRT intervention in older community-dwelling women with sarcopenia. The study was approved by the Research Ethics Committee of the Faculty of Rehabilitation Sciences of Anonymized, with the ethics code IR.SUMS.REHAB.REC.1399.013, and was conducted in accordance with the principles of the Declaration of Helsinki. Before commencing the training course, all participants provided written informed consent, and were aware of and agreed to the study’s terms and conditions. Also, this study has a clinical trial number Anonymized, which was registered on 4 April 2021.
Inclusion criteria were: Women aged over 60 years who met the guidelines of the European Research Group for sarcopenia, which was defined as a decrease in muscle mass (ASMI less than 6.76 kg/m2) and poor physical performance (grip strength less than 20 kg and gait speed less than 0.8 m/s) [Citation19]. Exclusion criteria were: A life expectancy of fewer than six months, any muscle abnormalities or problems, a history of knee or hip surgery, Alzheimer’s disease, Parkinson’s disease, chronic diseases such as shortness of breath, kidney disease, heart disease, and uncontrolled diabetes. Subjects who had been treated with any testosterone or estrogen hormones or other pharmacological interventions and drugs affecting the neuromuscular and endocrine system were also excluded. To ensure that the subjects could participate in the exercise plan, they completed the physical activity questionnaire of Reading. Overall, our study aimed to investigate the effects of a one-month HIIRT intervention on muscle-related biomarkers in sarcopenic older women. The study design was rigorous, and we ensured that all participants met specific inclusion and exclusion criteria. We believe that the results of this study could provide valuable insights into the efficacy of HIIRT as a potential intervention for sarcopenia in older women, which could have important implications for improving their quality of life.
2.2. Participants and sample size
One hundred older women who attended the older center in Shiraz were initially recruited for the study. However, after applying the inclusion and exclusion criteria, 50 women between the ages of 60 and 70 who had sarcopenia, with decreased muscle mass and reduced physical performance, were identified as eligible participants. The sample size was determined using G*Power 3.1.2 software, with consideration of a 95% confidence level, an alpha level of 0.05, a power of 80%, and an attrition rate of 10%. Eventually, a final sample size of 40 participants was determined, with 10 individuals assigned to each group [Citation19].
2.3. Randomization
Participants in the study were assigned a unique identification number and randomized using a computer-based block randomization method to ensure unbiased group assignment. The sequence of randomization was generated by an expert and provided to the project manager to maintain confidentiality. The principal investigator then informed the participants of their assigned treatment session schedule, which was determined by the independent randomization center. Finally, the participants were divided into four groups: Control group (N = 10, C), Detraining group (N = 10, DT), Maintenance Training 1 group (N = 10, MT1), and Maintenance Training 2 group (N = 10, MT2).
2.4. Diet control
To prevent any confounding factors in the training protocol, the participants’ diet was closely monitored and controlled throughout the study using Three Day Food Diary Record in three stages (week 0, week 8 and week 12), and no changes were made to their dietary patterns. The subjects’ diet was evaluated and analyzed using a specialized program, Nutritionist Pro (Axxya system, Stafford, TX), to ensure uniformity in their dietary intake throughout the study period. Participants were instructed to accurately record the amount of protein and all food and liquids they consumed, and were asked to maintain their regular dietary habits during the study period without making any changes.
2.5. Assessment of body composition and determination of sarcopenic individuals
In this study, skeletal muscle mass was measured using bioelectrical impedance analysis (BIA) with the InBody 470 device (manufactured in Tokyo, Japan). BIA was chosen due to its ease of measurement, reasonable cost, speed, non-invasiveness, lack of radiation exposure, safety, and reliability, as well as its strong correlation with DEXA and MRI methods. The analysis was performed by experienced sports science experts, with participants standing on a special platform wearing minimal clothing, without shoes, socks, or any metallic objects, and without moving during the scan, which took approximately 60 seconds. The soles of both feet were placed on electrode sensors, and two electrode sensors were attached to both hands. The instrument measured 20 repetitions ranging from KH1 to KH1000. Skeletal muscle mass of the limbs (ASM) was evaluated by summing the muscle mass of both arms and legs. The ASM index (ASMI) was then calculated by dividing the ASM by the square of the participant’s height in kilograms per square meter [Citation19,Citation20]. Muscle mass analysis was performed according to the guidelines of the European Working Group on Sarcopenia in Older People (EWGSOP) [Citation21].
2.6. Determining exercise intensity
Before starting the training protocol, the subjects performed one-Repetition Maximum (1RM) test with different exercises that used in the training protocol. It’s involved the following steps: prior to the test, the subjects performed a warm-up using the minimum weight of their preference (using very light weights). Subsequently, they selected a weight based on their estimation that allowed them to complete 10 repetitions correctly and fully. The calculation of the subjects’ 1RM was done by inputting the weight used and the number of repetitions into the Brzezinski formula as follows [Citation22]:
2.7. Exercise protocol
2.7.1. Stage one (mesocycle 1 (basic physical fitness/muscle endurance phase))
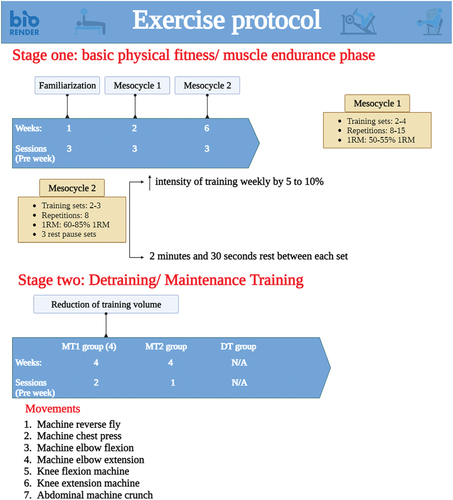
Initially, a familiarization week comprising of three training sessions was implemented. Subsequently, the first mesocycle commenced, lasting for two weeks and consisting of six sessions (three sessions per week). The objective of this mesocycle was to establish fundamental physical fitness, muscle endurance, and hypertrophy. During this mesocycle, the training sets ranged from 2 to 4, with repetitions varying between 8 and 15, using a load of 50 to 55% of the 1RM. Each session encompassed seven exercises (All the exercises were done with the machine) targeting the major muscle groups of the whole body, Included: machine reverse fly, machine chest press, machine elbow flexion and extension, knee flexion and extension machine, and abdominal machine crunch. Essentially, this mesocycle focused on hypertrophy and muscle endurance, aiming to initiate muscle growth and develop basic physical fitness for participation in the HIIRT protocol. The total training duration, including warm-up and cool-down, ranged from 30 to 40 minutes per session (See ).
Figure 1. Schematic figure of stage 1 and 2.
2.7.2. Mesocycle 2 (HIIRT protocol)
After completing mesocycle 1, the participants progressed to mesocycle 2, which involved training three days a week for six weeks. Each training session in this mesocycle lasted for 35 minutes, including five minutes of warm-up and five minutes of cool-down. Each training session consisted of 2 to 3 sets of 8 repetitions. This mesocycle incorporated three rest-pause sets. Rest-pause is a high-intensity training method. Each set performed using this technique comprised of 4 to 6 repetitions, with a 20-second recovery period, followed by 2 repetitions performed to fatigue, another 20-second recovery, and finally, 1 or 2 repetitions performed to failure. A rest period of 2 minutes and 30 seconds was provided between sets. The exercises were executed at an intensity level of 60–85% of the 1RM, and the workload increased by 5–10% on a weekly basis, in accordance with the subjects’ ability and the principle of overload. Further details on the reasons and benefits of using this exercise protocol for older individuals can be found elsewhere [Citation21].
2.7.2.1. Stage two/detraining/maintenance training
The entire study period consisted of a three-stage schedule that included the first mesocycle (hypertrophy), the second mesocycle (strength), and the third mesocycle (reduction of training volume). During the period of reducing the training volume (maintenance protocol), the MT1 group performed exercises for four weeks with half the volume of the first stage protocol, i.e. the HIIRT protocol (reducing the number of days to two days per week and reducing the training sets to one session of one set and one session of two sets). The MT2 group performed exercises for four weeks with a volume of one third of the HIIRT protocol (reducing the number of days to one day per week and reducing the training sets to one session of two sets). During this period, the DT group did not participate in any exercise program and continued their normal daily activities. Group C only engaged in normal daily activities until the end of the study.
2.7.3. How to determine the training volume in the maintenance protocol
The training volume was determined by calculating the sum of the total number of repetitions, sets, sessions, and training movements, and then multiplying the number of sets by the number of repetitions. For the maintenance training group, a 50% reduction in volume was achieved by performing a total of 24 repetitions per week (two days a week, with one-day consisting of two sets with eight repetitions using the rest-pause technique, and the other day consisting of one set with eight repetitions using the same technique). For the MT2 group, two reductions in training volume were implemented, resulting in a 67% reduction in volume, which was equivalent to performing a total of 16 repetitions per week (one day per week, with two sets of eight repetitions using the rest-pause technique).
2.8. Blood sampling method
Blood samples were collected from the participants on three occasions (week 0, week 8, and week 12). A laboratory technician collected venous blood samples from the participants and stored them in tubes. The sampling was performed in a sitting position after at least 15 minutes of rest, between 7 am and 9 am, after a 10-hour fast and 48 hours after the last training session. A total of 10 ml of blood was drawn from the antecubital vein and placed in a tube. All samples were centrifuged for 20 minutes at 3000 rpm, and the supernatants were collected carefully and were stored at −80°C until analysis [Citation13,Citation14,Citation22]. The serum level of IGF-1 was measured using a specialized human hormone kit (E20, Mediagnost, Germany) with sensitivity of 0.091 ng/ml, and the ELISA method. The serum level of MSTN was measured using ELISA kit (E0403Hu, R&D, U.S.A.) based on the Biotin double antibody sandwich technology with sensitivity of 5.52 ng/l. Serum Fstn level was measured by ELISA kit (E1010Hu, Bioassay Technology Laboratory, U.S.A.) with sensitivity of 0.24 ng/ml., serum GH level also was measured by ELISA kit (Cat.No.DG.hGH.01, DiaZist, IRI) with sensitivity of 0.2 ng/ml. also The serum level of Cort was measured using ELISA kit (PC: 3625–300, Monobind Inc, CA 9263, U.S.A.) with sensitivity of 91.5 pg equivalent to 0.366 µg/dl. The Analysis of blood samples were carried out in the specialized laboratory of hormonology of Professor Saeb in Shiraz, Iran.
2.9. Statistical analysis
The data were analyzed using descriptive and inferential statistics. The demographic characteristics of the subjects, including age, weight, and height, as well as the research variables in the pre-test, post-test 1, and post-test 2, were expressed using descriptive statistics, such as mean and standard deviation. To examine the changes in the research variables from pre-test to post-test 1 within each group, one-way analysis of variance was used, assuming the normality of the data distribution. Additionally, to examine the changes in the research variables from post-test 1 to post-test 2 and from pre-test to post-test 2 separately for each group, the parametric test of one-way analysis of variance within the group was used, assuming the normality of the data. To facilitate the understanding of the course of changes from the beginning to the end of the study (week 0 to week 12), one-way repeated measures analysis of variance was conducted within each group, using the pre-test, post-test 1, and post-test 2 stages. The comparison of variables from pre-test to post-test 1 between the EX and C groups was performed using analysis of covariance (ANCOVA) test, assuming the normality of the data and establishing the condition of homogeneity of variances and regression slope. The pre-test values were used as covariates to increase accuracy and control the possible imbalance in the random selection process. Additionally, the effect size was calculated, and a large effect size was considered as 80%, a medium effect size as 50%, and a small effect size as 20%. To compare the four groups (MT1, MT2, DT, and C) from post-test 1 to post-test 2, one-way analysis of variance with Tukey’s post hoc test for pairwise comparisons was used, assuming the normality of the data. To remove the effect of possible differences between groups in post-test 1 (which was considered as a pre-test for post-test 2 at this stage), the difference in scores was calculated, and then the average scores were compared. All analyses were conducted using SPSS version 23 statistical software, and a significance level of 0.05 was used.
3. Results
displays the basic characteristics and sarcopenia indices of the studied groups at week 0, and no significant differences were observed between the groups. The results indicated that IGF-1 levels increased significantly in the MT1 group (f [Citation1,Citation9] = 7.20; p = 0.02; η2 = 0.44), but not in the MT2 group. Therefore, during the maintenance period, at least two training sessions per week with the HIIRT protocol are required to maintain these adaptations (). In the DT group, a significant decrease was observed after four weeks of training cessation (f [Citation1,Citation9] = 12.70; p = 0.006; η2 = 0.58), but IGF-1 levels remained higher than the baseline. Conversely, a significant decrease was observed in group C from weeks 8 to 12 (f [Citation1,Citation9] = 6.62; p = 0.03; η2 = 0.42), and the levels were lower than the baseline ().
Table 1. Baseline characteristics and sarcopenia index of each group (mean ± SD)*.
Table 2. Basal serum hormone concentrations at weeks 0, 8, and 12 (mean ± SD).
Table 3. Basal serum hormone concentrations at weeks 0, 8, and 12 (mean ± SD).
The results indicated that MSTN levels decreased significantly in the MT1 group (f [Citation1,Citation9] = 17.76; p = 0.002; η2 = 0.66). The MT2 group’s results indicated that during the retention period of one HIIRT protocol session, it is not sufficient to maintain the adaptations resulting from the training. Therefore, during the maintenance period, at least two training sessions per week with the HIIRT protocol are required to maintain these adaptations (). The DT group showed a non-significant increase in MSTN levels after four weeks of training cessation, while group C exhibited a significant increase compared to the baseline state (f [Citation1,Citation9] = 7.38; p = 0.02; η2 = 0.45) ().
The results indicated that Fstn levels increased significantly in the MT1 group (f [Citation1,Citation9] = 21.96; p = 0.001; η2 = 0.70). However, the increase in Fstn levels in the MT2 group was not significant. Therefore, during the maintenance period, at least two training sessions per week with the HIIRT protocol are required to maintain these adaptations (). Fstn levels significantly decreased after four weeks of training cessation in the DT group (f [Citation1,Citation9] = 7; p = 0.02; η2 = 0.43), but remained higher than the baseline. Conversely, group C showed a significant decrease in Fstn levels and was lower than the baseline (f [Citation1,Citation9] = 6.62; p = 0.03; η2 = 0.42) ().
To compare the groups between post-test 1 and post-test 2, the difference of scores for each factor was calculated, and the difference of means was compared using a one-way analysis of variance test. This was done first to eliminate any possible differences and sort the groups in post-test 1. The results indicated a significant difference between the groups (F [Citation3,Citation23] = 8.25; p = 0.0001; η2 = 0.40). The IGF-1 levels increased in both the MT1 and MT2 groups during the maintenance training period, and there was no significant difference between the two groups (p = 0.07). Conversely, due to quitting training, IGF-1 levels decreased in the DT group, and a significant difference was observed between the MT1 and DT groups (p = 0.0001) and between the MT2 and DT groups (p = 0.005). The difference between MT1 and C was significant (p = 0.005), while there was no significant difference between MT2 and C (p = 0.23). There was no significant difference between the DT and C groups ().
Figure 2. The results of the one-way analysis of variance test, the significant comparison of the mean difference between post-test 1 and post-test 2 serum levels of MSTN (ng/L) and Fstn (ng/L) in MT1, MT2, DT, C groups. * significance of MT1 with the control group; ** significance of MT2 with the control group; *** significance of DT with the control group; $ significance of MT1 with the DT group and # significance of MT2 with the DT group.
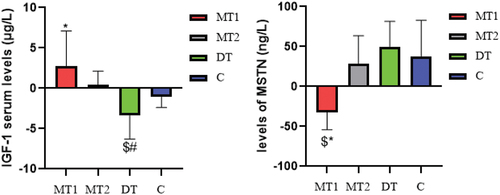
The results of comparing the mean difference between the groups showed a significant difference between the groups (F [Citation3,Citation23] = 3.77; p = 0.02; η2 = 0.23). Furthermore, MSTN levels decreased in the MT1 group but increased in the other groups.There was no significant difference between the MT1 and MT2 groups (p = 0.07), but the difference between MT1 and DT (p = 0.01) and between MT1 and C groups (p = 0.003) was significant. However, the MT2 group did not differ significantly from any of the groups. Also, there was no significant difference between the C and DT groups (). Therefore, at least two training sessions per week with the HIIRT protocol are needed to maintain the adaptations created in MSTN after a period of HIIRT protocol.
The results of comparing the average difference between the groups that there is a significant difference between the groups (F [Citation3,Citation23] = 6.95; p = 0.001; η2 = 0.36). Also, the results showed that Fstn levels increased in both MT1 and MT2 groups, but the difference between these two groups was not significant (p = 0.75), while it decreased in DT and C groups, and the difference between the two groups was not significant (p = 0.14). The difference between MT1 and DT (p = 0.0001) and also with group C (p = 0.01) was significant. Also, the difference between MT2 and DT (p = 0.001) and group C (p = 0.03) was significant ().
Figure 3. The results of the one-way analysis of variance test, the significant comparison of the mean difference between post-test 1 and post-test 2 serum levels of Fstn (ng/L) and cot (ng/L) in MT1, MT2, DT, C groups. * significance of MT1 with the control group; ** significance of MT2 with the control group; *** significance of DT with the control group; $ significance of MT1 with the DT group and # significance of MT2 with the DT group.
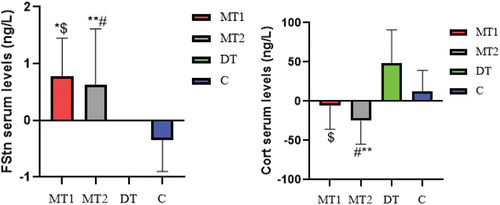
The results of comparing the mean difference of the groups showed that there is a significant difference between the groups (F [Citation3,Citation23] = 9.17; p = 0.0001; η2 = 0.43). Also, the results showed that Cort levels decreased in both MT1 and MT2 groups, but the difference between these two groups was not significant (p = 0.20). While it increased in DT and C groups and the difference between the two groups was significant (p = 0.01). The difference between MT1 and DT (p = 0.001) was significant, but not with group C (p = 0.21). The difference between MT2 group and DT (p = 0.0001) and C group (p = 0.01) was significant ().
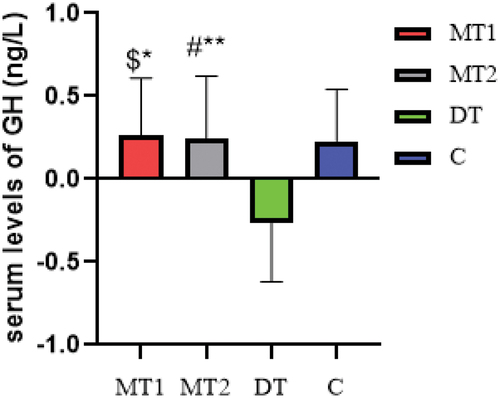
The results of comparing the average difference of the groups showed that there is a significant difference between the groups (F [Citation3,Citation23] = 6.43; p = 0.001; η2 = 0.34). Also, the results showed that GH levels increased in both MT1 and MT2 groups, but the difference between these two groups was not significant (p = 0.89). While it decreased in DT and C groups and the difference between the two groups was not significant (p = 0.84). The difference between MT1 and DT (p = 0.002) and group C (p = 0.004) was significant. Also, the difference between MT2 group and DT (p = 0.003) and C group (p = 0.006) was significant ().
Figure 4. The results of the one-way analysis of variance test, the significant comparison of the mean difference between post-test 1 and post-test 2 serum levels of HJ (ng/L) in MT1, MT2, DT, C groups. * significance of MT1 with the control group; ** significance of MT2 with the control group; *** significance of DT with the control group; $ significance of MT1 with the DT group and # significance of MT2 with the DT group.
4. Discuss
In the present study, for the first time in Iran, the changes in hormonal profile were investigated using a periodized resistant training protocol in older sarcopenic women. The findings of the current study indicated that the HIIRT protocol (phase 1) significantly affected and improved the anabolic and catabolic hormones such IGF-1, Fstn, GH, MSTN and Cort in the EX group. And in phase 2, the effectiveness of different doses of the HIIRT protocol for maintaining hormonal adaptations resulting from periodized resistance training in sarcopenic older women was investigated. The results showed that training with one-third volume (one training session, two sets of HIIRT protocol with rest-pause technique, intensity 90–100% of 1RM) compared to no training is sufficient to maintain the hormonal adaptations in sarcopenic older women. Furthermore, it was observed that periodized training with an emphasis on the use of the HIIRT protocol made the adaptations obtained in short-term training withdrawal better than the primary state, indicating the protocol’s efficiency and effectiveness for older adults.
Despite the importance of determining the minimum training dose during the maintenance period (reducing the training volume) to maintain the acquired adaptations in older adults, limited studies have been conducted on this issue. In connection with athletes, tapering is one of the accepted methods of reducing the amount of training to prepare for sports competitions, and research results show that short-term periods of reducing the amount of training from one to four weeks do not have adverse effects on the performance of athletes. However, studies on periods of volume depletion in normal and older subjects are limited [Citation24]. In a situation where a person cannot participate in all the training sessions in order to maintain the adaptations obtained after a regular training period, reducing the training volume (less than two training sessions per week) is superior to altogether leaving the training [Citation17,Citation24,Citation25]. Therefore, it is important and necessary not to give up strength training for the older. While it seems that throughout the year, periods of reduced training volume not only do not reverse the acquired adaptations but are an important practical strategy [Citation24].
IGF-1 is a growth factor that decreases with age and is one of the causes of sarcopenia. Anabolic activity of IGF-1 and GH increases in response to exercise training [Citation22]. In the present study, after eight weeks of priodized resistance training (consisting of two mesocycles of hypertrophy and HIIRT), IGF-1 increases in all intervention groups, but this increase is insignificant. While, with the continuation of training after 12 weeks (despite the application of the mesocycle to reduce the training volume), it increased by 31% (η2 = 0.44) and 6%, respectively, in the MT1 and MT2 groups. In the DT group, despite the decrease, it was 2% higher compared to the baseline condition, while in the C group, a 1% decrease was observed compared to the baseline condition. According to research results, long-term periods of resistance training increase the levels of IGF-1 in older adults, and most studies emphasize the benefits of resistance training for long-term training periods (more than 16 weeks) for the benefit of sarcopenic older [Citation7,Citation13]. However, in the present study, a significant increase in IGF-1 was observed in a shorter period (12 weeks), probably due to the specific type of protocol designed, the high intensity of the HIIRT protocol, and the use of the rest-pause technique. In line with the results of the present study, KarimiFard et al. (2023) [Citation14] reported an increase in IGF-1 following rest pause exercises in healthy young men, While Moro et al. (2020) [Citation18] stated that eight weeks of HIIRT protocol does not change IGF-1 serum levels. Probably, the reason for this lack of change and differentiation of the results with the current research depends on the age and health conditions of the Moro study subjects (healthy young men). In the present study, the HIIRT protocol was implemented for sarcopenic older adults. Considering that the basal levels of serum IGF-1 in older adults are lower than in young people [Citation26,Citation27]. and the response of this factor to resistance training protocols may also be different. In another study, Moro et al. (2017) [Citation28] reported a decrease in the serum levels of IGF-1 in older adults in response to HIIRT. The reason for this discrepancy is probably the difference in the training protocol’s type and number of sessions (2 sessions per week vs. three sessions per week) and the health status of the subjects (healthy older men and women vs. sarcopenic older women). Because basal IGF-1 levels of sarcopenic older are lower than healthy older [Citation18], this leads to differences in exercise response. Shojaei et al. (2022) [Citation29] and Nascimento et al. (2018) [Citation30] reported no significant change in IGF-1 in healthy older women in response to 12 weeks of low and moderate-intensity resistance training, respectively, which contradicts the results of the present study. Probably, the difference in the intensity of the training protocols caused the difference in the results. The amount of hormones related to muscle growth depends on the intensity and volume of exercises involving the muscles, also because high-intensity resistance training produces more anabolic hormones, including GH, than low-intensity resistance training [Citation14,Citation26]. Therefore, in the current study, the high intensity of the HIIRT protocol probably caused an increase in anabolic hormones. In addition, in the studies mentioned earlier, the lack of change in muscle mass due to low training intensity did not result in increased GH production and IGF-1 stimulation in older women [Citation28–30]. In our previous research, we have shown that the current training protocol causes muscle hypertrophy [Citation31], increases lean body mass and ASMI, and improves the health status of the subjects from the sarcopenic stage to the pre-sarcopenia stage, which is one of the valuable results of the HIIRT protocol [Citation21]; Therefore, considering that muscle growth is the result of a balance between positive regulators such as IGF-1 and negative regulators such as MSTN; Presumably, applying load on the muscles has shifted this balance toward the positive regulators of muscle growth, and the increase in IGF-1 levels can confirm this. Also, the volume and type of exercise affect the response of MSTN and Cort. Research results show that intense resistance training protocol such as HIIRT is more effective than other training protocols in increasing muscle growth mediators and hypertrophy [Citation13,Citation24,Citation30].
In the present study, GH increased significantly after eight weeks of training in all intervention groups, and during the volume reduction period, it increased by 35% (η2 = 0.82) and 35% (η2 = 0.48) in the MT1 and MT2 groups, respectively. Also, in the DT group, despite the decrease, it was 16% higher compared to the baseline state, while in the C group, it decreased by 11% compared to the baseline state. GH is an anabolic hormone whose levels decrease in the older. One of the reasons why IGF-1 does not change in response to exercise is low GH levels, especially in older women. Considering the essential role of GH in human growth and its connection with muscle recovery, scientists have been paying attention as one of the treatment methods for sarcopenia [Citation32]. Bian et al. (2020) [Citation33] also emphasized this important issue in their research that the serum concentration of GH and IGF-1 is related to sarcopenia in older adults, and the increase of GH in response to exercise can increase IGF-1. Probably, in the present study, the increase of GH in response to the high intensity of the HIIRT protocol caused the increase of IGF-1. According to the results, one training session per week can maintain the improvement obtained from the first training phase in IGF-1 and GH levels, but two training sessions per week continue the improvement process.
MSTN is one of the muscle growth inhibitors, but there is disagreement about its relationship with age-related muscle atrophy. However, many studies have shown that a high concentration of MSTN is related to muscle mass, and its serum levels increase with age. The results of the present study showed that the serum levels of MSTN in the MT1 and MT2 groups decreased by 38% (η2 = 0.66) and 8%, respectively, and in the DT group, despite the increase, it was 2% lower than the baseline state. While in group C, it increased by 18% (η2 = 0.45) compared to the baseline state. In line with the results of the present study, KarimiFard et al. (2023) [Citation14] reported the reduction of MSTN following rest pause exercises in healthy young men. Negaresh et al. (2019) [Citation22] and Mafi et al. (2018) [Citation34] have also reported an increase in Fstn and a decrease in MSTN in response to resistance training in sarcopenic older men and women, respectively. Fstn is one of the antagonists of MSTN, and one of its most important functions is binding to MSTN receptors and inhibiting them. The results of the present study showed that Fstn in the MT1 and MT2 groups increased by 20% (η2 = 0.70) and 9%, respectively, and in the DT group, despite the decrease, it was 16% higher than the baseline state. While in group C, it decreased by 10% compared to the baseline state. According to the results, at least two weekly training sessions are necessary to maintain and improve Fstn levels. It is worth mentioning that the MSTN-Fstn system is one of the therapeutic targets of sarcopenia [Citation7], and increasing Fstn through resistance training is one of the inhibitory mechanisms of MSTN and prevents muscle mass breakdown and atrophy [Citation27]. However, the response to resistance training is different, and one of the reasons for the difference in the ability to respond to hypertrophy and adaptation to resistance training is the individual differences and the age of people; Because the serum levels of MSTN in young people, healthy older and sarcopenic older are different, and the basal levels of MSTN in older adults are higher than in young people, and this, in turn, causes differences in response to exercise [Citation34,Citation35].
Cortisol is one of the important biomarkers of sarcopenia and is well-known as a catabolic factor, and its levels are increased in sarcopenic individuals. The results of the present study showed that Cort in MT1 and MT2 groups decreased by 25% (η2 = 0.58) and 38% (η2 = 0.58), respectively, and in the DT group, despite the increase, it was 1% lower than the baseline state, while in Group C increased by 5% compared to the baseline. Chronic inflammation is one of the causes of increased cortisol in the sarcopenic older [Citation7]. One of the possible reasons for the slow increase of IGF-1 in response to resistance training is the presence of chronic low-level inflammation and the creation of inflame-aging conditions due to muscle homeostasis disorders. This, in turn, causes the breakdown of muscle mass and causes sarcopenia in the older [Citation13,Citation31]. While more extended periods of activity and high-intensity exercises, such as the protocol of the present study (HIIRT), cause a more significant reduction in inflammation and glucocorticoids, including cortisol [Citation28,Citation33,Citation34], remove its inhibitory effect on the GH/IGF-1 axis and a result Increases IGF-1 [Citation7,Citation13,Citation35]. In addition, sarcopenic older women with a body fat percentage greater than 30% are considered obese, and both obesity and aging lead to inflammation [Citation36]. Walker et al. (2018) [Citation25], in the study of the effect of 2 mesocycles of 12 weeks on sarcopenic older women, stated that during the volume reduction period, the cortisol level increases and the cross-sectional area of muscle and insulin also decrease and return to the baseline levels before exercise. At the same time, the anabolic hormones evaluated in the present study increased during the volume reduction period. In the first and second phases of Walker’s research, exercises with moderate intensity (50 to 60% 1RM) were performed, but in the present study, in the first phase of the strength mesocycle with the HIIRT protocol (intensity 60 to 85% 1RM) and in the maintenance period of the mentioned protocol (intensity 90 to 100% 1RM) was used. In Walker’s research, the low activity intensity during the volume reduction period probably could not maintain adaptations because the amount of hormones related to muscle growth depends on the intensity and volume of exercises involving the muscles. Also, high-intensity resistance training produces more anabolic hormones than low-intensity resistance training [Citation14,Citation23,Citation26]. Therefore, in the present study, the high intensity of the HIIRT protocol may have caused an increase in anabolic hormones, followed by a decrease in catabolic hormones. In line with the present study, Iverson et al. (2021) [Citation37] stated that the period reducing the training volume can maintain the adaptations created in the older. Also, Tavaris et al. (2017) [Citation17] stated that the period of reducing the training volume maintains the acquired adaptations, which is probably due to the use of high-intensity strength training. However, the evaluated factors (muscle strength and cross-sectional area) and the studied group (healthy young men) differed from the present study. Therefore, it can be said that during the volume reduction period for the older, attention should be paid to the training intensity, volume, and rest between sets, because, according to the mentioned materials, if the volume reduction is significant, the acquired consistency will be lost. Nevertheless, suppose this volume reduction is appropriate, and the HIIRT protocol is used. In that case, it is likely that adaptations will be maintained and even improved due to the high intensity of the exercises. In order to maintain adaptations, the reduction of training volume during the maintenance period should be such that it can create a minimum threshold (reduction of training volume of about 50–60% of the initial training volume) to maintain muscle adaptations [Citation17,Citation23]. According to the results of the present study on sarcopenic older women, reducing the training volume by one-third (about a 67% reduction compared to the initial training volume) is the necessary threshold to maintain the morphological adaptations of the muscles. Therefore, the role of training volume in maintaining adaptations is much more important than the number of training sessions [Citation37]. Therefore, in the present study, in order to prevent the fatigue and frustration of the older toward intense exercises and not experiencing the plateau state and stopping the progression of adaptations or causing overtraining during the HIIRT protocol, the volume reduction period was also implemented with the same protocol so that overcompensation occurs without causing fatigue.
The strength of this study lies in its ability to achieve positive results within a short period of time. This achievement is likely attributed to the unique design of exercises in the HIIRT protocol, which emphasizes short rest periods and high exercise intensity. The rest-pause technique employed in this protocol is superior to traditional resistance exercises as it minimizes the time spent maintaining training volume. In this technique, the individual performs 4 to 6 repetitions followed by a 20-second recovery, then two repetitions to fatigue, another 20-second recovery, and finally 1 or 2 additional repetitions until exhaustion. This approach allows for high-intensity exercises to be performed in a concise timeframe without compromising the training volume. Consequently, this strategy not only enhances power efficiency but also saves time. Moreover, this approach leads to increased muscle activity, creating an optimal anabolic environment necessary for muscle hypertrophy. It generates the required mechanical and metabolic stimulation, resulting in changes in the secretion of myokines such as IGF-1, MSTN, and Fstn. These factors contribute to muscle growth and development.
The current study had certain limitations that should be acknowledged. Firstly, the small number of participants in each group (n = 10) limited the statistical power of the study. Future investigations should consider incorporating larger sample sizes to ensure maximal statistical power and robustness of the findings. Secondly, the study focused solely on older, sarcopenic women. To provide a more comprehensive understanding, future research should encompass investigations of older individuals with dynapenia, pre-sarcopenia, as well as healthy men and women from various clinical cohorts. This broader inclusion would allow for a more representative and diverse study population. Additionally, the present study did not involve the use of biopsies to measure hormones and their gene expression at the tissue level. To gain further insights in this area, future research should aim to include these specific measurements. This would provide a deeper understanding of the underlying mechanisms and hormonal responses associated with the interventions. Lastly, the study did not report data related to changes in muscle cross-sectional area and functional factors associated with sarcopenia. However, the authors plan to address these aspects in an upcoming article, where the relevant data will be presented. Overall, these identified limitations emphasize the need for future research to address these aspects, including larger sample sizes, diverse study populations, tissue-level analyses, and comprehensive reporting of relevant outcome measures. In terms of practical implications derived from the present investigation, the results offer a novel approach for prescribing high-intensity interval resistance training (HIIRT) in the population of sarcopenic older women. Additionally, it provides a model for periodization that has the potential to optimize both hypertrophic and neural adaptations in short-term periodized resistance training. Prescribing resistance exercise and implementing periodized resistance training using the HIIRT protocol for older women has shown improvements in the hormonal profile of sarcopenic elderly individuals. Moreover, it promotes high adherence to exercise, which is crucial for fostering a healthy lifestyle. Considering that time constraints often act as a major barrier to regular exercise and participation in physical activities, HIIRT appears to be a suitable exercise protocol. By incorporating short, intense intervals, HIIRT maximizes efficiency while still delivering the desired benefits. Furthermore, it is advisable to incorporate a volume reduction mesocycle to prevent older individuals from experiencing excessive fatigue or becoming demotivated due to intense exercises. This approach helps to avoid training plateaus, maintain progress in adaptations, and prevent the onset of overtraining. By strategically managing volume reduction, individuals can overcompensate without experiencing excessive fatigue. In summary, the findings of this study offer practical applications for the prescription of HIIRT in sarcopenic older women. This exercise modality not only improves the hormonal profile but also promotes exercise adherence, ultimately contributing to a healthy lifestyle. Additionally, incorporating volume reduction mesocycles can help prevent fatigue, training plateaus, and overtraining, ensuring continued progress and adaptation.
5. Conclusion
In general, it can be said that in the present study, 6 weeks HIIRT protocol improved hormonal adaptations and both types of maintenance protocols had positive effects on the adaptations created in the hormonal profile (IGF-1, GH, Fstn, MSTN, and Cort). Nevertheless, the greater the intensity and volume of training, the greater the anabolic stimulation due to the creation of the necessary mechanical stimulation. Therefore, creating an anabolic environment provides inhibition mechanisms for catabolic factors, including MSTN and Cort. In the MT1 group, these positive effects were more due to the larger volume of exercises. Therefore, reducing the number of sessions and exercise volume does not have a negative effect on the hormonal profile of sarcopenic older women, but in examining the volume reduction period and comparing two types of maintenance protocols with one-half and one-third volume of the initial exercise, the dose-response effect is evident; Therefore, considering the positive effects of this exercise protocol in improving sarcopenia and considering that the HIIRT is a Time efficiency and time-saving protocol, it seems that HIIRT is a suitable exercise protocol for the older during the volume reduction period.
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Reviewer disclosures
Peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Ethics statement
The study was approved by the Research Ethics Committee of the Faculty of Rehabilitation Sciences of Anonymized, with the ethics code IR.SUMS.REHAB.REC.1399.013, and was conducted in accordance with the principles of the Declaration of Helsinki
Author contribution statement
Idea, Conceptualization, visualization methodology, investigation, resources, data curation, software, validation, formal analysis, Project Administration and editing, ZA and F.D writing – original draft preparation, A.A.H, and M.A.D.
Acknowledgments
The authors wish to thank all those who participated in this research.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Additional information
Funding
References
- Janssens GE, Grevendonk L, Perez RZ, et al. Healthy aging and muscle function are positively associated with NAD+ abundance in humans. Nature Aging. 2022;2(3):254–63. doi: 10.1038/s43587-022-00174-3
- Alkhayl FFA, Ismail AD, Celis-Morales C, et al. Muscle protein synthesis and muscle/metabolic responses to resistance exercise training in South Asian and white European men. Sci Rep. 2022;12(1):2469. doi: 10.1038/s41598-022-06446-7
- Dent E, Woo J, Scott D, et al. Toward the recognition and management of sarcopenia in routine clinical care. Nat Aging. 2021;1(11):982–90. doi: 10.1038/s43587-021-00136-1
- Therakomen V, Petchlorlian A, Lakananurak N. Prevalence and risk factors of primary sarcopenia in community-dwelling outpatient elderly: a cross-sectional study. Sci Rep. 2020;10(1):19551. doi: 10.1038/s41598-020-75250-y
- Galancho-Reina I, Sanchez-Oliver AJ, Gonzalez-Matarin PJ, et al. The role of muscle tissue and resistance training in cardiometabolic health. Int J Sports Sci Med. 2019;3:1–12.
- Ko YJ, Ko I-G. Voluntary wheel running exercise improves aging-induced sarcopenia via activation of peroxisome proliferator-activated receptor gamma coactivator-1α/fibronectin type III domain-containing protein 5/adenosine monophosphate-activated protein kinase signaling pathway. Int Neurourol J. 2021;25(Suppl 1):S27.
- Ladang A, Beaudart C, Reginster J-Y, et al. Biochemical markers of musculoskeletal health and aging to be assessed in clinical trials of drugs aiming at the treatment of sarcopenia: consensus paper from an expert group meeting organized by the European society for clinical and economic aspects of osteoporosis, osteoarthritis and musculoskeletal diseases (ESCEO) and the centre Académique de Recherche et d’Expérimentation en Santé (CARES SPRL), under the auspices of the world health organization collaborating center for the epidemiology of musculoskeletal conditions and aging. Calcif Tissue Int. 2023;112(2):197–217. doi: 10.1007/s00223-022-01054-z
- Marcos-Pardo PJ, Orquin-Castrillón FJ, Gea-García GM, et al. Effects of a moderate-to-high intensity resistance circuit training on fat mass, functional capacity, muscular strength, and quality of life in elderly: a randomized controlled trial. Sci Rep. 2019;9(1):7830. doi: 10.1038/s41598-019-44329-6
- Eckardt N, Braun C, Kibele A. Instability resistance training improves working memory, processing speed and response inhibition in healthy older adults: a double-blinded randomised controlled trial. Sci Rep. 2020;10(1):2506. doi: 10.1038/s41598-020-59105-0
- Bernier M, Enamorado IN, Gómez-Cabrera MC, et al. Age-dependent impact of two exercise training regimens on genomic and metabolic remodeling in skeletal muscle and liver of male mice. Npj Aging. 2022;8(1):8. doi: 10.1038/s41514-022-00089-8
- Rodrigues F, Domingos C, Monteiro D, et al. A review on aging, sarcopenia, falls, and resistance training in community-dwelling older adults. Int J Environ Res Public Health. 2022;19(2):874. doi: 10.3390/ijerph19020874
- Enes A, Alves RC, Schoenfeld BJ, et al. Rest-pause and drop-set training elicit similar strength and hypertrophy adaptations compared with traditional sets in resistance-trained males. Appl Physiol Nutr Metab. 2021;46(11):1417–1424. doi: 10.1139/apnm-2021-0278
- Amiri N, Fathei M, Mosaferi Ziaaldini M. Effects of resistance training on muscle strength, insulin-like growth factor-1, and insulin-like growth factor–binding protein-3 in healthy elderly subjects: a systematic review and meta-analysis of randomized controlled trials. Hormones. 2021;20(2):247–257. doi: 10.1007/s42000-020-00250-6
- Karimifard M, Arazi H, Mehrabani J. Twelve weeks rest–pause and traditional resistance training: effects on myokines and performance adaptations among recreationally trained men. Stresses. 2023;3(1):302–315. doi: 10.3390/stresses3010022
- Mellen RH, Girotto OS, Marques EB, et al. Insights into pathogenesis, nutritional and drug approach in sarcopenia: a systematic review. Biomedicines. 2023;11(1):136. doi: 10.3390/biomedicines11010136
- Fielding RA. The role of progressive resistance training and nutrition in the preservation of lean body mass in the elderly. J Am Coll Nutr. 1995;14(6):587–594. doi: 10.1080/07315724.1995.10718547
- Tavares LD, de Souza EO, Ugrinowitsch C, et al. Effects of different strength training frequencies during reduced training period on strength and muscle cross-sectional area. Eur J Sport Sci. 2017;17(6):665–672. doi: 10.1080/17461391.2017.1298673
- Moro T, Marcolin G, Bianco A, et al. Effects of 6 weeks of traditional resistance training or high intensity interval resistance training on body composition, aerobic power and strength in healthy young subjects: a randomized parallel trial. Int J Environ Res Public Health. 2020;17(11):4093. doi: 10.3390/ijerph17114093
- Makizako H, Nakai Y, Tomioka K, et al. Effects of a multicomponent exercise program in physical function and muscle mass in sarcopenic/pre-sarcopenic adults. J Clin Med. 2020;9(5):1386. doi: 10.3390/jcm9051386
- Bao W, Sun Y, Zhang T, et al. Exercise programs for muscle mass, muscle strength and physical performance in older adults with sarcopenia: a systematic review and meta-analysis. Aging Dis. 2020;11(4):863. doi: 10.14336/AD.2019.1012
- Hooshmandi Z, Daryanoosh F, Nemati J, et al. Effect of high-intensity interval resistance training on appendicular skeletal muscle mass index measured by bioelectric impedance analysis in sarcopenic elderly women. Women’s Health Bulletin. 2021;8(4):211–9.
- Negaresh R, Ranjbar R, Baker JS, et al. Skeletal muscle hypertrophy, insulin-like growth factor 1, myostatin and follistatin in healthy and sarcopenic elderly men: the effect of whole-body resistance training. Int J Prev Med. 2019;10(1):10. doi: 10.4103/ijpvm.IJPVM_310_17
- D-C L, Shook RP, Drenowatz C, et al. Physical activity and sarcopenic obesity: definition, assessment, prevalence and mechanism. Future Sci OA. 2016;2(3):FSO127. doi: 10.4155/fsoa-2016-0028
- Kang H. Sample size determination and power analysis using the G* power software. J Educ Eval Health Prof. 2021;18:18. doi: 10.3352/jeehp.2021.18.17
- Walker S, Serrano J, Van Roie E. Maximum dynamic lower-limb strength was maintained during 24-week reduced training frequency in previously sedentary older women. J Strength Cond Res. 2018;32(4):1063–1071. doi: 10.1519/JSC.0000000000001930
- Murlasits Z, Reed J. Muscular adaptations to periodized resistance-training in older adults. Sci Sports. 2020;35(4):216–222. doi: 10.1016/j.scispo.2019.10.007
- Ribeiro AS, Schoenfeld BJ, Souza MF, et al. Traditional and pyramidal resistance training systems improve muscle quality and metabolic biomarkers in older women: a randomized crossover study. Exp Gerontol. 2016;79:8–15. doi: 10.1016/j.exger.2016.03.007
- Moro T, Tinsley G, Bianco A, et al. High intensity interval resistance training (HIIRT) in older adults: effects on body composition, strength, anabolic hormones and blood lipids. Exp Gerontol. 2017;98:91–98. doi: 10.1016/j.exger.2017.08.015
- Shojaee M, Haghighi AH, Askari R. The effect of a resistance-power training and vitamin D supplementation on serum IGF-1 concentration and physical function in elderly women. Razavi Int J Med. 2022;10(4):15–21.
- Nascimento MAD, Gerage AM, Silva DRPD, et al. Effect of resistance training with different frequencies and subsequent detraining on muscle mass and appendicular lean soft tissue, IGF-1, and testosterone in older women. Eur J Sport Sci. 2019;19(2):199–207. doi: 10.1080/17461391.2018.1496145
- Hooshmandi Z, Daryanoosh F, Jahani P. Resistance training may improve rectus femoris muscle parameters in elderly women. Res Mol Med. 2022;10(2):0–.
- Shanazari Z, Faramarzi M, Banitalebi E, et al. Effect of moderate and high-intensity endurance and resistance training on serum concentrations of MSTN and IGF-1 in old male Wistar rats. Hormone Mol Biol Clin Invest. 2019;38(2):20180066. doi: 10.1515/hmbci-2018-0066
- Bian A, Ma Y, Zhou X, et al. Association between sarcopenia and levels of growth hormone and insulin-like growth factor-1 in the elderly. BMC Musculoskelet Disord. 2020;21(1):1–9. doi: 10.1186/s12891-020-03236-y
- Mafi F, Biglari S, Afousi A, et al. Epicatechin supplementation and resistance training-induced improvement of muscle strength and circulatory levels of plasma follistatin and myostatin in sarcopenic older adults. J Aging Phys Act. 2018;27(3):1–27. doi: 10.1123/japa.2017-0389
- Kwon JH, Moon KM, Min K-W. Exercise-induced myokines can explain the importance of physical activity in the elderly: an overview. Healthcare (Basel). 2020 Oct 1;8(4):378. doi: 10.3390/healthcare8040378. PMID: 33019579; PMCID: PMC7712334.
- Herbert P, Hayes LD, Sculthorpe N, et al. High-intensity interval training (HIIT) increases insulin-like growth factor-I (IGF-I) in sedentary aging men but not masters’ athletes: an observational study. Aging Male. 2017;20(1):54–59. doi: 10.1080/13685538.2016.1260108
- Iversen VM, Norum M, Schoenfeld BJ, et al. No time to lift? Designing time-efficient training programs for strength and hypertrophy: a narrative review. Sports Med. 2021;51(10):2079–2095. doi: 10.1007/s40279-021-01490-1