Abstract
Background The mechanical properties of present-day percutaneous repairs of Achilles tendon ruptures are not known.
Material and methods Artificially-created ruptures in 24 human cadaveric Achilles tendons were repaired with an open Bunnell repair, a percutaneous calcaneal tunnel or a percutaneous bone-anchor repair. In the open technique no.1 PDS-II absorbable suture material was used, and in the percutaneous techniques either no.1 PDS-II or no.1 Panacryl absorbable suture material was used. The specimens were tested in a materials testing machine until failure occurred.
Results The common mode of failure was suture breakage in non-anchor repairs, and anchor pullout in anchor repairs. The average strength of the repairs varied from 166 N (SD 60) to 211 N (SD 30), with no differences between the techniques (p = 0.5).
Interpretation Taking costs into account, the percutaneous calcaneal tunnel technique and the open technique are the methods of choice.
Various procedures have been described for the treatment of acute Achilles tendon rupture. Before the 1980s, nonoperative treatment was the most common approach (Nistor Citation1981). Recent studies have suggested that surgical treatment may have advantages over nonsurgical treatment (Möller et al. Citation2001, Wong et al. Citation2002), and that percutaneous repairs are preferable to open procedures (Lim et al. Citation2001). There have been very few mechanical studies regarding differences in strength of the various types of surgical Achilles tendon repair (Hockenbury and Johns Citation1990, Mortensen and Saether Citation1991, Watson et al. Citation1995, Cretnik et al. Citation2000, Jaakkola et al. Citation2000).
We have assessed the strength of a percutaneous bone-anchor repair and a calcaneal tunnel repair, and have compared these to the strength obtained from the classical open repair for acute Achilles tendon rupture. We also compared the strength of 2 different bioresorbable suture materials, monofilament PDS-II and braided Panacryl, for use in the repairs.
Materials and methods
Free suture tests
To assess the strength of commonly used suture material, we tested single-strand no.1 PDS-II and Panacryl (Johnson & Johnson, Brussels, Belgium) in a screwdriven Lloyd Instruments LRX test machine (Lloyd Instruments, Hampshire, UK). The sutures were tested in a loop set-up. The loop was closed with 8 alternating knots; it was 20 cm long. The sutures were preconditioned for 20 cycles at a rate of 6 mm/s up to 30 N, followed by a linear extension done at 6 mm/s until failure occurred. A preload of 2 N was maintained between the cycles. Each test was repeated 5 times. Force and extension were measured and recorded by computer.
Tendon tests
We used 24 fresh-frozen human cadaveric lower legs with a mean age of 79 (SD 12) years. A bone-tendon unit consisted of the Achilles tendon with a part of the os calcis. A simulated rupture was made by a sharp cut through the tendon 4 cm cranial to the calcaneal insertion.
The tendons were repaired by one of the following methods: 1. open technique: 2 PDS-II no.1 (n = 5), 2. percutaneous calcaneal-tunnel technique: 2 PDS-II no.1 (n = 4), 3. percutaneous calcaneal-tunnel technique: 2 Panacryl no.1 (n = 5), 4. percutaneous repair: 2 Mitek anchors and 2 PDS-II no.1 (n = 5), 5. percutaneous repair: 2 Mitek anchors and 2 Panacryl no.1 (n = 5).
In the open repair group, the tendon parts were sutured using the Bunnell method (). For the percutaneous repairs, the Bunnell method was used for the proximal intra-tendineous part. In the calcaneal tunnel groups (2 and 3), a 2.0-mm hole was drilled transversely through the calcaneus and the sutures were transported through the tunnel in the calcaneus using a suture retriever ().
Figure 1. Schematic drawing of suture techniques:a.open method with Bunnell sutures, b. calcaneal tunnel method, c. bone anchor method.
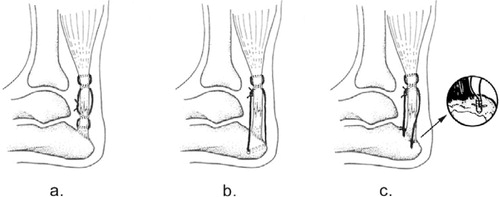
In the bone anchor groups (4 and 5), 2 bone anchors were used. The anchors were placed according to the instructions of the manufacturer (). All repairs had 4 strands of suture material passing from the distal part of the tendon to the proximal part, which were tied together with 8 alternating knots.
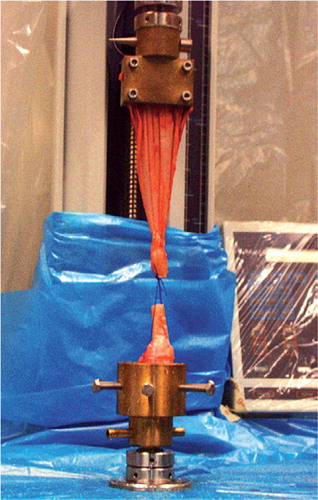
The repaired bone-tendon units were put into the LRX testing machine, with the os calcis fixed in a bone clamp with 6 screws and the tendon in a tendon clamp. Both clamps were custommade (). The LRX-crosshead speed was set at 6 mm/s for detailed recording of force and extension data. The specimens were preconditioned 20 times with a preload of between 2 N and 30 N, followed by a linear extension until failure. Between the cycles, a preload of 2 N was maintained. Failure was defined as either breaking of the suture, tendon rupture, anchor pullout, or calcaneal tunnel failure. Force and crosshead displacement were recorded. Force-displacement curves and ultimate load were assessed in order to compare the different methods.
Figure 2. Test specimen in custom-made clamps at the moment of failure.
Statistics
Because of the small numbers of specimens per group, statistical analysis was performed with a nonparametric one-way ANOVA of all groups (Kruskal-Wallis and Mann-Whitney test), with the significance level set at p ≤0.05 (Jandel Sigma Stat 2.0 statistics package, SPSS Inc., Chicago, IL). The statistical power, assuming 30% minimal relevant difference, was approximately 80%.
Results
Free suture test
The mode of failure was suture breakage at the knot. The average strength in a two-strand set-up of PDS-II was 96 N (SD 9.2), and that of Panacryl was 99 N (SD 5.7). There was no difference in strength (p = 0.4). Up to a load of 50 N, PDS-II showed more lengthening than Panacryl, with a compliance of 0.41 mm/N (SD 0.02) as opposed to 0.19 mm/N (SD 0.03) (p = 0.008). The Panacryl wire yielded after a load of 53 N.
Tendon tests
In the 5 open repairs the suture broke in 4 cases, while in 1 case the intact suture was ripped out of the tendon. Failure in the 9 tunnel repairs occurred at the suture in 8 cases. In 1 case, the tunnel itself failed. In 9 of 10 anchor repairs, the failure was anchor pullout. Suture breakage was seen once. No differences in strength were found between the different repair techniques (p = 0.5) ().
Table 1. Tendon test results
Discussion
The failure strength of the free suture strands in our study corresponded with the manufacturer's values (personal communication). We found the Panacryl and PDS-II sutures to be of equal strength, but there was a difference in compliance up to a load of 50 N. This may have some influence on the amount of distension between the tendon ends during loading, and should be the subject of further study.
All the anchors were positioned according to the manufacturer's instructions. Even so, all but one of the anchor repairs failed through pullout of an anchor. This might be due to the high age of the donors. In senile osteopenia, the amount of trabecular and cortical bone is reduced (Simon Citation1994). It is known that the amount of osteoporosis of the calcaneus corresponds to the overall bone condition of the patient (Wehrli et al. Citation2002). We did not assess bone mineral density, but as most of the specimens were old, we can assume that osteoporosis in the calcaneus was present. Failure strength of bone anchors depends on cortical bone thickness (Roth et al. Citation1998). The manufacturer could not supply us with pullout data for this type of anchor. Thus, it may be advisable not to use bone anchors in elderly and osteoporotic patients.
Another possible explanation for anchor failure in the anchor repair groups could be that forces are unequally distributed over both anchors. The tightest loop/anchor combination will sustain most of the load, and will therefore be pulled out first. The bone anchors cost approximately EUR 185 each. One repair requires 2 anchors, which makes this repair more expensive than the other repairs in the study.
This is the first cadaveric study to test the percutaneous calcaneal tunnel technique. The failure strengths found for this repair are comparable with the results of other studies in which 4 suture strands were used ().
Table 2. Overview of mechanical studies of Achilles tendon repair
We used the open Bunnell repair as the golden standard to which we could compare the other repairs. The suture was the weakest link in the open Bunnell and in the calcaneal tunnel groups. The strength of the repair benefits from more suture strands crossing the rupture (). As tested by Jaakkola et al. (Citation2000), the triple-bundle technique with 6 strands showed a higher loading capacity. However, using more suture strands might compromise the tendon or the wound healing.
Although rehabilitation after Achilles tendon repair was not the subject of our study, our advice would be to protect the repair during early mobilization. During walking, the load on an Achilles tendon is around 1430 N (SD 500) for a person weighing 70 kg (Finni et al. Citation1998). During running, this can rise to 5740 N (Scott and Winter Citation1990). Both loads are many times greater than the strength of our repairs.
In conclusion, we found the repairs that we studied to be of equal strength. It would not be advisable to use bone anchor repairs for elderly and osteoporotic patients. Taking costs into account, the percutaneous calcaneal tunnel technique or the open technique may be preferable. The clinical implications of the various repairs were not studied, and thus no repair can be advocated as being ‘the best’. The forces on the Achilles tendon during walking and running exceed the strength of all repairs by manyfold; thus, careful postoperative treatment is imperative.
- Cretnik A, Zlaipah L, Smrkolj V, Kosanovic M. The strength of percutaneous methods of repair of the Achilles tendon: a biomechanical study. Med Sci Sports Exerc 2000; 32(1)16–20
- Finni T, Komi P V, Lukkariniemi J. Achilles tendon loading during walking: application of a novel optic fiber technique. Eur J Appl Physiol Occup Physiol 1998; 77(3)289–91
- Hockenbury R T, Johns J C. A biomechanical in vitro comparison of open versus percutaneous repair of tendon Achilles. Foot Ankle 1990; 11(2)67–72
- Jaakkola J I, Hutton W C, Beskin J L, Lee G P. Achilles tendon rupture repair: biomechanical comparison of the triple bundle technique versus the Krakow locking loop technique. Foot Ankle Int 2000; 21(1)14–7
- Lim J, Dalal R, Waseem M. Percutaneous vs. open repair of the ruptured Achilles tendon--a prospective randomized controlled study. Foot Ankle Int. 2001; 22(7)559–68
- Möller M, Movin T, Granhed H, Lind K, Faxén E, Karlsson J. Acute rupture of tendo Achilles. A prospective randomised study of comparison between surgical and non-surgical treatment. J Bone Joint Surg (Br) 2001; 83(6)843–8
- Mortensen N H, Saether J. Achilles tendon repair: a new method of Achilles tendon repair tested on cadaverous materials. J Trauma 1991; 31(3)381–4
- Nistor L. Surgical and non-surgical treatment of Achilles tendon rupture. A prospective randomised study. J Bone Joint Surg (Am) 1981; 63(3)394–9
- Roth C A, Bartolozzi A R, Ciccotti M G, Wetzler M J, Gillespie M J, Snyder-Mackler L, Santare M H. Failure properties of suture anchors in the glenoid and the effects of cortical thickness. Arthroscopy 1998; 14(2)186–91
- Scott S H, Winter D A. Internal forces of chronic running injury sites. Med Sci Sports Exerc 1990; 22(3)357–69
- Simon S R. Orthopaedic basic science. Am Academy of Orthop Surg 1994; 159
- Watson T W, Jurist K A, Yang K H, Shen K L. The strength of Achilles tendon repair: an in vitro study of the biomechanical behaviour in human cadaver tendons. Foot Ankle Int 1995; 16(4)191–5
- Wehrli F W, Hilaire L, Fernandez-Seara M, Gomberg B R, Song H K, Zemel B, Loh L, Snyder P J. Quantitative magnetic resonance imaging in the calcaneus and femur of women with varying degrees of osteopenia and vertebral deformity status. J Bone Miner Res 2002; 17(12)2265–73
- Wong J, Barrass V, Maffulli N. Quantitative review of operative and nonoperative management of Achilles tendon ruptures. Am J Sports Med 2002; 30(4)565–75