A 20-year-old woman was hit by a rolling rock. She was rescued immediately without any other apparent injuries. Radiographs showed a central fracture of the first sacral vertebra and pubic symphysis diastasis of 30 mm with bilateral pubic rami fractures (). CT revealed that the vertical midline fracture was limited to the first sacral vertebra. Bilateral sacral compression fractures were also present at the level of the S2–S3 junction (). The patient was operated for pubic diastasis 48 hours later and symphyseal closure was maintained by a 5-hole reconstruction plate. The bilateral ramii fractures and the slight opening in the right sacroiliac joint were managed with a pelvic anterior external fixator. It was suggested that by anterior external fixation, a stable fixation in such a slight posterior sacroiliac opening could be maintained and it could be more beneficial for the ramii fractures rather than a wide exploration on both sides. Because the lesion was vertically stable, and because anterior instability was more severe than posterior unilateral opening, an additional posterior fixation was not considered. The external fixator was removed after 2 months. Full weight bearing was allowed after 3 months. At 9 months, the fractures were healed and the patient was pain-free, with normal hip motion.
Figure 1. A vertical fracture line on the S1 vertebra could easily be seen on plain film.

Figure 2. CT scan showing the fracture line and slight disruption of the right sacroiliac joint (A). Bilateral compression fractures on both sides are shown with arrows in panel B.
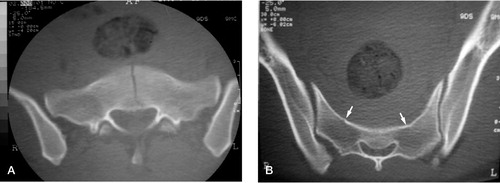
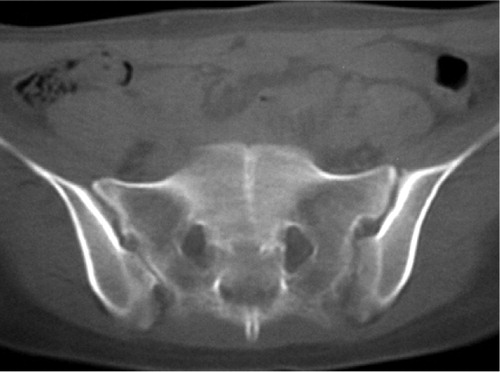
Figure 2. CT scan at 9 months showing healed fracture line.
Discussion
Uncommon sacral fractures usually occur by shear forces on the pelvic ring: zone I fractures in the region of the ala, zone II fractures in the region of the sacral foramina, and zone III fractures involving the central canal (Denis et al. Citation1988). Isolated sacral fractures are seen less commonly and they are commonly transversely oriented. In this report, we describe an unusual sacrum fracture in which the fracture was vertically oriented in the midline of the first sacral vertebra.
Zone III (central) sacral fractures are rare, and only a few cases have been reported in the literature (Weisel et al. Citation1979, Moed and Morawa Citation1984, Denis et al. Citation1988, Carter and Lambert Citation1990). To our knowledge, no isolated vertical midline fracture of the first sacral vertebra has been described previously.
A sacral fracture should be suspected when there is a displaced anterior pelvic fracture with an intact sacroiliac joint. Vertical sacral fractures are frequently associated with low-lying dural sac and spina bifida occulta (Nabil et al. Citation1996). The bifid spinal processes are thought to act as stress risers in producing longitudinal fractures (Carter and Lambert Citation1990). Vertical sacral fractures most commonly occur in alar or foraminal zones. The transverse fractures are seen frequently in patients with suicidal intent and have been referred to as the jumper's fracture (Moed and Morawa Citation1984). The transverse fractures usually occur at S2-S3 level because the upper two segments of the sacrum are stabilized by the sacroiliac joint, and the coccyx may act as a lever arm on the sacral body at S2–S3 level, where the apex of normal sacral kyphosis is located (Fountain et al. Citation1977).
The pelvic injury in our patient seems to have been an open book injury with pubic symphysis diastasis and bilateral pubic rami fractures. On the other hand, bilateral sacral compression fractures were present, suggesting a lateral compression injury. Currently known classifications of pelvic fractures are usually based on the injury mechanism causing the fracture, and are named as external rotation, lateral compression or vertical shear. Such an unclassified isolated fracture of the sacrum (S1) cannot be explained by these force patterns, according to known mechanisms. In the presence of anterior pelvic lesions, assessment of the sacrum should be done carefully—even if the sacroiliac joints are stable.
- Carter T R, Lambert K. Pubic diastasis with longitudinal fracture of the sacral body: Case report. J Trauma 1990; 30: 627–9
- Denis F, Davis S, Comfort T. Sacral fractures: An important problem. Retrospective analysis of 236 cases. Clin Orthop 1988, 227: 67–81
- Fountain S S, Hamilton R D, Jameson R M. Transverse fractures of the sacrum. A report of six cases. J Bone Joint Surg (Am) 1977; 59: 486–9
- Moed B R, Morawa L G. Displaced midline longitudinal fracture of the sacrum. J Trauma 1984; 24: 435–7
- Nabil A E, Ashok B, Benjamin S. Zone III fractures of the sacrum. A case report. Spine 1996; 21: 2390–6
- Weisel S W, Zeide M S, Terry R L. Longitudinal fractures of the sacrum: Case report. J Trauma 1979; 19: 70–1