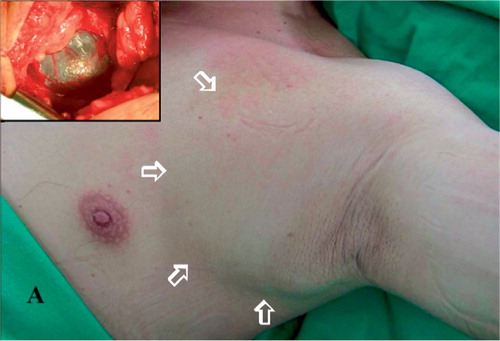
A 78-year-old man presented with a rapidly enlarging soft tissue mass at the subclavian region of the left shoulder and progressive pitting edema of his left upper limb. There had been symptoms for 1 week. The mass was fluctuant, ballotable, non-tender, non-pulsatile, translucent and fixed to the chest wall. () There were no other previous symptoms or signs, but 2 years previously, the patient had a proximal femur fracture with a painful nonunion that forced him to use walking aids. He constantly used axillary crutches, which sometimes caused him mild shoulder pain.
Figure 1. (A) Photograph showing a large ballotable mass over the left infraclavicular fossa and axilla. The inset shows the intraoperative view of the tumor. Note the characteristic appearance of a cystic hygroma, containing clear serous fluid and encapsulated with a thin membrane.
CT of the chest demonstrated a well-defined homogenous 10 × 8 × 4-cm cystic mass under the pectoralis minor muscle and attaching to the chest wall, compressing subclavian vessels ().
(B) Computed tomogram with contrast enhancement of the chest. A well-defined homogenous cystic mass is located underneath the pectoralis minor muscle and is attaching to the chest wall. This also showed that the ipsilateral subclavian vessels were compressed by the cystic mass.

A hip hemiarthroplasty with bipolar endoprosthesis was done in the same session as an excision of the tumor was performed through a double-incision approach, one incision lateral to the edge of the pectoralis muscle, and the other over the infra-clavicular fossa. The mass originated from the apical nodes and subclavian lymph trunk. Grossly, it was hygroma-like, containing clear serous fluid and encapsulated by a thin membrane (). Histologically, it was composed of dilated lymphatic channels with intervening fibrous tissue and lymphoid aggregates. A layer of flattened, elongated endothelial cells lined the lymphatic spaces. () The microscopic appearance was consistent with a macrocystic lymphatic malformation, a lesion generally considered to be a congenital malformation.
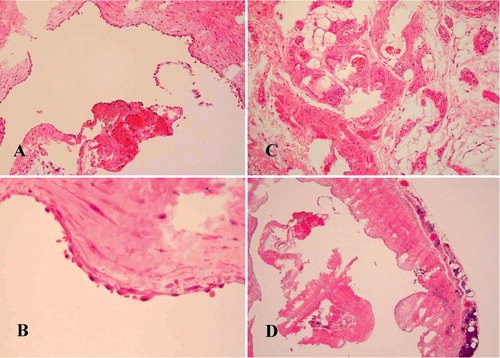
Figure 2. (A) Photomicrograph showing the dilated cystic structures (H & E);original magnification × 100) (B) Higher-power view of the cystic wall showing a lining layer of flattened, elongated endothelial cells (H & E;× 400) (C) Tissue biopsy specimen showing the presence of aggregated red cells in the variablesized lymphatic channels (H & E;× 200) This implies that an irritative incident can cause hemorrhage into the cystic structures, and can then facilitate speedy growth of the mass.(D) Lower-power view of the tumor origin showing the characteristic microscopic picture of intervening fibrous tissue and lymphoid aggregates (H & E; × 40).
Postoperatively, the patient had complete resolution of the limb edema within a day and also recovered his right hip function smoothly. He was restricted to weight-bearing ambulation as much as was tolerable, under the assistance of a walker for three months. He was then allowed free mobilization. 2 years after surgery, he had no residual symptoms.
Discussion
All lymphatic malformations—by definition—are believed to be present at birth, but some only become manifest at a later age. Between 65% and 75% are diagnosed at birth, and nearly 90% are clinically detected by the end of the second year of life (Fliegelman et al. Citation2000, Kennedy et al. Citation2001). Occurrence in adults is extremely rare and usually represents late recurrence of a lymphatic malformation treated earlier. Although several possible mechanisms (traumatic, infectious, iatrogenic, neoplastic, and hormonal) of adult lesions have been proposed, there are still only a few case reports in the literature (Baer and Davis Citation1989). In fact, we have not been able to find a similar commentary reporting a rapidly enlarging lymphatic malformation in an elderly crutch-dependent patient without any past history of a previously detectable lesion.
Axillary crutches can reduce the load on the lower limbs in patients with fractures or painful joints, and help with balance. When using axillary crutches the patient has to lock his elbow in extended position, forcefully adducting his shoulder and pushing the crutch against the ground at the same time as the injured leg. There are several documented complications of chronic axillary crutch use, including axillary artery stenosis, aneurysm formation, axillo-brachial thrombo-embolic disease, radial nerve crutch palsy, ulnar nerve palsy, brachial plexus compressive neuropathy, stress fracture, and upper-limb overuse injury (Ettien Citation1980, Lee et al. Citation1987, Poddar et al. Citation1993, Raikin and Froimson Citation1997, Garcia Suarez et al. Citation2001, Koh et al. Citation2002). The hip nonunion forced our patient to use crutches. He recalled left-shoulder and pectoral pain. After such chronic overuse of the pectoralis muscles, a cystic tumor unexpectedly appeared on his left infra-clavicular fossa. The tumor enlarged rapidly, extended toward the axilla day by day and eventually produced arm swelling due to the mass effect on the vessels.
The natural history of lymphatic malformation is variable. As with our case, an originally small lesion might fail to afford adequate transport capacity for clearing the increased lymphatic load when faced with some form of stress such as an overuse syndrome, resulting in venous obstruction and hence an increased volume of lymph (Brorson Citation2000). The resultant dynamic insufficiency or high output failure of the lymphatic system probably caused the activation of a dormant subclavian lymphatic malformation. The accumulation of lymph in the cystic structures and the formation of additional endothelial sprouts further increased the size of the lesion and then made venous obstruction more severe. The above sequence of events became a vicious circle, and consequently led to continuous swelling of the arm. The normalization of the arm swelling after surgery indicates that there was no established mechanical insufficiency of the lymphatic system.
The additional endothelial sprouts could spread the lesion further into areas of least resistance, invading tissue planes, and even penetrating into the mediastinum (Fliegelman et al. Citation2000). Although various methods of treatment have been attempted (Kennedy et al. Citation2001), complete excision of the cystic mass effectively relieves the acute mass effect on the vessels, and hence the arm swelling. If the arm swelling persists after surgery, indirect lymphoscintigraphy should be performed to rule out the possible coexistence of reduced lymph transport, i.e. mechanical insufficiency or low output failure of the lymphatic system (Brorson Citation2000).
- Baer S, Davis J. Cystic hygroma presenting in adulthood. J Laryngol Otol 1989; 103: 976–7
- Brorson H. Liposuction gives complete reduction of chronic large arm lymphedema after breast cancer. Acta Oncol 2000; 39: 407–20
- Ettien J T. Crutch-induced aneurysms of the axillary artery. Am Surg 1980; 46: 267–9
- Fliegelman L J, Friedland D, Brandwein M, Rothschild M. Lymphatic malformation: Predictive factors for recurrence. Otolaryngol Head Neck Surg 2000; 123: 706–10
- Garcia Suarez G, Garcia Garcia J, Perez Carro L. Stress fracture of the ulna associated with crutch use. J Orthop Trauma 2001; 15: 524–5
- Kennedy T L, Whitaker M, Pellitteri P, Wood E. Cystic hygroma/lymphangioma: a rational approach to management. Laryngoscope 2001; 111: 1929–37
- Koh E S, Williams A J, Povlsen B. Upper-limb pain in longterm poliomyelitis. QJM 2002; 95: 389–95
- Lee A W, Hopkins S F, Griffen W O, Jr. Axillary artery aneurysm as an occult source of emboli to the upper extremity. Am Surg 1987; 53: 485–6
- Poddar S B, Gitelis S, Heydemann P T, Piasecki P. Bilateral predominant radial nerve crutch palsy. A case report. Clin Orthop 1993; 297: 245–6
- Raikin S, Froimson M I. Bilateral brachial plexus compressive neuropathy (crutch palsy). J Orthop Trauma 1997; 11: 136–8