Abstract
Background Intramedullary plugs are key factors in improving cement fixation of the femoral component. We investigated the performance of 3 commercially available resorbable cement restrictors in vitro and in vivo.
Methods We measured the migration of the SEM II, the C-plug, and the REX plug in 15 Sawbones synthetic femurs and in 103 patients during total hip surgery. Cement pressures were also measured distally and proximally in vitro.
Results and interpretation Our in vitro results showed poor performance of the C-plug compared with the REX and SEM II plugs. In vivo, the mean migration was least for the SEM plug and most for the C-plug. The smaller sizes performed significantly better than the larger ones for all 3 plug types. The overall in vivo performance of all 3 plug types was unsatisfactory. Differences between the SEM II and REX plugs were small and therefore not significant. The SEM II performed better than the REX, the former being much cheaper and easier to insert. The Rex plug looks promising; however, the insertion device must be improved for better results. The C-plug proved to be unstable.
To achieve adequate (peak) pressures for cementbone interdigitation during stem insertion, adequate plugging of the distal femoral canal is essential (Song et al. Citation1994). Intramedullary plugs are widely regarded as one of the key elements in improving cement technique (Suominen et al. Citation1996). The main reason for this is the augmented cement pressurization when using a plug (Maltry et al. Citation1995). Any cement leakage and plug migration will result in reduced cement pressure. Another advantage of using intramedullary plugs is the restricted spread of cement in the femur. This makes removal of the distal cement easier during revision of a cemented stem. Also, biodegradability of the plug makes surgery easier. Removing nonresorbable plugs can be as difficult as removing distal cement.
Older designs of cement plugs, such as the Thackray and Cemlock plugs, have been shown to perform poorly (Bulstra et al. Citation1996, Freund et al. Citation2003). In vivo trials with the most frequently used resorbable plug also show poor results (Visser et al. Citation2002). To avoid the necessity of using Kirschner wires to prevent the plug from migrating (Northmore-Ball et al. Citation1991), new gelatine-based resorbable designs have been manufactured for improved performance. In vitro testing of these newer designs has shown promising results (Heisel et al. Citation2003a, Citationb).
Most comparative trials of plugs have been carried out in vitro, to increase the reproducibility of the tests. In vitro findings may, however, not be the same as in patients. In order to estimate the stability of 2 commonly used types of resorbable intramedullary plugs and to evaluate a newer more promising type of plug with an expanding mechanism, we undertook a prospective comparative study in vivo. An in vitro study was also performed to evaluate the mechanical performance of these 3 types of plugs.
Material, patients and methods
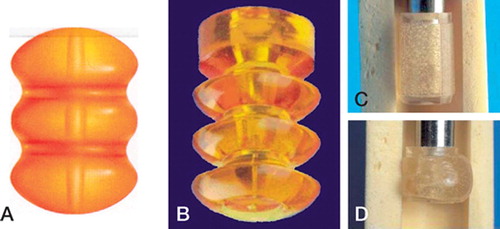
We tested 3 intramedullary resorbable cement plugs in vitro and in vivo. 1. The SEM II plug (Biomet, Warsaw, IN): a cylindrical, larva-shaped gelatine-based plug, available in sizes 8–18 (odd and even sizes). 2. The C-plug (DePuy International): also a round, larva-shaped gelatine-based plug, available in sizes 10–18 (even sizes only). Both these plugs fixate mechanically by friction. 3. The REX plug (A-One Medical B.V., Oss, the Netherlands), a cylindrical gelatine-based plug specially designed to fit medullary canals that are not reamed in a circular manner. This plug is available in small, medium, and large sizes and can be fixated at a specified depth in the femoral canal by a firing mechanism ().
Figure 1. The SEM II plug (A), the C-plug (B) and the REX cement plug (before and after firing, C and D).
In vitro tests
We carried out in vitro tests on the REX and SEM II plugs and the C-plug in the Bioengineering Research Laboratory at Anglia Ruskin University, using Sawbones composite femurs, model 1130–27 (Sawbones, Malmo, Sweden). 15 tests were performed, 5 per restrictor, using the “medium” plug sizes. The medullary canals were reamed so that the distal ends were shaped in an oblong shape of 12 mm by 14 mm, using a numerically-controlled machine (by computer), to simulate inaccuracy that may be incurred during the reaming process during surgery. To accommodate 2 pressure transducers, 2 holes were drilled through the femurs, 20 mm and 120 mm below the medial proximal end of the prepared femur (Entran 70 bar and Kulite 17 bar). A linear potentiometric displacement transducer (LPDT) (Techni Measure, Warwickshire, B80 7NJ) was positioned at the base of the cement plug to measure migration during cement pressurization. Cement leakage was also measured. Cement plugs were then inserted 130 mm from the medial proximal end for all the tests, and according to the manufacturer's instructions. SimplexP cement was vacuum-mixed following the manufacturer's recommendations, introduced into the intramedullary canal of the prepared Sawbones femur, and pressurized for 30 sec using a DePuy pressurizer. The femoral prosthesis was then introduced at a controlled speed of 10 mm/sec into the femur, when the cement was still in a doughy state, 80–100 seconds after mixing the cement.
A special jig was manufactured to fix the prepared femur and stem in an Instron 8874 mechanical testing machine for controlled insertion of the femoral prosthesis into the prepared femurs. Data captured by the pressure transducers were digitized, using an analog/digital converter (Instrunet 100) and recorded electronically. Room temperature was kept at 20°C and each test was repeated 5 times.
In vivo tests
We carried out investigations on 103 patients (), 29 males and 74 females. We measured the differences in migration between the SEM II plug (n 37), the C-plug (n 31) and the REX plug (n 35). The 3 types of plugs have different sizes, as described above (numerical or categorial). In the case of using a C- or a SEM II plug, the size was determined according the instructions of the respective manufacturers. The diameter of the canal was measured and the corresponding size was choosen. (The possible advantage of increasing stability by oversizing of the plugs was not the subject of the study and was therefore not investigated.)
Table 1. Details of cement plugs used on 103 patients during the in vivo investigations
To be able to compare the 3 types of plugs statistically, we created 3 groups (small, medium, large) in each type of restrictor. The division was made based on the REX system, which refers to the size of the femoral canal measured during the operation. After the diameter is measured, the corresponding plug is defined. Small plugs were used for medullary canal diameters of up to 8 mm, medium plugs for diameters of 9–12 mm, and large plugs were used for diameters of 13 mm or more.
Based on these 3 categories of diameters of the canal, the corresponding C-plugs, REX plugs and SEM II plugs were classified in the following size categories: small, medium or large. shows the numbers of the different sizes of each type of cement plug used in the in vivo study.
SP II stems (Link, Hamburg, Germany) were fixed using a direct lateral approach. All sizes of the SP II prostheses used were of the same length. The plugs were inserted according to the manufacturer's instructions. The depth to which the plug was inserted during surgery was measured, using a custom-made device that could be fixed to the plug-inserting device (). We measured the distance between an easily recognizable point on a standardized radiograph (the most medial edge of the osteotomy of the proximal femur) and the upper level of the restrictor. The plugs were placed at a fixed depth of 130 mm from this point. The cement was injected in a retrograde fashion without the use of a pressurizer. The femoral stem was inserted within 150 sec of the onset of cement mixing.
Figure 2. Custom-made measuring device that can be fixed to the plug-inserting device. The arm must be placed on the medial edge of the osteotomy.

The migration was determined on standardized radiographs, using the stem length to calculate the enlargement of the radiograph and differences caused by malalignment of the femur. To exclude small measuring inaccuracies, we defined a plug as being clinically stable when migration was less than 1 cm.
Statistics
For statistical analysis of the test results, we used an analysis of variance. Since there were 3 groups to compare, we used post-hoc tests (Tukey HSD, Scheffe, LSD) to perform all possible pairwise comparisons between these groups while accounting for the fact that multiple statistical tests are being performed. The amount of migration itself was analyzed as a continuous variable (not a dichotomized version such as yes/no migration). Homogeneity of variances was assessed using Levene's test. On the orginal scale the test was just significant. After a log transformation, hetereogeneity could be assumed (p = 0.5). However, the parameters are difficult to interpret on a log scale. Since the overall model p-value changed only marginally and remained very significant, and since the individual contributions of plug size and plug type were significant in both models, we chose to report the estimates from the original model, although we realize that—formally speaking—heterogeneity was present. Thus, the clinically used 1 cm criterion for stability was not a criterion for the statistical analysis regarding the amount of migration.
Results
In vitro tests
The C-plug was unstable 4 of 5 times. The SEM II was unstable once, and there was minimal cement leakage 4 times. The REX plug was stable all times, without cement leakage. Distal cement pressure was significantly higher with the REX plug and the SEM II plug ( and ).
Figure 3. Average distal cement pressure for the 3 cement plugs during introduction of the stem.
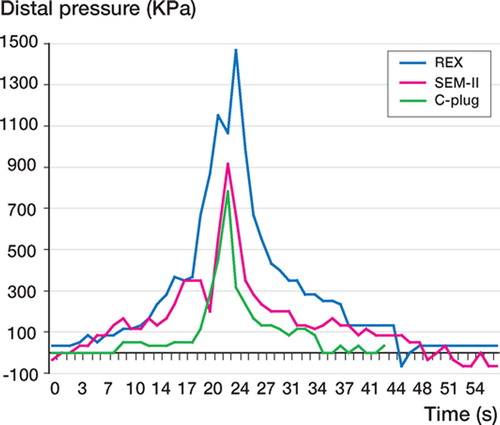
Table 2. Results of peak pressure and migration values for the cement plugs averaged over 5 tests
In vivo tests
17 of the 37 SEM II migrations were within the 1-cm margin. The C-plug was used 31 times and was stable only 8 times, according to our clinical criterion for stability. The REX plug was stable 16 times out of 35. 2 variables had significant influence on the results: the type of plug (p = 0.02) and the size of plug used (p = 0.02).
shows the mean migration according to the type of plug, corrected for the effect of size. The SEM II plug performed best and the C-plug worst. Regarding the sizes of the plugs (), the large and small plugs resulted in large migrations. Medium-sized plugs of all types performed satisfactorily. The SEM II plug performs well in small sizes also.
Table 3. Migration according to the type of plug, corrected for the effect of size
Table 4. Migration according to size of plug, corrected for the effect of plug type
Different pairwise comparisons (Tukey HSD, Scheffe, LSD) between the 3 types of plugs all indicated that the difference in mean migration between the SEM II plug and the others was significant (p = 0.05 level). There was no significant difference between the REX plug and C-plug.
Discussion
The use of resorbable restrictors in cemented hip arthroplasty certainly has advantages compared to other types of restrictors. All commercially available cement restrictors migrate to some extent under all circumstances. In fact, the overall in vivo performance of all 3 types of resorbable restrictors we tested was unsatisfactory; surprisingly, even that of the REX plug.
The SEM II plug was the most stable of the 3. This is surprising because in a previous study, the SEM plug did not perform very well (Visser et al. Citation2002). A possible explanation might be the fact that the SP II stem is relatively short whereas the Stanmore prosthesis, which was used in the previous study, is longer (particularly the larger sizes). When a longer stem is used, the plug is often placed below the isthmus. This could result in more plug migration than when a short stem is used.
As in other studies, especially with the small and large femurs, the C-plug and the REX plug did not perform well (Noble et al. Citation1998). The poor results of the C-plug may be due to its design. It is much more flexible than the others, thereby creating less friction than the SEM II plug, which is far more rigid. Previous in vitro investigations on the performance of cement restrictors using perfectly reamed synthetic Sawbones femurs gave given favorable results for the C-plug (Mootanah et al. Citation2003). The poor results with the C-plug in our in-vitro study may be because its design cannot cope with imperfections made to the distal end of the femur during the reaming process.
In the in vitro tests, the REX plug proved to be stable. Differences in the in vitro performance between the SEM II plug and the REX plug were small and not significant. Apart from the satisfying stability of the SEM II plug and the REX plug in the in vitro tests, the difference in performance of the REX plug, both in vitro and in vivo, is notable. Distal peak pressures measured in vitro were high compared to recent studies (Kapoor et al. Citation2004). Differences in distal peak pressure might be caused by the femoral component used, the diameter of the femoral canal, the viscosity of the cement, and—of course—plug migration or leakage.
The problems we encountered with the REX plug in vivo were caused by difficulties in getting the right balance between pressurizing the gelatinebased plugs and the use of the inserting device that could fire too soon, leaving the plug in the original uncompressed shape and therefore unable to function properly. One of the reasons for this problem is the large diameter of the inserting device, which leaves little room for maneuver—especially in narrow femoral canals. Thus, the plug could have been pressurized sideways, causing the release mechanism to activate earlier than it should. The failures for the “small” group may be explained by this mechanism. Adjustments have already been made to overcome this problem (flexible and thinner inserting devices are being tested). The incongruence between the number of REX plugs that were stable and the mean migration may be the result of the reaming required when the REX plug is used. When the REX plug migrates, it moves further than the other plugs do, probably because the release mechanism of the inserting device was triggered earlier than required, or due to the absence of the distal spongiosa from the plug. The lack of grip in large femurs might explain the unsatisfactory results in the large group. Reaming to a specified level may be one solution. However, this plug already requires more skill than the others, and it is not advisable to add more steps to the procedure.
These problems partially explain the disappointing in vivo results for the REX plug compared to its performance in vitro. Insertion of the REX plug in vitro can be done virtually without friction, or without any pressure in the opposite direction. Other reasons for the differences between the results of in vitro and in vivo tests may be the absence of moisture and lower temperature in vitro, both of which can influence the state of the gelatine material in vivo and therefore the friction at the interface between the plugs and bone. When using cadaveric femora, the differences in temperature may be even greater.
On the basis of this study, we do not recommend the use of the C-plug in cemented hip arthroplasty. The Rex plug is a promising design; however, insertion problems in vivo lead to disappointing results, so the insertion technique must be improved. The SEM II plug performs well in the case of a short stem and has a reproducible insertion technique.
The authors gratefully acknowledge the suppliers of cement plugs and bone cement for the in vitro tests, namely A-One Medical B.V., Biomet, DePuy International and Stryker. The sponsors did not plan the experiment, and took no part in data collection, interpretation of the data, or writing of the manuscript.
Contributions of authors
MK was the main investigator for the clinical trial (in vivo study) and second investigator in the in vitro trial; he was also co-writer of both the protocol and the manuscript. CPJ was co-writer of both the protocol and the manuscript, and supervised the clinical trial. RM was the main investigator in the in vitro trial, and co-writer of the manuscript. RB performed statistical analysis, and was co-writer of both the protocol and the manuscript
- Bulstra S K, Geesink R G, Bakker D, Bulstra T H, Bouwmeester S J, van der Linden A J. Femoral canal occlusion in total hip replacement using a resorbable and flexible cement restrictor. J Bone Joint Surg (Br) 1996; 78(6)892–8
- Freund K G, Herold N, Rock N D, Riegels-Nielsen P. Poor results with the shuttle stop. Acta Orthop Scand 2003; 74(1)37–41
- Heisel C, Norman T, Rupp R, Pritsch M, Ewerbeck V, Breusch S J. In vitro performance of intramedullary cement restrictors in total hip arthroplasty. J Biomech 2003a; 36(6)835–43
- Heisel C, Norman T L, Rupp R, Mau H, Breusch S J. Stability and occlusion of six different femoral cement restrictors. Orthopade 2003b; 32(6)541–7
- Kapoor B, Datir S P, Davis B, Wynn-Jones C H, Maffulli N. Femoral cement pressurization in hip arthroplasty. Acta Orthop Scand 2004; 75(6)708–12
- Maltry J A, Noble P C, Kamaric E, Tullos H S. Factors influencing pressurisation of the femoral canal during cemented total hip arthroplasty. J Arthroplasty 1995; 10(4)492–7
- Mootanah R, Pratt D, Ingle P, Cheah K, Dowell J. An in-vitro comparative study of the performance of different commercially available intramedullary femoral plugs during total hip replacement. Proc Int Soc Biomech 2003; 19, on CD
- Noble P C, Collier M B, Maltry J A, Kamaric E, Tullos H S. Pressurisation and centralisation enhance the quality and reproducibility of cement mantles. Clin Orthop 1998, 355: 77–89
- Northmore-Ball M D, Narang O V, Vergroesen D. Distal femoral plug migration with cement pressurisation in revision surgery and a simple technique for its prevention. J Arthroplasty 1991; 6(3)199–201
- Song Y, Goodman S B, Jaffe R A. An in vitro study of femoral intramedullary pressures during hip replacement using modern cement technique. Clin Orthop 1994, 302: 297–304
- Suominen S, Antti-Poika I, Tallroth K, Santavirta S, Voutilainen P, Lindholm T S. Femoral component fixation with and without intramedullary plug. Arch Orthop Trauma Surg 1996; 115: 276–79
- Visser C P, Eygendaal D, Coene L N, Tavy D L. Comparative prospective trial of 3 intramedullary plugs in cemented total hip arthroplasty. J Arthroplasty 2002; 17(5)576–8