Abstract
Background Controversy exists as to whether polyethylene (PE) penetration of hip prostheses is underestimated when the measurements are made on radiographs obtained in supine position as compared to weight-bearing position.
Patients and methods We examined 111 patients by radiostereometric analysis (RSA) in the supine and weight-bearing positions.
Results The mean 3-D penetration was 0.68 mm (SD 0.58, range 0.04–3.05) for the supine position and 0.70 mm (SD 0.57, range 0.08–3.01) for the weight-bearing position. The correlation between supine and weight-bearing examinations was 0.99 (p < 0.001). The degree of penetration made no difference. There was no statistically significant difference as to whether the first examination was performed early, i.e. after 3 months, or after 12 months (p = 0.7).
Interpretation The small systematic difference in penetration values between the supine and the weight-bearing positions is of no clinical or methodological importance. ▪
The relationship between rapid polyethylene (PE) wear and osteolysis following total hip arthroplasty (THA) is well documented (Livermore et al. Citation1990, Dumbleton et al. Citation2002). Dumbleton concluded that an annual wear rate of between 0.1 and 0.2 mm implied a risk of osteolysis. There is controversy as to whether PE penetration of hip prostheses is underestimated when the measurements are made on radiographs obtained in supine position as compared to weight-bearing position.
Smith et al. (Citation1999) found that linear wear—also called penetration—was underestimated in standard radiographs taken in the supine position in comparison with results found for the weight-bearing position. In contrast, using a validated, computer-assisted method for the evaluation of plain radiographs, Moore et al. (Citation2000) found no difference between examinations made in the weight-bearing and supine positions.
We assessed whether PE penetration measurements obtained in the supine and weight bearing positions really differ when using the most precise noninvasive measuring technique available. We also evaluated whether the starting point for the wear measurements matters, and whether the measurement error was related to the degree of penetration.
Patients and methods
This prospective study was performed between 1998 and 2003. 111 patients (111 hips), previously enrolled in a randomized, clinical and radiostereometric study of the Elite Plus hip prosthesis, were entered into the present study as they appeared for their scheduled follow-up examinations at 3, 6, 12, 24 and 60 months postoperatively. When entering the studyand at the subsequent examinations, radiographs for RSA were obtained both with the patient supine and in standing position. This gave different starting points for the reference examination. 49 patients had a starting point at 2–4 months and 47 patients had a starting point at 11–14 months postoperatively. 14 patients had a starting point between 5 and 10 months, and 1 patient had it at 24 months. The patients in the study received written and oral information and consented to participate. The ethics committee of our university had approved the Elite Plus study.
The prosthesis, surgical technique and RSA
The patients were operated on in the supine position and the hip was exposed through a lateral approach without trochanteric osteotomy. The Elite Plus stem (DePuy, Warsaw, IN) with either a stainless steel or a zirconium oxide head was used. The acetabular component was a Charnley Ogee Hylamer or Enduron polyethylene socket (DePuy). Palacos with gentamycin bone cement was used in all cases.
8 (6–10) tantalum beads, 0.8 mm in diameter, were inserted into both the periacetabular bone and the proximal femur. 9 beads of the same diameter were implanted into the all-polyethylene socket. RSA was performed using the uniplanar technique (Selvik Citation1989). Radiographs were first obtained in the supine position and immediately thereafter in standing position with the patient bearing weight equally on both legs, with the back and pelvis straight against a Plexiglas support.The first radiographic examination of each patient wasused as reference examination. The reference examination and the last available examination were used to compare penetration into the PE between the supine and weight-bearing measurements.
The UmRSA software (RSA Biomedical, Umeå, Sweden) was then used to calculate the relative motion (between the examinations) of the center of the femoral head and the geometric center of gravity of the 8 markers in the socket. The displacement of the femoral head was calculated as total or 3-D (three-dimensional) displacement, i.e. the length of the resulting vector (Kärrholm et al. Citation1997). A limit of 0.2 mm (CI 99%) for significant PE penetration has previously been calculated from duplicate supine examinations (Önsten et al. Citation1998). The measurement error, between a micrometer “true value” and a value obtained by RSA using a phantom, has been calculated to be 0.010 mm (SD 0.15, accuracy 0.42) (von Schewelov et al. Citation2004).
Statistics
We used Student’s paired t-test for dependent samples to compare the results obtained in the standing and the supine position. Correlation and regression analyses of the penetration values were done. 95% confidence intervals were calculated. The value of the individual supine measurements was subtracted from that of the weight-bearing measurements, and the differences were plotted as a scatter plot according to Bland and Altman Citation(1986).
Results
The mean 3-D penetration, from all 111 measurements, was 0.68 mm (SD 0.58, range 0.04–3.05) for supine position and 0.70 mm (SD 0.57, range 0.08–3.01) for weight-bearing position (p = 0.007; paired t-test) at mean 31 (3–57) months from the start of examination and mean 38 (6–60) months postoperatively.
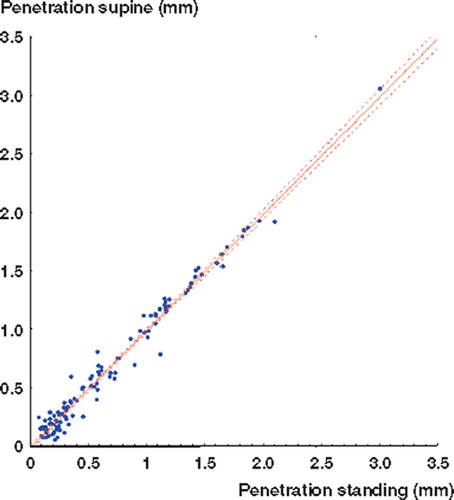
The correlation between the values obtained in the supine and the weight-bearing positions was r = 0.99 (p < 0.001), with regression coefficient = 0.98 (p < 0.001, ).
Figure 1. Polyethylene penetration in the supine and the weight-bearing positions.
Bland-Altman plots showing that the individual difference between weight-bearing and supine measurements is distributed evenly around the mean difference of 0.02 mm between the two groups with regard to (a) the time of the first examination, and (b) the degree of head penetration ().
Figure 2. The results of each individual supine result subtracted from the weight-bearing result. The difference has been plotted as a scatter-plot according to Bland and Altman Citation(1986). The line represents the mean difference (± 2 SD) between the supine and the weight bearing measurements. Left panel: The effect of time for the first (reference) examination. (One result with reference examination at 24 months with the mean difference 0.002 mm has not been plotted on the graph). Right panel: Effect of the degree of head penetration into the polyethylene.
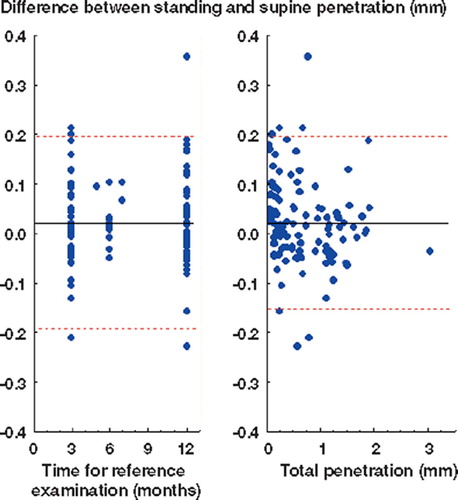
There was no difference whether the first reference examination was performed early, i.e. after 3 (2–4) months, or later, i.e. after 12 (11–14) months (). The mean difference between supine and weight-bearing results was 0.02 mm (CI −0.007–0.04) with 3 months as reference examination and 0.02 mm (CI−0.004–0.05) with 12 months as reference examination. The mean difference between the measurements using 3 and 12 months as reference examination was 0.007 (CI −0.04–0.03) (p = 0.7; independent t-test by group).
The number of measurable tantalum beads and configuration number were marginally lower in the weight-bearing group
RSA quality factors: mean number of measurable tantalum beads, mean configuration number, and mean error of the RSA examinations for weight-bearing and supine examinations. N = 111
Discussion
In this RSA study, we found that it is adequate to use radiographs acquired in the supine position for measurement of wear/penetration in all PE hip sockets. The difference between the mean penetration values obtained in the supine and weight-bearing positions was as low as 0.02 mm, and well below the error of the method. The correlation between the values obtained in the supine and weight-bearing positions was strong (r = 0.99) and the Bland-Altman scatter plots show that the differences between the supine and the weight-bearing measurements are equally distributed around the mean value (). Although statistically significant, the systematic difference only has the implication that a penetration of 1 mm in the supine position at 10 years will be underestimated as 0.98 mm and the annual wear underestimated as 0.098 instead of 0.1mm. Thus, the small systematic difference between supine and weight-bearing wear measurements can be disregarded. Our results are at least valid for penetrations ranging from 0–2 mm, but not unlikely also for penetration values above 2 mm.
Our findings are applicable to any other radiographic method used to measure head penetration, irrespective of the precision of that method. Thus, in the evaluation of new prosthetic designs, supine wear measurements must be adequate to show abnormal annual wear rates.
Whether the reference examination was performed at 3 months or after 12 months postoperatively had no influence on our results. Unfortunately, it is not possible to perform RSA examinations in the weight-bearing position immediately after surgery for humanitarian and technical reasons, which was also concluded by Digas et al. (Citation2003). Thus, from our study we cannot demonstrate whether penetration measurements based on radiographs obtained in the supine position shortly after surgery are correct. Digas et al. (Citation2003) studied wear, using the RSA technique, for two types of polyethylene. The 61 hips in the Digas study were examined in both the supine and the weight-bearing positions, but the reference examinations were performed at different time points—the supine examinations after 7 days and the weight-bearing examinations after 3 months. The authors found a mean linear wear or penetration at 24 months of 0.06 and 0.13 mm (0.07 mm, p = 0.03), respectively, for the two PE types, when measured on radiographs obtained in the weight-bearing position. Thus, these results did not include the first 3 months. The mean wear in the supine position was 0.13 and 0.18 mm (p = 0.08), respectively, which included the first 3 months of “wearin” or cold flow. Digas et al. (Citation2003) concluded that the difference in mean wear between the groups, measured in the supine position, did not reach statistical significance whereas it did in the weight-bearing position. The head penetration at 3 months measured in the supine position was approximately 0.06 mm. If 0.06 mm is subtracted from the results of the measurements in the supine position, we find that wear measured in the supine position for the first PE would be 0.07, and it was 0.06 with weight bearing. The corresponding values were 0.13 and 0.12 for the second PE. Linear wear or penetration is the result of measurement error, initial creep and true wear. The follow-up time in the Digas study was 2 years, and thus the effect of initial creep constitutes a major part of the reported head penetration measured in the supine position.
Most wear studies are based on immediate post-operative examinations. This may produce erroneous results due to initial creep and presumed lack of muscle tension, etc. Thus, we consider that the 3 or 12-month examination should serve as reference examination for measurements of linear wear/penetration in total hip prostheses.
It has been suggested that wear is often multidirectional (Akisue et al. Citation1999) and that the tension over the joint should decrease with more advanced wear. If this were true, the difference in wear between supine and weight-bearing examinations would increase. However, this was not the case in our study ( and ).
Smith et al. (Citation1999) studied wear in 23 patients with hip arthroplasty. The first immediate postoperative radiograph in the supine position was used as reference for the subsequent supine and weight-bearing examinations. The films were measured by two methods, the Livermore et al. (Citation1990) and the Scheier and Sandel (Citation1976) methods. An “arbitrary” limit for “significant difference between lying and standing” of 0.05 mm per year was introduced. The number of measurements with significant differences was then used for statistical comparison, and Smith and co-workers thus found a “clinically significant underestimation (p < 0.05)”; they also suggested two reasons for this underestimation. Firstly, a change in pelvic orientation, when weight bearing, ensures that the thinnest polyethylene is brought into relief, i.e. the thinnest part of the PE is brought into contour on the radiograph. As RSA is a three-dimensional examination, it is not dependent on the orientation of the pelvis. Secondly, the authors put forward that the head of the femoral component assumes the position of maximal displacement along its wear path when the radiograph is taken during weight bearing. To use the first postoperative supine examination as a reference for the following one(s), both supine and weight-bearing positions can be questioned. It is unclear to us how the “arbitrary significant difference” was chosen. Using simultaneous double examinations of supine and weight-bearing wear measurements over time, we could not find any clinically relevant difference that could support the findings of Smith and co-workers. Their results are also contradicted by the results published by Moore et al. (Citation2000), who examined radiographs of 47 hip arthroplasties. The radiographs had been obtained on the same occasion, with the patient both in the supine, standing and various other positions in order to determine how the femoral head changed position in the cup under different loading conditions. The authors found no difference in linear wear between the examinations, regardless of the position of the pelvis or whether or not the radiographs were obtained in the weight-bearing position. Methodological differences most likely explain the different conclusions reached in the studies of Smith et al. (Citation1999), Moore et al. (Citation2000), Digas et al. (Citation2003) and the study presented here.
We conclude that there is no reason to perform penetration measurements from radiographs obtained in the weight-bearing position, at least not if the measurements are initiated 3 months after surgery at the earliest. Furthermore, measurements of PE penetration in total hip arthroplasty are not sensitive to the degree of wear, at least not up to about 2 mm of PE penetration in our study.
We are grateful to Jan-Åke Nilsson, senior statistician at the Department of Internal Medicine, Malmö University Hospital, for invaluable advice.
No competing interests declared
Author contributions
Study design TvS, IÖ. Surgery TvS, IÖ, ÅC. Measurements PM, TvS. Material preparation and statistics TvS. Manuscript TvS, ÅC.
- Akisue T, Bauer T W, Yamaguchi M, Matejczyk M B, Stilberg B N. Multidirectional deformation in fully congruent acetabular components. J Arthroplasty 1999; 14: 1011–8
- Bland J, Altman D. Statistical methods for assessing agreement between two methods of clinical measurement Lancet. Feb 8, 1986; 307–10
- Digas G, Kärrholm J, Thanner J, Malchau H, Herberts P. Highly cross-linked polyethylene in cemented THA. Clin Orthop 2003, 417: 126–38
- Dumbleton J, Manley M, Edidin A. A literature review of the association between wear rate and osteolysis in total hip arthroplasty. J Arthroplasty 2002; 17: 649–61
- Kärrholm J, Herberts P, Hultmark P, Malchau H, Nivbrandt B, Thanner J. Radiosterometry of Hip protheses. Review of methodology and clinical results. Clin Orthop 1997; 344: 94–110
- Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg (Am) 1990; 72: 518–28
- Moore K D, Barrack R L, Sychterz C J, Jaswin S, Yang A M, Engh C A. The Effect of weight-bearing on the Radiographic measurement of the position of the femoral head after total hip arthroplasty. J Bone Joint Surg (Am) 2000; 82(1)62–9
- Önsten I, Carlsson A S, Besjakov J. Wear in uncemented porous and cemented polyethylene sockets. J Bone Joint Surg (Br) 1998; 80(2)345–50
- Scheier H, Sandel J. Wear affecting the plastic cup in metalplastic endoprostheses. N Gschwend, H U Debrunner. Hans Huber, Bern 1976; 186–90, In: Total hip prosthesis
- Selvik G. Roentgen stereophotogrammetry. A method for the study of kinematics of the skeletal system. Acta Orthop Scand (Suppl 232) 1989; 60
- Smith P N, Ling R S M, Taylor R. The influence of weight-bearing on the measurement of polyethylene wear in THA. J Bone Joint Surg (Br) 1999; 81(2)259–65
- von Schewelov T, Sanzén L, Börlin N, Markusson P, Önsten I. Accuracy of radiographic and radiostereometric wear measurement of different hip prostheses An experimental study. Acta Orthop Scand 2004; 75(6)691–700