
Abstract
Background and purpose — Implant inducible micromotions have been suggested to reflect the quality of the fixation interface. We investigated the usability of dynamic RSA for evaluation of inducible micromotions of the Oxford Unicompartmental Knee Arthroplasty (UKA) tibial component, and evaluated factors that have been suggested to compromise the fixation, such as fixation method, component alignment, and radiolucent lines (RLLs).
Patients and methods — 15 patients (12 men) with a mean age of 69 (55–86) years, with an Oxford UKA (7 cemented), were studied after a mean time in situ of 4.4 (3.6–5.1) years. 4 had tibial RLLs. Each patient was recorded with dynamic RSA (10 frames/second) during a step-up/step-down motion. Inducible micromotions were calculated for the tibial component with respect to the tibia bone. Postoperative component alignment was measured with model-based RSA and RLLs were measured on screened radiographs.
Results — All tibial components showed inducible micromotions as a function of the step-cycle motion with a mean subsidence of up to −0.06 mm (95% CI: −0.10 to −0.03). Tibial component inducible micromotions were similar for cemented fixation and cementless fixation. Patients with tibial RLLs had 0.5° (95% CI: 0.18–0.81) greater inducible medio-lateral tilt of the tibial component. There was a correlation between postoperative posterior slope of the tibial plateau and inducible anterior-posterior tilt.
Interpretation — All patients had inducible micromotions of the tibial component during step-cycle motion. RLLs and a high posterior slope increased the magnitude of inducible micromotions. This suggests that dynamic RSA is a valuable clinical tool for the evaluation of functional implant fixation.
Conventional radiostereometric analysis (RSA) has proven valuable in the evaluation of fixation for hip and knee arthroplasty, as early RSA evaluations have shown high predictive value for later aseptic component loosening (Kärrholm et al. Citation1994, Ryd et al. Citation1995, Nieuwenhuijse et al. Citation2012, Pijls et al. Citation2012). As an alternative to measure component migration over time, RSA has been used to measure real-time inducible component micromotion, defined as "reversible motion of the prosthesis relative to the bone induced by external force" (Toksvig-Larsen et al. Citation1998). The magnitude of component inducible micromotion has been suggested to reflect the development and quality of the prosthesis—bone/cement—bone fixation interface (Hilding et al. Citation1995, Regnér et al. Citation2000, Uvehammer Citation2001). Inducible micromotion of knee prostheses has previously been measured under static loaded conditions or during limited range of motion (Hilding et al. Citation1995, Toksvig-Larsen et al. Citation1998, Bragonzoni et al. Citation2005, Digas et al. Citation2013).
Currently, RSA is developing towards pulsed synchronized exposures with higher frame rates and a larger recording area (dynamic RSA), which makes the method ideal for evaluation of inducible micromotions during normal loaded functions. This may provide a better understanding of factors that compromise implant fixation (Kärrholm et al. Citation2006). Some of the main factors that have been suggested to affect the fixation of Oxford UKA are: component alignment, the fixation method, and the development of periprosthetic radiolucent lines (RLLs) (Aleto et al. Citation2008, Pandit et al. Citation2009, Gray et al. Citation2010, Kendrick et al. Citation2012, Citation2015, Small et al. Citation2013).
The purpose of this study was to investigate the usability of dynamic RSA for the evaluation of inducible micromotions of the Oxford UKA tibial component during a step-up and step-down motion, and to evaluate factors that have been suggested to compromise the fixation interface. We evaluated inducible micromotions for (1) fixation methods (cemented vs. cementless), (2) component alignment, (3) tibial RLLs, and (4) clinical outcome.
Patients and methods
Participants ()
Table 1. Patient demographics of the cemented and cementless Oxford UKA groups, taking account of the presence of tibial RLLs
15 patients from a randomized multicenter study regarding long-term fixation of cemented and cementless hydroxyapatite-coated Oxford UKA (Biomet Inc., Warsaw, IN) accepted an invitation to this cross-sectional study. The patient group in the randomized multicenter study consisted of 79 individuals who all underwent UKA surgery in the period 2009–2011. Since their surgery, they had been followed with RSA and screened radiographs to determine implant migration of the tibial component and RLLs. The 2-year RSA data, which were available at patient recruitment, showed no excessive migration, but the 5-year follow-up that followed showed that 1 of the 15 patients had continuous migration (unpublished data; Clinical Trials: NCT00679120).
24 patients (10 cementless and 14 cemented) were invited and 9 declined; the other 15 were evaluated after we had obtained informed consent. The inclusion criteria for this cross-sectional study were being mobile (having no problem with 30-cm step-up), having good marker distribution (condition number (CN) < 80), and having given informed consent. In addition, we attempted to include patients with tibial RLLs and an equal number with cemented and cementless fixation.
Dynamic RSA ()
Table 2. Methodological results of dynamic RSA on all 15 patients
Set-up
The dynamic RSA set-up consisted of a direct digital dedicated stereo X-ray system (AdoraRSA suite; NRT, Aarhus, Denmark). 2 ceiling-mounted X-ray tubes with automatic positioning were set horizontally at 40 degrees with respect to each other, and the distance between the tubes and detectors was set at the maximum of 330 cm to obtain the largest possible recording area (exercise zone for the patient). The 2 digital X-ray image detectors (CXDI-70C; Canon, Tokyo, Japan) where slotted behind a uniplanar carbon-fiber calibration box (Carbon Box 14; Medis Medical Imaging Systems BV, Leiden, the Netherlands). The resolution of the dynamic images was 79 dpi.
Recordings
Each patient was recorded with dynamic RSA (10 frames/s) during a continuous in-plane step-up and step-down motion (step-cycle motion) on a 30-cm box. The step-cycle motion was performed single-legged with the operated leg at self-selected speed (). This resulted in unequal numbers of measurement frames between patients.
Figure 1. An overview of the dynamic RSA set-up for the step-cycle motion (with the patient standing in the initial unloaded starting position for the step-up motion). a. The orientation of the Oxford UKA. b. The component-specific reference axis of the tibial component used for the RSA analysis.
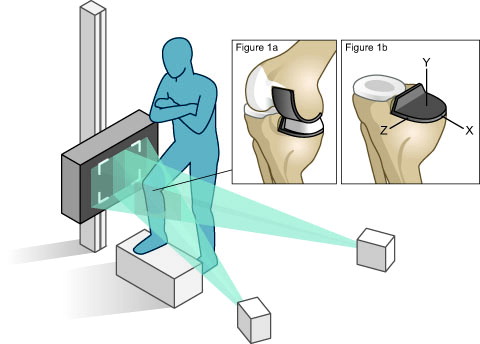
During the recordings, great effort was made to correct patient positioning, assisted by built-in laser guidance, ensuring a standardized set-up. 2 balance-railings ensured patient safety. The recordings were obtained as a DICOM file and converted to high-quality JPEG images using Matlab 2014b (The MathWorks Inc., Natick, MA).
Model-based RSA analysis
Model-based RSA version 4.01 (RSAcore; LUMC, Leiden, the Netherlands) was used for analysis of the recordings. Each patient recording was calibrated using the first frame, and a patient-specific marker configuration model (MC model) of the tibial bone markers was constructed. The MC model makes the RSA analysis more robust regarding occluded markers (Kaptein et al. Citation2005). The method assumes a proper accuracy of the MC model; thus, each model was checked visually for errors using 3 different frames. CAD models of the tibial component were provided by Biomet Inc.
For each RSA frame, micromotions of the tibial component with respect to the tibia bone (MC model), were computed using 3 different unloaded reference RSA frames. These unloaded reference frames were selected from the unloaded starting position (). This procedure was used to reduce the effect of the random error in the reference RSA frame on the micromotion results. The inducible micromotions are expressed as translations, rotations, and maximum total point motion (MTPM) with respect to the tibial component (). MTPM is defined as the amount of translation of the surface point of the tibial component model with the largest translation vector (Valstar et al. Citation2005). For a left-sided knee, the X-translations and the Z-rotations were mirrored to reflect a right-sided knee (ISO Citation2013).
Precision analysis
The 3 unloaded reference frames were used as "double exposures" in order to approximate the precision. The precision analysis was performed pairwise: 1-2, 2-3, 3-1 ().
Table 3. Tibial component precision analysis (n = 15) based on pairwise analysis of the 3 unloaded reference framesTable Footnotea
Quantification of tibia inducible micromotions
For the purpose of data quantification, we described the inducible micromotions as a function of percent step-cycle motion (step-up: 0–50%; step-down: 50–100%) and calculated the mean inducible micromotion (MIM) for each centile interval (0–10%, 10–20%, etc.). MIMs were calculated from a minimum of 2 measurement frames and a maximum of 4, and were used in further statistical analysis.
To describe the maximal total amount of inducible micromotion for each patient, we calculated the range of the MIMs for each migration parameter for the complete step-cycle motion. This summation measure will be denoted the maximal total inducible micromotion (MTIM).
Radiographic outcome measures ()
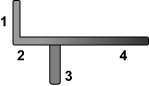
Screened radiographs from the 5-year follow-up were used to detect RLLs beneath the tibial tray. A radiologist (LR) performed all the measurements and an RLL was noted when radiolucency was ≥1 mm thick. Tibial RLLs were divided into 4 regions: (1) adjacent to the vertical wall, (2) lateral flat region, (3) adjacent to the vertical stem, and (4) medial flat region (). The 4 cases with tibial RLLs were treated as one group in the analysis.
Figure 2. AP view of the Oxford tibial component, illustrating the regions used for RLL registration.
Posterior slope and varus slope of the tibial component were measured in the postoperative RSA examination by calculating the relative angle between the tibial component and the anatomical axis of the tibia bone using model-based RSA. For this, we used the 3D orientation of the tibial CAD model and the anatomical axis of the tibia bone, which was found by fitting an EGS cone model to the proximal tubular tibia bone (Kaptein et al. Citation2006).
Clinical outcome measures
Oxford knee score (OKS; range: 0–48), visual analog pain score (VAS; range: 0–10), and American Knee Society score (AKSS; knee score: range 0–100; function score: range 0–100) were recorded for all patients on the same day as the examination with dynamic RSA (Dawson et al. Citation1998). 2 pain VAS scores were evaluated: 1 for rest and 1 for everyday activities.
Statistics
We considered the most important test parameters to be Y-translations (subsidence), Z-rotations (medio-lateral tilt), and X-rotations (anterior-posterior tilt). Repeated-measures ANOVA (with Greenhouse-Geiser corrections) were used to test whether the step-cycle motion had a statistically significant effect on MIMs. Repeated-measures ANOVA F-statistics will be reported as: F(dftime, dferror) = F-value (p-value). 2-sample Satterthwaite t-tests were used to compare the magnitude of the MTIMs between the cemented group and the cementless group, and between patients with and without tibial RLLs. Gaussian distributions were evaluated in QQ-plots. Spearman’s rho was used to test for correlations between the MTIMs and component alignment and between MTIMs and clinical outcome scores. 95% confidence intervals (CIs) were calculated for component alignment, MTIMs, and MIMs. Any p-values less than 0.05 were considered statistically significant. All analyses and graphs were computed using Stata 13.0 software.
Ethics and registration
Approval for the study was obtained from the local ethics committee (1-10-72-285-14; d. 11/11/2014) and the Data Protection Agency (1-16-02-470-14; d. 01/09/2014), and the study was carried out in line with the Helsinki Declaration (II). Detailed information and inclusion criteria for the randomized study can be found at ClinicalTrials.gov (Clinical Trials identifier: NCT00679120).
Results
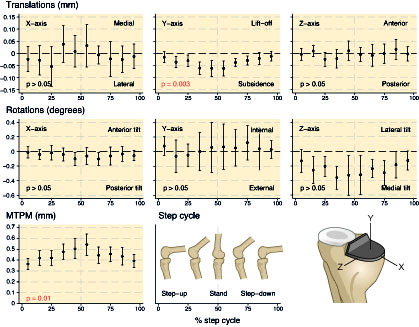
The step-cycle motion had a statistically significant effect on tibial component inducible micromotions in all 15 knees. Inducible micromotions were represented in Y-translations (subsidence) F(5, 69) = 4 (p = 0.003) and MTPM F(3, 44) = 4 (p = 0.01) (). The largest MIM was −0.06 mm subsidence (CI: −0.10 to −0.03) and 0.54 mm MTPM (CI: 0.44–0.65) for centile interval 50–60% (stand-phase). After a sensitivity analysis (removing the patients with continuous migration), these results were still evident (p ≤ 0.01).
Figure 3. Graphs presenting the mean inducible micromotions (MIMs) of all migration parameters as a function of the % step-cycle motion for the overall patient group (n = 15) with 95% CIs. The p-values are derived from repeated-measures ANOVA tests.
Fixation method
There was no statistically significant difference in MTIMs between the cemented group and the cementless group (p ≥ 0.2) ().
Table 4. Mean difference in the maximal total inducible micromotions (MTIMs) for cemented and cementless Oxford UKAs and patients with and without tibial radiolucent lines (RLLs)
Tibial radiolucent lines
The 4 patients with RLLs (n = 2 cemented, n = 2 cementless) all had 1- to 2-mm partial RLLs located at the vertical wall (region 1). 1 patient had a 1-mm RLL in region 2 (cemented) and 1 patient had a 1-mm RLL in region 3 (cementless). On average, patients with tibial RLLs had 0.5° (CI: 0.18–0.81) greater MTIM medio-lateral tilt (Z-rotations) than patients without tibial RLLs (p = 0.01) ().
Component alignment
Mean postoperative posterior slope of the tibial components was 5° (CI: 3–8). A positive correlation (r = 0.7, p = 0.01) was found between the degree of posterior slope and the MTIM anterior-posterior tilt (X-rotations). The patient with the most extreme degree of posterior slope (12°) had 0.83° of MTIM anterior-posterior tilt during the step-cycle motion, which was considerably greater than the mean MTIM (n = 15) of 0.34° (CI: 0.23–0.44). This particular patient also had pain during daily activities (VAS =4), tibial RLLs, and was measured with continuous migration of 1.3 mm between the 2- and 5-year follow-up (conventional RSA).
Mean varus slope was 6° (CI: 4–7), and there was no statistically significant correlation with MTIMs (r ≤ 0.4, p ≥ 0.2).
Clinical outcome scores
14 of the 15 patients were very satisfied with the Oxford UKA (as measured with AKSS). None of the patients had pain during rest, although 3 patients had pain during everyday activities (2 with VAS =4 and 1 with VAS =3). There was no statistically significant correlation between pain and MTIM (r ≤ 0.4, p ≥ 0.1). Likewise, AKSS and OKS were not statistically significantly correlated with MTIMs (r ≤ 0.5, p ≥ 0.1); nor was age, sex, or BMI (r ≤ 0.5, p ≥ 0.1).
Discussion
We have shown that cemented and cementless Oxford UKA tibial components have inducible micromotions as a function of the step-cycle motion, and that the magnitude of the inducible micromotions increases with the presence of RLLs and the degree of posterior slope. These findings support the use of dynamic RSA for the evaluation of inducible micromotions and for assessment of factors that have been suggested to compromise the fixation of the Oxford UKA tibial component.
The micromotions measured were very small and often below the precision attainable, which ranged from 0.11 to 0.34 mm for translations and from 0.36 to 0.88° for rotations. Yet, a valid and statistically significant result can still be obtained when enough measurements are made.
The accuracy of dynamic model-based RSA is complex, as inaccurate surface models may cause different fitting errors, depending on the pose of the implant (Kaptein et al. Citation2003). A phantom experiment performed before this study did not show systematic bias when the Oxford UKA was evaluated under automated bicycle motions using exactly the same set-up (unpublished data). Nevertheless, it is crucial to evaluate the direction of inducible micromotions and the biomechanical rationale.
We found that tibial component inducible micromotions were represented as subsidence and MTPM for the overall patient group. Subsidence is to be expected, since the Oxford UKA has a fully congruent design with a mobile bearing to minimize shear force and induce compressive loading (Simpson et al. Citation2008, Kendrick et al. Citation2015). It is, however, surprising that subsidence followed a quadratic trend with a maximum during stand-phase, as one would expect the peak during the mid-phase of step-up and step-down, due to the muscle forces applied to the tibial plateau (Zhao et al. Citation2007). An explanation could be that a stable fixation interface acts like a spring, from which the implant only subsides until a certain point—and that it occurs gradually with the outflow of fluid in the fixation interface. Another explanation could be that the muscle forces apply more load to the natural condyle during the initial phase, while with a straight knee the muscles relax a bit, causing the load to be applied to the prosthetic condyle.
MTPMs were considerably greater than subsidence and followed a similar trend. Larger values of MTPM are to be expected, as it represents the largest translation vector of the tibial component and includes the noise of both translations and rotations (Valstar et al. Citation2005).
We did not find statistically significant anterior-posterior or medio-lateral tilt in the overall patient group. This was unexpected, as sliding of the mobile bearing induces edge-loading of the tibial component.
The measured subsidence and MTPM are probably of benign nature, as all patients except 1 had a stable and mature fixation, as judged from the 5-year follow-up conventional RSA. Still, it is theoretically better to have as small magnitudes of inducible micromotions as possible since they are thought to fatigue the cement, inhibit bony ingrowth, and reflect the quality of the fixation interface (Pilliar et al. Citation1986, Hilding et al. Citation1995, Jasty et al. Citation1997, Regnér et al. Citation2000, Uvehammer and Kärrholm Citation2001, Cristofolini et al. Citation2008).
We found similar magnitudes of inducible micromotions for the cemented and cementless Oxford UKA, which is in line with recent publications that also found no difference in fixation properties after the first year (Pandit et al. Citation2009, Akan et al. Citation2013, Kendrick et al. Citation2015).
The 0.5° greater magnitudes of medio-lateral tilt in patients with RLLs compared to patients without RLLs seem logical, as RLLs represent fibro-cartilaginous interposition in the fixation interface. This is thought to reflect suboptimal fixation and increased stress in the underlying bone (Gray et al. Citation2010, Kendrick et al. Citation2012). Also, the RLLs were mainly located adjacent to the lateral vertical wall, which corresponds well with the medio-lateral tilt motion.
The correlation between the degree of posterior slope and the magnitude of inducible anterior-posterior tilt is interesting, as there is a good biomechanical explanation. A study evaluating Oxford UKA tibial load in 60 tibial composite Sawbones measured a large increase in posterior strain immediately distal to the prosthesis when the tibial component was implanted with a posterior slope of 5° and beyond (Small et al. Citation2013). Similar findings were obtained by Sawatari et al. (Citation2005). Aleto et al. (Citation2008) observed that posterior collapsing of UKA tibial components was associated with a mean posterior slope of 12°.
There are different reports in the literature on the extend to which inducible micromotions are caused by the properties of the fixation interface (implant-cement or cement-bone/prosthesis-bone) or the elastic properties of the bone. Toksvig-Larsen et al. (Citation1998) observed that the size of inducible micromotions did not change after the formation of the fibrous tissue, and concluded that inducible micromotions were partly due to the elastic properties of the bone. Other studies have suggested that micromotion mainly occurs in the fixation interface (Ryd et al. Citation1987, Regnér et al. Citation2000). In our study, at least some of the inducible micromotions happened in the RLLs and from the suboptimal loadings caused by increasing posterior slope. The clinical significance of these findings is unknown, although it does indicate a good agreement between the conditions of the implant (extreme malalignment, tibial RLLs) and the size of inducible micromotions. This is especially evident from the patient with the extreme posterior slope (12°), tibial RLL, and pain during activities, as very large anterior-posterior tilting motions were measured. The fact that this patient had considerable continuous migration supports this finding, and the tibial component was probably loose. This suggests that dynamic RSA is a useful clinical tool for the evaluation of the fixation of symptomatic implants.
We acknowledge that the study had limitations such as the small group size, the marginal group stratification, and that multiple hypothesis testing increased the risk of type-I and type-II error. However, it is important to emphasize that the purpose of this study was not to generalize the results, but to see whether dynamic RSA can be used to measure inducible micromotions and possible clinical problems.
It should also be noted that the summation measure used for hypothesis testing was the MTIM. MTIM solely represents the magnitude (range) of inducible micromotions and does not account for the trend or direction of motion. Furthermore, the precision provided is not based on true double examinations as stated in the ISO Citation2013 standard. True double examinations in dynamic RSA are difficult to obtain, as this requires 2 consecutive recordings matched at corresponding loading phases. This is problematic with regard to X-ray dosage, requires a lot of work, and complicates the precision analysis.
To summarize, all Oxford UKA tibial components had inducible micromotions represented as subsidence and MTPM. The inducible micromotions followed a clear trend, as they increased during the step-up motion and decreased during the step-down motion. There was no difference in the magnitude of inducible micromotions between cemented and cementless tibial components. The degree of posterior slope and the presence of partial radiolucent lines of ≥1 mm showed correlation to larger magnitude of inducible micromotions.
These findings advocate the use of dynamic RSA for the evaluation of inducible micromotions and component fixation in symptomatic implants. With further methodological advancements and the establishment of threshold values defining loose implants, dynamic RSA has the potential to become a valuable clinical tool.
KH, PBJ, BLK, and MS had the idea for the research and designed the study. KH performed the dynamic RSA examinations, performed RSA- and data analysis, and wrote the first draft of the article. MS, BLK, and PBJ helped with data analysis and interpretation. LR performed the radiological measurements. All the authors revised the draft manuscript.
The study was performed under the Danish Innovation Fund grant "Transforming radiological technology for assessment of implant fixation: from research tool to clinical application" (69-2013-1). We thank the reviewers for their excellent comments and suggestions, through which the quality of the paper has been substantially improved.
No competing interests declared.
Related Research Data
- Akan B, Karaguven D, Guclu B, Yildrim T, Kaya A, Armangil M, Cetin I. Cemented versus uncemented Oxford unicompartmental knee arthroplasty: is there a difference? Adv Orthop Hindawi Publ Corp 2013; (2013): 1–6.
- Aleto T J, Berend M E, Ritter M A, Faris P M, Meneghini R M. Early failure of unicompartmental knee arthroplasty leading to revision. J Arthroplasty 2008; 23 (2): 159–63.
- Bragonzoni L, Russo A, Loreti I, Montagna L, Visani A, Marcacci M. The stress-inducible displacement detected through RSA in non-migrating UKR. Knee 2005; 12 (4): 301–6.
- Cristofolini L, Affatato S, Erani P, Leardini W, Tigani D, Viceconti M. Long-term implant-bone fixation of the femoral component in total knee replacement. J Eng Med 2008; 222 (3): 319–31.
- Dawson J, Fitzpatrick R, Murray D W, Carr A. Questionnaire on the perceptions of patients about total knee replacement. J Bone Joint Surg (Br) 1998; 80–B (1): 63–9.
- Digas G, Johansson P, Kärrholm J. Inducible displacements of the cup and the femoral head during active range of motion: Dynamic RSA studies of cemented total hip replacements. J Orthop Res 2013; 31 (11): 1686–93.
- Gray H A, Zavatsky A B, Gill H S. The sclerotic line: Why it appears under knee replacements (a study based on the Oxford Knee). Clin Biomech 2010; 25 (3): 242–7.
- Hilding M B, Yuan X, Ryd L. The stability of three different cementless tibial components. A randomized radiostereometric study in 45 knee arthroplasty patients. Acta Orthop Scand 1995; 66 (1): 21–7.
- ISO. Implants for surgery — Roentgen stereophotogrammetric analysis for the assessment of migration of orthopedic implants. ISO 16087: 2013(E).
- Jasty M, Bragdon C R, Zalenski E, O’Connor D, Page A, Harris W H. Enhanced stability of uncemented canine femoral components by bone ingrowth into the porous coatings. J Arthroplasty 1997; 12 (1): 106–13.
- Kaptein B L, Valstar E R, Stoel B C, Rozing P M, Reiber J H C. A new model-based RSA method validated using CAD models and models from reversed engineering. J Biomech 2003; 36 (6): 873–82.
- Kaptein B L, Valstar E R, Stoel B C, Rozing P M, Reiber J H C. A new type of model-based Roentgen stereophotogrammetric analysis for solving the occluded marker problem. J Biomech 2005; 38 (11): 2330–4.
- Kaptein B L, Valstar E R, Cees W S, Berend C S, Piet M R. Model-based RSA of femoral hip stem using surface and geometrical shape models. Clin Orthop Relat Res 2006; (448): 92–7.
- Kärrholm J, Borssén B, Löwenhielm G, Snorrason F. Does early micromotion of femoral stem prostheses matter? 4-7-year stereoradiographic follow-up of 84 cemented prostheses. J Bone Joint Surg (Br) 1994; 76 (6): 912–7.
- Kärrholm J, Gill R H S, Valstar E R. The history and future of radiostereometric analysis. Clin Orthop Relat Res 2006; (448): 10–21.
- Kendrick B J L, James A R, Pandit H, Gill H S, Price A J, Blunn G W, et al. Histology of the bone-cement interface in retrieved Oxford unicompartmental knee replacements. Knee 2012; 19 (6): 918–22.
- Kendrick B J L, Kaptein B L, Valstar E R, Gill H S, Jackson W F M, Dodd C A F, Price A J, Murray D W. Cemented versus cementless Oxford unicompartmental knee arthroplasty using radiostereometric analysis: A randomised controlled trial. Bone Joint J 2015; 97-B (2): 185–91.
- Nieuwenhuijse M J, Valstar E R, Kaptein B L, Nelissen R G H H. Good diagnostic performance of early migration as a predictor of late aseptic loosening of acetabular cups - results from ten years of follow-up with roentgen stereophotogrammetric analysis (RSA). J Bone Joint Surg (Am) 2012; 94 (10): 874.
- Pandit H, Jenkins C, Beard D J, Gallagher J, Price A J, Dodd C A F, Goodfellow J W, Murray D W. Cementless Oxford unicompartmental knee replacement shows reduced radiolucency at one year. J Bone Joint Surg (Br) 2009; 91 (2): 185–9.
- Pijls B G, Valstar E R, Nouta K, Plevier J W, Fiocco M, Middeldorp S, Nelissen R G H H. Early migration of tibial components is associated with late revision: a systematic review and meta-analysis of 21,000 knee arthroplasties. Acta Orthop 2012; 83 (6): 614–24.
- Pilliar R M, Lee J M, Maniatopoulos C. Observations on the effect of movement on bone ingrowth into porous-surfaced implants. Clin Orthop Relat Res 1986; (208): 108–13.
- Regnér L, Carlsson L, Kärrholm J, Herberts P. Tibial component fixation in porous- and hydroxyapatite-coated total knee arthroplasty: a radiostereo metric evaluation of migration and inducible displacement after 5 years. J Arthroplasty 2000; 15 (6): 681–9.
- Ryd L, Lindstrand A, Rosenquist R, Selvik G. Micromotion of conventionally cemented all-polyethylene tibial components in total knee replacements. A roentgen stereophotogrammetric analysis of migration and inducible displacement. Arch Orthop Trauma Surg 1987; 106 (2): 82–8.
- Ryd L, Albrektsson B E J, Carlsson L, Dansgaard F, Herberts P, Lindstrand A, Regner L, Toksvig-Larsen S. Roentgen stereophotogrammetric analysis as a predictor of mechanical loosening of knee prostheses. Bone Joint Surg (Br) 1995; 77 (3): 377–83.
- Sawatari T, Tsumura H, Iesaka K, Furushiro Y, Torisu T. Three-dimensional finite element analysis of unicompartmental knee arthroplasty–the influence of tibial component inclination. J Orthop Res 2005; 23 (3): 549–54.
- Simpson D J, Gray H, D’Lima D, Murray D W, Gill H S. The effect of bearing congruency, thickness and alignment on the stresses in unicompartmental knee replacements. Clin Biomech 2008; 23 (9): 1148–57.
- Small S R, Berend M E, Rogge R D, Archer D B, Kingman A L, Ritter M A. Tibial loading after UKA: Evaluation of tibial slope, resection depth, medial shift and component rotation. J Arthroplasty 2013; 28 (2): 179–83.
- Toksvig-Larsen S, Ryd L, Lindstrand A. Early inducible displacement of tibial components in total knee prostheses inserted with and without cement: a randomized study with roentgen stereophotogrammetric analysis. J Bone Joint Surg (Am) 1998; 80 (1): 83–9.
- Uvehammer J. Knee joint kinematics, fixation and function related to joint area design in total knee arthroplasty. Acta Orthop 2001; 72 (Supplementum 299): 1–52.
- Uvehammer J, Kärrholm J. Inducible displacements of cemented tibial components during weight-bearing and knee extension observations during dynamic radiostereometry related to joint positions and 2 years history of migration in 16 TKR. J Orthop Res 2001; 19 (6): 1168–77.
- Valstar E R, Gill R, Ryd L, Flivik G, Börlin N, Kärrholm J. Guidelines for standardization of radiostereometry (RSA) of implants. Acta Orthop 2005; 76 (4): 563–72.
- Zhao D, Banks S A, D’Lima D D, Colwell C W, Fregly B J. In vivo medial and lateral tibial loads during dynamic and high flexion activities. J Orthop Res 2007; 25 (5): 593–602.