
ABSTRACT
This study investigated the effects of custom-fitted compression garments (CG) worn during recovery over a multi-day training camp in elite judo players (judoka). A single blind, placebo-controlled study was carried out in 11 elite judoka, using a two-way crossover design. Two three-day training camps were completed in CG and placebo conditions in a random order. Changes in performance and physiological markers were compared between conditions. Judoka were assessed before training for (maximal) isometric knee extension and grip strength, countermovement jump performance and bench-press velocity, alongside soreness, limb circumferences, plasma creatine kinase activity (CK) and perceived bruising. Measurements were repeated after 12, 36 and 43 h of training, whereupon judoka rated the effectiveness of each intervention. Knee extension and bench-press performance demonstrated significant familiarization (p < 0.001), and were excluded from subsequent analysis. Jump performance was unaffected by training (p > 0.05). Grip strength declined throughout training (p < 0.001), with peak decrements of −9.7% indicating mild muscle damage. Increases in bruising, CK and soreness demonstrated highly variable, if significant (p < 0.001) responses. Although CG were perceived as significantly more effective than placebo for recovery (p = 0.046), no effects were observed for any other outcome (p > 0.05). Compression conferred no statistically significant impact upon recovery markers in elite judoka throughout training. Muscle damage responses were inconsistent in this population. Individual athletes would be advised to monitor habitually-used performance measures while using CG to ascertain whether perceptual benefits translate into enhanced recovery.
Highlights
Compression garments were perceived as more effective for recovery than placebo by elite judoka.
However, no measures of performance or muscle damage were enhanced by CG.
Randori was associated with inconsistent muscle damage responses in elite judoka, while lower-body performance was not impaired.
Individual athletes would be advised to monitor habitually-used performance measures while using CG to ascertain whether perceptual benefits translate into enhanced recovery.
Introduction
Judo is a grappling sport in which prodigious levels of strength and power are required in the upper and lower body for success at the elite level (Bonitch-Góngora, Bonitch-Domínguez, Padial, & Feriche, Citation2012 Callister, Callister, Fleck, & Dudley, Citation1990;). Specifically, grip strength is considered to be a key performance indicator (Bonitch-Góngora et al., Citation2012; Franchini, Del Vecchio, Matsushigue, & Artioli, Citation2011; Kons et al., Citation2018), as establishing superiority in grip disputes increases the effectiveness of subsequent attacks (Courel-Ibáñez, Franchini, Femia, Stankovic, & Escobar-Molina, Citation2014). However, muscular performance in both the upper and lower body is demonstrably impaired following training and competition as a result of exercise-induced muscle damage (EIMD) (Bonitch-Góngora et al., Citation2012; Callister et al., Citation1990; Detanico, Dal, Franchini, Fukuda, & Dos, Citation2017). While the term EIMD describes observations of post-exercise myofibrillar disruption, this phenomenon may be functionally defined from the resulting reductions in isometric force that occur due to both structural and neuromuscular deficits (Owens, Twist, Cobley, Howatson, & Close, Citation2019). Importantly for athletes, impaired muscle function following EIMD may persist for several days alongside increased soreness, limb swelling and impaired mobility (Goto & Morishima, Citation2014; Owens et al., Citation2019).
Although athletes become less susceptible to EIMD following training (Falvo, Schilling, & Smith, Citation2010), competitive judoka may still suffer prolonged deficits in neuromuscular function following free sparring (or “randori”), which persist for at least 48 h alongside increases in soreness and circulating concentrations of intracellular enzymes (Detanico et al., Citation2017). Furthermore, even elite judoka (international representatives) have been shown to suffer reductions in isokinetic strength and running performance in the days following intensified training (Callister et al., Citation1990), as well as deterioration of isometric performance following successive matches (Bonitch-Góngora et al., Citation2012). As Olympic success requires five consecutive victories in a single day, and multi-day training camps are commonplace at the elite level (Laskowski, Ziemann, Olek, & Zembron-Lacny, Citation2011), the application of effective recovery strategies is a major objective in judo (Bonitch-Góngora et al., Citation2012; Laskowski et al., Citation2011).
The use of compression garments (CG) is a popular recovery strategy amongst athletes, and may be particularly effective for recovery from EIMD, with enhanced strength recovery frequently reported alongside ameliorated trauma, soreness and swelling (Brown et al., Citation2017; Goto & Morishima, Citation2014). However, no studies have been carried out to assess the effectiveness of CG for recovery in elite judoka. Furthermore, the benefits of CG for recovery in elite athletes have not been established, with a scarcity of data on exclusively elite performers. Additionally, whilst grip strength is a key determinant of success in judo (Bonitch-Góngora et al., Citation2012; Callister et al., Citation1990), no studies have been carried out to investigate the effects of CG on the recovery of this measure.
Optimal compression pressures for recovery have yet to be defined. Although a recent study on the lower body (Hill et al., Citation2017) reported superior recovery from clinical grade stockings (applying 24.3 ± 3.7 mmHg and 14.8 ± 2.2 mmHg at the calf and thigh, respectively) compared to commercially available CG (14.8 ± 2.1 mmHg and 8.1 ± 1.3 mmHg), the literature is otherwise largely equivocal (Beliard et al., Citation2015; Brown et al., Citation2017). The establishment of optimal pressures is further complicated by the scarcity of studies reporting directly measured values (Brown et al., Citation2017), with many studies reporting pressures predicted by manufacturers or estimated from mathematical modelling (Brown et al., Citation2017; Kraemer et al., Citation2001). As portable pressure monitors that provide valid and reliable readings have become available over the last decade (Partsch & Mosti, Citation2010), the properties of CG can now be more accurately characterized. Furthermore, as CG sold in standard sizes may provide inconsistent compression pressures (Hill, Howatson, Van Someren, Davidson, & Pedlar, Citation2015), greater control may be achieved following recent developments in the manufacture of custom-fitted CG using 3D scanning technology (Kuzmichev & Cheng, Citation2020).
The present study was therefore carried out to investigate the effects of custom-fitted CG for recovery of neuromuscular function and muscle damage markers in both the upper and lower body over a multi-day training camp in elite judoka.
Materials and methods
Ethics approval was obtained from St Mary’s University research ethics committee. Eleven elite judoka (Great Britain representatives) provided informed consent and completed two three-day training camps using both CG (stockings and arm-sleeves) and placebo for recovery in a random order. Judoka were randomized into two groups via block randomization before the first trial, subsequently completing the alternative condition during the subsequent camp. Testing took place during two Olympic National Squad Training camps (ONST), over six months. Participating judoka had all medalled in the European championships at U23 level, and competed in (International) Grand Slam tournaments as seniors, with one athlete having competed at the Olympics and World Championships. Each ONST was preceded by one week of reduced training. Testing was carried out before training, then after 12, 36 and 43 h, to assess recovery ().
Figure 1 . Schematic of study design.
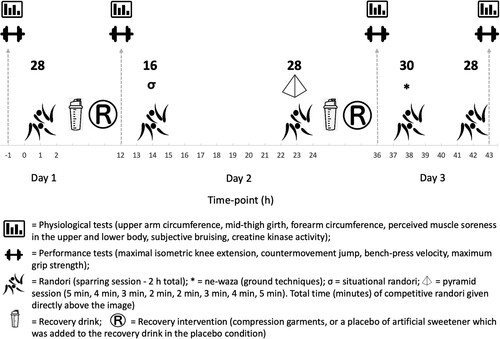
Scheduled training was identical for both camps (). Sessions lasted for 2 h in total, with periods of randori preceded by a guided warm up and technical practice, and followed by a group warm down. Throughout ONST, pairs of judoka would grapple and rest alternately, resulting in work:rest ratios ∼ 1:1. Judoka completed bouts of simulated competition in which all legal techniques could be utilized (“free” randori), as well as sessions designed to mimic specific competition scenarios (“situational” randori – ). Specifically, the sessions on Friday evening and Sunday afternoon comprised of 7 × 4 min bouts, while training on Saturday afternoon featured a “pyramid” session (bouts of 5 min duration, decreasing sequentially by a minute each round until 2 min, then back). Each of these sessions required 28 min of randori per judoka (). Sessions of situational randori, as well as ground fighting techniques (ne-waza) were completed on Saturday and Sunday mornings, respectively. These sessions involved 16 min (Saturday) and 30 min (Sunday) of randori per judoka ().
A single familiarization session was employed the week before the first trial for all tests of muscle function (Bonitch-Góngora et al., Citation2012 Goto & Morishima, Citation2014;) with the exception of grip strength which was habitually used as part of routine athlete monitoring. All testing was carried out without compression garments being worn. Judoka were assessed for upper and lower body soreness using a 200 mm visual analogue scale (Bell, Stevenson, Davison, & Howatson, Citation2016), with results then scaled from 0 to 10. Subsequently, relaxed limb circumferences were measured at the mid-thigh, bicep and forearm in accordance with the guidelines of the International Society of Anthropometry and Kinanthropometry (ISAK). All anthropometric measures were taken by an ISAK-qualified anthropometrist demonstrating coefficients of variation (CV) ≤ 2.5% for test-retest scores. Bruising was scored according to athletes’ habitual monitoring on a scale of 1–5 (5 indicating no bruising), before capillary blood samples (3–500 μl) were taken with a lithium heparin micro-cuvette (Microvette, Sarstedt, Leicester, UK) for the analysis of plasma creatine kinase activity (CK). Plasma was separated by centrifugation at 4°C at 3500 rpm for 10 min (Mikro 220R D-78532, Tuttlingen, Germany) and immediately frozen at −80°C. Analysis was carried out at a later date using a spectrophotometric assay with a between-run precision of 1.2% (CK-NAC, RX Daytona, Randox, County Antrim, Northern Ireland). Muscular function was then assessed from maximal voluntary isometric contraction (MVIC) of the knee extensors (MIE Medical Research Ltd., Leeds, UK), isometric grip strength (Takei Digital Hand-Grip Dynamometer 4001, Takei Scientific Instruments Co., Niigata-City, Japan), peak countermovement jump (CMJ) force (PS-2142, Pasco Scientific, Roseville, CA, USA) and mean bench-press bar-velocity with a load of 50% body-mass (PUSH band, PUSH Inc., Toronto, Canada). The best result from three attempts was reported, each separated by two minutes’ recovery. Assessment of MIVC was carried out for three seconds at 90° as measured with a goniometer, with judoka seated on a plyometric box. Grip strength was measured for three seconds in the favoured hand, with the elbow extended (Gatt, Smith-Moore, Steggles, & Loosemore, Citation2018). Countermovement jumps were performed with hands on hips, and judoka asked to jump as high as possible with no instruction on the depth of countermovement given. After ONST, judoka were asked to rate the effectiveness of recovery interventions out of 10 to the nearest 0.5, with 10 being defined as the “most effective recovery intervention imaginable”.
Recovery interventions were provided after the final daily training session on the first and second day of ONST. All athletes received a drink providing 15 g protein and 30 g carbohydrate (Arla Protein Shake, Arla Foods, Leeds, Yorkshire, UK) which was consumed immediately after training. In the placebo condition, a spoonful of sucralose-based sweetener (2 g carbohydrate, 0.1 g protein) was added to the shakes in plain sight, and judoka informed that the powder was a lactate-buffer designed to aid recovery (Splenda, Heartland Food Products Group, Carmel, Ind. USA.). In the CG condition, judoka wore custom-fitted full-length stockings and arm sleeves, which had been fitted previously following 3D scanning of the limbs (Isobar Compression, Manchester, UK). Compression pressures () were guided by existing literature (Brown et al., Citation2017; Hill et al., Citation2017). Athletes put on CG immediately after training and wore them overnight until the next day’s training session, being instructed to remove them only to wash. Compression pressures () were measured in a standing position (Kikuhime pressure Measuring System, Harada Corp, Osaka, Japan) at the medial calf, mid-thigh, medial malleolus, wrist and bicep landmarks as defined by ISAK.
Table 1. Participant characteristics.
All performance tests were assessed for learning effects by comparing baseline values recorded at each ONST with a related-samples t-test (SPSS Statistics 25, IBM, New York, USA), as well as comparing values between camps using a two-way, time (× 4) by ONST (× 2) related-samples analysis of variance (ANOVA). Results were discarded if familiarization occurred. Additionally, reliability was quantified from CV and intra-class correlation coefficient (ICC) values (Hopkins, Citation2000). Between-session reliability was calculated from the differences between peak values at baseline, while intra-session reliability was calculated from the differences between each of the athletes’ three attempts. Values for ICC were classed as “moderate”, “good”, or “excellent” if values fell between 0.4-0.59, 0.6 - 0.74 and 0.75–1 respectively (Cicchetti, Citation1994; Hopkins, Citation2000).
Data were assessed for normality by visually inspecting Q-Q plots run on residual values, before employing the Shapiro–Wilk test. Non-normal data were log-transformed and re-assessed, and parametric statistics employed where the assumption of normality was met. Between-condition differences for the recovery of all measures were subsequently assessed using a two-way, time (× 4) by condition (× 2) related-samples ANOVA. Significance was set a priori at p ≤ 0.05. Results were presented as means ± SD. Effect sizes (Cohen’s d) were reported as the difference between changes from baseline between conditions (ES [LCL, UCL]), where LCL and UCL represent the lower and upper 90% confidence limits (Batterham & Hopkins, Citation2006), except for soreness and bruising which were calculated from raw values. The threshold values for standardized changes were as follows: ≤ 0.2 (trivial), > 0.2 (small), > 0.5 (moderate), > 0.8 (large) (Batterham & Hopkins, Citation2006).
Results
Participant characteristics are presented in . There were no baseline differences between conditions for any variable (p > 0.05). Analysis of calculated residuals revealed that the assumption of normality was violated for CK data only. Accordingly, values for CK were log-transformed before analysis with parametric statistics, with all other variables being analysed from raw data.
Prior familiarization was insufficient for MVIC, as shown by greater baseline values at the second ONST (t = − 4.86, p = 0.001), and greater average values over the camp (F = 16.4, p = 0.002). Between-session reliability values for MVIC were CV = 8.3% and ICC = 0.84, while intra-session reliability was described by coefficients of CV = 7.3% and ICC = 0.83. Although baseline values for bench-press velocity did not improve significantly between trials (t = −1.87, p = 0.091; CV = 12.3% and ICC = 0.72), two-way ANOVA demonstrated that average velocity was greater over the second ONST (F = 9.15, p = 0.013). Within-session reliability for bench-press velocity was quantified as (CV = 7.2% and ICC = 0.87). These measures were therefore omitted from subsequent analysis, but included separately for readers’ information (Supplementary Table).
Jump performance was consistent between ONST, as shown by similar values at baseline (t = −1.582, p = 0.145; CV = 9.5%, ICC = 0.92), and throughout each camp (F = 2.86, p = 0.121). Furthermore, this measure demonstrated a high degree of intra-session reliability (CV = 4.2%, ICC = 0.94). However, jump performance was not subject to fatigue from training (F = 0.771, p = 0.519). In contrast, baseline measures of grip were shown to be reliable within sessions (CV = 6.4%, ICC = 0.95), between ONST (t = 0.45, p = 0.965; CV = 4.94%, ICC = 0.98), and to decline over training (F = 9.51, p < 0.001). The deterioration in grip strength throughout training was not different between ONST (F = 0.876, p = 0.464). However, this measure was not influenced by CG (F = 0.299, p = 0.826; ).
Table 2. The effect of custom-fitted compression garments on markers of muscle damage and performance over time.
The between-session reliability of mid-thigh, upper-arm and forearm circumference measurements was characterized by CVs of 2.4%, 3.1% and 2.7% respectively, with ICC values of 0.98, 0.96 and 0.96. Upper-arm (F = 3.89, p = 0.018), mid-thigh (F = 3.22 p = 0.036) and forearm (F = 8.48, p < 0.001) circumferences all changed significantly throughout training, although these changes were not affected by compression (). Bruising, CK, upper and lower body soreness all increased throughout ONST, with no significant effects from CG (). Following ONST, compression was perceived as significantly more effective than placebo for recovery (CG = 6.0 ± 1.0 arbitrary units, CON 5.0 ± 2.0 arbitrary units; t = 2.281, p = 0.046), which represented a large effect (ES = 0.84 [0.21, 1.46]).
Discussion
The principal finding of this study was that CG were ineffective for improving recovery in elite judoka when worn overnight between consecutive days of randori. Whilst this finding is discordant with the majority of evidence on the use of CG for strength recovery (Brown et al., Citation2017), key differences exist between the current study and those reporting positive outcomes. Firstly, it is possible that any damage incurred during ONST was insufficient to benefit from compression. This may have been due to the specific exercise employed, the highly trained status of the elite athletes studied, or a combination of these factors. For example, a previous study examining the effects of compression in highly trained hockey players also reported no benefit from CG when worn for 48 h following the Loughborough Intermittent Shuttle Test (LIST) (Pruscino, Halson, & Hargreaves, Citation2013). However, EIMD was insufficient to impair squat-jump performance in this sample. In the current trial, although grip strength declined 12 h after randori as is typical following EIMD (Khamwong, Nosaka, Pirunsan, & Paungmali, Citation2012 Souron, Nosaka, & Jubeau, Citation2018;), peak reductions of < 10% were far lower than those reported following eccentric wrist extensions in untrained participants (Khamwong et al., Citation2012) and instances in which CG have enhanced recovery (Brown et al., Citation2017; Goto & Morishima, Citation2014; Kraemer et al., Citation2001). Large standard deviations for CK and swelling responses (), also suggest muscle damage was inconsistent in this sample. Secondly, the deterioration of grip strength has previously been attributed to metabolic factors (Bonitch-Góngora et al., Citation2012; Callister et al., Citation1990; Laskowski et al., Citation2011), which may be less responsive to compression (Brown et al., Citation2017).
Importantly, although CG have been shown to attenuate EIMD in the thighs and upper arms (Brown et al., Citation2017 Goto & Morishima, Citation2014;), this is the first study to investigate the use of compression sleeves for next day recovery of grip strength. However, the physiological characteristics of specific muscles may vary in ways that could influence responses to both EIMD and compression. For instance, the muscles of the forearm contain a high proportion of type I fibres (Fugl-Meyer, Eriksson, Sjostrrim, & Soderstrom, Citation1982), which may be less susceptible to EIMD than type II (Friden & Lieber, Citation2001). As no studies have yet reported direct (e.g. histological) evidence of EIMD in the forearm, further research is required to provide mechanistic insight to better inform recovery interventions.
The lack of effects on grip strength may also be related to the failure of CG to ameliorate symptoms of inflammation. Whilst the functional benefits of compression are commonly associated with improved swelling and soreness throughout recovery (Brown et al., Citation2017 Goto & Morishima, Citation2014;), increases in both upper body soreness and forearm circumference were unaffected by CG (). While the reasons for this are unclear, differences with existing literature may be due to the elite athlete population studied, or the unique exercise challenge employed (randori). The lack of effects on strength and soreness may also be due to the pressures applied. Although the pressures selected for the present study were guided by previous trials (Hill et al., Citation2017 Partsch, Damstra, & Mosti, Citation2011;), optimal compression pressures for recovery are undefined, with no dose–response studies on recovery having been carried out in the upper body. Although insignificant, CG were also associated with a “moderate” increase in soreness at 43 h (0.74 [0.21, 1.21] – ). As clinical data suggests that increasing compression pressure might be harmful beyond an optimum (Partsch et al., Citation2011) it is therefore possible that applied pressures were excessive for optimal recovery in the upper body.
In the current study, CG were ineffective for moderating increases in limb circumference (). Such findings are in marked contrast with existing literature, in which CG have been consistently reported to attenuate swelling throughout recovery alongside improved functional outcomes (Brown et al., Citation2017; Goto & Morishima, Citation2014; Kraemer et al., Citation2001). Although the exact mechanisms by which CG aid recovery remain ambiguous, the observed null effects for both swelling and recovery may be related. Indeed, swelling and associated vascular stasis serve to increase the exposure of damaged tissue to leukocyte-rich wound fluid; propagating inflammation via increased leukocyte adhesion and cytotoxic activity (Paulsen, Mikkelsen, Raastad, & Peake, Citation2012; Valle et al., Citation2013). In support of this hypothesis, previous research has shown that wearing CG throughout downhill running significantly reduced subsequent leukocyte infiltration and morphological disruption (Valle et al., Citation2013). Interestingly, reductions in both inflammation (Beidler et al., Citation2009) and oxidative stress (Flore et al., Citation2007) have been reported alongside improvements in vascular function from compression in a clinical setting. However, there is currently insufficient data to establish whether EIMD is consistently associated with swelling in the forearm, with a recent study reporting impaired grip strength following eccentric wrist extensions with no concomitant change in forearm circumference (Khamwong et al., Citation2012). If CG do enhance recovery via anti-inflammatory mechanisms, such benefits may depend upon their capacity to ameliorate swelling.
Findings from the current trial may also be used to guide the selection of performance tests for monitoring EIMD in elite strength and power athletes. Although EIMD is functionally quantified from declines in isometric strength (Byrne & Eston, Citation2002), the MVIC protocol used in the current study was subject to significant learning effects between trials. This was despite an initial familiarization session (Toonstra & Mattacola, Citation2013), and four subsequent experimental tests between ONST. Field testing required that portable equipment was used without the capacity for restricting movement as with an isokinetic dynamometer. Despite instructing athletes to maintain a consistent posture, the lack of secure fastening might have allowed athletes to subtly alter their position and modify their technique. Indeed, even with the use of strapping, a previous study using a portable dynamometer reported that an average of 5 ± 2 sessions was required before a plateau was established in recreational athletes (Morton et al., Citation2005). Additionally, although this protocol has previously proved reliable and resistant to learning effects in untrained participants (Toonstra & Mattacola, Citation2013) our results may emphasize the need to consider the population-specific nature of reliability data (Di Fabio, Citation1999).
Whilst jump performance demonstrated a high degree of both between-session and intra-session reliability, this measure was not impaired by randori. As previous research suggests that movements involving the stretch-shortening cycle may be less affected by EIMD (Byrne & Eston, Citation2002), it is therefore unclear if this finding reflects a lack of meaningful neuromuscular impairment, or the insensitivity of this particular measure. This phenomenon may also have accentuated the learning effects observed for bench-press velocity. Although declines in grip strength are indicative of EIMD in the forearm, damage in other muscle groups was unclear. However, observed learning effects and the resilience of particular measures to EIMD may have obscured low levels of muscle damage. Future research is required to establish reliable, judo-specific tests of muscle function that are sensitive to EIMD in elite judoka.
Limitations
Whilst compression was perceived as significantly more effective for recovery than placebo, the absence of any other effects may simply suggest that blinding was ineffective. This represents a major limitation to the current study. Additionally, it is possible that training status may have differed between trials conducted at different points in the year, although any such variation had no effect on either grip or jump performance. Furthermore, logistical constraints prevented the collection of post-exercise measures after the first day of ONST. As post-exercise strength loss is a valid indicator of the severity of EIMD (Paulsen et al., Citation2012), such information may have helped better characterize fatigue. It was also not possible to directly quantify training load in this elite sport setting. As the sample was limited to elite judoka, the necessarily small sample size represents another important limitation.
Conclusion
Custom-fitted CG worn between bouts of randori were perceived as effective for recovery in elite judoka. However, no other outcome measures were influenced by compression. Accordingly, individual athletes would be advised to monitor performance responses while using CG to ascertain whether perceptual benefits of compression effectively translate to functional recovery. Future work should investigate the use of CG in this population for the recovery of habitually used tests of muscle function, or following thorough familiarization on at least five occasions. Further research is required to identify reliable, valid, and meaningful sports-specific tests that are sensitive to muscle damage in elite judoka.
Supplemental Material
Download MS Word (21.9 KB)Acknowledgments
Thanks to all of the athletes and staff at British Judo, and in particular Louise Bloor for helping coordinate the study. We would also like to acknowledge Isobar Compression for providing custom-fitted compression garments free of charge. No funding was received, nor potential conflict of interests highlighted by the authors.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Batterham, A. M., & Hopkins, W. G. (2006). Making meaningful inferences about magnitudes. International Journal of Sports Physiology and Performance, 2, 50–57.
- Beidler, S. K., Douillet, C. D., Berndt, D. F., Keagy, B. A., Rich, P. B., & Marston, W. A. (2009). Inflammatory cytokine levels in chronic venous insufficiency ulcer tissue before and after compression therapy. Journal of Vascular Surgery, 49, 1013–1020.
- Beliard, S., Chauveau, M., Moscatiello, T., Cros, F., Ecarnot, F., & Becker, F. (2015). Compression garments and exercise: No influence of pressure applied. Journal of Sports Science & Medicine, 14, 75–83.
- Bell, P., Stevenson, E., Davison, G., & Howatson, G. (2016). The effects of montmorency tart cherry concentrate supplementation on recovery following prolonged, intermittent exercise. Nutrients, 8, 441.
- Bonitch-Góngora, J. G., Bonitch-Domínguez, J. G., Padial, P., & Feriche, B. (2012). The effect of lactate concentration on the handgrip strength during judo bouts. The Journal of Strength & Conditioning Research, 26, 1863–1871.
- Brown, F., Gissane, C., Howatson, G., Van Someren, K., Pedlar, C., & Hill, J. (2017). Compression garments and recovery from exercise: A meta-analysis. Sports Medicine, 47, 2245–2267.
- Byrne, C., & Eston, R. (2002). The effect of exercise-induced muscle damage on isometric and dynamic knee extensor strength and vertical jump performance. Journal of Sports Sciences, 20, 417–425.
- Callister, R., Callister, R., Fleck, S., & Dudley, G. (1990). Physiological and performance responses to overtraining in elite judo athletes. Medicine & Science in Sports & Exercise, 22, 816–824.
- Cicchetti, D. V. (1994). Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychological Assessment, 6, 284.
- Courel-Ibáñez, J., Franchini, E., Femia, P., Stankovic, N., & Escobar-Molina, R. (2014). Effects of kumi-kata grip laterality and throwing side on attack effectiveness and combat result in elite judo athletes. International Journal of Performance Analysis in Sport, 14, 138–147.
- Detanico, D., Dal, J. P., Franchini, E., Fukuda, D. H., & Dos, S. S. (2017). Effects of traditional judo training session on muscle damage symptoms. The Journal of Sports Medicine and Physical Fitness, 57, 872–878.
- Di Fabio, R. P. (1999). Studies of reliability: Show me the question. Journal of Orthopaedic and Sports Physical Therapy, 29, 370–371.
- Falvo, M., Schilling, B., & Smith, A. (2010). Repeated bout effect is absent in resistance trained men. An electromyographic analysis. Journal of Electromyography and Kinesiology, 19, e529–e535.
- Flore, R., Gerardino, L., Santoliquido, A., Catananti, C., Pola, P., & Tondi, P. (2007). Reduction of oxidative stress by compression stockings in standing workers. Occupational Medicine, 57, 337–341.
- Franchini, E., Del Vecchio, F. B., Matsushigue, K. A., & Artioli, G. G. (2011). Physiological profiles of elite judo athletes. Sports Medicine, 41, 147–166.
- Friden, J., & Lieber, R. L. (2001). Eccentric exercise-induced injuries to contractile and cytoskeletal muscle fibre components. Acta Physiologica, 171, 321–326.
- Fugl-Meyer, A. R., Eriksson, A., Sjostrrim, M., & Soderstrom, G. (1982). Is muscle structure influenced by genetical or functional factors? A study of three forearm muscles. Acta Physiologica Scandinavica, 114, 277–281.
- Gatt, I., Smith-Moore, S., Steggles, C., & Loosemore, M. (2018). The takei handheld dynamometer: An effective clinical outcome measure tool for hand and wrist function in boxing. The Hand, 13, 319–324.
- Goto, K., & Morishima, T. (2014). Compression garment promotes muscular strength recovery after resistance exercise. Medicine & Science in Sports & Exercise, 46, 2265–2270.
- Hill, J. A., Howatson, G., Van Someren, K. A., Davidson, S., & Pedlar, C. R. (2015). The variation in pressures exerted by commercially available compression garments. Sports Engineering, 18, 115–121.
- Hill, J., Howatson, G., Van Someren, K., Gaze, D., Legg, H., Lineham, J., … Pedlar, C. (2017). Effects of compression garment pressure on recovery from strenuous exercise. International Journal of Sports Physiology and Performance, 12, 1–22.
- Hopkins, W. G. (2000). Measures of reliability in sports medicine and science. Sports Medicine, 30, 1–15.
- Khamwong, P., Nosaka, K., Pirunsan, U., & Paungmali, A. (2012). Prophylactic effect of hot pack on symptoms of eccentric exercise-induced muscle damage of the wrist extensors. European Journal of Sport Science, 12, 443–453.
- Kons, R. L., Dal Pupo, J., Ache-Dias, J., Garcia, T., Da Silva, R. R., Katicips, L. F. G., & Detanico, D. (2018). Effect of official judo matches on handgrip strength and perceptual responses. Journal of Exercise Rehabilitation, 14, 93.
- Kraemer, W. J., Bush, J. A., Wickham, R. B., Denegar, C. R., Gomez, A. L., Gotshalk, L. A., … Putukian, M. (2001). Continuous compression as an effective therapeutic intervention in treating eccentric-exercise-induced muscle soreness. Journal of Sport Rehabilitation, 10, 11–23.
- Kuzmichev, V., & Cheng, Z. (2020). Sizing and fit for pressure garments. Anthropometry, apparel sizing and design. Cambridge, UK. Woodhead Publishing.
- Laskowski, R., Ziemann, E., Olek, R. A., & Zembron-Lacny, A. (2011). The effect of three days of judo training sessions on the inflammatory response and oxidative stress markers. Journal of Human Kinetics, 30, 65–73.
- Morton, J. P., Atkinson, G., Maclaren, D. P., Cable, N. T., Gilbert, G., Broome, C., … Drust, B. (2005). Reliability of maximal muscle force and voluntary activation as markers of exercise-induced muscle damage. European Journal of Applied Physiology, 94, 541–548.
- Owens, D. J., Twist, C., Cobley, J. N., Howatson, G., & Close, G. L. (2019). Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? European Journal of Sport Science, 19, 71–85.
- Partsch, H., Damstra, R. J., & Mosti, G. (2011). Dose finding for an optimal compression pressure to reduce chronic edema of the extremities. International Angiology, 30, 527–533.
- Partsch, H., & Mosti, G. (2010). Comparison of three portable instruments to measure compression pressure. International Angiology: A Journal of the International Union of Angiology, 29, 426–430.
- Paulsen, G., Mikkelsen, U. R., Raastad, T., & Peake, J. M. (2012). Leucocytes, cytokines and satellite cells: What role do they play in muscle damage and regeneration following eccentric exercise? Exercise Immunology Review, 18, 42–97.
- Pruscino, C. L., Halson, S., & Hargreaves, M. (2013). Effects of compression garments on recovery following intermittent exercise. European Journal of Applied Physiology, 113, 1585–1596.
- Souron, R., Nosaka, K., & Jubeau, M. (2018). Changes in central and peripheral neuromuscular fatigue indices after concentric versus eccentric contractions of the knee extensors. European Journal of Applied Physiology, 118, 805–816.
- Toonstra, J., & Mattacola, C. G. (2013). Test-retest reliability and validity of isometric knee-flexion and-extension measurement using 3 methods of assessing muscle strength. Journal of Sport Rehabilitation, 22, 1–5.
- Valle, X., Til, L., Drobnic, F., Turmo, A., Montoro, J. B., Valero, O., & Artells, R. (2013). Compression garments to prevent delayed onset muscle soreness in soccer players. Muscles, Ligaments and Tendons Journal, 3, 295.