
ABSTRACT
The aim of this study is to determine if bone mineral density (BMD) and bone asymmetry differs between female cricket fast bowlers, spin bowlers and batters. BMD was determined at the total body, lumbar spine, and proximal femurs in 12 fast bowlers, 13 batters and 11 spin bowlers from pre-season DXA scans. High Z-scores at the total body, lumbar spine, and proximal femur were observed in all cricketers (mean Z-scores: +1.4 to +3.3) compared with a general age matched reference population. Fast bowlers had significantly greater BMD on the contralateral side of the lumbar spine compared with the ipsilateral side (p = 0.001, 5.9–12.1%). No asymmetry was found between hips in all groups. All cricket positions demonstrated high BMD at all measured sites. The lumbar spine of fast bowlers is asymmetric, with significantly greater BMD on the contralateral side of the spine, particularly at L4, possibly in response to the asymmetric lumbar loading patterns observed in bowling.
Highlights
Elite female cricketers demonstrate high BMD at total body, lumbar spine and proximal femur sites, regardless of playing position compared with a general age and ethnic group matched reference population.
Fast bowlers have greater BMD on the contralateral (opposite bowling arm) side of the lumbar spine compared with the ipsilateral side, while a symmetrical pattern was observed in spin bowlers and batters.
No asymmetry in BMD or section modulus between hips was observed at any proximal femur site for any cricket position.
Introduction
Bone adapts to the habitual mechanical loads imposed upon it from both muscular and impact forces to improve its strength and resilience to fracture (Robling, Citation2009). The adaptation of bone to physical activity is site-specific to the region under greatest loading. For example, baseball players have significantly greater structural and bone strength indices in their dominant humerus compared to their non-dominant humerus (Warden, Bogenschutz, Smith, & Gutierrez, Citation2009). Further, sports which involve high impact and multidirectional lower limb loading patterns, such as volleyball, football and field hockey, demonstrate significantly greater hip bone mineral density (BMD) (Bellver, Del Rio, Jovell, Drobnic, & Trilla, Citation2019), and section modulus (Ferry et al., Citation2011) compared with sedentary controls or low impact activities.
Cricket fast bowling has an asymmetrical movement pattern characterised by multi-planar trunk movements and large ground reaction forces (Alway, Felton, Brooke-Wavell, Peirce, & King, Citation2021), which may contribute to the large estimated loading placed upon the lumbar spine (Zhang, Ma, & Liu, Citation2016). Coupled with the high match volume demands of elite cricket (Orchard et al., Citation2015), these factors likely contribute to male fast bowlers having significantly greater L1-L4 BMD than other cricket playing roles or sedentary controls (Alway, Peirce, King, Jardine, & Brooke-Wavell, Citation2019). The accrual of bone is greatest on the contralateral (to bowling arm) side of L3 and L4, where BMD is up to 14.6% greater than the ipsilateral side (Alway et al., Citation2019). Further, male fast bowlers have significantly elevated contralateral and ipsilateral hip BMD and section modulus compared with a control population, which suggests that these regions also experience significant loading, but BMD or section modulus did not differ between hips (Lees et al., Citation2018). A major cause of time-loss in female cricket is through lumbar bone stress injuries (Evans, Langley, & Ranson, Citation2015). One of the risk factors to bone stress injuries is site-specific low BMD, which has been observed in the lower leg of female track and field athletes who sustained tibial bone stress injuries (Bennell et al., Citation1996). Therefore, understanding what typical lumbar BMD values are in this population may be of use for medical practitioners for determining players who may be at risk of sustaining injury.
Female fast bowlers bowl at a slower velocity and adopt a different technique compared to males. Females have a slower run-up velocity, lower ground reaction forces and greater contributions from contralateral pelvis and trunk rotations compared with male fast bowlers (Felton, Lister, Worthington, & King, Citation2019), (Stuelcken & Sinclair, Citation2009). Females bowl considerably less than males in matches: analysis of publicly available scorecards demonstrated that the average female County Cricket Club is scheduled to compete on 15 days per season (first class = 4 days, list A and twenty over = 1 d), compared with 93 match days for the male equivalent. Finally, females have smaller lumbar vertebrae (Zhou, Mccarthy, Mcgregor, Coombs, & Hughes, Citation2000) and greater lumbar lordosis (Been, Barash, Pessah, & Peleg, Citation2010) than males.
The differences in technique, workload and lumbar spine geometry between sexes may result in a different osteogenic pattern in female fast bowlers. Therefore, the aims of this study were to determine, in females, whether BMD differs significantly by cricket position, and whether there is asymmetry in BMD between ipsilateral and contralateral sides of the lumbar spine, or asymmetry between the hips, within each position.
Materials and methods
37 elite female cricketers, including fast bowlers, spin bowlers and batters, competing in either national senior or development squads participated in the study. Bowlers were defined as any player who averaged more than 18 deliveries per professional innings, calculated from publicly available scorecards. Fast bowlers were defined as those for whom the wicketkeeper would usually “stand back” (Alway et al., Citation2021). Spin bowlers were defined as those who the wicketkeeper would usually “stand up” and imparted spin on the ball using wrist or finger spin techniques. Batters were defined as those whose primary position was batting, averaged less than 18 bowling deliveries per professional innings, and included wicketkeepers. Exclusion criteria for all participants were any disease or medication that affects bone health; any conditions that may contraindicate X-ray exposure, no time-loss injuries in the previous 3 months, and no known current lumbar bone stress injuries, or known unusual pathological changes (healed fractures, osteophytes, arthritic changes) to the lumbar spine which can affect BMD. The study was approved by the Loughborough University Ethics Approvals (Human Participants) Sub-Committee and the National Research Ethics Service. All participants provided written informed consent prior to commencement of the study.
Participants underwent total body, anteroposterior (AP) and lateral lumbar spine, and dual femur dual X-ray absorptiometry (DXA) scans on a GE-Lunar iDXA densitometer (Madison, WI, USA) using standard positioning protocols during pre-season. Scans were analysed using Lunar enCORE (v. 17.0). Total body scans were used to determine BMD, Z-score, fat free mass and body fat. AP lumbar spine scans were used to determine L1-L4 BMD and Z-Score. Further, a custom analysis of the AP lumbar spine scan was conducted which used the lateral third of each vertebral body to determine BMD of the ipsilateral and contralateral sides of each vertebra (Alway et al., Citation2019). Lateral decubitus lumbar spine scans were used to determine BMD of the L3 vertebral body and posterior elements (Alway et al., Citation2019). Dual-femur scans were used to determine BMD, Z-score and section modulus of the contralateral (landing leg in bowling or throwing) and ipsilateral femoral neck and total hip. Menstrual function and oral contraceptive use were determined from a questionnaire. Eumenorrhea was defined as at least 9 menses in the previous 12 months in the preceding year with no oral contraceptive use in the preceding 3 months (Ackerman et al., Citation2015). Therefore menstrual function could only be determined in participants who were not taking oral contraceptives. Participants who were either oligomenorrheic or amenorrheic were excluded from the study due to the negative association between impaired menstrual function and BMD accrual in athletes (Nichols, Rauh, Barrack, & Barkai, Citation2007). To determine total bone loading, a bone specific physical activity questionnaire was used (Weeks & Beck, Citation2008).
Repeatability of each analysis was determined using repeat scans in 24 participants on the same day with repositioning and demonstrated precision (RMS-SD, %CV) was: total body BMD (0.011 g/cm2, 0.99%), fat free mass (0.85 kg, 1.31%) and body fat % (0.34%, 2.11%); L1-L4 BMD (0.007 g/cm2, 0.46%); contralateral femoral neck BMD (0.012 g/cm2, 0.95%); contralateral total hip BMD (0.020 g/cm2, 1.38%) and section modulus (48.36 cm3, 4.32%); rear femoral neck BMD (0.018 g/cm2, 1.40%); rear total hip BMD (0.013 g/cm2, 1.01%) and section modulus (45.30 cm3, 4.25%); posterior elements BMD (0.029 g/cm2, 3.66%); vertebral body BMD (0.028 g/cm2, 2.55%); and unilateral lumbar spine BMD (0.025–0.042 g/cm2, 1.69%–2.45%).
All statistical analyses were calculated within SPSS (v. 27, IBM, USA). After assessing data for normality and homoscedasticity, one-way ANOVA (Kruskal–Wallis test for non-parametric data) was used to determine if activity group differed in age, height, body mass, fat-free mass, body fat %, bone loading, professional matches participated in across their career and average balls bowled per match. Pearson Chi-Square tests (Fisher-Freeman-Halton Exact Test if expected counts were below 5) were used to investigate between group differences in oral contraception use. Age and fat free mass were used as covariates due to the strong relationships between lean mass and bone mineral density (Baxter-Jones, Faulkner, Forwood, Mirwald, & Bailey, Citation2011; Ho-Pham, Nguyen, & Nguyen T, Citation2014). Any other significant differences between groups in participant characteristics were used as covariates in the comparison of bone properties between groups. Further one-way ANOVAs were used to determine differences between groups in unadjusted and adjusted (for potential covariates) total body, L1-L4, contralateral and ipsilateral femoral neck and total hip BMD and Z-scores, as well as L3 vertebral body and posterior elements BMD. All significant ANOVAs used a post-hoc Bonferoni test to determine specific differences between groups.
Two-way mixed repeated measures ANOVA determined between and within group differences in BMD between ipsilateral and contralateral sides of the lumbar spine, and in BMD and section moduli between ipsilateral and contralateral hips. If there were significant interactions between: vertebral level and position, vertebral side and position, vertebral level, vertebral side and position, or hip and position; further one-way ANOVAs were used to determine between group differences, while a paired t-test was used to determine within group differences. An alpha level of 0.05 was set for all measures, and Cohen’s d (r for non-parametric data) was calculated to determine effect sizes for differences between groups.
Results
One participant (1 spin bowler) was oligomenorrheic and was removed from the analysis. There were significant differences between groups in average balls bowled per match (p < 0.001, ). Fast bowlers and spin bowlers bowled significantly more balls per game than batters (p < 0.001, r = 0.850), but no differences in balls bowled per game were found between fast and spin bowlers (p = 0.955, r = 0.178). No significant differences were observed between groups in age (p = 0.264), height (p = 0.115), body mass (p = 0.704), fat free mass (p = 0.263), body fat percentage (p = 0.199), professional matches (p = 0.411), oral contraceptive use (p > 0.999) and questionnaire derived bone loading (p = 0.551, ).
Table 1. Mean ± SD, or median (IQR) for non-parametric data, age, height, body mass, fat free mass, body fat, menstrual function, oral contraceptive use, professional matches played and average number of balls bowled per professional match of batters, fast bowlers and spin bowlers.
After adjustment for age and fat free mass (fat free mass only for Z-scores), there were no significant differences between groups in: total body BMD (p = 0.536) and Z-score (p = 0.152); L1-L4 BMD (p = 0.422) and Z-score (p = 0.084); L3 vertebral body (p = 0.719) and posterior element BMD (p = 0.363); contralateral femoral neck (p = 0.497) and total hip Z-scores (p = 0.404); ipsilateral femoral neck (p = 0.493) and total hip Z-scores (p = 0.710). Adjusted and unadjusted data can be found in .
Table 2. Mean ± SD unadjusted and adjusted (for age and fat free mass) total body, L1-L4, lateral L3 vertebral body and lateral L3 posterior element BMD (g/cm2) and unadjusted and adjusted (for fat free mass) total body, L1-L4, and ipsilateral (IL) and contralateral (CL) femoral neck and total hip Z-scores of batters, fast bowlers and spin bowlers.
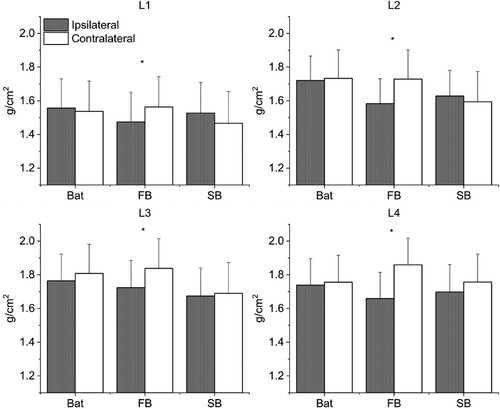
After adjustment for age and fat free mass, there was a significant interaction between vertebral side and group on BMD (p = 0.001, ES = 0.379). No significant interactions were found between vertebral level and group on BMD (p = 0.097, ES = 0.118), or between vertebral side, vertebral level and group on BMD (p = 0.188, ES = 0.88). Post-hoc analysis revealed that there were no between group differences in ipsilateral (p = 0.321) or contralateral (p = 0.251) side BMD of the lumbar spine. Within group analysis demonstrated that mean BMD was significantly greater on the contralateral side of the lumbar spine compared with the ipsilateral side in fast bowlers (8.4%, p < 0.001, d = 1.50), with the greatest asymmetry being found at L4 (L1 = 5.9%, L2 = 9.2%, L3 = 6.7%, L4 = 12.1%). No asymmetry was found in batters (p = 0.68, d = 0.12) or spin bowlers (p = 0.95, d = 0.02).
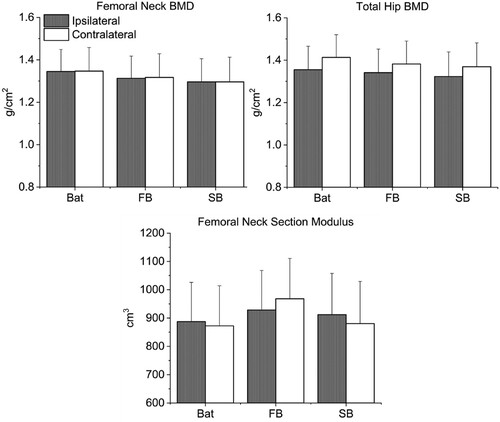
After adjustment for age and fat free mass, there were no significant differences according to side (contralateral/ipsilateral) or activity in femoral neck BMD (p = 0.985, ES = 0.001), total hip BMD (p = 0.656, ES = 0.027) or section modulus (p = 0.098, ES = 0.139, ).
Discussion
This is the first study to report on BMD in elite female cricketers, and demonstrated that female cricketers, regardless of playing position, have elevated BMD compared to the general population at total body, lumbar spine and proximal femur sites as evidenced by Z-scores in excess of +1.8. Further, female fast bowlers had significantly greater BMD on the contralateral side of the lumbar spine, highlighting the unique unilateral loading characteristics of cricket fast bowling.
No differences were found between any of the groups in total body BMD and Z-score (), which likely reflects the overall positive osteogenic effect of regular participation in a high intensity, multi-directional weight bearing activity, as evidenced by mean total body Z-scores more than 2.5 standard deviations greater than a reference population. The elite setting, providing access to strength and conditioning facilities and nutritional support may also contribute. Regular strength training has been shown to have a positive osteogenic effect in young women (Mosti et al., Citation2014), while adequate nutrition facilitates positive accrual of bone to physical activity (Sale & Elliott-Sale, Citation2019). Women participating in other weight bearing activities such as basketball, football, track sprint and jumping athletes and volleyball also demonstrate elevated total body BMD compared with a sedentary or low impact athletic populations (Stanforth, Lu, Stults-Kolehmainen, Crim, & Stanforth, Citation2016).
Batters, fast bowlers and spin bowlers all demonstrated high lumbar BMD and Z-Scores, comparable to other elite female athletes who participate in high lumbar loading activities, such as volleyball (Bellver et al., Citation2019). Whole L1-L4 BMD and Z-scores did not differ between positions in the current study (), suggesting that all positions experience significant osteogenic adaptation at the lumbar spine, despite differences in typical movement patterns.
Batters can employ a number of different shots depending on the trajectory and speed of the ball, and it is likely that powerful rotations of the lumbar and thoracic spine are required during the downswing phase, as seen in the front-foot straight drive (Peploe, McErlain-Naylor, Harland, & King, Citation2019), which may generate significant bone strains within the lumbar spine from the surrounding musculature, eliciting a positive bilateral osteogenic response.
While fast bowlers did not have significantly greater L1-L4 BMD than other positions, they did demonstrate marked lumbar asymmetry, where the contralateral side of the lumbar spine has significantly greater BMD than the ipsilateral side, particularly at L4 (12.1%, ). This peak asymmetry magnitude is similar to that observed in elite male fast bowlers, who demonstrated 14.6% greater BMD on the contralateral side of L4 (Alway et al., Citation2019). This site-specific region of BMD experienced by both male and female fast bowlers likely has a common biomechanical aetiology, resulting in a comparable strain polarity, despite differences in techniques used to generate ball speed between sexes (Felton et al., Citation2019). Both male and female fast bowlers experience rapid multiplanar trunk motions (Felton et al., Citation2019), coupled with high vertical ground reaction forces, horizontal braking forces and vertical loading rates at front foot contact (Alway et al., Citation2021; Stuelcken & Sinclair, Citation2009), which likely puts great strain on the inferior, contralateral lumbar spine. This similar observed asymmetry between sexes occurs despite the much lower workload of female fast bowlers. Very few loading cycles are required to stimulate a significant osteogenic response to mechanical loading, with no differences in bone formation being observed between 36 and 1800 loading cycles of high strain activity (Rubin & Lanyon, Citation1984). The lower ball velocity generated by female fast bowlers compared to male fast bowlers suggests that the forces experienced at the lumbar spine may be lower in female fast bowlers. However, women have smaller vertebrae than men (Zhou et al., Citation2000), with greater lumbar lordosis (Been et al., Citation2010), which may result in comparable strain magnitude being generated within the contralateral side of the lumbar spine. The asymmetric fast bowling techniques, coupled with workloads high enough to elicit osteogenic adaptation, likely elicits high mechanical strains within the contralateral side of the lumbar spine triggering bone modelling and remodelling processes at these specific sites (Frost, Citation2003). This may result in the asymmetry observed at the lumbar spine in fast bowlers, which may be derived from both muscular forces, from forceful contractions of the surrounding musculature, and impact forces, from the large ground reaction forces experienced at front foot contact (Robling, Citation2009).
Figure 1. Adjusted (fat free mass and age) mean (SD) unilateral ipsilateral and contralateral lumbar spine BMD between batters (Bat), fast bowlers (FB) and spin bowlers (SB). *denotes significant within-group differences.
No lumbar asymmetry was observed in batters or spin bowlers, suggesting that their loading is typically bilateral, or not of great enough magnitude to elicit a significant asymmetric response. For example, male spin bowlers have a slower ball velocity (Mean ± SD. Spin: 20.4 ± 1.3, Fast: 34.9 ± 1.7 m/s) (Sanders, Felton, & King, Citation2018), (Worthington, King, & Ranson, Citation2013), lower peak vertical and horizontal ground reaction forces (Vertical: Spin: 2.3 ± 0.9 BW, Fast: 6.7 ± 1.4; Horizontal: Spin 1.0 ± 0.5 BW, Fast: 4.5 ± 0.8) (Beach, Ferdinands, & Sinclair, Citation2014), (King et al., Citation2016), and smaller peak thorax rotation angular velocity (Spin: 264 ± 126°/s, Fast: 485 ± 285°/s) (Beach, Ferdinands, & Sinclair, Citation2018), (Burnett, Barrett, Marshall, Elliott, & Day, Citation1998) than fast bowlers, suggesting that less forceful asymmetric loading is placed on the spine during the spin bowling action.
Batters, fast bowlers and spin bowlers all demonstrated proximal femur Z-scores in excess of +2.4 (), demonstrating the osteogenic potential of participating in cricket at the proximal femur, similar to the findings observed in male fast bowlers (Lees et al., Citation2018). The high BMD at both femoral neck and total hip sites is comparable to elite female athletes participating in high impact sports, such as volleyball (Bellver et al., Citation2019). There was no significant difference in BMD or section modulus between or within groups (), similar to the findings observed in male fast bowlers (Lees et al., Citation2018). This demonstrates that the total bone loading on the proximal femur is similar between and within positions. Across positions there are some shared tasks which may contribute to the elevated Z-scores observed at the proximal femur. Firstly, all cricketers will engage in multiple bouts of high velocity running throughout the game. In a twenty over cricket match, international standard female cricketers have been shown to cover in excess of 5000 m, with short bouts of high intensity running (> 21 km/h) comprising over 50 metres of these (Garcia-Byrne et al., Citation2020). High intensity running is known to have a significant osteogenic effect upon BMD at the proximal femur, with track sprinters demonstrating significantly elevated BMD compared with sedentary or low impact athlete populations (Piasecki et al., Citation2018). Secondly, all cricketers will be required to overarm throw the ball while fielding. During throwing, the musculature surrounding the hips acts to stabilise the torso as it accelerates over a planted front leg, and to accelerate rotation of the pelvis towards the target, (Oliver & Keeley, Citation2010) possibly eliciting a significant bone strain across the proximal femur. Finally, batters may bowl during training, and bowlers will bat during training and in matches.
Figure 2. Adjusted (fat free mass and age) ipsilateral and contraltaeral hip BMD and section moduli between batters (Bat), fast bowlers (FB) and spin bowlers (SB).
Specific movement patterns related to each position may provide an explanation of the high proximal femur Z-scores and BMD observed across playing roles in cricketers. During batting, to develop the power needed to generate the bat speed for successful execution for many of the shots used by batters, forceful, rapid, sequential rotations of the pelvis and trunk are required, which generates kinetic energy which is transferred distally into the arms and the bat (Peploe et al., Citation2019). During front-foot batting, where the batters’ weight is shifted over the front foot, the pelvis is a key component of maximising launch distance of the ball. Firstly, the pelvis resists the rotation of the thorax, which is rotating away from the bowler, to create a pelvis-thorax separation angle at the initiation of the downswing (Peploe et al., Citation2019). Secondly, during the downswing, the pelvis rapidly rotates towards the bowler (Peploe et al., Citation2019). Both would require significant activation of the muscles involved in pelvic rotation and stabilisation, such as the gluteal muscle group, which attach to the proximal femur, possibly eliciting a significant bone strain across this region. While there is no published muscle activity data during cricket batting, evidence from similar movements, such as a golf swing, demonstrate high activation of the gluteal muscle group during the downswing phase (Marta, Silva, Castro, Pezarat-Correia, & Cabri, Citation2012).
During both fast and spin bowling, both proximal femurs may experience large forces from both gravitational and muscular sources which may elicit similar osteogenic responses at each proximal femur. During fast bowling, ground reaction forces and loading rates during bowling are both substantially higher at front foot contact compared with back foot contact (Hurrion, Dyson, & Hale, Citation2000), with mean peak vertical ground reaction forces and average vertical loading rates at front foot contact reported as 6.9 bodyweights and 357 body weights per second respectively (Alway et al., Citation2021), compared with 2.4 bodyweights and 78 body weights per second respectively at back foot contact (Hurrion et al., Citation2000). Fast bowlers also experience powerful contractions of the musculature surrounding the hips to generate torques to stabilise the lumbo-pelvi-hip complex and to transfer force from the lower body to the upper body to assist in the generation of ball speed (Forrest, Hecimovich, & Dempsey, Citation2016). While spin bowlers bowl slower than fast bowlers, and produce lower ground reaction forces and likely lower muscular torques. The bone strains elicited may be great enough to result in a positive adaptation at the proximal femur. Alternatively, it may be that the other components of cricket (such as batting or fielding) also contribute to the adaptation of the hips of spin bowlers.
Strengths of this study include the unique cohort of elite cricket fast bowlers across positions who were scanned on the same DXA scanner at the same stage of the season. While the similar BPAQ results suggest similar training volumes between positions, the BPAQ questionnaire only records training frequency per week rather than hours training per week. In addition, BPAQ may not be specific enough to differentiate the differences in skeletal loading between cricket positions, where intensities and volumes likely differ, which may have impacted the results in the current study. The lateral lumbar scan uses a soft tissue reference region that may less accurately reflect the soft tissue overlying the bone, particular at the posterior elements, which may affect the attenuation characteristics and measured BMD and BMC (Tothill & Pye, Citation1992). As soft tissue composition was likely similar between athletic groups, this error should not invalidate these comparisons.
Future research should look to explore if the marked asymmetry of the lumbar spine in fast bowlers differs depending on technique, age, workload or according to bone stress injury history. Finally, future research should explore what the architectural changes of the lumbar spine are in response to fast bowling.
Elite female cricketers demonstrate high bone mineral density across total body, lumbar spine and proximal femur sites, likely due to the combination of large muscular induced forces and impact which are involved with batting and bowling, which provide a powerful osteogenic stimulus. Fast bowlers have an asymmetric lumbar spine, where there is greater BMD on the contralateral side of the spine.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ackerman, K. E., Sokoloff, N. C., De Nardo Maffazioli, G., Clarke, H. M., Lee, H., & Misra, M. (2015). Fractures in relation to menstrual status and bone parameters in young athletes. Medicine & Science in Sports & Exercise, 47(8), 1577–1586. doi:10.1249/MSS.0000000000000574
- Alway, P., Felton, P., Brooke-Wavell, K., Peirce, N., & King, M. (2021). Cricket fast bowling technique and lumbar bone stress injury. Medicine & Science in Sports & Exercise, 53(3), 581–589. doi:10.1249/mss.0000000000002512
- Alway, P., Peirce, N., King, M., Jardine, R., & Brooke-Wavell, K. (2019). Lumbar bone mineral asymmetry in elite cricket fast bowlers. Bone, 127, 537–543. doi:10.1016/j.bone.2019.07.030
- Baxter-Jones, A. D. G., Faulkner, R. A., Forwood, M. R., Mirwald, R. L., & Bailey, D. A. (2011). Bone mineral accrual from 8 to 30 years of age: An estimation of peak bone mass. Journal of Bone and Mineral Research, 26(8), 1729–1739. doi:10.1002/jbmr.412
- Beach, A. J., Ferdinands, R. E. D., & Sinclair, P. J. (2014). The kinematic differences between the leg-spin and off-spin bowling techniques in cricket. In: ISBS Proceedings Archive., 300-303.
- Beach, A. J., Ferdinands, R. E. D., & Sinclair, P. J. (2018). The relationship between segmental kinematics and ball spin in type-2 cricket spin bowling. Journal of Sports Sciences, 36(10), 1127–1134. doi:10.1080/02640414.2017.1358460
- Been, E., Barash, A., Pessah, H., & Peleg, S. (2010). A New look at the geometry of the lumbar spine. Spine (Phila Pa 1976), 35(20), 1014–1017.
- Bellver, M., Del Rio, L., Jovell, E., Drobnic, F., & Trilla, A. (2019). Bone mineral density and bone mineral content among female elite athletes. Bone, 127(February), 393–400. doi:10.1016/j.bone.2019.06.030
- Bennell, K. L., Malcolm, S. A., Thomas, S. A., et al. (1996). Risk factors for stress fractures in track and field athletes: A twelve- month prospective study. American Journal of Sports Medicine, 24(6), 810–818. doi:10.1177/036354659602400617
- Burnett, A. F., Barrett, C. J., Marshall, R. N., Elliott, B. C., & Day, R. E. (1998). Three-dimensional measurement of lumbar spine kinematics for fast bowlers in cricket. Clinical Biomechanics, 13(8), 574–583. doi:10.1016/S0268-0033(98)00026-6
- Evans, R., Langley, B., & Ranson, C. (2015). Four-year injury surveillance of an international women’s cricket squad. In: 5th World Congress of Science and Medicine in Cricket.
- Felton, P. J., Lister, S. L., Worthington, P. J., & King, M. A. (2019). Comparison of biomechanical characteristics between male and female elite fast bowlers. Journal of Sports Sciences, 37(6), 665–670. doi:10.1080/02640414.2018.1522700
- Ferry, B., Duclos, M., Burt, L., et al. (2011). Bone geometry and strength adaptations to physical constraints inherent in different sports: Comparison between elite female soccer players and swimmers. Journal of Bone and Mineral Metabolism, 29(3), 342–351. doi:10.1007/s00774-010-0226-8
- Forrest, M., Hecimovich, M., & Dempsey, A. (2016). Lumbopelvic muscle activation patterns in adolescent fast bowlers. European Journal of Sport Science, 16(6), 677–684. doi:10.1080/17461391.2015.1135985
- Frost, H. M. (2003). Bone’s mechanostat: A 2003 update. Anat Rec Part a, 275A(August), 1081–1101. doi:10.1002/ar.a.10119
- Garcia-Byrne, F., Buckley, J. D., Bishop, C., et al. (2020). External and internal workload demands of women’s twenty 20 cricket competition. Journal of Science and Medicine in Sport, 23(1), 89–93. doi:10.1016/j.jsams.2019.09.006
- Ho-Pham, L. T., Nguyen, U. D. T., & Nguyen T, V. (2014). Association between lean mass, fat mass, and bone mineral density: A meta-analysis. Journal of Clinical Endocrinology and Metabolism, 99(1), 30–38. doi:10.1210/jc.2013-3190
- Hurrion, P. D., Dyson, R., & Hale, T. (2000). Simultaneous measurement of back and front foot ground reaction forces during the same delivery stride of the fast-medium bowler. Journal of Sports Sciences, 18(12), 993–997. doi:10.1080/026404100446793
- King, M. A., Worthington, P. J., Ranson, C. A., et al. (2016). Does maximising ball speed in cricket fast bowling necessitate higher ground reaction forces ? does maximising ball speed in cricket fast bowling necessitate higher ground. Journal of Sports Sciences, 34(8), 707–712. doi:10.1080/02640414.2015.1069375
- Lees, M. J., Beggs, C. B., Barlow, M. J., et al. (2018). Bone density and cross-sectional geometry of the proximal femur Are bilaterally elevated in elite cricket fast bowlers. Journal of Clinical Densitometry, 21(3), 399–405. doi:10.1016/j.jocd.2017.06.005
- Marta, S., Silva, L., Castro, M. A., Pezarat-Correia, P., & Cabri, J. (2012). Electromyography variables during the golf swing: A literature review. Journal of Electromyography and Kinesiology, 22(6), 803–813. doi:10.1016/j.jelekin.2012.04.002
- Mosti, M. P., Carlsen, T., Aas, E., Hoff, J., Stunes, A. K., & Syversen, U. (2014). Maximal strength training improves bone mineral density and neuromuscular performance in young adult women. Journal of Strength and Conditioning Research, 28(10), 672–677.
- Nichols, J. F., Rauh, M. J., Barrack, M. T., & Barkai, H. S. (2007). Bone mineral density in female high school athletes: Interactions of menstrual function and type of mechanical loading. Bone, 41(3), 371–377. doi:10.1016/j.bone.2007.05.003
- Oliver, G. D., & Keeley, D. W. (2010). Gluteal muscle group activation and its relationship with pelvis and torso kinematics in high-school baseball pitchers. Journal of Strength and Conditioning Research, 24(11), 3015–3022.
- Orchard, J., Blanch, P., Paoloni, J., Kountouris, A., Sims, K., & Brukner, P. (2015). Cricket fast bowling workload patterns as risk factors for tendon, muscle, bone and joint injuries. British Journal of Sports Medicine, 49(16), 1064–1068. doi:10.1136/bjsports-2014-093683
- Peploe, C., McErlain-Naylor, S. A., Harland, A. R., & King, M. A. (2019). Relationships between technique and bat speed, post-impact ball speed, and carry distance during a range hitting task in cricket. Human Movement Science, 63(April 2018), 34–44. doi:10.1016/j.humov.2018.11.004
- Piasecki, J., McPhee, J. S., Hannam, K., et al. (2018). Hip and spine bone mineral density are greater in master sprinters, but not endurance runners compared with non-athletic controls. Archives of Osteoporosis, 13(1). doi:10.1007/s11657-018-0486-9
- Robling, A. G. (2009). Is bone’s response to mechanical signals dominated by muscle forces? Medicine & Science in Sports & Exercise, 41(11), 2044–2049. doi:10.1249/MSS.0b013e3181a8c702.Is
- Rubin, C., & Lanyon, L. (1984). Regulation of bone formation by applied dynamic loads. J Bone Jt Surg, 66A(3), 397–402.
- Sale, C., & Elliott-Sale, K. J. (2019). Nutrition and athlete bone health. Sport Med., 49(s2), 139–151. doi:10.1007/s40279-019-01161-2
- Sanders, L., Felton, P. J., & King, M. A. (2018). Kinematic parameters contributing to the production of spin in elite finger spin bowling. Journal of Sports Sciences, 36(24), 2787–2793. doi:10.1080/02640414.2018.1474531
- Stanforth, D., Lu, T., Stults-Kolehmainen, M. A., Crim, B. N., & Stanforth, P. R. (2016). Bone mineral content and density Among female NCAA division I athletes across the competitive season and over a multi-year tiem frame. Journal of Strength and Conditioning Research, 30(10), 2828–2838.
- Stuelcken, M. C., & Sinclair, P. J. (2009). A pilot study of the front foot ground reaction forces in elite female fast bowlers. Journal of Science and Medicine in Sport, 12(2), 258–261. doi:10.1016/j.jsams.2007.10.016
- Tothill, P., & Pye, D. W. (1992). Errors due to non-uniform distribution of fat in dual X-ray absorptiometry of the lumbar spine. The British Journal of Radiology, 65(777), 807–813. doi:10.1259/0007-1285-65-777-807
- Warden, S. J., Bogenschutz, E. D., Smith, H. D., & Gutierrez, A. R. (2009). Throwing induces substantial torsional adaptation within the midshaft humerus of male baseball players. Bone, 45(5), 931–941. doi:10.1016/j.bone.2009.07.075
- Weeks, B. K., & Beck, B. R. (2008). The BPAQ: A bone-specific physical activity assessment instrument. Osteoporosis International, 19(11), 1567–1577. doi:10.1007/s00198-008-0606-2
- Worthington, P. J., King, M. A., & Ranson, C. A. (2013). Relationships between fast bowling technique and ball release speed in cricket. Journal of Applied Biomechanics, 29(1), 78–84.
- Zhang, Y., Ma, Y., & Liu, G. (2016). Lumbar spinal loading during bowling in cricket: A kinetic analysis using a musculoskeletal modelling approach. Journal of Sports Sciences, 34(11), 1030–1035. doi:10.1080/02640414.2015.1086014
- Zhou, S. H., Mccarthy, I. D., Mcgregor, A. H., Coombs, R. R. H., & Hughes, S. P. F. (2000). Geometrical dimensions of the lower lumbar vertebrae – analysis of data from digitised CT images. European Spine Journal, 9, 242–248.