
ABSTRACT
We examined the longitudinal associations of accelerometer-measured physical activity and sedentary time with leg muscle strength (LMS), balance, and falls in middle-aged women. This was a 5-year cohort study among 308 women aged 36–56 years. We used linear mixed-effects models to examine associations of baseline and change in accelerometer-measured sedentary time, light physical activity (LPA) and moderate-to-vigorous physical activity (MVPA) with baseline and 5-year change in LMS and balance (timed up and go test [TUG], functional reach test [FRT], lateral reach test [LRT], and step test [ST]), and negative binomial/Poisson and log-binomial regression as appropriate to assess associations with falls after 5-year follow-up. Greater baseline MVPA was associated with better baseline LMS (β = 4.65 kg/SD, 95% CI: 1.37, 7.93) and TUG (β = −0.09 s/SD, 95% CI: –0.18, –0.01) but not with change in them over 5 years. Baseline MVPA was not associated with FRT at baseline but associated with a greater decrease in FRT (β = −0.87 cm/SD, 95% CI: –1.57, –0.17). Increased MVPA over 5 years was associated with less deterioration in FRT (β = 0.88 cm/SD, 95% CI: 0.14, 1.61). Increased sedentary time over 5 years was associated with a larger decrease in FRT (β = −0.82 cm/SD, 95% CI: –1.58, –0.07). Higher baseline LPA was associated with higher falls risk (IRR = 1.27, 95% CI: 1.02, 1.57). Higher baseline MVPA may benefit LMS and balance, while increasing MVPA in the medium term has little effect on change in these outcomes in mid-life. Detrimental association of LPA with falls may be due to greater exposures to environmental hazards.
Highlights
Our study for the first time examined the longitudinal associations of objectively measured physical activity and sedentary time with leg muscle strength, balance and falls in middle-aged women.
Higher baseline moderate-to-vigorous physical activity (MVPA) may be beneficial for muscle strength and balance at baseline but increasing MVPA in the medium term has little effect on change in LMS or balance outcomes in middle-aged women.
Higher baseline light physical activity (LPA) was associated with an increased risk of falls.
The detrimental association of LPA with falls may be due to a greater exposure to environmental hazards in midlife, which needs to be clarified in future research.
Introduction
Falls are the major cause of hip fracture and the second leading cause of unintentional injury-related mortality worldwide (World Health Organization, Citation2021). Around thirty to forty percent of community-dwelling older persons fall each year and women have a higher risk than men (Callisaya et al., Citation2011). Of note, similarly high incidences of falls have more recently also been reported in middle-aged people (Wang et al., Citation2020). Muscle strength and balance, major modifiable risk factors of falls in older adults, start to decline in middle-age (EI Haber et al., Citation2008), suggesting that this is a critical life stage to reduce the risk of falling. However, much less research effort has been made to understand the prevention of falls in this age group.
While there is substantial evidence of associations between physical activity and falls in older adults, only a single cross-sectional study has investigated such associations in middle-aged women. A systematic review and meta-analyses of 10 prospective cohort studies suggests that engaging in physical activity and avoiding sedentary behaviour helps to reduce risk of falling among older adults (Lee, Citation2020). In the only study in middle-aged adults, those who reported engaging in physical activity were less likely to report falls than those who did not (Caban-Martinez et al., Citation2015).
As with falls, evidence that physical activity is beneficial for the modifiable risk factors for falls of muscle strength and balance is substantial in older adults but limited in middle-aged women. A meta-analysis of 16 randomised controlled trials in older adults showed that improving physical activity was an effective intervention to improve balance (Papalia et al., Citation2020). Several longitudinal studies have also demonstrated that increasing physical activity could benefit maintenance of muscle function in older adults (Scott et al., Citation2011; Scott et al., Citation2015). In contrast, studies investigating the association between physical activity or sedentary time with leg muscle strength (LMS) or balance in middle-aged adults to date are only cross-sectional (Chahal et al., Citation2014; Straight et al., Citation2015; Willoughby & Copeland, Citation2015; Sipila et al., Citation2020; Cooper et al., Citation2020; Takae et al., Citation2020; Abe et al., Citation2015; Ward-Ritacco et al., Citation2014), were in small convenience samples (Chahal et al., Citation2014; Straight et al., Citation2015; Willoughby & Copeland, Citation2015; Takae et al., Citation2020; Abe et al., Citation2015; Ward-Ritacco et al., Citation2014) and only one investigated the independent effects of MVPA and sedentary time on LMS and postural stability (Willoughby & Copeland, Citation2015). Thus, while there is evidence from a broad range of studies that physical activity reduces loss in muscle function and balance in older adults, it is uncertain whether physical activity is associated with such age-related declines in middle-aged adults. This information would be beneficial for clinicians, researchers, public health practitioners and policy makers.
Therefore, the aim of our study was to examine the longitudinal associations of objectively measured physical activity and sedentary time with LMS, balance, and incident falls in middle-aged women. We hypothesise that greater baseline physical activity and increased physical activity over 5 years will have beneficial associations with LMS, balance and falls, and conversely that such associations of sedentary time will be detrimental.
Methods
Participants
The study participants were drawn from 470 women (response rate of 64%) who were randomly selected from the Tasmania electoral roll and originally participated in a 2-year randomised controlled trial (RCT) of osteoporosis education intervention in 2000 (Winzenberg et al., Citation2006). The original participants were excluded if they had previous measurement of bone density, history of thyroid disease, renal failure, malignancy, rheumatoid arthritis, a history of hysterectomy or hormone replacement therapies, were pregnant or planning pregnancy within 2 years of study entry, or lactating. Of 470 women, 347 (74%) were followed up again in 2011–2012 (baseline of the current study) (Wu et al., Citation2018). In 2017–2019, we invited all women from the baseline survey to participate in a 5-year follow-up. Participants were included in the analyses if they had at least one of the outcome measures and had at least 5 valid days of physical activity recorded at baseline or 5-year follow-up. The Tasmania Health and Medical Human Research Ethics Committee approved this study (H0016156), and all participants gave written informed consent.
Physical activity
We used accelerometers (ActiGraph GTlM, Pensacola, FL, USA) to measure ambulatory physical activity for 7 consecutive days at baseline and 5-year follow-up. Participants wore the accelerometer over the right hip. Accelerometer counts were recorded in 60-s epochs. A valid day was defined as having at least 10 h of accelerometer wearing. Participants recorded start and finish times each day in a diary, and the duration and reason for any time where they took the accelerometer off, as well as the circumstances potentially affecting accelerometer readings (e.g. driving on uneven ground). Accelerometer wear time was derived from diary data, and any time that the participants recorded taking the accelerometer off was defined as non-wear time. Total counts divided by total wear time per day (counts/min [CPM]) was used to indicate total physical activity. A cut-off of <150 CPM was used to define time spent sedentary (Kozey-Keadle et al., Citation2011). Cut-offs for light physical activity (LPA) and MVPA were 151–1748 CPM and ≥1749 CPM, respectively (Brooks et al., Citation2005). Average sedentary time and time spent in LPA and MVPA were calculated by total time for each activity intensity divided by the number of valid days. The 5-year changes in average time at each intensity were calculated by subtracting baseline value from that after 5 years.
LMS and balance
LMS and balance were measured at baseline and the 5-year follow-up. Dynamometry (TTM Muscular Meter, Tokyo, Japan) was used to measure LMS to the nearest kilogram (Dore et al., Citation2010). This test measures isometric strength, predominantly of the quadriceps and hip extensors. The examiner demonstrated the correct technique to the participant before testing. Participants stood on the back of the dynamometer platform, with back straight against a wall and knees flexed to an angle of 115°. They then lifted a bar connected to the dynamometer by a chain using maximum force using their legs, with the back and neck straight. A published figure illustrates the assessment (Scott et al., Citation2011). The mean of two readings was calculated for analyses. At baseline, the intraclass correlation coefficient for this test was 0.94 (95% CI: 0.92–0.95) (Wu, Wills, et al., Citation2017).
We assessed balance using four commonly used clinical tests: timed up and go test (TUG), step test (ST), functional reach test (FRT), and lateral reach test (LRT). These tests differentiate between fallers and non-fallers in older adults (Isles et al., Citation2004). All have been validated in older women and have normative values determined in women of the age in our study (Isles et al., Citation2004). Briefly, TUG measures dynamic balance and gait. Participants sat in an armchair (45 cm high) with their back against the chair, and then stood without using the arms, walked 3 metres, turned, walked back, and sat down. The average time of two trials was used for analyses.
The ST measures speed of performing a dynamic stepping task. It is an assessment of reactive steps in an upright position in response to the challenge of stepping onto a target. Participants stood 5 cm from an 8.5-cm-high block positioned against a wall and placed the whole foot of one leg onto the block and returned it to the floor repeatedly as fast as possible for 15 s. The number of steps was recorded for both sides and the mean number of steps for each side was used for analyses.
The FRT measures the ability to reach forward with each arm from a bilateral stance position. Participants stood with feet a comfortable distance apart behind a line perpendicular and adjacent to a wall. The arm closest to the wall was raised to shoulder height and the position of the knuckle of the middle finger measured. Participants leaned forward as far as possible, and the position of the knuckle was recorded at the point of furthest reach. The mean of the three trials on each side was used for analyses.
The LRT measures the ability to reach to the side in bilateral stance. Participants stood with their backs near but not touching a wall with the heels 10 cm apart. Participants raised both arms to shoulder height while the position of the third finger's tip on the side being measured was marked on the wall. Participants then lowered the arm not being measured and reached sideways as far as possible with the arm being measured. The position of furthest reach was marked and the difference between the two marks calculated. The mean of the three trials on each side was used for analyses.
Falls
A fall was defined as “an unexpected event in which the participant comes to rest on the ground, floor, or lower level” (World Health Organization, Citation2021). At 5-year follow-up, participants were asked to record any fall monthly for 12 months by questionnaire. In the questionnaire, participants were asked if they had experienced any fall in the month and, if yes, to report the dates, location and any reason of the fall(s), and any injuries from the fall(s). An injurious fall was defined as at least one fall that caused any injuries in the month. We gave participants three monthly questionnaires at a time and they returned them via a pre-paid envelope. A research assistant phoned participants to confirm if there were any falls if questionnaires were not returned within two weeks of the end of each three months. Those who fell more than once within 12 months were classified as having multiple falls. Three count/binary variables were used for analyses: number of falls, number of injurious falls, and multiple falls (Yes/No).
Anthropometry and other factors
Height was measured using a stadiometer (The Leicester height measure, Invicta Plastics Ltd, Oadby, England), weight using a single set of calibrated scales (Heine, Dover NH USA), and body mass index (BMI) calculated (weight/height2, kg/m2). We used a standardised questionnaire to collect current smoking status (Yes/No), education level (Primary school/high school [less than or up to grade 10]; high school/college [completed grade 12]; tertiary institution [university, College of Advanced Education (CAE), or other tertiary institution]), hours of employment (0, less than or equal to 20 or >20 h per week), menopausal status, marital status. We also took venous blood samples, and assayed serum 25-hydroxyvitamin D level (25OHD) using liquid chromatography (LC)-tandem mass spectrometry (LC-MS/MS). This assay measures 25OHD2 and 25OHD3 separately with a coefficient of variation (CV) 3% to 6%, using an internal standard.
Statistical analyses
These were exploratory analyses undertaken in a cohort which had the primary aim of determining the incidence of falls measured prospectively in middle-aged women (Wang et al., Citation2020) so a priori sample size calculations were not performed as recommended by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Vandenbroucke et al., Citation2014). Mean (standard deviation, SD) or median (interquartile range, IQR) was used as appropriate to describe continuous variables; number (%) was used to describe categorical variables.
We used linear mixed-effects models to examine associations of baseline and 5-year change in time spent sedentary, in LPA and MVPA with change in LMS and balance measures over 5 years by including exposure of interest (e.g. baseline time spent sedentary) and an interaction term with time (e.g. baseline time spent sedentary × time). The beta coefficients for the exposure of interest indicate the cross-sectional association of the exposure with the outcome at baseline, while the coefficients for the interaction indicate the association of the exposure with the change of outcome over 5 years. These analyses were adjusted for confounders (age, weight, height, education, employment, marital status smoking, menopausal status, serum 25-hydroxyvitamin D level at baseline), which were selected based on biological and statistical rationales using three steps. Step 1: Age, height, and weight at baseline were compulsory covariates and included in all models. Step 2: We considered other potential confounders based on biological plausibility, including baseline and change in menopausal status, educational level, smoking, marital status, history of fractures, employment, and serum 25-hydroxyvitamin D level at baseline. Step 3: we tested if these potential confounders meet the assumption for confounding using statistical methods, as previously done (Wu, Callisaya, et al., Citation2017).
Each multivariable model of the associations between 5-year change in the exposures of sedentary time, LPA and MVPA with change in each outcome were also adjusted for the baseline value of exposure.
We then adjusted for MVPA when sedentary time was the exposure and vice versa. Similarly, we adjusted for MVPA when LPA was the exposure. We did not adjust for sedentary time when LPA was the exposure or vice versa because of collinearity (Chastin et al., Citation2014).
Negative binomial/Poisson regressions were used as appropriate to assess associations of baseline and 5-year change in time spent sedentary and in LPA and in MVPA with one-year incidence of any falls/injurious falls (count variables) at 5-year follow-up. Log-binomial regressions were used to assess associations of baseline and 5-year change in each exposure with one-year incidence of multiple falls. As aforementioned, we conducted the same adjustments in these models.
All analyses were performed in Stata version 16.0 (Stata Corp, College Station, TX, USA), and a two-tailed p value <0.05 was considered statistically significant.
Results
Of 347 women at baseline, 278 participated in the 5-year follow-up. Among 347 women, at baseline, 39 were excluded because of insufficient number of valid accelerometer days or outcome not being measured; thus, 308 women were included in the analyses. Among 278 women who participated the 5-year follow-up, 115 (42%) participants reported at least one fall over one year. presents the baseline characteristics of the participants. The mean number (SD) of valid days of accelerometer was 7.34 (0.97). The median values for sedentary time, and time spent in LPA and MVPA were 535, 267, and 37 min/day, respectively ().
Table 1. Baseline characteristics of participants (N = 308).
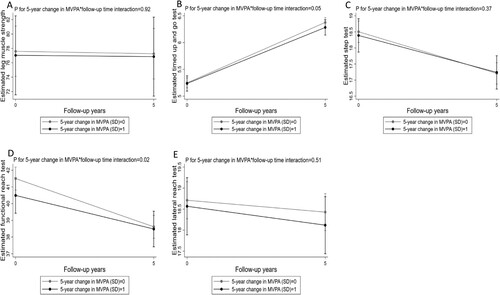
After adjustment for confounders, higher baseline MVPA (per SD of 28 min) was associated with higher LMS (β = 4.65 kg/SD; 95% CI, 1.37–7.93) and better performance on TUG (β = −0.09 s/SD; 95% CI, –0.18 to –0.01) but baseline MVPA was not associated with change in these outcomes over 5 years (P for MVPA*time interaction 0.27 and 0.54 respectively, (a and b)). Baseline MVPA was not associated with FRT at baseline but was associated with a greater decrease in FRT (β = −0.87 cm/SD; 95% CI, –1.57 to –0.17) (P for MVPA*time interaction = 0.02, (d)). Increased MVPA over 5 years was associated with less deterioration in performance on FRT (β = 0.88 cm/SD; 95% CI, 0.14–1.61, respectively) (P for MVPA*time interaction = 0.02, (d)).
Figure 1. Multivariable mixed effects model for estimated leg muscle strength and balance measures with 95% CIs at baseline and five-year follow-up for pre-specified values of baseline MVPA. Baseline MVPA was standardised and pre-specified values were 0 and 1 standard deviation (SD). The coefficient for the interaction between baseline MVPA and follow-up time was demonstrated by the difference between the two slopes (black and gray solid lines), that is, the difference in the five-year change of the outcome for one-SD increase of baseline MVPA. The coefficient for baseline MVPA was demonstrated by the difference in estimated values at baseline (black and gray points at year 0). The models included baseline MVPA, follow-up time, and the interaction between baseline MVPA and follow-up time, adjusted for baseline age, weight (including its interaction with time), height, education, employment, marital status, smoking, menopausal status, serum 25-hydroxyvitamin D levels and baseline sedentary time.
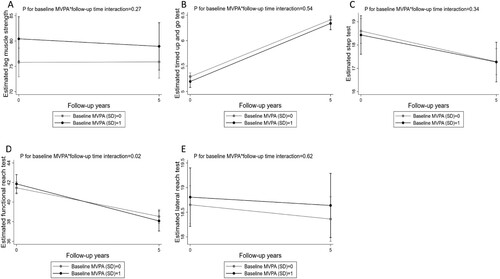
Figure 2. Multivariable mixed effects model for estimated leg muscle strength and balance measures with 95% CIs at baseline and five-year follow-up for pre-specified values of 5-year change in MVPA. 5-year change in MVPA was standardised and pre-specified values were 0 and 1 standard deviation (SD). The coefficient for the interaction between 5-year change in MVPA and follow-up time was demonstrated by the difference between the two slopes (black and gray solid lines), that is, the difference in the five-year change of the outcome for one-SD increase of 5-year change in MVPA. The coefficient for 5-year change in MVPA was demonstrated by the difference in estimated values at baseline (black and gray points at year 0). The models included 5-year change in MVPA, follow-up time, and the interaction between 5-year change in MVPA and follow-up time, adjusted for baseline age, weight (including its interaction with time), height, education, employment, marital status, smoking, menopausal status, serum 25-hydroxyvitamin D levels and 5-year change in sedentary time.
Increased sedentary time over 5 years was associated with more deterioration in performance on FRT (β = −0.82 cm/SD; 95% CI, –1.58 to –0.07) (P for sedentary time*time interaction = 0.03, Supplementary Figure 2D, online resource). Higher baseline LPA was associated with an increased risk of falls (IRR = 1.27, 95% CI: 1.02, 1.57, ).
Table 2. Associations between sedentary time and time spent in light physical activity and in MVPA with 1-year incident/injurious/multiple falls.
There were no other associations of baseline or change in sedentary time or time spent in LPA and MVPA with any outcome.
Discussion
To our knowledge, this is the first study describing longitudinal associations between objectively measured physical activity and sedentary time with muscle strength, balance, and incident falls in middle-aged women. Its findings suggest that higher baseline MVPA may be beneficial for muscle strength and balance (as measured by TUG) at baseline, perhaps because baseline levels reflect an individual's history of MVPA; however, increasing MVPA in the medium term has little effect on change in LMS or balance outcomes in middle-aged women. The association of higher baseline LPA with an increased risk of falls is unexpected but we postulate this could be due to higher levels of LPA leading to higher exposure to environmental hazards (for example uneven surfaces or loose gravel) for falling.
Data on associations between objectively measured physical activity with musculoskeletal outcomes in middle-aged women are sparse. Results of cross-sectional studies are generally consistent with our results but ours is the first longitudinal study to investigate this. The four cross-sectional accelerometer-based studies found that greater MVPA was associated with greater leg muscle strength (Chahal et al., Citation2014; Straight et al., Citation2015), better postural stability (Willoughby & Copeland, Citation2015) and balance performance (Cooper et al., Citation2020). However, our longitudinal data found that increasing MVPA was not associated with change in LMS nor with most balance measures.
The null finding of our longitudinal data might be because the participants had good LMS and balance performance at baseline compared to older women (aged 60–69 years) (Isles et al., Citation2004), which may lead to slower loss of LMS/balance function. It is also possible that cross-sectional associations are seen because longer-term MVPA maybe beneficial for LMS and balance and baseline levels might better reflect an individual's history of MVPA. Alternatively, other kinds of activity may be more beneficial to LMS. For example, a resistance-training programme in line with American Heart Association guidelines has been demonstrated to result in increased muscle strength (Gennuso et al., Citation2013). While a using dynamometry (TTM Muscular Meter) is challenging for frail individuals, this is unlikely to affect our results in these younger women with good LMS at baseline. We are not aware of any studies comparing isometric and isokinetic muscle strength as falls risk factors. Isokinetic exercise can be considered functionally superior to isometric exercise, providing more significant improvements in muscle strength measurements in patients with knee osteoarthritis (Bahsi et al., Citation2022) though such exercise did not demonstrate improvements in postural sway in older adults (Kay et al., Citation2020). Future longitudinal studies are needed that recruit people with poorer balance, assess other types of physical activity besides ambulatory physical activity, and examine the associations between physical activity with isokinetic strength in middle-aged people.
An exception to the pattern of MVPA lacking associations with most balance measures is the surprising finding that higher baseline MVPA was associated with a decrease in FRT; however, increasing MVPA was associated with less deterioration in performance on FRT over 5 years. The decrease in FRT related to baseline MVPA might be a result of regression to the mean (Barnett, Citation2004), that is, greater baseline MVPA may reflect a higher level of FRT at baseline although not statistically significant and people with higher levels of FRT at baseline may have a higher decrease over 5 years. Although the effect size (β = 0.88) is slightly smaller than the estimated minimal clinically important difference (MCID) of the measure of 0.92 (Wyrwich, Citation2004), an accumulation over longer duration may still be clinically important. Therefore, we suggest that increasing MVPA in mid-life might be beneficial for health gains over a longer duration, though this needs confirmation in future research.
Higher baseline sedentary time was not associated with LMS and any balance measures at baseline but increasing sedentary time was associated with a greater decrease in performance on FRT over 5 years. Our cross-sectional finding is consistent with the only one previous cross-sectional study in 49 middle-aged women (mean age = 56.6, SD = 4.1 years), showing no significant association between sedentary time and postural stability or peak torque of the knee extensors or flexors, after adjusting for MVPA (Willoughby & Copeland, Citation2015). However, cross-sectional studies in older adults conducted by Santos et al. (Citation2012) and Davis et al. (Citation2014) both reported objectively measured sedentary time to be associated with measures of balance and lower extremity function independently of MVPA. It might be because the effect of sedentary behaviour accumulates as people age and is more likely to be observed in older adults. Indeed, we observed a longitudinal relationship between increasing sedentary time and higher decrease in FRT over 5 years and the effect size (β = −0.82) is only slightly smaller than the estimated MCID of the measure of 0.92.
Our result that higher baseline LPA was associated with an increased risk of incident falls 5 years later is consistent with that of the only other longitudinal study of physical activity and falls which included middle-aged women (Bea et al., Citation2017). However, that study also included older women (aged 50–79 years) and did not examine the relationship specifically in middle-aged women. This is important as a previous meta-analysis of prospective cohort studies (Lee, Citation2020) found that very high amount of MVPA was associated with decreased risk of falling in older adults compared to low amount of MVPA. Although it is intuitive that physical activity has beneficial effect on muscular skeletal health and consequently decreases the risk of falls, physical activity may also increase the risk of falls because of a greater exposure to potentially fall associated situations in middle-aged adults. As our previous analyses (Wang et al., Citation2020) in the same sample showed that 60% of falls were due to tripping and slipping and 13% for environmental hazards (for example uneven surfaces or loose gravel), and the causes of tripping and slipping were also likely to be environmental factors, such as slopes, uneven pathways and ramps. Risk factors for falls in middle-aged adults might be different from that in older adults, with a more important role of physical activity related environmental hazards in terms of causes of falling in middle-aged adults. However, this needs to be clarified in future research. Future studies should also explore modalities of physical activity that are safe for active people, such as swimming or high intensity progressive resistance training (Kanegusuku et al., Citation2015; Merom et al., Citation2014).
The key strengths of this study were objective quantification of physical activity and sedentary time and its reporting of longitudinal study data in an under-investigated population. The objective measurement of physical activity and sedentary time is important as questionnaires may not capture unstructured physical activity or LPA (e.g. shuffling) (Amagasa et al., Citation2017) and could over-report physical activity while under-report sedentary behaviours (Dyrstad et al., Citation2014). However, as with all waist-mounted monitors, accelerometer is limited in its capacity to capture non-ambulatory activity such as cycling, swimming, or resistance training. Another limitation was missing data due to loss to follow-up. Women lost to follow up had lower LMS and poorer balance than those retained, which may lead to an underestimation of the effect size of the association between PA and sedentary time with LMS and balance. However, we used linear mixed-effects models to minimise the impact of missing data by maximum likelihood estimation. Although this is a longitudinal study, we cannot exclude the possibility of reverse causation – it is possible if that those who have less decline in balance performance over 5 years might be more likely to increase physical activity. However, given that randomised controlled trials demonstrate that various types of physical exercise such as balance exercise programme do improve balance in older adults (Papalia et al., Citation2020), some degree of causality is likely. The women in this cohort had participated in a behavioural intervention including physical activity to improve osteoporosis-preventive behaviours, thus the levels of physical activity might be higher than the general population of women in this age group. However, the time spent in MVPA in our study at 12 years (about 259 min/week) was similar to that in adults aged 45–54 years in 2011–2012 Australian Health Survey (Australian Bureau of Statistics, Citation2013) (about 239 min/week of MVPA, walking for fitness and transport), suggesting the impact of this is likely to be small. Selection bias might exist due to 64% response rate, However, although the proportion of current smokers (17%) in the sample was lower than the Tasmanian prevalence of daily smoking (29%) in women aged 24–44 years in 1988, the wide spread of socioeconomic factors like educational level and the unemployment rate approximates the overall population figures. In addition, women who had previous bone density testing (which in this age group is likely to only have occurred to investigate potential bone disease) and who had a range of conditions that might affect bone density were excluded from the original randomised controlled trial. Therefore, the study findings are likely to be generalisable to white women who were healthy at the age of study entry but not those with conditions potentially affecting bone health.
In conclusion, higher baseline MVPA may be beneficial for LMS and balance, perhaps because baseline levels reflect an individual's history of MVPA. However, increasing MVPA in the medium term has little effect on change in LMS and balance in middle-aged women. Additional research is needed to determine the impact of typical physical activity not captured by accelerometer, such as resistance training, on LMS and balance in middle-aged adults. The detrimental association of LPA with falls may be due to a greater exposure to environmental hazards in midlife, which needs to be clarified in future research.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical Standards.
Sponsor's role
The funders had no role in the design of the study, in the collection, analysis, or interpretation of the data; in the writing of the manuscript, or in the decision to publish the results.
Author contributions
Study design: Feitong Wu, Tania Winzenberg, Graeme Jones, and Michele Callisaya. Study conduct: Tania Winzenberg and Feitong Wu. Data collection and management: Feitong Wu, Tania Winzenberg, and Mengmeng Wang. Data analysis: Mengmeng Wang and Feitong Wu. Data interpretation: all authors. Drafting manuscript: Mengmeng Wang. Revising manuscript content: all authors. Approving final version of manuscript: all authors. Mengmeng Wang takes responsibility for the integrity of the data analysis.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Supplemental Material
Download PDF (1.1 MB)Acknowledgements
We thank all the volunteers and participants involved in the present study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abe, T., Thiebaud, R. S., Loenneke, J. P., & Mitsukawa, N. (2015). Association between toe grasping strength and accelerometer-determined physical activity in middle-aged and older women. Journal of Physical Therapy Science, 27(6), 1893–1897. https://doi.org/10.1589/jpts.27.1893
- Amagasa, S., Fukushima, N., Kikuchi, H., Takamiya, T., Oka, K., & Inoue, S. (2017). Light and sporadic physical activity overlooked by current guidelines makes older women more active than older men. The International Journal of Behavioral Nutrition and Physical Activity, 14(1), 59. https://doi.org/10.1186/s12966-017-0519-6
- Australian Bureau of Statistics. (2013). Australian health survey: physical activity. Retrieved August 10, 2021, from https://www.abs.gov.au/statistics/health/health-conditions-and-risks/australian-health-survey-physical-activity/latest-release#data-download.
- Bahsi, A., Altindag, O., Akaltun, M. S., Aydeniz, A., Avci, E. E., & Gur, A. (2022). Comparison of the effects of isokinetic, isometric, and isotonic exercises on knee osteoarthritis using ultrasound. Cureus, 14(8), e28324. https://doi.org/10.7759/cureus.28324
- Barnett, A. G. (2004). Regression to the mean: What it is and how to deal with it. International Journal of Epidemiology, 34(1), 215–220. https://doi.org/10.1093/ije/dyh299
- Bea, J. W., Thomson, C. A., Wallace, R. B., Wu, C., Seguin, R. A., Going, S. B., LaCroix, A., Eaton, C., Ockene, J. K., LaMonte, M. J., Jackson, R., Jerry Mysiw, W., & Wactawski-Wende, J. (2017). Changes in physical activity, sedentary time, and risk of falling: The women's health initiative observational study. Preventive Medicine, 95, 103–109. https://doi.org/10.1016/j.ypmed.2016.11.025
- Brooks, A. G., Gunn, S. M., Withers, R. T., Gore, C. J., & Plummer, J. L. (2005). Predicting walking METs and energy expenditure from speed or accelerometry. Medicine & Science in Sports & Exercise, 37(7), 1216–1223. https://doi.org/10.1249/01.mss.0000170074.19649.0e
- Caban-Martinez, A. J., Courtney, T. K., Chang, W. R., Lombardi, D. A., Huang, Y. H., Brennan, M. J., Perry, M. J., Katz, J. N., Christiani, D. C., & Verma, S. K. (2015). Leisure-time physical activity, falls, and fall injuries in middle-aged adults. American Journal of Preventive Medicine, 49(6), 888–901. https://doi.org/10.1016/j.amepre.2015.05.022
- Callisaya, M. L., Blizzard, L., Schmidt, M. D., Martin, K. L., McGinley, J. L., Sanders, L. M., & Srikanth, V. K. (2011). Gait, gait variability and the risk of multiple incident falls in older people: A population-based study. Age and Ageing, 40(4), 481–487. https://doi.org/10.1093/ageing/afr055
- Chahal, J., Lee, R., & Luo, J. (2014). Loading dose of physical activity is related to muscle strength and bone density in middle-aged women. Bone, 67, 41–45. https://doi.org/10.1016/j.bone.2014.06.029
- Chastin, S. F., Mandrichenko, O., Helbostadt, J. L., & Skelton, D. A. (2014). Associations between objectively-measured sedentary behaviour and physical activity with bone mineral density in adults and older adults, the NHANES study. Bone, 64, 254–262. https://doi.org/10.1016/j.bone.2014.04.009
- Cooper, R., Stamatakis, E., & Hamer, M. (2020). Associations of sitting and physical activity with grip strength and balance in mid-life: 1970 British cohort study. Scandinavian Journal of Medicine & Science in Sports, 30(12), 2371–2381. https://doi.org/10.1111/sms.13793
- Davis, M. G., Fox, K. R., Stathi, A., Trayers, T., Thompson, J. L., & Cooper, A. R. (2014). Objectively measured sedentary time and its association with physical function in older adults. Journal of Aging and Physical Activity, 22(4), 474–481. https://doi.org/10.1123/JAPA.2013-0042
- Dore, D., Quinn, S., Ding, C., Winzenberg, T., Zhai, G., Cicuttini, F., & Jones, G. (2010). Natural history and clinical significance of MRI-detected bone marrow lesions at the knee: A prospective study in community dwelling older adults. Arthritis Research & Therapy, 12(6), R223. https://doi.org/10.1186/ar3210
- Dyrstad, S. M., Hansen, B. H., Holme, I. M., & Anderssen, S. A. (2014). Comparison of self-reported versus accelerometer-measured physical activity. Medicine & Science in Sports & Exercise, 46(1), 99–106. https://doi.org/10.1249/MSS.0b013e3182a0595f
- EI Haber, N., Erbas, B., Hill, K. D., & Wark, J. D. (2008). Relationship between age and measures of balance, strength and gait: Linear and non-linear analyses. Clinical Science, 114(12), 719–727. https://doi.org/10.1042/CS20070301
- Gennuso, K. P., Zalewski, K., Cashin, S. E., & Strath, S. J. (2013). Resistance training congruent with minimal guidelines improves function in older adults: A pilot study. Journal of Physical Activity and Health, 10(6), 769–776. https://doi.org/10.1123/jpah.10.6.769
- Isles, R. C., Choy, N. L., Steer, M., & Nitz, J. C. (2004). Normal values of balance tests in women aged 20-80. Journal of the American Geriatrics Society, 52(8), 1367–1372. https://doi.org/10.1111/j.1532-5415.2004.52370.x
- Kanegusuku, H., Queiroz, A. C., Silva, V. J., de Mello, M. T., Ugrinowitsch, C., & Forjaz, C. L. (2015). High-intensity progressive resistance training increases strength with no change in cardiovascular function and autonomic neural regulation in older adults. Journal of Aging and Physical Activity, 23(3), 339–345. https://doi.org/10.1123/japa.2012-0324
- Kay, A. D., Blazevich, A. J., Fraser, M., Ashmore, L., & Hill, M. W. (2020). Isokinetic eccentric exercise substantially improves mobility, muscle strength and size, but not postural sway metrics in older adults, with limited regression observed following a detraining period. European Journal of Applied Physiology, 120(11), 2383–2395. https://doi.org/10.1007/s00421-020-04466-7
- Kozey-Keadle, S., Libertine, A., Lyden, K., Staudenmayer, J., & Freedson, P. S. (2011). Validation of wearable monitors for assessing sedentary behavior. Medicine & Science in Sports & Exercise, 43(8), 1561–1567. https://doi.org/10.1249/MSS.0b013e31820ce174
- Lee, J. (2020). The association between physical activity and risk of falling in older adults: A systematic review and meta-analysis of prospective cohort studies. Geriatric Nursing, 41(6), 747–753. https://doi.org/10.1016/j.gerinurse.2020.05.005
- Merom, D., Stanaway, F. F., Handelsman, D. J., Waite, L. M., Seibel, M. J., Blyth, F. M., Naganathan, V., & Cumming, R. G. (2014). Swimming and other sporting activities and the rate of falls in older men: Longitudinal findings from the concord health and ageing in Men project. American Journal of Epidemiology, 180(8), 830–837. https://doi.org/10.1093/aje/kwu199
- Papalia, G. F., Papalia, R., Diaz Balzani, L. A., Torre, G., Zampogna, B., Vasta, S., Fossati, C., Alifano, A. M., & Denaro, V. (2020). The effects of physical exercise on balance and prevention of falls in older people: A systematic review and meta-analysis. Journal of Clinical Medicine, 9(8), 2595. https://doi.org/10.3390/jcm9082595
- Santos, D. A., Silva, A. M., Baptista, F., Santos, R., Vale, S., Mota, J., & Sardinha, L. B. (2012). Sedentary behavior and physical activity are independently related to functional fitness in older adults. Experimental Gerontology, 47(12), 908–912. https://doi.org/10.1016/j.exger.2012.07.011
- Scott, D., Blizzard, L., Fell, J., & Jones, G. (2011). Prospective associations between ambulatory activity, body composition and muscle function in older adults. Scandinavian Journal of Medicine & Science in Sports, 21(6), e168–e175. https://doi.org/10.1111/j.1600-0838.2010.01229.x
- Scott, D., Ebeling, P. R., Sanders, K. M., Aitken, D., Winzenberg, T., & Jones, G. (2015). Vitamin d and physical activity status: Associations with five-year changes in body composition and muscle function in community-dwelling older adults. The Journal of Clinical Endocrinology & Metabolism, 100(2), 670–678. https://doi.org/10.1210/jc.2014-3519
- Sipila, S., Tormakangas, T., Sillanpaa, E., Aukee, P., Kujala, U. M., Kovanen, V., & Laakkonen, E. K. (2020). Muscle and bone mass in middle-aged women: Role of menopausal status and physical activity. Journal of Cachexia, Sarcopenia and Muscle, 11(3), 698–709. https://doi.org/10.1002/jcsm.12547
- Straight, C. R., Ward-Ritacco, C. L., & Evans, E. M. (2015). Association between accelerometer-measured physical activity and muscle capacity in middle-aged postmenopausal women. Menopause (New York, N. Y.), 22(11), 1204–1211. https://doi.org/10.1097/GME.0000000000000447
- Takae, R., Hatamoto, Y., Yasukata, J., Kose, Y., Komiyama, T., & Yoshimura, E. (2020). Association of lower-extremity muscle performance and physical activity level and intensity in middle-aged and older adults: A doubly labeled water and accelerometer study. The Journal of Nutrition, Health & Aging, 24(9), 1023–1030. https://doi.org/10.1007/s12603-020-1514-1
- Vandenbroucke, J. P., von Elm, E., Altman, D. G., Gotzsche, P. C., Mulrow, C. D., Pocock, S. J., Poole, C., Schlesselman, J. J., Egger, M., & Initiative, S. (2014). Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. International Journal of Surgery, 12(12), 1500–1524. https://doi.org/10.1016/j.ijsu.2014.07.014
- Wang, M., Wu, F., Callisaya, M. L., Jones, G., & Winzenberg, T. (2020). Incidence and circumstances of falls among middle-aged women: A cohort study. Osteoporosis International, 32(3), 505–513. https://doi.org/10.1007/s00198-020-05617-4
- Ward-Ritacco, C. L., Adrian, A. L., Johnson, M. A., Rogers, L. Q., & Evans, E. M. (2014). Adiposity, physical activity, and muscle quality are independently related to physical function performance in middle-aged postmenopausal women. Menopause (New York, N. Y.), 21(10), 1114–1121. https://doi.org/10.1097/GME.0000000000000225
- Willoughby, T., & Copeland, J. L. (2015). Sedentary time is not independently related to postural stability or leg strength in women 50-67 years old. Applied Physiology, Nutrition, and Metabolism, 40(11), 1123–1128. https://doi.org/10.1139/apnm-2015-0066
- Winzenberg, T., Oldenburg, B., Frendin, S., De Wit, L., Riley, M., & Jones, G. (2006). The effect on behavior and bone mineral density of individualized bone mineral density feedback and educational interventions in premenopausal women: A randomized controlled trial [NCT00273260]. BMC Public Health, 6, 12. https://doi.org/10.1186/1471-2458-6-12
- World Health Organization. (2021). Falls. Retrieved September 21, 2021, from https://www.who.int/en/news-room/fact-sheets/detail/falls.
- Wu, F., Callisaya, M., Wills, K., Laslett, L. L., Jones, G., & Winzenberg, T. (2017). Both baseline and change in lower limb muscle strength in younger women are independent predictors of balance in middle age: A 12-year population-based prospective study. Journal of Bone and Mineral Research, 32(6), 1201–1208. https://doi.org/10.1002/jbmr.3103
- Wu, F., Wills, K., Laslett, L. L., Oldenburg, B., Jones, G., & Winzenberg, T. (2017). Moderate-to-vigorous physical activity but not sedentary time is associated with musculoskeletal health outcomes in a cohort of Australian middle-aged women. Journal of Bone and Mineral Research, 32(4), 708–715. https://doi.org/10.1002/jbmr.3028
- Wu, F., Wills, K., Laslett, L. L., Riley, M. D., Oldenburg, B., Jones, G., & Winzenberg, T. (2018). Individualized fracture risk feedback and long-term benefits after 10 years. American Journal of Preventive Medicine, 54(2), 266–274. https://doi.org/10.1016/j.amepre.2017.10.018
- Wyrwich, K. W. (2004). Minimal important difference thresholds and the standard error of measurement: Is there a connection? Journal of Biopharmaceutical Statistics, 14(1), 97–110. https://doi.org/10.1081/BIP-120028508