

ABSTRACT
Background
In early 2020, the COVID-19 pandemic emerged bringing risk of disease, disability and death to all Americans. As public health officials scrambled to respond, dental offices were shuttered leaving little access to dental care.
Methods
Collaborating with medical colleagues and partnering with the local public health department, the Asian Health Services (AHS) dental team developed a preparedness plan to ensure the safe and effective ongoing delivery of oral health care services, respond to the national public health state of emergency and support local public health efforts to contain the pandemic.
Results
AHS dental services remained operational throughout the COVID-19 pandemic due to the swift and strategic response of the dental team. COVID-19 contact tracing, testing and vaccination became new services rendered by dental personnel, which are now integrated into policies, programs and services. Professional education and training were also updated to ensure sustained preparedness.
Conclusions
By having a comprehensive and coordinated preparedness plan in place, AHS was able to effectively support public health efforts and serve the oral health care needs of the community.
Practical Implications
Preparedness efforts implemented by a coordinated effort between AHS’s medical and dental leadership in cooperation with local public health officials during the recent COVID-19 pandemic may serve as a future model for all health care professionals.
Asian Health Services (AHS) is a federally qualified health center (FQHC), located in Oakland, California. Since its founding in 1974, AHS has been a trusted leader in health care access and advocacy for Asians and Pacific Islanders. Today, AHS provides integrated medical, dental, behavioral and specialty mental health care services to more than 50,000 patients in Alameda County and the surrounding areas.
In early 2020, health care services at AHS, like other health care providers across the United States, were significantly disrupted by the emergence of the COVID-19 pandemic. COVID 19, also known as SARS CoV 2 or coronavirus disease 2019, initiated an unprecedented panic across the globe. In the United States, public health officials scrambled to understand the virus and its scope. Legislators, researchers, health care professionals and the public at large watched and waited anxiously for direction and reassurance. Daily reports conflicted, and fear grew steadily as the virus spread.Citation1
What made this virus so challenging according to Center for Disease Control and Prevention (CDC) experts was the fact that it had never been seen in a human, and as such, no one was immune to it. In addition, officials recognized that the upper respiratory system was the primary target of the virus which spread easily from person to person through aerosol droplets, causing severe disease, disability and death. With no immune protection and no vaccine readily available, the crisis intensified.Citation2,Citation3
For health care professionals, new regulations requiring specialized face masks and infection control procedures left many dental practices in the dark as infection control supplies quickly became redirected under federal and state mandates toward first responders and front-line professionals.Citation4 Those dental practices that remained open to provide emergency dental care were forced to deal with staff furloughs, layoffs, reduced number of patients and the high costs of supplies.
In Oakland, California, AHS began observing patient cancellations at a rate higher than usual, like those observed in 2003 during the SARS period. Professional conferences were cancelled, as word of a viral outbreak in China circulated. AHS leadership summoned health center officers, including the chief medical officer and chief dental officer, and launched a preparedness plan to respond to a potential epidemic.
Methods
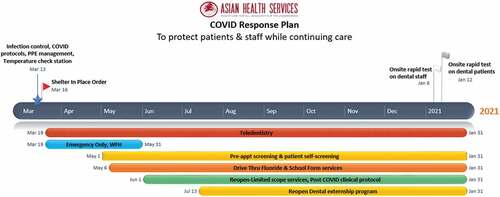
AHS created a health center preparedness plan (), which proved to be the most important strategy for ensuring continuous, safe and effective delivery of oral health care services to patients; responding to the national public health state of emergency; and for supporting local public health efforts to contain the pandemic. It created a fundamental operational guide, which included communication, staffing, scheduling, financing and regulatory compliance. The following components were incorporated into the AHS “Public Health Preparedness Plan” that has subsequently served as the framework for the health center’s ongoing emergency preparedness efforts.
Figure 1. The health center preparedness plan proved to be the most important strategy for ensuring continuous, safe and effective delivery of oral health care services to patients.
Convene Leadership Response Team
AHS convened a leadership response team, with representatives from key departments within the health center. The response team met daily to discuss pandemic alerts and information received from federal, state and local authorities and its implication for the health center. The response team continues to meet regularly and has become an integral component of the health center’s future readiness response.
Consider and Plan for All Possible Scenarios and Events
As a first step, the leadership team had to consider how to transition services from in person to virtual, continue urgent in-person care, advance health center policies and protocols to align and comply with new COVID-19 regulations and maintain viable administrative and practice models. To accomplish this, AHS reviewed current policies and protocols, explored a series of potential COVID-19-related scenarios and events and then considered how such events would impact AHS’s existing operations. The group then laid out a preparedness plan for each potential event.
Consider All Solutions Including the Use of Advanced Technologies
Once all potential events were considered, the response team laid out potential solutions and developed an operational plan that would create a roadmap for the health center’s leadership, providers, staff and patients. Securing a mechanism for effective communication between the leadership and providers, as well as providers and patients was the primary objective for AHS.
Electronic equipment was purchased and distributed to all staff working from home, so that operations would continue seamlessly. Laptops, iPhones and iPads were used for communication and coordination of in-person and telehealth medical and services as well as COVID-19 screening, contact tracing and subsequently vaccines.
Teledental visits began on March 19, 2020, only four days after Gov. Gavin Newsom issued the executive stay at home order.Citation5 Staff conducted patient outreach by phone to assess patient needs, schedule appointments, fill prescriptions and address lab work and/or referrals. Many patients required technical assistance regarding the use of Zoom and other phone and virtual meeting technologies and staff were well prepared to provide it.
Conduct Education and Training
AHS developed and implemented COVID-19-specific education and training for all providers and staff. The education focused on COVID-19 facts as they were emerging and being reported by federal, state and local authorities. AHS monitored federal and state websites for regulatory updates; and policy changes were implemented daily to ensure compliance. Under the national public health state of emergency, the HIPAA regulation was relaxed to permit the use of nonsecure devices such as iPhones and tablets for virtual communication between providers and patients. This opened the door for broader telemedicine and teledental policies and an increase in use of telemedical and dental services to ensure ongoing access.
Protect Health Center Staff and Patients
As part of the health center’s efforts to ensure ongoing safety for staff and patients, the AHS leadership communicated regularly with the local public health department to learn and share information regarding COVID-19 screening and testing for both patients and staff, how to manage positive test results, contact tracing and follow-up. AHS followed CDC protocols for distancing and infection control and monitored the CDC’s COVID-19 reports daily. Adjustments to health center policies and protocols followed CDC recommendations as they were released.Citation6
An infection control committee consisting of clinical staff from all departments was formed. This group was assigned the role of monitoring federal and state regulations as well as professional guidelines, including and not limited to the CDC, the American Dental Association (ADA) and the California Dental Association (CDA), to identify any pertinent content that should be incorporated into health center policies and protocols.
In addition, AHS hired environmental engineering consultants to review the physical facilities and make strategic recommendations for each of the individual clinic sites. Occupational Safety and Health Administration (OSHA), Environmental Protection Agency (EPA) and American Medical Association (AMA) guidelines were identified for use by the health center. Together, with the consultants, the infection control committee updated policies and protocols based on CDC, OHSA, ADA, EPA, CDA and AMA recommendations, with strategies for distancing, including physical barriers as well as personal protective equipment (PPE) such as N95 masks, gowns, gloves and other equipment necessary to maintain safe clinical operations.Citation7,Citation8
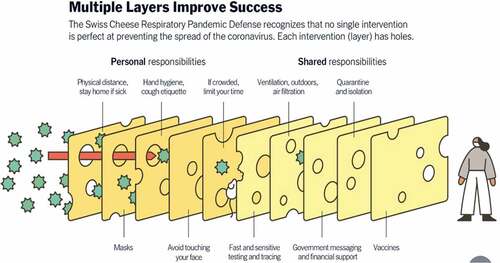
To ensure the best possible outcomes for preventing the spread of COVID-19 among staff and patients, AHS implemented the Swiss cheese model () The Swiss cheese model builds on the notion that no one preventive strategy is sufficient to prevent disease, disability and death. The analogy suggests that as with each slice of cheese, holes exist, so too do vulnerabilities exist in each preventive strategy. The model further suggests however that when slices of cheese are stacked together, the holes disappear. In this analogy, when several preventive strategies or safeguards are strategically executed, risk of transmission is diminished.Citation9 Therefore, when considering how to effectively prevent the spread of COVID 19, several preventive strategies should be employed and overlapped to ensure the successful break in the transmission of disease.
Figure 2. Asian health services implemented the Swiss cheese model to ensure the best possible outcomes for preventing the spread of COVID 19 among staff and patients.
In March 2020, AHS adopted the use of physical partitions made of Plexiglass to safeguard against the spread of disease. Barriers were set up in administrative offices as well as between staff workstations. Masks became mandatory for all staff and patients. Social distancing was implemented. Portable air cleaners and HVAC filters were installed to reduce any lingering airborne virus. The amount of time staff was permitted in the lunchroom was reduced to 15 minutes. And COVID-19 screening, testing, contact tracing and vaccination was initiated.
AHS also opened a vaccination clinic to serve community members. Several mass vaccination events took place. The first adult mass vaccination took place in April 2021 in Oakland with more than 500 Oakland residents received vaccination within three hours. Several dentists were present to assist with the vaccination efforts. Several more mass public vaccination events followed. The first pediatric mass vaccination event took place in December 2021.Citation10
New Roles and Responsibilities Including Expansion of Scope of Practice
Once COVID-19 Testing became available at the health center, dental staff were trained alongside of AHS medical colleagues. In August 2020, AHS was the first health center to be selected by the local public health department as a pilot site for testing dental patients for COVID 19. The successful pilot was then expanded and by January 2021, all health center patients were tested for COVID-19 prior to dental treatment. Between January and December 2021, 181 COVID-19 tests were administered by dental personnel. Of those, only one was COVID-19 positive. Between January and May of 2022, 3,019 tests were administered by dental personnel and 28 were COVID-19 positive.
When vaccinations became available, AHS dental providers were encouraged to participate in the CDC COVID-19 vaccination training. Those who participated were scheduled to deliver vaccines at local clinics and mass vaccination events. Between January 2021 and May 2022, a total of 40,693 individuals received vaccinations by AHS medical and dental staff. AHS staff working from home in all departments supported the community’s contact tracing efforts.
Contact tracing began between June November 2020. Within the local area, 6,480 community members tested positive. Of those, 4,154 persons were interviewed and provided guidance and COVID-19 resources. In addition, 1569 close contacts were identified. Of those, 1,267 persons were interviewed and were provided guidance and resources. Twenty four percent of total interviews were conducted in languages other than English – strengthening communication and trust between public health and non-English speaking communities in the county.
Create and Align a Financial Model That Supports Sustainability
To ensure fiscal responsibility and sustainability, AHS developed several financial models considering the health center’s patient pool and payment structure. The goal of this strategy was to ensure that new policies and/or protocols either limiting services or expanding them would be financially viable to the health center’s bottom line and not subject the health center to any fiscal vulnerability nor liability. The team then overlayed a financial model for each anticipated event, considering the fiscal viability of that model if it were implemented. This exercise established a level of confidence in practice management that was essential to AHS health center leadership. These models helped AHS prepare and respond promptly during the pandemic.
Despite strategic financial planning by AHS leadership, Medicaid reimbursement for dental services during this time period was not sufficient to support the tele dental care model being introduced. While telemedical payments were reimbursed at the same in-person encounter rate, tele dental visits were not. Tele dental visits were reimbursed using a fee for service model which only initially paid for triaging dental care. This created a financial burden to the health center and limited access to dental care for many of AHS’s patients.Citation11,Citation12
Collect Data and Monitor CQI
AHS embraces continuous quality improvement for all administrative and clinical operations. As such, the AHS data team collected and analyzed data regularly during this time. Given the number of interventions being established, the evaluation team monitored qualitative and quantitative data for each COVID-19 preventive strategy as well as the expanded role of dental providers in supporting local public health surveillance, screening, contact tracing and vaccination efforts.
Results
In response to the COVID-19 pandemic, which largely shuttered dental practices across the U.S., AHS leaned in and acted. Early on, health center leadership developed a flexible and wide-ranging preparedness plan to retain staff, sustain operations and promptly mobilize a strategic response should the virus take hold. AHS’s plan included several critical steps:
Convene leadership response team to lead, monitor, advice and support.
Consider and plan for all possible scenarios and events.
Consider all solutions including the use of advanced technologies.
Conduct education and training.
Protect health center staff and patients.
Maintain administrative and clinical services delivery.
Explore new roles and responsibilities including expansion of scope of practice.
Create and align a financial model that supports sustainability.
Collect data and monitor CQI.
When health officials declared the national public health state of emergency, AHS was prepared and ready to step into action shifting operations to tele health for both medical and dental services. Having the preparedness plan in place permitted the rapid transition of health care from largely in-person care to virtual. Health center providers and staff were readily able to assess patient needs, prioritize and triage patients, schedule urgent appointments, fill prescriptions and make referrals. For those patients needing immediate care, the AHS dental team was prepared to render treatment safely in person, as new CDC recommendations for advanced infection control policies and procedures were put in place.
Discussion
During a National Public Health State of Emergency or other period of public concern and fear, health care providers must serve as community leaders, demonstrating knowledge, strength and confidence offering full support and ongoing service delivery to the public. Having a public health emergency preparedness plan in place demonstrates a provider’s capacity and readiness to lead, advise and support the public during a period of crisis. It also ensures the ongoing and uninterrupted delivery of health care services to the public. Such a plan does not remove all challenges, however. During the COVID-19 pandemic, dental reimbursement was not sufficient to support adequate care for dental patients. More needs to be done to ensure that dental services are not impeded by policies that limit care and do not fully reimburse for care such as tele dental services. During the first year of the pandemic, medical, behavioral health and specialty mental telehealth visits were all reimbursed at rates similar to in-person rates. Teledental visits were paid a mere $15 to $17 dollars a visit.Citation13
Lessons Learned
Having a public health emergency preparedness plan in place helped AHS sustain operations, respond effectively to the needs of the patients, community during the national public health state of emergency and support local public health officials deal with the pandemic.
Creating and convening a group to lead, monitor events and responses and advise helped to curtail the fear and concern of the public, staff and patients.
Considering all potential events, creating strategies to respond to all events and overlaying financial models will help to maintain operations and sustain fiscal viability.
Conducting education and training to ensure that all providers and staff are fully aware and knowledgeable of federal and state health care and health provider regulations and guidelines; health center updated policies and protocols; and any new compliance measures will more effectively support ongoing care and operations.
Supporting the local public health infrastructure by expanding dental scope of practice to support surveillance, testing, contact tracing and vaccinations, will broaden its capacity to curtail an epidemic and keep the public safe.
Conclusions
The COVID-19 pandemic caught nearly all Americans by surprise. Few were prepared for the disease, disability and death that resulted. With this in mind, all health care organizations should develop a public health preparedness plan, educate providers and staff and conduct practice exercises to ensure ongoing preparedness. AHS realized early on that developing a preparedness plan to address the emerging needs of the health center was critical to meeting the comprehensive needs of its patients. The collaboration and partnership between AHS and the local public health department and dental societies were critical in supporting disease containment efforts.Citation14 The public health role dental professionals may take in such circumstances cannot be overstated.
Practical Implications
Experience and knowledge gained from the COVID-19 pandemic call for improvements in preparedness by all health care provider groups, as well as changes to policies, programs and services. Efforts implemented during the recent National Public Health State of Emergency should serve as a future framework and call to action for all health care professionals. To better prepare oral health care professionals in their support of broader public health efforts during a public health crisis, all dental practices should develop a public health preparedness plan. Such a plan should include annual leadership and staff training, with a focus on population health, epidemiology, surveillance, community-based prevention, professional intervention and community action in the event of a public health or community crisis. The preparedness plan should also include provisions for acting upon emergent regulatory changes as well as updates to policies and protocols; implementation strategies; and continuous quality improvement.
Additional information
Notes on contributors
Huong Le
Huong Le, DDS, MA, Chief Dental Officer, Asian Health Services, faculty member at UCSF School of Dentistry, Western University College of Dental Medicine, Arizona School of Dentistry and Oral Health, University of Pacific and California North State University, College of Dental Medicine.
Mary E. Foley
Mary E. Foley, MPH is the Executive Director of the Medicaid, Medicare, CHIP Services Dental Association and Evaluation Consultant for several of the Western universities, College of Dental Medicine HRSA grants.
References
- Muralidar S, Ambi SV, Sekaran S, Krishnan UM. The emergence of COVID-19 as a global pandemic: understanding the epidemiology, immune response and potential therapeutic targets of SARS CoV 2. Biochimie. December 2020;179:85–5. 10.1016/j.biochi.2020.09.018. Epub 2020 Sep 22. PMCID: PMC7505773.
- Centers for Disease Control and Prevention. How COVID-19 spreads.
- Forthal DN, Buchmeier MJ. Why is COVID-19 so dangerous? UCI Health. April 29, 2020. Accessed June 22, 2022.
- Centers for Disease Control and Prevention. CDC updates COVID-19 infection prevention and control guidance. 2022.
- Executive Department State of California. Executive order N 33 20. 2020.
- Centers for Disease Control and Prevention. Healthcare workers: information on COVID 19. 2022.
- Unite States Department of Labor, Occupational Safety and Health Administration. Guidance on returning to work.
- Environmental Protection Agency. Air cleaners, HVAC filters and coronavirus (COVID 19). Accessed June 2020.
- Ngo T. To slow the spread of COVID 19, we need to bring back the Swiss cheese model of pandemic response. Health Affairs Forefront December 20, 2021. Accessed June 2022.
- Eykelbosh A. A rapid review of the use of physical barriers in nonclinical settings and COVID-19 transmission. National Collaborating Centre for Environmental Health. November 17, 2021.
- Stone W. Under financial strain, community health centers ramp up for coronavirus response. NPR March 24, 2020.
- California Health Care Foundation. The pandemic’s financial impact on California’s community health centers: largest centers suffer significant losses. 2021.
- California Department of Health Care Services. Teledentistry FAQs for medical dental providers during novel coronavirus (COVID 19) restrictions. MediCal Provider Handbook Section 4 Treating Beneficiaries:4 14 and 4 15. March 24, 2020.
- Aronoff D, Girling L, Hsieh K. covid-19.acgov.org/covid19-assets/docs/clinical-guidance/everybody-has-a-plan-dental-webinar-2020.09.24.pdf