

ABSTRACT
Background
Traumatic intrusion is considered one of the most severe dentoalveolar injuries; however, there is limited research detailing the management and treatment of these injuries, particularly in immature permanent teeth.
Case Description
This case report describes the management of a severe traumatic intrusion presenting with an uncomplicated crown fracture, pulp necrosis and external root resorption in a 7-year-old African American female. The left maxillary central incisor (tooth No. 9) was intruded approximately 10 mm and inaccessible. The tooth was orthodontically extruded over the course of five months. Once exposed, a regenerative endodontic procedure under oral sedation was completed. Clinical and radiographic examinations during the follow-up period showed cessation of the resorption process and discontinuation of signs and symptoms.
Practical Implications
This case demonstrates that severe intrusive injuries in immature permanent teeth can be effectively managed with revascularization even when initiation of revascularization must be delayed due to extended time needed for orthodontic repositioning.
Continuing Education Credit Available: The practice worksheet is available as supplemental material for this article: https://doi.org/10.1080/19424396.2023.2176580.
A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20
Traumatic dentoalveolar injuries occur very frequently within the pediatric population and most commonly effect the maxillary incisors.Citation1,Citation2 Intrusion injuries account for approximately 2% of traumatic dentoalveolar injuries in permanent teeth.Citation2 Intrusion injuries occur when a tooth is pushed axially into the tooth socket; thereby crushing the periodontal ligament and damaging the cementum, alveolar bone, and vasculature.Citation3–5 Intrusive injuries are classified based on the degree of clinical displacement as mild (<3 mm), moderate (3 mm-7 mm) and severe (>7 mm).Citation6,Citation7 Traumatic intrusion is considered one of the most severe dentoalveolar injuries and the prognosis for healing and tooth retainment decreases with increasing intrusion severity.Citation5,Citation8 Furthermore, intrusion injuries have the potential to cause permanent orofacial issues that last into adulthood.Citation6 Premature loss of an anterior tooth, particularly in young patients, can lead to malocclusion, negative parafunctional tongue habits, impair aesthetics and damage the self-esteem of the patient.Citation9 While intrusion injuries are severe and may have negative consequences, there is limited research detailing the management and treatment of these injuries, particularly in immature permanent teeth.
Literature states that intrusion injuries result in pulp necrosis in 45% of teeth with immature apices and 100% in cases of mature apices.Citation5,Citation10–12 For severely intruded teeth with immature apices, the risk of pulpal necrosis increases.Citation4,Citation5,Citation8 Currently, the literature suggests two major procedures for managing a non-vital immature permanent tooth with an open apex – apexification and revascularization. The first, and more well-known procedure is apexification. In apexification procedures, the end of a root is closed with an apical barrier such as ga collagen plug and then packed with mineral trioxide aggregate (MTA) or gutta percha to fill the canal space.Citation8,Citation9,Citation13 While this procedure usually results in successful removal of infected pulp, the tooth is much more susceptible to fracture due to the incomplete formation of the root and thin dentinal walls.Citation14
Another possible treatment option for non-vital immature permanent teeth is revascularization. In this procedure, the root canal is filled with calcium hydroxide or triple antibiotic paste and then bleeding is induced to promote revascularization of the pulp and continued root development.Citation9,Citation14–17 While this revascularization technique has been attempted for non-vital immature permanent teeth, minimal literature could be found documenting an attempt to revascularize a severely intruded immature permanent tooth in the five months following orthodontic extrusion. The purpose of this case report is to demonstrate how revascularization can be used to manage traumatized immature permanent teeth with pulp necrosis and external root resorption after five months of orthodontic repositioning.
Case Summary
Appointment 1: Initial Examination
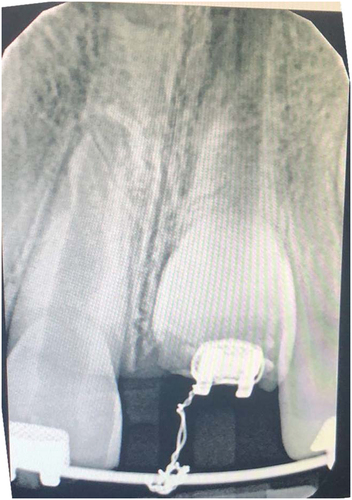
A 7-year-old African American female presented to Howard University Pediatric Dental Clinic for a limited oral exam regarding intrusion of tooth No. 9 (). The patient sustained the injury approximately two weeks prior to the first appointment at Howard University Pediatric Dental Clinic (). At the initial appointment, a limited oral exam was performed, and an intraoral photo () and occlusal radiograph () were obtained. The radiograph revealed a severely intruded maxillary left central incisor, tooth No. 9, uncomplicated enamel-dentin crown fracture at the incisal edge and widened PDL space surrounding the mesial and distal root aspects (). The patient did not present with any dental pain. The tooth was non-mobile and intruded approximately 10 mm with only 2 mm of the clinical crown showing. Any tooth intruded greater than 7 mm may undergo spontaneous extrusion, however re-eruption could take much longer than a few weeks.Citation6,Citation18 If spontaneous eruption does not occur within two to four weeks, the International Association of Dental Traumatology (IADT) Guidelines state that the tooth should be repositioned orthodontically or surgically.Citation6,Citation19
Figure 1. Intruded tooth No. 9 on the first day of initial injury. Photo taken by mother at time of incident.

Figure 2. Appointment 1 intraoral photo taken two weeks after initial injury.

Figure 3. Appointment 1 radiograph.

At this appointment, the tooth was not tested for pulp vitality due to the severity of the intrusion and literature stating that in 96% of cases, intrusions result in necrotic diagnosis.Citation5,Citation20 Additionally, pulp testing was delayed to avoid further exacerbating the anxiety of the child.Citation21 The child demonstrated FRANKL 3 behavior, characterized by reluctant acceptance of treatment displaying caution and apprehension.Citation22
A variety of multidisciplinary treatment options were discussed with the parents including the risks, benefits and alternatives for treatment. Periodontal exposure of the tooth followed by orthodontic repositioning and revascularization were selected as the best option by the provider and parent. The team agreed to proceed with revascularization with the understanding that the prognosis would be guarded for long-term survival. The benefits of revascularization include maintenance of short-term aesthetics, function and alveolar bone preservation for potential future implant placement if tooth failure occurs as the child continues growth and development.
Appointment 2: Consultations and Orthodontic Button Placement
At the second appointment, consults from an orthodontist and periodontist were obtained. The orthodontic team determined that the tooth could be orthodontically extruded with light continuous forces, thereby permitting endodontic access and preventing ankylosis.Citation23 Extrusion with light continuous forces helps maintain the PDL space, alveolar bone level and minimize replacement resorption, while excessive heavy forces increase the risk for PDL damage, ankylosis and root resorption.Citation23
A periodontist assessed the supporting structures surrounding the intruded tooth and performed vitality tests of tooth No. 9 and adjacent teeth. Pulp vitality testing was performed at this appointment in adherence to American Academy of Endodontics (AAE) recommendations stating that pulp testing should be completed at the next follow-up visit following a traumatic injury.Citation24 The pulp testing verified the non-vitality of tooth No. 9 with no response and confirmed that there were no concomitant pulpal injuries in the adjacent teeth as they all had normal responses.
A limited view CBCT scan was also obtained. The CBCT showed no signs of alveolar fracture or abnormal pathology. The CBCT scans were unavailable for visualization in this article due to compatibility difficulties when downloading the images.
The periodontal team determined that the main goal of this case was to maintain an adequate amount of bone and tissue long enough to create an esthetic periodontium in case animplant or prosthesis is needed in the future. The periodontist advised against surgically repositioning the tooth as a surgical flap may result in subsequent tooth loss and interfere with periodontal healing.Citation25 To decrease the risk for complications and increase the likelihood of maintaining periodontal stability long-term, the periodontist agreed to perform a gingivectomy on tooth No. 9 to facilitate orthodontic button placement necessary for orthodontic extrusion.
After the consults, the patient was taken to the pediatric clinic for tooth No. 9 gingivectomy (). The gingivectomy was completed to expose more tooth surface for orthodontic button placement. The region was anesthetized, approximately 2 mm of attached gingiva was excised with an external bevel incision on the facial surface of tooth No. 9. Only 2 mm of attached gingiva was excised so that an appropriate amount of tissue would be left to create an esthetic periodontium in the future if a definitive prosthesis such as an implant or bridge is warranted (). Hemostasis was achieved and an MBT bracket was placed on tooth No. 9 with composite (). Nitrous oxide inhalation sedation was used throughout the procedure and 100% oxygen was provided for five minutes after the procedure.
Figure 4. Appointment 2 after gingivectomy.

Figure 5. Appointment 2 orthodontic button placement.

At the end of the appointment, verbal and written postoperative instructions were given to the patient and parent. The patient was encouraged to continue an at home oral hygiene regimen including brushing twice per day using a fluoridated toothpaste, daily flossing and daily chlorhexidine gluconate 0.12% mouth rinse until gingival health improves.Citation6 The parent also understood that following the gingivectomy, orthodontic extrusion and endodontic revascularization, the tooth still has a questionable prognosis.Citation26–28
Appointment 3: Orthodontic Band and Wire Placement
Three days after the second appointment, the patient’s mother called to report that the patient was playing in the grocery store and bumped her mouth on the grocery cart handle. The patient was instructed to come into the clinic for an emergency appointment immediately, but mother reported that tooth No. 8 chipped and did not want to bring patient in for an exam as the next appointment was only three days away. The conversation was documented.
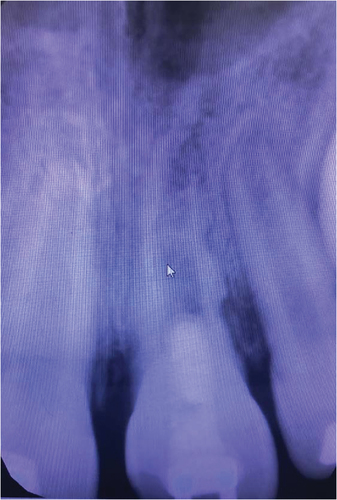
When the patient arrived at the clinic, another periapical radiograph of teeth Nos. 8 and 9 was taken (). Upon review of the periapical radiograph, a nutrient canal was observed, presenting as a jagged radiolucent line through the root of tooth No. 9. External root resorption of tooth Nos. 8 and 9 was also observed, as the roots of the teeth showed widened PDL spaces, open apices and ragged moth-eaten mesial and distal aspects of the roots. Vitality tests were performed on teeth Nos. 7–10. The pulpal response was normal in Nos. 7, 8 and 10, and no response was obtained from tooth No. 9.
Figure 6. Appointment 3 periapical radiograph showing uncomplicated fracture on teeth Nos. 8 and 9, external inflammatory root resorption, widened PDL spaces, open apices, ragged moth-eaten mesial and distal aspects of the roots. Tooth No. 9 bracket engaged to main arch wire with ligature tie.
The fracture on tooth No. 8 was fixed with a composite bandage. The surface was rinsed, glass ionomer liner placed (TheraCal, Bisco, San Jose, Calif.) and a thin layer of composite applied to seal the tooth. Orthodontic bands were placed on teeth Nos. 3 and 14, and brackets placed on teeth Nos. 7, 8 and 10. A 0.018 × 0.025 stainless steel main arch wire was engaged to the molar tubes and brackets on teeth Nos. 7, 8 and 10. With a separate ligature tie, the bracket was engaged on tooth No. 9 and tied to the main arch wire () to begin extrusion. The patient was given verbal and written oral hygiene instructions and dismissed with orthowax and chlorhexidine rinse. The patient returned to the orthodontist for biweekly visits for the next three months until the tooth was extruded enough to obtain lingual access to the tooth for revascularization ().
Figure 7. Orthodontic progress photo at three months since initial injury.
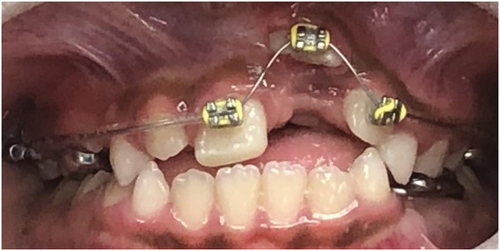
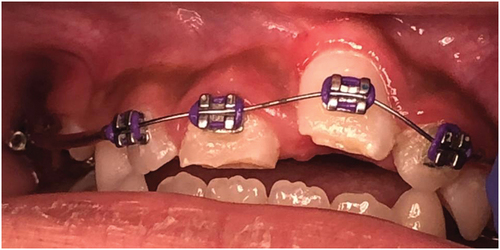
Figure 8. Orthodontic progress photo at four months since initial injury.
Appointment 4: First Revascularization Appointment
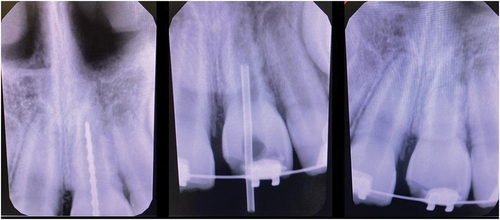
The revascularization technique was obtained from the AAE guidelines.Citation17 A preoperative radiograph was obtained and 36 mg of mepivacaine (Carbocaine, Cook-Waite, New York) was administered via local infiltration as any anesthetic with epinephrine may cause vasoconstriction and hinder bleeding.Citation17,Citation29 Initially, a rubber dam was placed in the usual manner, however the patient’s behavior did not allow continued use throughout the duration of treatment and an Isolite (Zyris, Santa Barbara, Calif.) was placed instead. The access opening was initiated from the lingual aspect of the tooth crown. The canal was identified. A barbed broach was used to remove remnants of necrotic pulp tissue; careful not to graze canal walls and avoid root apex. No bleeding was observed, as expected. The pulp chamber and canal were gently irrigated with 20 mL NaOCl (1% concentration) using apical negative pressure irrigation (EndoVac, Kerr Corp., Brea, Calif.) for five minutes. A working length radiograph was then obtained (, left). The canal was then irrigated with 20 mL of 17% ethylenediaminetetraacetic acid (EDTA) for five minutes and dried with paper points. EDTA is an “irrigant known to expose endogenous growth-factor proteins embedded in the dentinal walls.”Citation9 Calcium hydroxide (CaOH) was placed into the canal using a syringe (, middle). A periapical radiograph was obtained to confirm CaOH placement (, right). The canal orifice was then covered with a 3 mm layer of temporary filling material (Cavit, 3 M, St. Paul, Minn.) and temporized with a fluoride releasing alternative glass ionomer (GC Fuji IX GP, GC America, Alsip, Ill.).
Figure 9. Appointment 5 first revascularization visit. (left) working length (middle) CaOH insertion (right) postoperative.
At the start of the appointment, consent for treatment was obtained from the parent; including nitrous consent, procedural consent and oral sedation consent. Hydroxyzine and meperidine were the oral sedation medications used. The patient’s vital signs were confirmed at the end of the appointment, and the patient was then dismissed with no complications and parent given verbal and written postoperative instructions.
Appointment 5: Second Revascularization Appointment
No signs or symptoms of persistent infection were observed. According to AAE guidelines, if swelling, pain or other symptoms persist then consider allowing additional disinfection treatment time by repeating first appointment procedure using another antimicrobial or alternative antimicrobial.Citation17
A preoperative radiograph was obtained, and the patient was anesthetized with 36 mg of mepivacaine via maxillary local infiltration. An isolite was placed and the temporary restoration was removed. The canal was then gently irrigated with EDTA to remove the CaOH and dried with paper points (). Bleeding was induced into the canal up to the cementoenamel junction (CEJ) by passing a No. 40 K-file through the apex. A small piece of gel foam was placed over the blood clot and MTA cap placed to the level of the CEJ (). The tooth access was then restored with composite resin. Consent for treatment was obtained from the parent; including nitrous consent, procedural consent and oral sedation consent. After confirming pre-sedation vital signs, hydroxyzine and meperidine were administered based on the patient’s weight. At the end of the appointment, the patient’s vital signs were confirmed, and the patient was then dismissed with no complications. The parent was provided verbal and written postoperative instructions.
Figure 10. Appointment 5 irrigation with EDTA.
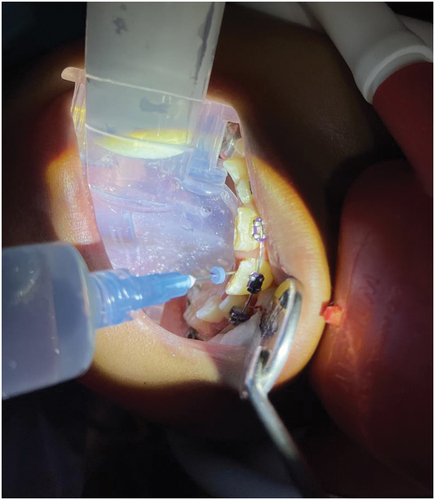
Figure 11. Appointment 5 postoperative PA with MTA cap and composite seal.
Over the next nine months following the second revascularization appointment, the patient attended monthly orthodontic visits to continue extruding the tooth and regain proper alignment of the tooth. The patient also returned for regular recall visits and was encouraged to continue an at home oral hygiene regimen including brushing twice per day using a fluoridated toothpaste, flossing and rinsing with chlorhexidine gluconate 0.12%.Citation6
Periapical radiographs were obtained over the next 14 months following the second revascularization appointment. At 14 months, clinical and radiographic examination showed cessation of the resorption process, the beginning of apical root closure and discontinuation of signs and symptoms (). Gingival inflammation was present due to the orthodontic appliance and poor oral hygiene (). The patient was placed on three month recalls for prophy and fluoride varnish application. In the future after orthodontic debonding, the patient will obtain a gingivectomy to adjust the gingival zenith of incisors, a final restoration and continue clinical and radiographic follow-up.
Figure 12. Periapical radiograph at 14 months postoperative showing cessation of the resorption process and apical root closure and root development.
Figure 13. Intraoral photo one year since initial injury. Gingival inflammation and uneven gingival zenith noted.

Discussion
Traumatic intrusion is considered one of the most severe dentoalveolar injuries. Intrusion injuries comprise only 0.5%-2% of all dental trauma injuries.Citation2,Citation30,Citation31 Severe intrusions make up a fraction of that percentage. Consequently, there is limited research detailing the management and treatment of severe intrusive injuries, particularly in immature permanent teeth.
Intrusion injuries have the poorest pulp vitality prognosis of all dentoalveolar injuries.Citation5,Citation10–12 Tooth survival is predominantly impacted by degree of intrusion. Tooth survival decreases with increasing severity of intrusion.Citation5 In a study analyzing the clinic outcomes of permanent incisor luxation, Humphrey and colleagues found that 90% to 100% of mild and moderate intrusions (<7 mm) survived for five years, while only 45% severe intrusions (>7 mm) survived in that same five years.Citation5 The majority of severely intruded incisors in this study experienced pulp necrosis in less than two years.Citation5
In addition to pulp necrosis, the poor tooth survival of severe intrusive injuries may also be due to injury related complications such as concomitant crown or root fracture, root resorption, marginal bone loss and/or ankylosis.Citation8,Citation20,Citation25,Citation32–35 The complications that were encountered in this case were pulp necrosis, uncomplicated crown fracture and external inflammatory root resorption.
In immature permanent teeth, pulp necrosis is the most common complication following an intrusion injury.Citation34 Pulp necrosis can occur in two ways; first, through severance of the pulp blood supply and secondly, through direct bacterial invasion of the dental pulp.Citation35,Citation36 In intrusion injuries, the pulp loses its source of nutrients and becomes necrotic when the tooth is pushed axially through the tooth socket crushing the periodontal ligament (PDL), alveolar bone and blood vessels.Citation35,Citation36
The rate for pulp necrosis increases when the intrusion is accompanied by an uncomplicated or complicated crown fracture.Citation8,Citation31,Citation36 In a normal functioning tooth, there is a continuous outward flow of dentinal fluid that flushes out sporadically migrating bacteria.Citation36,Citation37 However, when the pulp vascular supply is damaged as in severe intrusive injuries, there is no intrapulpal pressure to facilitate the outward flow of dentinal fluid that usually prohibits bacterial invasion.Citation36 With this cessation of dentinal fluid flow, microorganisms are able to enter the pulp through the exposed dentinal tubules from an uncomplicated crown fracture. Therefore, when an intrusion is accompanied by an uncomplicated fracture as in this case, bacteria is able to quickly infect the pulp resulting in a diagnosis of infected pulp necrosis.
Both the American Academy of Pediatric Dentistry (AAPD) and AAE recommend that a necrotic pulp in an immature permanent tooth be managed with endodontic revascularization.Citation17,Citation38 Revascularization procedures have two steps; first, the root canal is filled with a biocompatible disinfecting agent such as calcium hydroxide or triple antibiotic paste. After three to four weeks and no recurrent signs or symptoms of pain or swelling, bleeding is induced and MTA cap placed to create a scaffold to encourage generation of new tissue within the root canal.Citation9,Citation14–17,Citation39 This is based off the fact that even if a pulp has lost vitality, residual pulp stem cells and apical papilla stem cells can still survive.Citation39 While it is generally recommended that revascularization be initiated immediately to disinfect the root canal system; in this case, revascularization was delayed by five months to allow for slow orthodontic repositioning of the tooth with light continuous forces. Slow orthodontic repositioning with light continuous forces decreases replacement resorption and aids in maintenance of the periodontium.Citation40
While orthodontic repositioning may be beneficial in decreasing ankylosis, external inflammatory root resorption still may occur soon after a traumatic incident or at a later time due to the severity of the intrusion.Citation41 External inflammatory root resorption was observed at the third appointment, approximately one month after the initial intrusive injury. External inflammatory root resorption occurs when the root’s cemental barrier is broken and inflammatory stimulators from the necrotic pulp diffuse through the dentin tubules and stimulate an inflammatory response in the periodontal ligament that resorbs the tooth structure.Citation9,Citation41 The treatment goal for external root resorption in this case was to remove the inflammatory stimulators and destroy the bacteria that is present by initiating endodontic revascularization.
As previously stated, ideally the team would have preferred to initiate revascularization immediately, however the tooth was inaccessible for endodontic access due to the severity of the intrusion. While surgically repositioning the tooth may have permitted more immediate pulpal access, this technique was not performed due to the high rate of complications that can occur particularly in pediatric patients with immature permanent teeth. Potential complications include pulp necrosis, external root resorption, ankylosis, marginal bone loss, contamination, infection, root fractures and iatrogenic exarticulation.Citation20,Citation25,Citation42
Orthodontic extrusion of a severely intruded tooth is recommended, since it is believed to facilitate remodeling of the supporting tissues and provide early endodontic access.Citation20,Citation25,Citation43 Additionally, placement of bands and wires in orthodontics does not require the use of local anesthetic making orthodontic repositioning less frightening for pediatric patients afraid of needles.Citation44 Orthodontic treatment may also be a motivating factor for many young patients to continue with extensive dental treatment.Citation44–46 In congruence with this literature, the team opted to continue with orthodontic extrusion and commence with revascularization once the tooth became accessible for lingual access.
In revascularization as in all endodontic procedures, rubber dam placement is the standard of care. The original treatment plan for this case included moderate oral conscious sedation and dental dam isolation. However, the child did not tolerate the rubber dam as indicated by excessive movement, whining and noncompliance upon placement. After evaluating the patient’s cooperative potential through observation and interaction with the patient, the uncooperative behavior subsided after the removal of the rubber dam and an Isolite was used alternatively. This decision was made in adherence to the AAPD guideline, “Behavioral Guidance for the Pediatric Dental Patient,” stating that maladaptive changes in patient behavior may require alterations to the treatment plan.Citation47
The risks and benefits of immediate treatment with an Isolite versus deferred treatment until the patient can tolerate a rubber dam was deliberated. After careful consideration, the decision was made to continue treatment with the Isolite, which provides light, suction, retraction and prevention of aspiration similar to a rubber dam.Citation48 Additionally, endodontists have documented that Isolites can be useful in pediatric patients with incompletely erupted teeth.Citation48 Lastly, delaying treatment by waiting for the patient to mature enough to tolerate rubber dam placement prior to revascularization may increase the risk of further bacterial invasion and external inflammatory root resorption over time; whereas immediate revascularization treatment with the Isolite may decrease that risk.
In the second revascularization appointment, MTA was placed at the cervical portion of the root canal. The AAE recommends MTA as the best biomaterial for sealing the pulp space in regenerative endodontics.Citation17 MTA has high biocompatibility, aids in dentin bridge formation and forms a good barrier,Citation9 however it causes gray staining. Perhaps a white MTA or a bioactive dental substitute (Biodentine, Safco Dental Supply, Buffalo Grove, Ill.) would have been a better material choice esthetically, but literature states that gray MTA, white MTA and Biodentine all contribute to tooth discoloration in some degree.Citation49
The AAE also recommends the use of glass ionomer cement for the cervical seal where aesthetics are a concern, however there is limited evidence demonstrating its success.Citation17,Citation49 MTA was properly used in this case to seal the tooth by creating a pulp space barrier. In the future upon apical closure and continued root development, the MTA can be removed and root canal treatment performed to regain tooth color.
Since 2018, the AAE has recommended the use of triple and double antibiotic pastes in low concentrations and calcium hydroxide to disinfect the root canal system during revascularization.Citation17,Citation50 Some antibiotic combination examples include: ciprofloxacin, metronidazole and minocycline or cefaclor, metronidazole and ciprofloxacin.Citation50
According to Althumairy and colleagues, high concentrations of triple antibiotic paste may hinder the survival of stem cells of the apical papilla, whereas calcium hydroxide promotes the survival and proliferation of these cells.Citation50,Citation51 The study also revealed that toxicity to stem cells is a concentration-dependent effect that can be avoided when the concentration of the paste is one mg per mL or less.Citation50,Citation51 Additionally, previous studies demonstrated that when minocycline, doxycycline, amoxicillin or cefaclor was used in the paste, clinically visible tooth discoloration was observed.Citation50
While multiple sources stated that calcium hydroxide and triple antibiotic pastes are equally effective in disinfecting the root canal system, calcium hydroxide was used in this case due to increased accessibility and decreased risk of concentration toxicity as can occur when using triple antibiotic paste. After the first revascularization appointment, the root resorption radiographically subsided, which demonstrates the effectiveness of calcium hydroxide in complete removal of the inflammatory stimulators in the tooth.
This case demonstrates that severe intrusive injuries in immature permanent teeth can be effectively managed with revascularization even when initiation of revascularization must be delayed due to extended time needed for orthodontic repositioning. After one year follow-up, all signs and symptoms have been discontinued and radiographs indicate cessation of the resorptive process. The parents and patient have been informed that the prognosis of long-term tooth retainment is still guarded, however, revascularization achieved the primary goal of retaining alveolar bone, maintaining dental function, preserving aesthetics and maintaining an adequate periodontium in case a future implant or prosthesis is needed in the future. Clinical and radiographic exams will be obtained at yearly intervals to determine if and when subsequent intervention is necessary. The hope is that this tooth continues to grow with the dentoalveolar complex, averts ankylosis and regains pulpal vitality.
Conclusion
This case is significant due to the rare occurrence of this injury particularly within the pediatric population, the severity of the intrusive injury, and the increased time delay between injury and endodontic revascularization therapy. Traumatic intrusion is a severe dentoalveolar injury and the prognosis for healing and tooth retainment decreases with increasing intrusion severity. However, this case shows that severe intrusive injuries in immature permanent teeth can be effectively managed with revascularization even when initiation of revascularization must be delayed due to extended time needed for orthodontic repositioning. Revascularization achieved the primary goal of retaining alveolar bone, maintaining dental function, preserving aesthetics and maintaining an adequate periodontium in case a future implant or prosthesis is needed in the future.
Supplemental Material
Download MS Word (31.9 KB)Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2176580
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Ariel Snell
Ariel Snell, DMD, MPH is a pediatric dental resident at Howard University College of Dentistry in Washington, D.C.
Jonathan Bacon
Jonathan Bacon, DDS, is an assistant clinical professor in the department of pediatric dentistry at Howard University College of Dentistry in Washington, D.C. He is a diplomate of the American Board of Pediatric Dentistry and the American Dental Board of Anesthesiology.
Crystal McIntosh
Crystal McIntosh, DDS, MS, is the director of the division of periodontics at Howard University College of Dentistry in Washington, D.C. She is a diplomate of the American Board of Periodontology.
Paula Nesbitt
Paula Nesbitt, DDS, MSD, is a director and assistant professor in the department of endodontics at Howard University College of Dentistry in Washington, D.C.
References
- Colak I, Markovic D, Petrovic B, Peric T, Milenkovic A. A retrospective study of intrusive injuries in primary dentition. Dent Traumatol. 2009;25(6):605–9. doi:10.1111/j.1600-9657.2009.00838.x. Accessed November 17, 2021.
- Andreasen JO, Bakland LK, Matras RC, Andreasen FM. Traumatic intrusion of permanent teeth. part 1. an epidemiological study of 216 intruded permanent teeth. Dent Traumatol. 2006;22(2):83–89. doi:10.1111/j.1600-9657.2006.00421.x. Accessed November 17, 2021.
- Wigen TI, Agnalt R, Jacobsen I. Intrusive luxation of permanent incisors in Norwegians aged 6-17 years: a retrospective study of treatment and outcome. Dent Traumatol. 2008;24(6):612–618. doi:10.1111/j.1600-9657.2008.00686.x. Accessed November 17, 2021.
- Council on Clinical Affairs. Guideline on management of acute dental trauma. AAPD Reference Manual. 2010;32(6): 202–212.
- Humphrey JM, Kenny DJ, Barrett EJ. Clinical outcomes for permanent incisor luxations in a pediatric population. I. intrusions. Dent Traumatol. 2003;19(5):266–273. doi:10.1034/j.1600-9657.2003.00207.x. Accessed April 6, 2022.
- Bourguignon C, Cohenca N, Lauridsen E, et al. International association of dental traumatology guidelines for the management of traumatic dental injuries: 1. fractures and luxations. Dent Traumatol. 2020;36(4):314–330. doi:10.1111/edt.12578. Accessed April 6, 2022.
- Diangelis AJ, Andreasen JO, Ebeleseder KA, et al. International association of dental traumatology guidelines for the management of traumatic dental injuries: 1. fractures and luxations of permanent teeth. Dent Traumatol. 2012;28(1):2–12. doi:10.1111/j.1600-9657.2011.01103.x. Accessed November 17, 2021.
- McDonald RE, Avery DR, Dean JA, Jones JE. Management of trauma to the teeth and supporting tissues. In: Dean J, Avery D McDonald R, eds. McDonald and Avery Dentistry for the Child and Adolescent. 9th ed. Saint Louis: Mosby; 2011: 403–442.
- Hargreaves KM, Cohen S, Berman LH. Pathways of the Pulp. 10th ed. St Louis: Mosby; 2011.
- Soares DA, Tulio MA, Westphalen FH, et al. Management of multiple dental trauma: case report with eight-year follow-up. Iran Endod J. 2018; 13(3):410–412. doi:10.22037/iej.v13i3.21090. Accessed November 17, 2021.
- Lima TFR, Silva EJNLD, Gomes BPFDA, Almeida JFAD, Zaia AA, Soares AJ. Relationship between initial attendance after dental trauma and development of external inflammatory root resorption. Braz Dent J. 2017;28(2):201–205. doi:10.1590/0103-6440201701299. Accessed November 17, 2021.
- Tzanetakis GN. Management of intruded immature maxillary central incisor with pulp necrosis and severe external resorption by regenerative approach. J Endod. 2018;44(2):245–249. doi:10.1016/j.joen.2017.11.006. Accessed November 17, 2021.
- AAPD. Pulp therapy for primary and immature permanent teeth. AAPD Reference Manual. 2014;38:353–361.
- Mittmann C, Kostka E, Ballout H, et al. Outcome of revascularization therapy in traumatized immature incisors. BMC Oral Health. 2020;20(1). doi:10.1186/s12903-020-01193-5. Accessed November 17, 2021.
- Yoshpe M, Einy S, Ruparel N, Lin S, Kaufman AY. Regenerative endodontics: a potential solution for external root resorption (case series). J Endod. 2020;46(2):192–199. doi:10.1016/j.joen.2019.10.023. Accessed November 17, 2021.
- Tong HJ, Rajan S, Bhujel N, Kang J, Duggal M, Nazzal H. Regenerative endodontic therapy in the management of nonvital immature permanent teeth: a systematic review-outcome evaluation and meta-analysis. J Endod. 2017;43(9):1453–1464. doi:10.1016/j.joen.2017.04.018. Accessed November 17, 2021.
- American Association of Endodontists. AAE Clinical Considerations for a Regenerative Procedure. 2018.
- Omar S, Freccia WF, Retamozo B, Bakland LK. Traumatically intruded permanent teeth: three case reports and a review of current recommendations. J Calif Dent Assoc. 2017;45(5):235–243. Accessed August 23, 2022.
- AlKhalifa JD, AlAzemi AA. Intrusive luxation of permanent teeth: a systematic review of factors important for treatment decision-making. Dent Traumatol. 2014;30(3):169–175. doi:10.1111/edt.12104. Accessed August 30, 2022.
- Andreasen J, Andreasen F, Andersson L. Textbook and color atlas of traumatic injuries to the teeth; 1994. doi:10.1016/0278-2391(95)90312-7. Accessed November 17, 2021.
- O’connell AC, Spadinger A. Trauma and sports dentistry. In: Nowak A Casamassimo P, eds. The Handbook of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2018: 177–190.
- Wells M, Townsend JA. Managing pain and behavior guidance. In: Nowak A Casamassimo P, eds. The Handbook of Pediatric Dentistry. Chicago: American Academy of Pediatric Dentistry; 2018: 242–264.
- Bach N, Baylard J, Voyer R. Orthodontic extrusion: periodontal considerations and applications. J Can Dent Assoc. 2004;70(11):775–780. Accessed April 19, 2022.
- Sigurdsson A. Treatment of traumatic dental injuries. Am Assoc Endodontists . 2014;2014:8.
- Sapir S, Mamber E, Slutzky-Goldberg I, Fuks AB. A novel multidisciplinary approach for the treatment of an intruded immature permanent incisor. Pediatr Dent. 2004;26(5):421–425. Accessed April 20, 2022.
- Kwok V, Caton JG. Commentary: prognosis revisited: a system for assigning periodontal prognosis. J Periodontoll. 2007;78(11):2063–2071. doi:10.1902/jop.2007.070210. Accessed April 20, 2022.
- Nguyen L, Krish G, Alsaleh A, et al. Analyzing the predictability of the Kwok and Caton periodontal prognosis system: a retrospective study. J Periodontol. 2021;92(5):662–669. doi:10.1002/JPER.20-0411. Accessed April 20, 2022.
- McGuire MK, Nunn ME. Prognosis versus actual outcome. III. the effectiveness of clinical parameters in accurately predicting tooth survival. J Periodontol. 1996;67(7):666–674. doi:10.1902/jop.1996.67.7.666. Accessed April 20, 2022.
- Nuni E. Pulp therapy for the young permanent dentition. In: Fuks A Peretz B, eds. Pediatric Endodontics: Current Concepts in Pulp Therapy for Primary and Young Permanent Teeth. Switzerland: Springer International Publishing; 2016: 117–148.
- Andreasen JO, Ravn JJ. Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg. 1972;1(5):235–239. doi:10.1016/s0300-9785(72)80042-5. Accessed November 17, 2021.
- Andreasen JO, Bakland LK, Andreasen FM. Traumatic intrusion of permanent teeth. part 2. A clinical study of the effect of preinjury and injury factors, such as sex, age, stage of root development, tooth location and extent of injury including number of intruded teeth on 140 intruded permanent teeth. Dent Traumatol. 2006;22(2):90–98. doi:10.1111/j.1600-9657.2006.00422.x. Accessed November 17, 2021.
- Al-Badri S, Kinirons M, Cole B, Welbury R. Factors affecting resorption in traumatically intruded permanent incisors in children. Dent Traumatol. 2002;18(2):73–76. doi:10.1034/j.1600-9657.2002.180205.x. Accessed April 5, 2022.
- Albadri S, Zaitoun H, Kinirons MJ. UK national clinical guidelines in paediatric dentistry: treatment of traumatically intruded permanent incisor teeth in children. Int J Paediatr Dent. 2010;20(s1):1–2. doi:10.1111/j.1365-263X.2010.01085.x. Accessed April 6, 2022.
- Andreasen FM, Pedersen BV. Prognosis of luxated permanent teeth — the development of pulp necrosis. Endod Dent Traumatol. 1985;1(6):207–220. doi:10.1111/j.1600-9657.1985.tb00583.x. Accessed April 5, 2022.
- Yu CY, Abbott PV. Responses of the pulp, periradicular and soft tissues following trauma to the permanent teeth. Aust Dent J. 2016;61(S1):39–58. doi:10.1111/adj.12397. Accessed April 6, 2022.
- Krastl G, Weiger R, Filippi A, et al. Endodontic management of traumatized permanent teeth: a comprehensive review. Int Endod J. 2021;54(8):1221–1245. doi:10.1111/iej.13508. Accessed August 30, 2022.
- Galler KM, Weber M, Korkmaz Y, Widbiller M, Feuerer M. Inflammatory response mechanisms of the Dentine–Pulp complex and the periapical tissues. Int J Mol Sci. 2021;22(3):1480. doi:10.3390/ijms22031480. Accessed April 20, 2022.
- AAPD. Pulp therapy for primary and immature permanent teeth. Pediatr Dent. 2020;2022-23:415–423.Accessed December 5, 2021.
- Namour M, Theys S. Pulp revascularization of immature permanent Teeth: a review of the literature and a proposal of a new clinical protocol. Sci World J. 2014;2014:1–9. doi:10.1155/2014/737503. Accessed April 6, 2022.
- Medeiros RB, Mucha JN. Immediate vs late orthodontic extrusion of traumatically intruded teeth. Dent Traumatol. 2009;25(4):380–385. doi:10.1111/j.1600-9657.2009.00771.x. Accessed April 13, 2022.
- Abbott PV. Prevention and management of external inflammatory resorption following trauma to teeth. Aust Dent J. 2016;61(S1):82–94. doi:10.1111/adj.12400. Accessed April 13, 2022.
- Oulis C, Vadiakas G, Siskos G. Management of intrusive luxation injuries. Endod Dent Traumatol. 1996;12(3):113–119. doi:10.1111/j.1600-9657.1996.tb00108.x. Accessed April 21, 2022.
- Becker A. Maxillary Central Incisors. In: The Orthodontic Treatment of Impacted Teeth. London:Martin Dunitz;1998 53–83. Accessed April 21, 2022.
- Fields HW, Christensen JR. Orthodontic procedures after trauma. Pediatr Dent. 2013;35(2):175–183. Accessed November 17, 2021.
- Sheats RD, Gilbert GH, Wheeler TT, King GJ. Pilot study comparing parents’ and third-grade schoolchildren’s attitudes toward braces and perceived need for braces. Community Dent Oral Epidemiol. 1995;23(1):36–43. doi:10.1111/j.1600-0528.1995.tb00195.x. Accessed April 21, 2022.
- Ernest MA, da Costa OO, Adegbite K, Yemitan T, Adeniran A. Orthodontic treatment motivation and cooperation: a cross-sectional analysis of adolescent patients’ and parents’ responses. J Orthod Sci. 2019;8(1):12. doi:10.4103/jos.JOS_36_17. Accessed April 21, 2022.
- AAPD. Behavior guidance for the pediatric dental patient. Reference Manual Pediatr Dent. 2020;2022-23:321–339.
- Wahl P, Andrews T. Isolation: a look at the differences and benefits of rubber dam and isolite. Endo Practice. 2010;3:52–55. Accessed August 30, 2022.
- Santos LGPD, Chisini LA, Springmann CG, et al. Alternative to avoid tooth discoloration after regenerative endodontic procedure: a systematic review. Braz Dent J. 2018;29(5):409–418. doi:10.1590/0103-6440201802132. Accessed July 14, 2022.
- Do Couto AM, Espaladori MC, Leite APP, Martins CC, de Aguiar MCF, Abreu LG. A systematic review of pulp revascularization using a triple antibiotic paste. Pediatr Dent. 2019;41(5):341–353. Accessed April 21, 2022.
- Althumairy RI, Teixeira FB, Diogenes A. Effect of dentin conditioning with intracanal medicaments on survival of stem cells of apical papilla. J Endod. 2014;40(4):521–525. doi:10.1016/j.joen.2013.11.008. Accessed July 14, 2022.