

ABSTRACT
Many patients and guardians prefer not to have teeth extracted as part of orthodontic treatment. Modified C-Palatal Plates (MCPPs) have been developed as an effective oral appliance. The design and procedure for placing these appliances involve a sequence of steps and specialized instruments such as a miniscrew driver. By understanding the biomechanics associated with MCPP placement, molar positioning can be optimized with less distal tipping and greater distalization. In addition to recognizing the various advantages of MCPPs, the implications of MCPPs should be considered, including the following: how far back the molars need to be moved, the effects of second and third molars in adolescents, the effects in maxillary pneumatization cases, potential impact on the airway, long-term stability, and a comparison of MCPPs to headgear. The purpose of this report is to introduce MCPP as an oral appliance that uses both miniscrews and miniplates to efficiently distalize molars minimizing the need for extraction.
Introduction
To extract or not extract? That is the question. This question has been debated since the beginning of the orthodontic specialty.Citation1 Extraction has been the conventional modality for treating patients with major dental crowding or protrusion. Specifically, in cases where the arch length discrepancy is 10 mm or greater, extraction is almost always required.Citation1 Typically, the four first premolars are extracted in such cases.
Extraction cases have mixed results. Sometimes the dentition is more stable, the tissue is healthier, the facial esthetics are improved, and there is little-to-no impact on the masticatory function, but other cases have highlighted the disadvantages of extracting teeth for orthodontic treatment. Not only does the patient lose healthy, vital teeth, but their facial esthetics may be compromised. Also, after extraction of premolars, there is the potential for relapse. Studies have shown that in as little as one year after treatment, the closed extraction space reopens.Citation2,Citation3
Having discussed some of the major concerns associated with orthodontic extraction therapy, contemporary voices have recently begun advocating for a non-extraction approach, including the use of miniscrews as temporary skeletal anchorage devices (TSADs). Miniscrews provide the convenience of placement and ease of removal, and are affordable; however, despite favorable advantages, TSADs have potential complications. For example, root damage might occur if the miniscrew is not removed in a timely manner. Depending on the proximity of the root damage to the pulp, it may be irreversible. Another noted risk with miniscrews is the possibility of them being ingested if they loosen as bone remodels with tooth movement.
However, when TSADs are placed in a non-tooth-bearing area of the palate where the bone quality is superior, the risk of damage to dental roots and the potential for interference with tooth movement during treatment are reduced.Citation4
Kook et al. introduced the Modified C-Palatal Plate (MCPP) as an oral appliance that uses both miniscrews and miniplates to efficiently distalize molars, minimizing the need for extraction.Citation4 MCPP simplifies the placement procedure without incision, reduces patient discomfort, and increases the efficiency of tooth movement. MCPPs are highly effective in distalization of the maxillary dentition in adolescent patients as well as in adults.
The purpose of this report is to introduce MCPPs as an oral appliance and to consider their placement, biomechanics, range of molar distalization, role in the development of second and third molar effects, effects in cases of maxillary pneumatization, impacts on the airway, their long-term stability, and to compare MCPPs to headgear.
Appliance Design
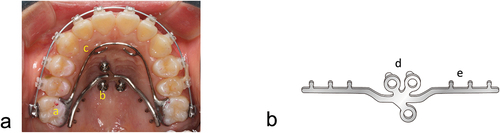
The MCPP as an appliance has two main components (). There is a palatal plate and a palatal retraction arch (PRA). The PRA is bonded to the first molars and is connected to the extended arms of the MCPP. MCPPs have three holes for three miniscrews to secure the device to the palatal area. Each screw is placed 2 mm from the midpalatal suture.Citation4 The screw holes have tubes that create even spacing to minimize soft tissue inflammation ().Citation5 Two arms with notches extend from the area of the three screws (). The notches serve to hook the closed coiled springs or power chains to the rest of the device.
Figure 1. A palatal skeletal anchorage appliance.
MCPP Placement
First, place the 3D jig-plate assembly on the palate (). The fabricated jig functions as a stent to precisely determine the location of the plate’s lever arms. With recent advancements in 3D technology, the PRA can be printed after using CAD/CAM scanning.Citation6 Ensure that the jig fits the occlusal surfaces of the molars and premolars. Next, insert self-drilling miniscrews through the screw tubes. The screws, 10 mm in length and 2.0 mm in diameter, are secured to the plate. Be sure not to blanch the palate to minimize the risk of applying excessive pressure. Then, use a torque driver at 30 rpm and apply force no greater than 30 Ncm.Citation5 Following the screw insertion, remove the jig by pulling with a gentle yet firm grasp from each side using utility pliers. Adjust as necessary by tightening the miniscrews and making fine adjustments to the lever arms.
Figure 2. MCPP and PRA placement.
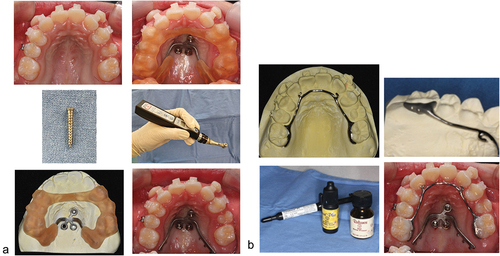
PRA Placement
Once the plate has been installed in the patient, etch the palatal surfaces of the first molars (). Using light cure adhesive paste, bond the bands of the wire to the lingual of the first molars. After both components of the appliance are positioned, connect the elastomeric chains or closed coil springs bilaterally from the notches on the plate arms to the anterior hooks on the PRA. Power chain elastics or open coil springs can be applied after the MCPP and PRA have been placed, allowing distalization to begin immediately.Citation4
MCPP Biomechanics
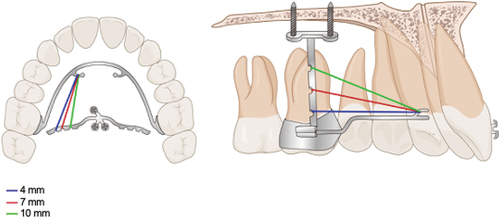
Once the MCPP has been placed as anchorage, the maxillary dentition can be moved. Anchorage on the palate is more stable than anchorage commonly placed on the buccal side as it allows for greater root control, increased distalization, intrusion, less distal tipping of the first molar, and avoids any involvement with tooth roots.Citation7 To modulate the amount of tipping and intrusion, the proper notch on the MCPP must be selected to connect the elastomeric chain or closed spring coil. Using the most apical notch on the MCPP arms, the force vector will align more closely with the center of resistance of the first molar and will result in less distal tipping, greater distalization, and greater intrusion of the molar.Citation8 The 10 mm notch will produce less tipping but more intrusion of the molar than the 4 mm notch. For total arch distalization, MCPPs require approximately 300 grams of force from each side, which can be accomplished with elastomeric chains.Citation8,Citation9 The duration of usage depends on the amount of distalization needed. For instance, the duration of usage differs between a patient with anterior open bite and a patient with full-step Class II occlusion.Citation10,Citation11 Moreover, the direction of the force movement can be regulated by adjusting the length and height of the (PRA).Citation8 The range of action is increased by the curved rather than straight arms of the MCPP, optimizing the force needed to distalize the teeth ().
Figure 3. Notches in the MCPP lever arm.
Pros and Cons of MCPP
There are various advantages to MCPP appliances compared to other traditional fixtures. When comparing them with conventional anchorage appliances such as cervical pull headgear, MCPPs offer a more effective way to distalize molars without patient cooperation.Citation12 A study emphasizing the dental forces for tooth movement showed that for adult patients with Class II malocclusion, the distalization of the first molars in relation to the vertical reference line was 3.06 mm with MCPPs, while the distalization of molars with cervical pull headgear was just 1.79 mm.Citation12 Other studies have shown MCPPs to be an equally and effective treatment modality as premolar extraction for Class II malocclusion with severe overjet. The results were essentially the same regardless of the treatment modality. There were no reported differences in treatment duration, skeletal change, nor soft tissue changes between the non-extraction treatment with MCPPs and the maxillary first molar extraction groups.Citation13
The main disadvantage of MCPP appliances is palatal soft tissue inflammation, especially in patients with poor oral hygiene.
Case Selection
MCPPs can be used to treat cases ranging from patients with conventional malocclusions such as Class II,Citation14,Citation15 or Class IIICitation16,Citation17 to bimaxillary protrusion.Citation18 The successful treatment with MCPPs has also been documented in cases of severe arch length discrepancy,Citation19 transposed canines and first premolars,Citation20 and patients with severe crowdingCitation21 and severe overjet.Citation15 The following factors may affect the success of treatment. A wide and shallow palatal vault anatomy is favorable over one that is narrow and deep due to facilitated hygiene thereby minimizing potential for inflammation. While the angulation of the first molar roots do not affect success rate, short roots especially of the first molar, however, prevent distalization of dentition with the MCPP. When considering the developing position of the maxillary third molar tooth germ, abnormal positions such as mesially or palatally tilted tooth germs may alter the success of treatment.
Case Report
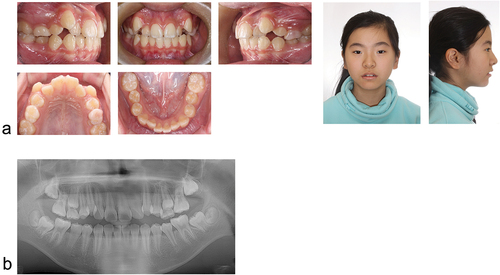
An 11-year-old female with late mixed dentition presented with the chief complaint of protruding maxillary canine teeth (). She presented with Class I molar relationship and Class II canine relationship on both sides. Her upper teeth showed severe crowding, while her lower teeth showed mild crowding with a few rotated teeth. Her second molars had not yet erupted, and no third molars were present in the maxilla. The patient had a symmetrical face with a relatively straight, slightly convex facial profile and mesofacial type. Her lips were in repose, and none of her midlines were shifted. The patient denied any oral habits or TMJ-specific contributions to her overall oral health status. Her upper arch length discrepancy was approximately 10 mm, and her lower arch had mild crowding (). To resolve the crowding while maintaining a good facial profile, the treatment plan involved total arch distalization using a MCPP.
Figure 4. Initial intraoral and facial photographs (a), panoramic radiograph (b).
For the first phase of treatment, brackets were placed just on the upper dentition (). Brackets with 0.022-inch slots were bonded to the maxillary primary second molar. A 0.009-inch stainless steel wire was used to ligate the maxillary first molar to the maxillary first premolar with a figure eight formation. This was done to preemptively prevent the formation of space between the first molar and the primary second molar after molar distalization. For this phase, a .016 NiTi was used as the initial wire, followed by a .018 NiTi wire.
Figure 5. Treatment Progress: after insertion of MCPP and PRA appliance (a), 10 months into treatment (b).

In the second phase of treatment, an MCPP and PRA were placed to distalize the molars and make room for the canines. Approximately three months into treatment, the canines were brought down into the arch (). Ten months into treatment, brackets were added to the mandibular teeth, and two buttons were added to the lingual surface of the lower right premolars to rotate them into proper alignment (). During the process of maxillary molar distalization, the molars were intruded, and incisors were extruded. This resulted in the disocclusion of the posterior teeth. To address this, first, elastomeric chains were applied from the screws to the hook between the lateral incisor and the canine using a 0.019 × 0.025″ SS wire (300 g per side) to perform total arch distalization. In order to correct the disocclusion of the maxillary posterior teeth, a box elastic was applied on both sides with 1/4-inch, 4.5 oz size elastics between the maxillary and mandibular first and second molars.
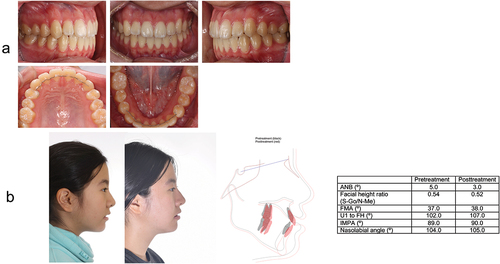
After 22 months of treatment, the protruding canines were brought down, and the crowding in both maxillary and mandibular dentitions was resolved. Most importantly, after debonding, the patient’s facial profile was maintained and lip competency was improved clinically (). Five years after removal, post-treatment records and cephalometric analysis comparison showed stable occlusion (). Class I molar and canine relationships, normal overjet, and overbite were achieved and maintained.
Figure 6. Debonding: Intraoral and facial photographs (a), panoramic radiograph and lateral cephalogram (b).
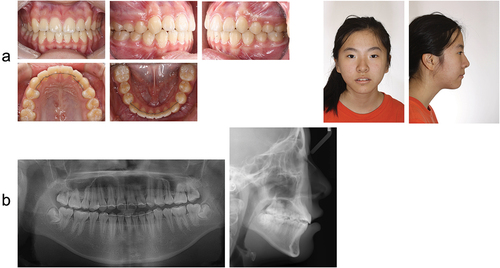
Figure 7. Retention: Intraoral and facial photographs, comparison of pre-treatment and 5 year retention with lateral cephalometric superimposition and measurements (a and b).
Discussion
Amount of Molar Distalization
In a study comparing the first molar positions after MCPP treatment and maxillary first premolar extraction treatment, none of the variables except for the position of the first molars were significantly different.Citation13 The skeletal variables, position of central incisors, and soft tissue variables did not differ significantly between the two groups. However, regarding the first molar positions, the first molars moved 5.4 mm distally with MCPP treatment while they shifted only by 1.2 mm mesially in extraction cases.Citation13 In another study looking at molar distalization for cases of severe arch length discrepancies, the lateral cephalometric analysis demonstrated that molar distalization using MCPPs allowed for the treatment of cases with arch length discrepancies of 10 mm or more. The molars were distalized by 4.2 mm in the maxilla and 1.9 mm in the mandible.Citation19
Second and Third Molar Positions After Total Arch Distalization
Another issue regarding the MCPP oral appliance is the effects of unerupted second and third molars. Distalization is difficult when second and third molars have not yet erupted because of potential third molar impaction, insufficient space for third molars, and delayed treatment timing. However, in a study comparing the long-term evaluation treatment effects of molar distalization in two groups with and without second molar eruption, Park et al. reported less tipping movement of the first and second molars as well as less distal tipping of the third molars in the group with second molar eruption.Citation22 Using cone-beam computed tomography (CBCT) to analyze the three-dimensional position of molars in the long term, the study demonstrated that both second and third molars showed favorable positions even after molar distalization. From a treatment timing standpoint, the study’s findings suggest that adolescents do not need to have their developing third molars extracted prior to distalization when MCPPs are used.
Pneumatization
Clinicians pose yet another concern regarding the potential complications of molar distalization in patients with maxillary sinus pneumatization. In some cases where the maxillary sinus is pneumatized into the posterior alveolar ridge, maxillary molar roots protrude into the sinus. Although this is not very common, if molars were to be distalized in such cases, not only would distalization be difficult due to the thick cortical bone below the sinus, but root resorption and tipping would be likely, and treatment times would be extended.Citation23 When comparing groups of patients with and without sinus pneumatization, there were no differences in skeletal and dental variables except for the overjet and nasolabial angle. Despite such concerns, Kim et al. demonstrated that even in cases with sinus pneumatization, molar distalization with MCPP could be performed.Citation23 The findings imply that there are no treatment timing differences for achieving molar distalization in patients that present with maxillary sinus pneumatization.
Airway
Clinicians and patients alike are interested in the impacts of MCPP treatment for total arch distalization of the maxillary dentition on the patient’s airway. Park et al. used CBCT analysis to determine that there were no changes in airway volume or cross-section of the oropharynx after total arch distalization with MCPP treatment.Citation24 It is expected that increased incisor retraction resulted in decreased tongue space, thereby decreasing airway volume in the group of patients that underwent extraction treatment. Unlike the non-extraction group of patients, the extraction group showed that the amount of distalization was inversely related to the amount of airway volume. A long-term study using CBCT further demonstrated that there were no significant airway space changes after distalization as well as in the post-retention period.Citation25
Stability
Clinicians wonder about stability after treatment with MCPP because post-treatment stability has significant implications for function and esthetics. Just as with any other treatment modality, there is always the possibility of relapse when using MCPPs. However, in the absence of major skeletal discrepancies or abnormalities, Shoaib et al. demonstrated minimal changes in the dental, skeletal, and soft tissue treatment effects three years post-treatment with MCPP.Citation26 Relapse in the maxillary first molars was only 12% of the achieved distalization and 35% of the intrusion. About 88% of the distal movement from MCPP treatment during the three years of observation was maintained. One explanation for the post-treatment stability is the distalization time.Citation26 MCPPs should therefore be considered a viable treatment option for maxillary total arch distalization with minimal loss in treatment effects.
Comparison with Headgear
In a study comparing the skeletal effects of the MCPP versus headgear appliances in adolescent patients, Sa’aed et al. showed that MCPPs resulted in a significant skeletal effect on the maxilla. Although headgear is known to affect treatment with regard to dental movement rather than skeletal movement, patients treated with headgear showed no major differences compared to patients treated with MCPP.Citation27 The MCPPs resulted in distalization of maxillary first molars with minimal distal tipping of molars, but such results did not differ from those who underwent headgear treatment. Given that the results of maxillary first molars distalization from both groups of patients with MCPP and headgear are comparable, other factors such as patient cooperation and appliance comfort should be considered. The headgear appliance is not only bulky but also depends heavily on the patient for treatment effects. The study implies that clinicians should consider the application of MCPP, especially for noncompliant patients with Class II malocclusion.
Conclusions
MCPPs are a beneficial oral appliance with numerous advantages, especially when patients reject extraction. It is an easy-to-apply device that does not interfere with growth and developing teeth while providing the convenience of chairside insertion. With MCPPs, the post-treatment outcomes of facial and dental esthetics, post-treatment stability, and functionality attest to the efficiency and effectivity of the oral appliance.
Additional information
Notes on contributors
Jae Hyun Park
Jae Hyun Park is the professor and chair of the Postgraduate Orthodontic Program at the Arizona School of Dentistry & Oral Health. He is a diplomate of the American Board of Orthodontics (ABO), where he serves as an examiner and director of their Board, representing the Pacific Coast Society of Orthodontists (PCSO). He will be the ABO president in 2024. Dr. Park has received several awards for scientific and clinical excellence, including the Charley Schultz Award (1st Place in the Scientific Category of the Orthodontic Resident Scholars Program) and the Joseph E. Johnson Award (1st Place in the Table Clinic Competition) from the American Association of Orthodontists (AAO). He also serves as an editorial board member of several international, peer-reviewed orthodontic and dental journals, including The Angle Orthodontist and Seminars in Orthodontics. He is also associate editor of the American Journal of Orthodontics and Dentofacial Orthopedics (AJO-DO), Orthodontics & Craniofacial Research, Korean Journal of Orthodontics, Journal of World Federation of Orthodontists, Journal of Clinical Pediatric Dentistry, and Journal of Esthetic and Restorative Dentistry. He was recently appointed deputy editor of the AJO-DO and the new clinical journal, AJO-DO Clinical Companion. Since 2008, while working as a full-time faculty member, he has published more than 340 scientific and clinical articles in peer-reviewed orthodontic and dental journals, including six cover pages in the AJO-DO, three books, and 23 book chapters. One of his Case of the Month articles in the AJO-DO was recently selected to receive the 2021 College of Diplomates of the American Board of Orthodontics (CDABO) Case Report of the Year Award during the AAO Annual Session. He lectures nationally and internationally and represented the AAO at the 2018 ADA Annual Session, where he presented a three-hour lecture. Dr. Park is editor-in-chief emeritus of the Journal of the PCSO (PCSO Bulletin) and past president of the Arizona State Orthodontic Association. Recently, he received the 2021 Award of Merit from the PCSO and will receive the 2023 AAOF Louise Ada Jarabak Memorial International Teachers and Research Award at the next AAO annual session. He also serves on the INBDE Ortho-Pediatric Dentistry/ADAT Test Construction Committee and is a CODA site visitor. He was appointed to be the 2021 and 2023 Scientific Program Chair at the CDABO annual meeting. Recently, Dr. Park was elected to replace the immediate past president of the National E.H. Angle Society of Orthodontists, Dr. Ronald Champion. Lastly, he was appointed to be a founding member of the AAO Committee on Conferences & Meetings. He will be serving on the AAO Annual Session Doctor’s Scientific Program Committee in this capacity.
Tiffany H. Park
Tiffany H. Park is finishing her third-year dental student at The University of Pennsylvania School of Dental Medicine in Philadelphia, PA. She received her Bachelor of Arts degree from Pomona College where she majored in studio art and minored in chemistry. Born and raised in Southern California, Tiffany hopes to return home after graduation.
Yoon-Ah Kook
Yoon-Ah Kook is the former president of the Korean Association of Orthodontists and former vice dean of the Graduate School of Clinical Dental Science at The Catholic University of Korea. He is currently a professor of Orthodontics at Seoul Saint Mary's Hospital. He is also a clinical professor at the Arizona School of Dentistry & Oral Health and at Saint Louis University. He finished his orthodontic residency program at the Herman Ostrow School of Dentistry of the University of Southern California. Dr. Kook has published 150 recent articles in international peer-reviewed journals and has also published several book chapters.
References
- Proffit WR. Orthodontic Treatment Planning: From Problem List to Specific Plan. Contemporary Orthodontics. Philadelphia: Elsevier; 2019; 209–8.
- Garib DG, Bressane LB, Janson G, Gribel BF. Stability of extraction space closure. Am J Orthod Dentofacial Orthop. 2016;149(1):24–30. doi:10.1016/j.ajodo.2015.06.019.
- Janson G, Valarelli DP, Rizzo M, Valarelli FP. Prevalence of extraction space reopening in different orthodontic treatment protocols. Am J Orthod Dentofacial Orthop. 2017;152(3):320–326. doi:10.1016/j.ajodo.2017.01.019.
- Kook YA, Kim SH, Chung KR. A modified palatal anchorage plate for simple and efficient distalization. J Clin Orthod. 2010;44(12):719–730; quiz 43.
- Kook YA, Lee DH, Kim SH, Chung KR. Design improvements in the modified C-palatal plate for molar distalization. J Clin Orthod. 2013;47(4):241–248; quiz 67–68.
- Kook YA, Lim HJ, Park JH, Lee NK, Kim Y. 3D digital applications of the modified C-palatal plate for molar distalization. J Clin Orthod. 2021;55:773–781.
- Lee SK, Abbas NH, Bayome M, et al. A comparison of treatment effects of total arch distalization using modified C-palatal plate vs buccal miniscrews. Angle Orthod. 2018;88(1):45–51. doi:10.2319/061917-406.1.
- Park JH, Kook Y-A, Kim YJ, Lee N-K. Biomechanical considerations for total distalization of the maxillary dentition using TSADs. Semin Orthod. 2020;26(3):139–147. doi:10.1053/j.sodo.2020.06.011.
- Park JH, Kook Y-A, Kim Y, Kwang HL, Lee N-K. Improved facial profile with non-extraction treatment of severe protrusion using TSADs. Semin Orthod. 2022;28(3):157–163. doi:10.1053/j.sodo.2022.10.015.
- Kook YA, Park JH, Kim Y, Ahn CS, Bayome M. Orthodontic treatment of skeletal class II adolescent with anterior open bite using mini-screws and modified palatal anchorage plate. J Clin Pediatr Dent. 2015;39(2):187–192. doi:10.17796/jcpd.39.2.b5317m147r228760.
- Han SH, Park JH, Jung CY, Kook YA, Hong M. Full-step class II correction using a modified C-palatal plate for total arch distalization in an adolescent. J Clin Pediatr Dent. 2018;42(4):307–313. doi:10.17796/1053-4628-42.4.13.
- Park CO, Sa’aed NL, Bayome M, et al. Comparison of treatment effects between the modified C-palatal plate and cervical pull headgear for total arch distalization in adults. Korean J Orthod. 2017;47(6):375–383. doi:10.4041/kjod.2017.47.6.375.
- Alfawaz F, Park JH, Lee NK, et al. Comparison of treatment effects from total arch distalization using modified C-palatal plates versus maxillary premolar extraction in class II patients with severe overjet. Orthod Craniofac Res. 2022;25(1):119–127. doi:10.1111/ocr.12507.
- Jung CY, Park JH, Ku JH, Lee N-K, Kim Y, Kook Y-A. Dental and skeletal effects after total arch distalization using modified C-palatal plate on hypo- and hyperdivergent class II malocclusions in adolescents. Angle Orthod. 2021;91(1):22–29. doi:10.2319/031720-188.1.
- Kook YA, Park JH, Bayome M, Jung CY, Kim Y, Kim S-H. Application of palatal plate for nonextraction treatment in an adolescent boy with severe overjet. Am J Orthod Dentofacial Orthop. 2017;152(6):859–869. doi:10.1016/j.ajodo.2016.09.033.
- Lee YS, Park JH, Kim J, Lee N-K, Kim Y, Kook Y-A. Treatment effects of maxillary protraction with palatal plates vs conventional tooth-borne anchorage in growing patients with Class III malocclusion. Am J Orthod Dentofacial Orthop. 2022;162(4):520–528. doi:10.1016/j.ajodo.2021.05.014.
- Park JH, Oh JY, Lee SY, Kook YA, Han SH. Correction of an adult class III malocclusion through regaining of orthodontic space and an implant restoration. J Esthet Restor Dent. 2022;34(1):297–308. doi:10.1111/jerd.12870.
- Kook YA, Park JH, Bayome M, Sa’aed NL. Correction of severe bimaxillary protrusion with first premolar extractions and total arch distalization with palatal anchorage plates. Am J Orthod Dentofacial Orthop. 2015;148(2):310–320. doi:10.1016/j.ajodo.2014.10.035.
- Lim HJ. Cephalometric and Model Evaluations After Molar Distalization Using Modified C-Palatal Plates in Patients with Severe Arch Length Discrepancy. The Catholic University of Korea; 2021.
- Kook YA, Ku JH, Park JH, Park CO, Kim Y. Treatment of transposed canines and first premolars using miniscrew anchorage. J Clin Orthod. 2022;56:167–174.
- Park JH, Saito T, Yoo SK, Alfaifi M, Kook YA. Distalization with a modified C-palatal plate for severe upper crowding and a missing lower incisor. Korean J Orthod. 2020;50(1):52–62. doi:10.4041/kjod.2020.50.1.52.
- Park JH, Kim Y, Park JH, Lee N-K, Kim S-H, Kook Y-A. Long-term evaluation of maxillary molar position after distalization using modified C-palatal plates in patients with and without second molar eruption. Am J Orthod Dentofacial Orthop. 2021;160(6):853–861. doi:10.1016/j.ajodo.2020.06.052.
- Kim S, Lee NK, Park JH, et al. Treatment effects after maxillary total arch distalization using a modified C-palatal plate in patients with class II malocclusion with sinus pneumatization. Am J Orthod Dentofacial Orthop. 2022;162(4):469–476. doi:10.1016/j.ajodo.2021.04.033.
- Park JH, Kim S, Lee YJ, et al. Three-dimensional evaluation of maxillary dentoalveolar changes and airway space after distalization in adults. Angle Orthod. 2018;88(2):187–194. doi:10.2319/121116-889.1.
- Chou AHK, Park JH, Shoaib AM, et al. Total maxillary arch distalization with modified C-palatal plates in adolescents: a long-term study using cone-beam computed tomography. Am J Orthod Dentofacial Orthop. 2021;159(4):470–479. doi:10.1016/j.ajodo.2020.02.011.
- Shoaib AM, Park JH, Bayome M, Abbas NH, Alfaifi M, Kook Y-A. Treatment stability after total maxillary arch distalization with modified C-palatal plates in adults. Am J Orthod Dentofacial Orthop. 2019;156(6):832–839. doi:10.1016/j.ajodo.2019.01.021.
- Sa’aed NL, Park CO, Bayome M, Park JH, Kim Y, Kook Y-A. Skeletal and dental effects of molar distalization using a modified palatal anchorage plate in adolescents. Angle Orthod. 2015;85(4):657–664. doi:10.2319/060114-392.1.