

ABSTRACT
Background
Harm reduction, practices that reduce the harms associated with substance abuse without necessarily reducing drug use or consumption, may be a successful strategy to decrease drug-overdose deaths.
Types of Studies Reviewed
Article reviewed studies and policies that focused on harm reduction, prescription opioid abuse, medical-dental integration, and factors contributing to the rise in opioid-related deaths.
Results
The purpose of this article is to call upon oral health practitioners to recognize substance use disorders and adopt harm reduction strategies to improve health outcomes for patients experiencing or at risk for the disease.
Practical Implications
The article proposes four harm reduction strategies (Screen, Intervene, Refer, Collaborate) for dental professionals to incorporate into their clinical practices to contribute toward drug-overdose prevention efforts in California.
Continuing Education Credit Available
The practice worksheet is available online in the supplemental material tab for this article. A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20.
Introduction
Substance-use disorders (SUD), its beginnings, treatments, outcomes, and all interventions in between are very complex. It is a medical disorder in which there are functional changes to the brain circuits and is defined by the Diagnostic and Statistical Manual of Mental Disorders 5th Edition as a “type of substance-related disorder that involve a pathologic pattern of behaviors in which patients continue to use a substance despite experiencing significant problems related to its use”.Citation1 These changes in the brain may actually be present prior to the addiction, predisposing the patient to SUD, and can persist long after the person stops using the substance.Citation2
Substance use disorders affect all ages and demographics. The 2016 Surgeon General’s Reports on Alcohol, Drugs and Health showed that males (3.8%), those of two or more races (4.9%), Native Hawaiian/Pacific Islander (4.5%) American Indian or native Alaskan (4.1%), Black or African American (3.5%), and White (2.8%) comprised the largest demographics meeting the diagnostic criteria for having an SUD with illicit drug use.Citation3 In California, 18- to 25-year olds are the largest age demographic for using any substance, alcohol, illicit drugs, and pain medication (16.1%) followed by 12+ years (8.8%), 26+ years (8.1%), and 12–17 years (4.6%).Citation4 Illicit drug use has been found across all income levels and in both rural and metropolitan environments.Citation5 Lastly, children are not excluded in this problem. When marijuana is excluded, 4.9% of 8th graders, 5.7% of 10th graders, and 8.0% of 12th graders in the United States have used an illicit drug in 2022; thus, the American Academy of Pediatrics recommends screening for substance abuse starting at age nine.Citation6,Citation7
The COVID-19 pandemic has further exacerbated this epidemic. The National Survey on Drug Use and Health in the last quarter of 2020 showed that 15.4% (or 25.9 million) of people aged 12 years and older say they drank “a little more or much more” than before the pandemic.Citation8 When looking at drugs other than alcohol, 10.3% (or 10.9 million) in the same age category reported drug use “a little more or much more” than before the pandemic, with the largest increase in 12–25 years old respondents.Citation8
A typical dental practice serves patients within one of the above at-risk groups. Therefore, it is necessary to be cognizant of the challenges facing patients at risk for or experiencing a substance use disorder. As healthcare professionals, we have ethical and moral obligations for the overall well-being of our patients. In 2020, the Surgeon General specifically called on dentists to play a role in providing healthy lifestyles for our patients in an effort to improve not just oral health but systemic health, since the two cannot be separated.Citation9 On a population level, substance use has been associated with deteriorating relationships, poor school performance, diminished mental health, and loss of employment.Citation10 Furthermore, while many Americans may not meet the definition of having an SUD, misuse of alcohol and drugs can put a person at a higher risk for overdose, motor vehicle accidents, and violence.Citation10
Childhood substance abuse has added long-term effects of impaired growth and development of the brain. Children who abuse substances are more likely to participate in risky activities such as dangerous driving and unprotected sex and have higher risks of substance abuse as adults.Citation9 Children who themselves do not use drugs and alcohol but witness substance abuse in their home are considered to have adverse childhood experiences (ACES).Citation11 Increased ACES in childhood leads to increased risks for substance abuse, chronic health problems, and mental illness and can lead to negative impacts on education and future jobs.Citation11
The concept of medical-dental integration is gaining momentum as a strategy to address SUD. In 2020, the Centers for Disease Control (CDC) Division of Oral Health (DOH) awarded funding to additional stakeholders to create a framework around medical-dental integration strategies, recommendations, and assessments.Citation12 On a state level, Smile California (website for Medi-Cal Dental Program) offers oral health toolkits for physicians and other staff in a primary care setting.Citation13 In December 2022, the University of California, San Francisco (UCSF) became the first academic health center on the West Coast to integrate medical and dental records allowing all healthcare professionals to provide more comprehensive patient care.Citation14 These examples demonstrate how dentists can work with medical providers to improve health outcomes for patients. Leveraging these relationships and modifying existing dental health counseling strategies can make a significant difference in substance abuse disorder outcomes. These strategies are simple, require little monetary investment, and can be implemented into existing dental practices.
The purpose of this article is to call upon oral health practitioners to recognize SUDs and adopt strategies to improve health outcomes for patients experiencing or at risk for the disease.
Dentistry’s Response to the Opioid Epidemic
Changes in Dental Pain Management Prescribing Practices
According to a study using nationwide insurance claims of more than 87 million adults from 2010 to 2016, over 16 million opioid prescriptions were filled by opioid-naive patients. While our medical colleagues reduced their opioid prescribing practices rapidly, dentists lagged in changing prescribing practices. Over the course of the study, the proportion of opioid prescriptions for dental care increased by 67.8%. Thus, in the timeframe of the study, opioid prescriptions for dental needs became a bigger share of overall opioid prescriptions, even though dentist decreased their overall prescription rate.Citation15 A 2019 California Health Interview Survey data showed that for individuals who misused prescription painkillers, the top reasons for taking the medications included chronic pain (52%), surgery that was not related to an accident (28%) and dental work (23%).Citation16 In response, in 2018, the American Dental Association (ADA) was among the first major health organizations to declare intention to reduce opioid prescribing practices in the dental community by adopting its “Interim Board Policy on Opioid Prescribing”.Citation17 This policy supported mandatory continuing education on controlled substances in addition to dentists registering with prescription drug monitoring programs (PDMP). Most recently, on January 1, 2023, California dentist licentiates are required to complete continuing education on the responsibilities and requirements of prescribing opioids.Citation18 All of these steps move toward reaffirming the importance of continual training and education on prescribing practices.
The Role of Drug Monitoring and Electronic Prescriptions
As of 2016, PDMPs were used nationally by only half of surveyed dentists. Of those using the monitoring program, most found that the practice did not change their intended prescription (40.2%), led them not to prescribe an opioid (33.5%), or prescribe fewer opioid doses (25.5%).Citation19 In 2018, California implemented the Controlled Substance Utilization Review and Evaluation System (CURES), an online database to track the prescription of controlled substances. However, an exemption was granted if the controlled substance was part of a patient’s surgical procedure and was less than a 5 days’ supply, allowing for a 5-day prescription regimen that was both in compliance with and yet avoided CURES utilization.Citation20 In 2019, the California Dental Association adopted an opioid policy that promoted a PDMP as well as assessing a patient’s full medical profile to evaluate for potential substance use disorder prior to prescribing opioids.Citation21 Most recently, 2022 brought California practitioners to further stringent requirements under Assembly Bill 2789, a mandatory electronic-prescribing measure for all prescriptions in the state of California.Citation22
Falling Short: Overdose Deaths Persist
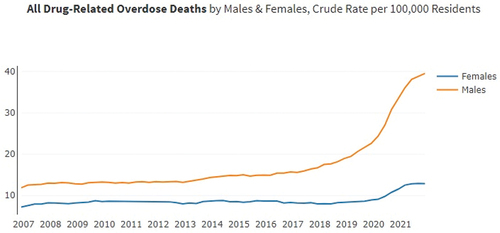
Despite these measures, the need for continued and ongoing vigilance persists. An area of success has been a continued downward trajectory of California’s opioid prescription rates that began in 2016 (). However, there has been a simultaneous increase in drug-related deaths and hospitalizations in the state. In 2021, 7,833 men and 2,583 women died from drug-related overdose, compared to the same timeframe the preceding year which registered 6,590 male and 2,304 female deaths ().Citation23 While efforts to reduce opioid prescription remain an area of intervention, such efforts now have diminishing returns. As demonstrated by the spike in all drug-related deaths, opioid prescription reduction alone is insufficient to curtail the damage to our patients and across our communities. There is a need for an evolving approach toward harm reduction to effect the change that prescription opioid management alone has not been able to achieve.
Figure 1. California opioid prescriptions, per 1,000 residents, 2009–2021.Citation23
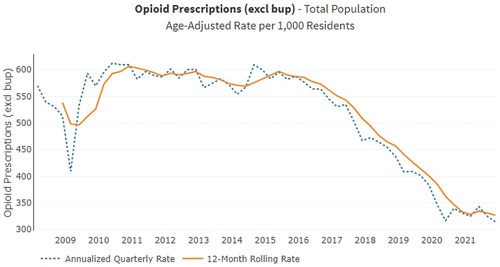
Figure 2. California drug-related overdose deaths, per 100,000 residents, 2007–2022.Citation23
Harm Reduction: A 4-Step Response to the Ongoing Opioid Epidemic
Harm Reduction: A Possible Solution?
According to Dr. Jerome Adams, former U.S. Surgeon General, more novel and comprehensive approaches are necessary to address the “opioid paradox;” a term which describes the rise in overdose deaths despite a 20-year low in opioid prescriptions.Citation24,Citation25 This rise has been attributed to an increase in illicit fentanyl, heroin, and methamphetamine use since 2016.Citation25 Harm reduction is a novel strategy that has been adopted and implemented by the medical profession. Instead of narrowly defining success as avoidance of the harmful behavior, specifically the use and abuse of the drug, harm reduction more broadly defines success as decreasing the adverse effects associated with substance abuse, primarily overdose and death.Citation26 It encompasses a multitude of targeted interventions that address safer drug use and consumption. Some critics argue that harm reduction fails to condemn or treat substance abuse and may promote continuous injuries. On the contrary, harm reduction is an evidence-based strategy with proven historical success in reducing transmission of HIV and hepatitis through needle exchange and condom distribution programs.Citation27 Harm reduction may also prove to be a successful strategy to end our nation’s “opioid paradox”.
The Theoretical Framework of Harm Reduction
Harm reduction is based upon the Stages of Change Model, which asserts that behavior change is a cyclical rather than a terminal process with individuals entering, exiting, and reentering behavioral stages based upon their readiness for change.Citation28 These stages include pre-contemplation, contemplation, preparation, action, maintenance, and termination. For patients to progress through these behavioral stages, healthcare providers work with patients in developing interventions that move them to the next stage of change. The goal is for patients to reach the termination stage. However, harm reduction assumes a more pragmatic approach by “meeting people where they are at” and focusing on interventions that promote safer behavior at any given stage of change, even with patients who express no desire to discontinue their drug use (pre-contemplation) or achieve abstinence (termination). It positions the individual in the “driver’s seat,” recognizes any positive change as “moving in the right direction,” and acknowledges everyone’s unique pathway to health.Citation29 According to the National Harm Reduction Coalition, harm reduction is designed to respect the rights of individuals who use drugs, empower them to reduce the harms, and recognize the social determinants that contribute and impact substance abuse.Citation30
Principles of Harm Reduction and Its Applicability in Primary Health Care
We will describe four key principles of harm reduction and provide evidence-based activities taking place in primary care settings that support these principles.Citation30
Principle 1: Drug Use is Part of Our World and Rather Than Ignore or Condemn, Work Towards Minimizing Its Harmful Effects
This principle is rooted in pragmatism, specifically that patients engage in unhealthy behaviors despite knowledge of associated adverse consequences. When healthcare providers accept this harsh reality, they become better positioned to recommend actions that can minimize the worst possible outcomes of overdose and death. In 2018, the California Naloxone Requirement Bill, AB 2760,Citation31 was passed, requiring prescribers to offer a prescription of naloxone or any other opioid reversal drug to patients at risk for an overdose and/or prescribed the following:
More than 90 or more morphine milligram equivalents of an opioid
An opioid and a benzodiazepine concurrently
Naloxone (4 mg/0.1 ml) is an opioid antagonist that blocks opioid receptor sites, reversing the effects of an overdose associated with fentanyl, heroin, or prescription opioids.Citation32 It can be administered intranasally or intramuscularly, with a reversal effect within 2 to 3 minutes.Citation32 Naloxone distribution was estimated to prevent one overdose for every 227 naloxone kits distributed, resulting in a 6% reduction in overdose deaths.Citation33 Increasing naloxone access is an evidence-based strategy that reduces the worst possible outcome associated with opioid use. Could dentists offer naloxone to all patients at risk for opioid overdose, including those with substance-use disorders and those prescribed opioid medications?
Principle 2: People Who Use Drugs Must Be the Primary Agents for Reducing the Harms Associated with Their Drug Use
Autonomy is a well-known principle in health care that gives patients the right to make their own healthcare decisions. When applied, autonomy empowers individuals to make safer decisions regarding their drug use and promotes incremental behavior changes that are less injurious. Since 2017, the California Department of Public Health has distributed fentanyl test strips to needle syringe access programs across the state. Fentanyl, a synthetic opioid more potent than both heroin and morphine, is a contaminant introduced into the drug supply. It causes rapid respiratory depression and is responsible for the increase in drug overdose deaths. Access to fentanyl test strips provides individuals with the autonomy to determine if their drugs are laced with fentanyl before use and inform others about the potential for a contaminated community drug supply. In a recent study, 45% of participants who received a positive result from a rapid fentanyl test strips reported using smaller amounts, 42% reported slower self-administration, and 38% reported using only in the presence of another individual.Citation34 In 2022, the Controlled Substance Bill, AB 1598, was signed into law legalizing testing equipment used to analyze substances for the presence of fentanyl and its associated analogs.Citation35 Fentanyl test strips are now available at local pharmacies, public health agencies, and on-line retailers. Could dentists direct patients to resources for safer drug use and consumption?
Principle 3: Provide Non-Judgmental Services and Resources to People Who Use Drugs
Health condition-related stigma includes a spectrum of negative beliefs and stereotypes about groups of individuals with specific diseases and health conditions.Citation36 Patients are more likely to experience denial of care, substandard care, prolonged wait times, and additional barriers to care with providers who hold negative stereotypes and beliefs about addiction.Citation37 To address stigmatization, medical education has modified their addiction curriculums to develop a more compassionate workforce competent in treating the complexities of the disease.Citation38 These curriculums promote the use of non-stigmatized language that is people-first (e.g. “person with an opioid use disorder”), incorporate medical terminology (e.g. “negative test result”), and use words that promote recovery (“taking steps in the right direction”).Citation39 These strategies create respectful relationships and build trusted provider–patient relationships, which may motivate patients to accept harm reduction strategies of care.
Of equal importance is looking beyond the physical needs of patients to the social environments that impact both the initiation and continuation of substance use. These factors include racism, homelessness, poverty, incarceration, domestic violence, and mental illness.Citation40 The REACH program (Respectful, Equitable Access to Compassionate Healthcare), a not-for-profit community-based medical practice in New York, is a program that conducts bio-psychosocial assessments, identifies patients’ treatment goals and social situations, provides primary medical care, and partners with agencies to provide housing.Citation41 Interprofessional collaborations connect patients to vital resources, provide health care within the social context of the patient, and work toward destigmatizing addiction beyond the boundaries of health care. As dental professionals, can we go beyond our own professional walls and develop interdisciplinary relationships with behavioral and social service colleagues to support patients with substance use disorders?
Principle 4: Understand Drug Use as a Complex, Multi-Faceted Disease, with a Continuum of Behaviors from Severe Use to Total Abstinence
Healthcare providers are trained in obtaining comprehensive patient health histories to detect diseases and conditions that impact quality of life and compromise treatment outcomes. The U.S. Preventive Health Services Task Force issued a recommendation that all adults ages 18 and older be screened for unhealthy drug use.Citation42
Obtaining a history of substance use is essential in appreciating not only the complexity of the disease but its impacts on treatment and health outcomes. Screening, brief intervention, and referral to treatment (SBIRT) is an evidence-based screening tool that has been easily implemented in a variety of healthcare settings and easily adapted by multidisciplinary professionals serving diverse populations.Citation43 It includes a series of structured questions to help identify patients with substance use disorders followed by a brief intervention aimed at raising patients’ awareness of both the inherent risks of substance misuse and any motivations toward less harmful consumption and use.Citation44 The use of SBIRT assists providers in establishing cross-disciplinary relationships with referral partners when patients need and request treatment, intervention, and harm reduction strategies. At-risk adolescents identified as using substances within the past year and who received SBIRT reported a significant reduction in substance use at follow-up.Citation45 Is screening for substance use disorders part of our professional responsibility as oral health providers?
Harm reduction is an effective evidence-based strategy to promote safer drug practices and may be a successful strategy to end our nation’s “opioid paradox.” However, success will require a multi-disciplinary response that addresses the physical, behavioral, and social impacts of the disease. Dental professionals are well poised to integrate harm reduction strategies into their clinical practice and develop interprofessional collaborations and strategies that reduce the risks of drug overdose and deaths in their patients. Before we propose these strategies, we will examine dentistry’s role in implementing medical integration strategies to decrease tobacco use in this country.
Medical-Dental Integration
An intercept between medical and dental disciplines is referred to as medical-dental integration or interprofessional practice. Medical-dental integration includes the incorporation of preventive dental care into primary medical care settings and medical screenings into oral health settings. Integration intends to refocus health care into patient-centered care and in doing so, improve health outcomes, and lower overall costs to healthcare systems.Citation46 For some patient populations where patients avoid traditional primary care practitioners entirely, the dental practitioner is a frequently visited healthcare provider. In these cases, dentists may be the only healthcare provider interacting with a patient wherein medical screening during these oral health encounters plays a significant role in the health of such patients. Dental patients deserve to be attended to fully and that includes making appropriate medical referrals and counseling when indicated – this can and should include substance use screening, counseling, and harm reduction efforts. To demonstrate a historical perspective and the impact of dentists’ role on patient-centered care, we look to the history of medical-dental integration using the model of tobacco cessation and oral cancer screening.
Tobacco Cessation, Oral Cancer Screening, and Dentistry’s Role
An example of medical-dental integration is tobacco cessation counseling and screening for suspicious oral lesions. The present model calls upon dentists to screen for tobacco use and provide referrals for counseling with varying degrees of intervention based on the practitioner’s training and comfort level. The concept is widely accepted as being within the scope of dentists.Citation47 Further, oral cancer screening is a critical component of the dental examination with the ADA publishing in 2010 and then updating in 2017, a Clinical Practice Guideline on the evaluation of potentially malignant disorders of the oral cavity. The ADA’s clinical practice guidelines include what might seem commonplace in dentistry today but are a demonstration of medical screening in an oral health setting: gathering of medical and social history regarding risk factors like tobacco and alcohol use, performing intraoral and extraoral tactile and visual examinations, taking a biopsy of any suspicious lesions, and referring to a medical provider when appropriate. These tasks when incorporated into a dental examination improve health outcomes for oral cancer through early detection and reduce patients’ exposures to known risk factors.Citation48
Dentistry’s Challenges and Successes in Tobacco Cessation and Oral Cancer Screening
Dentists might presently accept the responsibilities of tobacco cessation and screening for potentially malignant disorders of the oral cavity, but it has not always been the case. A 2008 publication described a concept of “clinical inertia” regarding the delay or failure to incorporate tobacco cessation intervention into dental practice.Citation49 These delays are costly in health as they prevent patients from receiving the most up-to-date and timely interventions and preventable conditions go underdiagnosed or undertreated. More recently, a 2020 study demonstrated that dentists successfully perform oral cancer screening in the United Kingdom. Forty percent of oral cancer cases were referred for evaluation by dental practitioners, whereas general medical practitioners referred 50% of cases. Further, cases referred by dentists tended to be asymptomatic and at an earlier stage of disease.Citation50 The dental profession has thus demonstrated a capacity and competence in improving health outcomes for patients in regard to oral cancer.
Expanding Medical-Dental Integration Efforts
Medical-dental integration continues to be an area of growth. In 2020, the Centers for Disease Control began a multi-year project to establish a national framework for areas to integrate medical and dental services in order to support populations with unmet oral health needs and associated chronic diseases. Other areas of medical integration in dental settings include screening for (and sometimes treating) obstructive sleep apnea,Citation51 providing nutrition counseling,Citation52 making immunization recommendations regarding Human Papillomavirus,Citation53 and even administering COVID-19 vaccines.Citation54 If dentists have incorporated and effected positive change on traditional medical issues, it is not a leap at all to address and curb substance use disorders in our patient populations. We do, however, need to get past our clinical inertia and get on with the task of providing whole-person care to meet our patients’ needs. What are these tasks that oral health practitioners can incorporate in order to achieve improved health outcomes for patients with a substance use disorder? How should oral health practitioners frame their mind-set, goals, and role in doing so?
Dentistry’s Role in Harm Reduction: A 4-Step Call to Action
Dentists are well poised to integrate the principles of harm reduction into their clinical practices. The tools of screening, intervention, referral, and interdisciplinary collaborations utilized to treat diseases of the oral cavity and address tobacco use can be easily amended as harm reduction strategies for patients with substance use disorders.
Step 1: Screen Patients for Substance Use Disorders Regardless of Perceived Risk
Screening dental patients is an essential component of any harm reduction strategy. Although 93% of dentists recognize the importance of screening patients for substance use disorders, the majority (84%) report lack of knowledge as the most significant barrier for implementing screening, and a significant minority (23%) believe that the dental environment is an inappropriate setting to inquire about illicit drug use.Citation55 While acknowledging that addiction is an “everywhere” and “everybody” problem, dentists must understand the urgency of addressing this issue. Predoctoral training needs to expand curriculums to develop a dental workforce competent in identifying patients with substance use disorders and recognizing the physical, behavioral, and oral manifestations of the disease. Efforts are currently underway, both at the national and state level, to increase screening and prescribing practice competencies. The U.S. Drug Enforcement Administration requires all prescribers of controlled substances, on or after June 27, 2023, to complete 8 hours of a one-time training on safe pharmacological management of dental pain and SBIRT for patients with, or at risk of developing opioid and other substance use disorders.Citation56 In January 2023, the Dental Board of California amended Title 16 (California Code of Regulations, Section 1016 and 1017) to require that all dental licensees complete a mandatory 2-hour course on the responsibilities and requirements of prescribing Schedule II opioids and the recognition of patients at-risk for or with substance use disorders.Citation57 These mandatory courses for licensure address real or perceived barriers associated with knowledge and implementation of screening practices.
The availability of on-line evidence-based screening and assessment tools ()Citation58 removes any barriers practitioners may have regarding where to obtain resources to assess patients’ misuse and consumption of controlled substances. In addition to these available resources, dentists should use their health history forms as a supplemental screening tool. Patients who report taking medications with a high potential for misuse (depressants, stimulants, and opioids) as well as those taking medications used to treat opioid-use disorders including Buprenorphine (Subutex, Suboxone, Zubsolv, Probuphine, Sublocade), Naltrexone (Revia, Depade, Trexan), and Methadone (Dolophine, Methadose, Methadone Intensol, Diskets) require further interviewing regarding frequency and duration of use and diagnosis.Citation59 Dentists can also consider amending their health history form to include questions that ask about current and past histories of non-prescription and illicit drug use. The screening process should be brief, universal, comprehensive, and target risky substance use behaviors.Citation60
Table 1. Clinician Administered Screening Tools | Source National Institute on Drug Abuse.Citation58
Step 2: Assess patients’ Readiness to Change and Interest in Harm Reduction Interventions
Assessing patients’ readiness for change and desire to move toward less harmful behaviors are necessary steps in “meeting patients where they are” in the cyclical process of behavior change. It empowers patients to be the vehicle of change, if they desire, to reduce the harms associated with their drug use. Motivational interviewing is an effective tool to explore patients’ ambivalence, perceived challenges, and intrinsic motivation to change harmful behaviors.Citation61 The basic tenets of motivational interviewing include open-ended questions, affirming statements, reflective listening, and summary statements, also known as OARS, to elicit self-motivating statements of harm reduction. It is important to remember that “words matter.” As dental professionals, we have the responsibility to deconstruct the stigmatization of addiction and avoid words that are accusatory, disapproving, judgmental, and labeling. Examples of motivational interviewing are summarized in .Citation62
Table 2. Basic Tenets of Motivational Interviewing (OARS).Citation62
Step 3: Prevent Drug Overdose Deaths by Increasing patients’ Access to Naloxone
Due to our understanding of prevention, dentists are well positioned to prevent drug overdose deaths in their patients. By complying with The California Naloxone Requirement Bill, AB 2760, and co-prescribing naloxone with opioids, dentists increase patients’ access to one of the most effective preventive measures for overdose.Citation31 Currently, pharmacies are the primary source for patients to obtain prescribed naloxone. However, some patients report hesitancy in picking up prescriptions for naloxone due to negative perceptions and stigmatization by pharmacy personnel.Citation63 To address this, efforts are underway nationally and locally to increase non-pharmacy access to naloxone not just for patients prescribed opioid pain medications but also for patients screened and identified as high-risk. In March of 2023, the Food and Drug Administration, approved Naloxone nasal spray for over-the-counter use to be sold directly to consumers.Citation64 The Naloxone Distribution Project, administered by the California Department of Public Health, is a network of county public health and behavioral agencies (emergency departments, fire authorities, homeless programs, and libraries) that provides free take-home naloxone kits.Citation65 These kits contain nasal formulations of naloxone, gloves, alcohol swabs, face shields for rescue breathing, and instructions on overdose awareness, response, and management. Although dental offices have not been identified as eligible distribution centers, dentists can direct patients to qualified centers or mail delivery services as an alternative to retail pharmacies ().Citation66 In addition, naloxone is now considered an essential medication in dental emergency kits.Citation67 All dental personnel should be trained on how to recognize the symptoms of opioid overdose including pupillary constriction, shallow breathing, cyanosis, and unconsciousness and how to administer naloxone in the event of an in-office overdose emergency.Citation68
Table 3. Patient Resources for Naloxone in California.Citation66
Step 4: Engage in Collaborative Relationships and Referrals with Medicine and Behavioral Health
Interdisciplinary collaboration and referral are critical steps in the harm reduction process that improves health outcomes for patients. The importance of developing collaborative relationships with medical and behavioral specialists cannot be understated. There is growing evidence of the bi-directional relationship between oral and systemic health and the multidirectional relationship with behavioral health.Citation69 Harm reduction requires an integrated model of care. However, more than 40% of dentists report a lack of referral resources as a perceived barrier to addressing patients' illicit drug use.Citation55 Therefore, it is essential for dental providers to become aware of professional resources for patients with substance use disorders. The Substance Abuse and Mental Health Resource Administration (SAMHSA) provides an online treatment locator and confidential helpline for substance use, mental health, primary care, and buprenorphine therapy.Citation70 The Wellness Program with the California Dental Association provides a list of treatment referral sources ().Citation71 By providing community resources, dentists increase patients’ access to behavioral and medical resources for harm reduction.
Table 4. Treatment Referral Resources | Source Substance Abuse and Mental Health Services Administration,Citation70 California Dental Association.Citation71
In addition, more integrated models of care exist within large provider organizations, such as federally qualified health centers and dental service organizations, where medical, dental, and behavioral health providers share the same practice space. In these models, electronic health records may be integrated allowing for collaborative and holistic treatment plans that include harm reduction strategies and cross-disciplinary screenings and referrals.Citation72
Conclusion
By working together, dentistry can forge partnerships aimed at creating compassionate, safe, and holistic care for patients who use drugs. The rise in opioid-related overdoses and deaths, despite a sharp decline in opioid prescription rates, requires a novel approach to address the current opioid epidemic impacting both our state and nation. Harm reduction decreases the worst possible outcomes associated with opioid use. Screening, assessing, increasing access to opioid-reversal agents, and establishing interdisciplinary collaborative and referral relationships, inherent in harm reduction, are well within the scope, competence, and responsibilities of dental professionals. Integrating harm reduction into our daily clinical practices will improve the quality of lives for our patients, and for those who use drugs, harm reduction may save their lives. Can these strategies of harm reduction make a difference for your patients?
Supplemental Material
Download MS Word (29.7 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2242570.
Additional information
Notes on contributors
Ronni Brown
Ronni Brown, DDS, MPH received her dental and public health training at the University of California, Los Angeles and completed a dental public health residency at the University of California, San Francisco. She is an international speaker and published author on the oral effects of substance use disorders. She practices with Wellpath at the Sonoma County Main Adult Detention Facility in Santa Rosa, California.
Wai-Yin Chan
Wai-Yin Chan MS, DMD, MPH is a pediatric dentist at a Federally Qualified Health Center practicing in San Diego County, California. She maintains privileges at Rady Children's Hospital and serves as clinical faculty for NYU-Langone Advanced Education in Pediatric Dentistry. Dr. Chan is a diplomate of the American Board of Pediatric Dentistry. Dr. Chan's interests include the integration of medicine and dentistry, promoting HPV immunization awareness, providing and advocating for the care of patients with special health needs and supporting resident education in the specialty of pediatric dentistry. Dr. Chan serves as San Diego County’s Champion Provider Fellow and on a variety of coalitions including the San Diego County Oral Health Coalition, San Diego Medical Dental Integration Workgroup, The San Diego Immunization Coalition and the San Diego PATH (Protecting Against HPV) Steering Committee.
Fadra Whyte
Fadra Whyte, DMD, MPH received her dental training at the University of Pennsylvania and her pediatric dental residency training at Lutheran Medical Center in Brooklyn, NY. She has since completed her master of public health with a focus in dental public health at A.T. Still University. Her interests include treatment of children with special health care needs, access to dental care issues, and medical-dental integration. She is faculty with NYU Langone Advanced Education in Pediatric Dentistry- San Diego and is the Chief Dental Officer for the County of San Diego.
References
- Black DW, Grant JE. DSM-5 Guidebook: The Essential Companion to the Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlinghton, VA: American Psychiatric Association Publishing; 2014.
- Goldstein RZ, Volkow ND. Dysfunction of the prefrontal cortex in addiction: neuroimaging findings and clinical implications. Nat Rev Neurosci. 2011;12(11):652–10. doi:10.1038/nrn3119.
- U.S. Department of Health and Human Services. Facing addiction in America. The surgeon general’s report on alcohol, Drugs, And Health. 2016. SMA 16-4991. https://addiction.surgeongeneral.gov/sites/default/files/surgeon-generals-report.pdf. Accessed September 6, 2022.
- California Health Care Foundation. Substance use in California; Prevalence and treatment. January, 2022. https://www.chcf.org/wp-content/uploads/2022/01/SubstanceUseDisorderAlmanac2022.pdf. Accessed September 6, 2022.
- Mack KA, Jones CM, Ballesteros MF. Illicit drug use, illicit drug use disorders, and drug overdose deaths in metropolitan and nonmetropolitan areas — United States. MMWR Surveill Summ. 2017;66(No. SS–19):1–12. doi:10.15585/mmwr.ss6619a1.
- Meich RA, Johnston LD, Patrick ME, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future National Survey Results on Drug Use, 1975-2022 Secondary Students. Ann Arbor, MI: Institute for Social Research, University of Michigan; 2023.
- CDC. Teen substance abuse & risks. Updated February 10, 2020. https://www.cdc.gov/ncbddd/fasd/features/teen-substance-use.html. Accessed September 6, 2022.
- Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: results from the 2020 national survey on drug use. October 2021. PEP21-07-01-003. https://www.samhsa.gov/data/sites/default/files/reports/rpt35325/NSDUHFFRPDFWHTMLFiles2020/2020NSDUHFFR1PDFW102121.pdf. Accessed September 6, 2022.
- U.S. Department of Health and Human Services. Oral health in America: a report of the surgeon general. Rockville, MD: U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2020.
- U.S. Department of Health and Human Services (HHS), Office of the surgeon general, facing addiction in America: the surgeon general’s spotlight on opioids. Washington, DC: HHS; September 2018.
- CDC. Fast facts: preventing adverse childhood experiences. Updated April 6, 2022. https://www.cdc.gov/violenceprevention/aces/fastfact.html. Accessed September 6, 2022.
- CDC Announces Medical-Dental Integration Partnership. Centers for disease control and prevention division of oral health. Updated October 28, 2020. https://www.cdc.gov/oralhealth/about/md-integration.html. Accessed May 28, 2023.
- Smile California. Primary care physician toolkit: Smile California; 2023. https://smilecalifornia.org/partners-and-providers/#Physician_toolkit. Accessed May 28, 2023.
- Fernandez E. UCSF is first to integrate records across medical and dental. The Regents of the University of California; December 5, 2022. https://www.ucsf.edu/news/2022/12/424361/ucsf-first-integrate-records-across-medical-and-dental. Accessed May 28, 2023.
- Larach DB, Waljee JF, Hu HM, et al. Patterns of initial opioid prescribing to opioid-naive patients. Ann Surg. 2020;271(2):290–295. doi:10.1097/SLA.0000000000002969.
- Muñoz TA, Arthur KN Adult prescription painkiller misuse in California, 2017-2019. https://www.cdph.ca.gov/Programs/CCDPHP/sapb/CDPH%20Document%20Library/Adult-Prescription-Painkiller-Misuse-in-California_2017-2019_final.pdf. Published 2022. Accessed September 19, 2022.
- Garvin J. ADA News: ADA adopts interim opioids policy. March, 2018. https://www.wsda.org/news/blog/2018/03/29/ada-adopts-interim-opioids-policy. Published March 29, 2018. Accessed September 13, 2022.
- Dental Board of California. Important notice: changes to continuing education courses required for license renewal effective January 1, 2023. https://www.dbc.ca.gov/formspubs/alert_imp_ce_changes.pdf. Published 2022. Accessed January 16, 2023.
- McCauley JL, Gilbert GH, Cochran DL, et al. Prescription drug monitoring program use: national dental PBRN results. JDR Clin Trans Res. 2019;4(2):178–186. doi:10.1177/2380084418808517.
- Medical Board of California. CURES 2.0 mandatory use begins October 2, 2018. https://www.mbc.ca.gov/Download/Fact-Sheets/CURES-Mandatory-Use.pdf. Published May 2018. Accessed September 13, 2022.
- California Dental Association. CDA opioid policy. https://www.cda.org/Portals/0/pdfs/policy_statements/policy_opioid.pdf. Published 2019. Accessed September 13, 2022.
- Wood. Assembly bill no. 2789 chapter 438. https://leginfo.legislature.ca.gov/faces/billTextClient.xhtml?bill_id=201720180AB2789. Published September 17, 2018. Accessed September 13, 2022.
- California Department of Public Health. California dashboard. California overdose surveillance dashboard. https://skylab.cdph.ca.gov/ODdash/. Published July 19, 2022. Accessed September 13, 2022.
- Kharasch ED, Clark JD, Adams JM. Opioids and public health: the prescription opioid ecosystem and need for improved management. Anesthesiology. 2022;136:10–30. doi:10.1097/ALN.0000000000004065.
- Manchikanti L, Singh VM, Staats PS, et al. Fourth wave of opioid illicit drug overdose deaths and diminishing access to prescription opioids and interventional techniques: cause and effect. Pain Physician. 2022;25(2):97–124. PMID: 35322965.
- Kapadia SN, Griffin JL, Waldman J, Ziebarth NR, Schackman BR, Behrends CN. A harm reduction approach to treating opioid use disorder in an independent primary care practice: a qualitative study. J Gen Intern Med. 2021;36(7):1898–1905. doi:10.1007/s11606-020-06409-6. Epub 2021 Jan 19. PMID: 33469774; PMCID: PMC7815286.
- Yau B, Sollows D, Young S, Buxton JA. The physician’s role in harm reduction. BDMJ. 2018;60:404–405.
- Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983;51(3):390–395. doi:10.1037/0022-006X.51.3.390.
- Gallagher K The humanistic roots of harm reduction. Society For Humanistic Psychology Newsletter 2017. www.apadivisions.org/division-32/publications/newsletters/humanistic/2017/10/harm-reduction. Accessed August 12, 2022.
- Principles of harm reduction: national harm reduction coalition. www.harmreduction.org/about-us/principles-of-harm-reduction/. Accessed August 12, 2022.
- California legislative information: assembly bill no. 2760. Prescription drugs; prescribers; naloxone and other FDA-approved drugs. 2017-2018. https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=201720180AB2760 Accessed August 12, 2022.
- National Institute on Drug Abuse. Naloxone for opioid overdose: life-saving science. https://nida.nih.gov/publications/naloxone-opioid-overdose-life-saving-scienceon2023. Updated 2017-03-30. Accessed May 22, 2023.
- Coffin PO, Sullivan SD. Cost-effectiveness of distributing naloxone to heroin users for lay overdose reversal. Ann Int Med. 2013;158(1):1–9. doi:10.7326/0003-4819-158-1-201301010-00003. Erratum in: Ann Intern Med. 2017 May 2;166(9):687. PMID: 23277895.
- Krieger MS, Goedel WC, Buxton JA, et al. Use of rapid fentanyl test strips among young adults who use drugs. Int J Drug Polic. 2018;61:52–58. doi:10.1016/j.drugpo.2018.09.009. Epub 2018 Oct 18. PMID: 30344005; PMCID: PMC6701177.
- California legislative information: assembly bill no. 1598. An act to amend Sections 11014.5 and 11364.5 of the health and safety code, relating to controlled substances. https://leginfo.legislature.ca.gov/faces/billNavClient.xhtml?bill_id=202120220AB1598. Accessed September 4, 2022.
- Stangl AL, Earnshaw VA, Logie CH, et al. The health stigma and discrimination framework: a global, crosscutting framework to inform research, intervention development, and policy on health-related stigmas. BMC Med. 2019;17(1):31. doi:10.1186/s12916-019-1271-3. PMID: 30764826; PMCID: PMC6376797.
- Nyblade L, Stockton MA, Giger K, et al. Stigma in health facilities: why it matters and how we can change it. BMC Med. 2019;17(1):25. doi:10.1186/s12916-019-1256-2. PMID: 30764806; PMCID: PMC6376713.
- Slack G. Teaching medical students how to prevent, treat addiction. Stanford Medicine; April, 2022. https://med.stanford.edu/news/all-news/2022/04/addiction-medicine-curriculum.html. Accessed August 12, 2022.
- Language matters. BCCDC National Harm Reduction Services. 2017. https://towardtheheart.com/assets/uploads/1512674325aOAkOYmxn5R3JpXBE1udQKm9ypzwBNP1OkjtwcJ.pdf. Accessed August 12, 2022.
- Galea S, Vlahov D. Social determinants and the health of drug users: socioeconomic status, homelessness, and incarceration. Public Health Rep. 2002;117(1):135–145. PMID: 12435837; PMCID: PMC1913691.
- Riazi F, Toribio W, Irani E, et al. Community case study of naloxone distribution by hospital-based harm reduction program for people who use drugs in New York City. Front Sociol. 2021;6:619683. doi:10.3389/fsoc.2021.619683. PMID: 34307540; PMCID: PMC8292929.
- Preventive Services Task Force US, Krist AH, Davidson KW, et al. Screening for unhealthy drug use: US preventive services task force recommendation statement. JAMA. 2020;323(22):2301–2309. doi:10.1001/jama.2020.8020. PMID: 32515821.
- Hargraves D, White C, Frederick R, et al. Implementing SBIRT (screening, brief intervention and referral to treatment) in primary care: lessons learned from a multi-practice evaluation portfolio. Public Health Rev. 2017;38:31. doi:10.1186/s40985-017-0077-0. PMID: 29450101; PMCID: PMC5809898.
- SBIRT: screening, brief interventions and referral to treatment. Substance Abuse And Mental Health Services Administration; 2022. https://www.samhsa.gov/sbirt. Accessed August 12, 2022.
- Soberay A, DeSorrento L, Pietruszewski P, Sitz M, Levy S. Implementing adolescent SBIRT: findings from the FaCES project. Subst Abus. 2021;42(4):751–759. doi:10.1080/08897077.2020.1846662. Epub 2021 Sep 7. PMID: 34491880.
- Oral health resources: Medical-Dental Integration. DentaQuest. https://dentaquest.com/oral-health-resources/medical-dental-integration/. Accessed January 6, 2023.
- Virtue SM, Waldron EM, Darabos K, et al. Dental students’ attitudes toward tobacco cessation in the dental setting: a systematic review. J Dent Educ. 2017;81(5):500–516. doi:10.21815/JDE.016.016.
- Lingen MW, Abt E, Agrawal N, et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity: a report of the American Dental Association. J Am Dent Assoc. 2017;148(10):712–727.e10. doi:10.1016/j.adaj.2017.07.032.
- Rindal DB, Rush WA, Boyle RG. Clinical inertia in dentistry: a review of the phenomenon. J Contemp Dent Pract. 2008;9(1):113–121. doi:10.5005/jcdp-9-1-113.
- Langton S, Cousin GCS, Plüddemann A, Bankhead CR. Comparison of primary care doctors and dentists in the referral of oral cancer: a systematic review. Br J Oral Maxillofac Surg. 2020;58(8):898–917. doi:10.1016/j.bjoms.2020.06.009.
- Policy statement on the role of dentistry in the treatment of sleep related breathing disorders. American Dental Association. Updated 2019. https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/oral-health-topics/ada_2019_policy_role_of_dentistry_sleep_related_breathing_disorders.pdf?rev=a6b7d4ff667c4325bd1cc402882e0235&hash=1FF15BB2D17D9EA639120DBB78D660E3. Accessed January 6, 2023.
- Policies and recommendations on diet and nutrition. American Dental Association. Updated 2016. https://www.ada.org/about/governance/current-policies#dietnutrition. Accessed January 6, 2023.
- Cancer (head and neck). American Dental Association. Updated September 30, 2022. https://www.ada.org/resources/research/science-and-research-institute/oral-health-topics/cancer-head-and-neck. Accessed January 6, 2023.
- Garvin J Dentists, dental students among providers now authorized to administer COVID-19 vaccine nationwide. American Dental Association. March 12, 2021. https://www.ada.org/publications/ada-news/2021/march/dentists-dental-students-among-providers-now-authorized-to-administer-covid-19-vaccine-nationwide#.Y7h5qyu4CGU.link. Accessed Jan. 6, 2023.
- McNeely J, Wright S, Matthews AG, et al. Substance-use screening and interventions in dental practices: survey of practice-based research network dentists regarding current practices, policies and barriers. J Am Dent Assoc. 2013;144(6):627–638. doi:10.14219/jada.archive.2013.0174. PMID: 23729460; PMCID: PMC3699308.
- American Dental Association. Controlled substance education requirement for DEA registration. Frequently asked questions. Revised April 10 2023. https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/practice/legal-and-regulatory/faq_mate-act.pdf?rev=2d62d028e6cf49869624d1cfa4e442c3&hash=A7D5EB01BC19DA0ADC5968E336996DA5. Accessed May 24, 2023.
- Department of Consumer Affairs. Dental Board of California. Continuing education requirements for renewal of license or permit. https://www.dbc.ca.gov/licensees/continuing_education.shtml. Accessed May 24, 2023.
- National Institute on Drug Abuse. Screening tools and prevention. validated screening tools. https://nida.nih.gov/nidamed-medical-health-professionals/screening-tools-prevention. Updated 2019-01-19. Accessed August 12, 2022.
- Substance Abuse and Mental Health Services Administration. Medications for substance use disorders. April 2023. https://www.samhsa.gov/medications-substance-use-disorders. Accessed May 29, 2023.
- Substance Abuse and Mental Health Services Administration. Screening brief intervention and referral to treatment (SBIRT) in behavioral health. April, 2011. https://www.samhsa.gov/sites/default/files/sbirtwhitepaper_0.pdf. Accessed May 25, 2023.
- Frost H, Campbell P, Maxwell M, et al. Effectiveness of motivational interviewing on adult behaviour change in health and social care settings: a systematic review of reviews. PLoS One. 2018;13(10):e0204890. doi:10.1371/journal.pone.0204890. PMID: 30335780; PMCID: PMC6193639.
- Building rapport with patients: OARS communication skills. Rockville, MD: Agency for Healthcare Research and Quality; 2018. https://www.ahrq.gov/evidencenow/tools/oars-model.html. Accessed January 8, 2023.
- Grant S, Smart R. Expert views on state-level naloxone access laws: a qualitative analysis of an online modified-Delphi process. Harm Reduct J. 2022;19(1):64. doi:10.1186/s12954-022-00645-1. PMID: 35676719; PMCID: PMC9175531.
- Food and Drug Administration. FDA approves first over-the-counter naloxone nasal spray. https://www.fda.gov/news-events/press-announcements/fda-approves-first-over-counter-naloxone-nasal-spray. Published March 29, 2023. Accessed May 22, 2023.
- Overdose prevention initiative. California Department of Public Health; 2022. www.cdph.ca.gov/Programs/CCDPHP/sapb/Pages/Naloxone.aspx. Accessed August 12, 2022.
- Find harm reduction services near you. National Harm Reduction Coalition. https://harmreduction.org/resource-center/harm-reduction-near-you/. Accessed August 12, 2022.
- Goodchild JH, Donaldson M, Malamed SF. Should naloxone be considered an essential medication in dental emergency kits? Gen Dent. 2020;68(3):14–17. PMID: 32348238.
- U.S. Department of Health and Human Services. Centers for Disease Control and Prevention. Preventing an opioid overdose. https://www.cdc.gov/drugoverdose/pdf/patients/Preventing-an-Opioid-Overdose-Tip-Card-a.pdf.
- Pitułaj A, Kiejna A, Dominiak M. Negative synergy of mental disorders and oral diseases versus general health. Dent Med Probl. 2019;56(2):197–201. doi:10.17219/dmp/105253. PMID: 31099501.
- Behavioral health and services treatment locator. Substance Abuse And Mental Health Services Administration; 2022. https://findtreatment.samhsa.gov/. Accessed August 12, 2022.
- Wellness Program. California Dental Association. https://www.cda.org/Wellness-Program. Accessed January 13, 2023.
- Oral health, mental health and substance use treatment: a framework for increased coordination and integration. Center for Excellence for Integrated Health Solutions, National Council for Mental Wellbeing; 2021.