

ABSTRACT
Background
Kabuki Syndrome is a rare genetic alteration of autosomal origin, known for five characteristics called Niikawa’s Pentad: skeletal abnormalities, short stature, mild to moderate intellectual and developmental disabilities, facial dysmorphism, dermatoglyphic alterations, and postnatal growth deficiency.
Case description
The present report aimed to highlight the main oral manifestations of Kabuki Syndrome in a nine-year-old patient, emphasizing the importance of a correct diagnosis and multidisciplinary care.
Continuing Education Credit Available
The practice worksheet is available online in the supplementary material tab for this article. A CDA Continuing Education quiz is online for this article: https://www.cdapresents360.com/learn/catalog/view/20.
Introduction
Discovered in Japan in 1981, Kabuki Syndrome (SK, Niikawa–Kuroki Syndrome, Kabuki Make-up Syndrome) is a rare genetic alteration of autosomal origin. Its manifestations include distinctive craniofacial features such as inferior lateral palpebral eversion, arched eyebrows, depressed nasal tip, and recurved ears. The Kabuki Syndrome received this name because the facial features of the affected patient resembled the actors in Kabuki – traditional Japanese theater. Studies show that this syndrome has no predominance by ethnicity, heredity, or gender.Citation1–4
Independently, Niikawa and Kuroki made the first transcriptions of the syndrome in 1981, pointing out the five characteristics known as the Niikawa Pattern: skeletal abnormalities, short stature, mild to moderate intellectual and developmental disabilities, facial dysmorphism, dermatoglyphic abnormalities, postnatal growth deficiency, microcephaly. Other manifestations may include: gastrointestinal, oral, and renal alterations, cardiac malformations, hearing loss, and susceptibility to infections.Citation1–4
Among the most prevalent alterations are the dysmorphic face, 100%; skeletal anomalies, 92%; dermatoglyphic alterations, 93%; mild to moderate intellectual and developmental disabilities, 92%; postnatal growth retardation, 83%.Citation5
The syndrome’s characteristics are related to genetic mutations of the KMT2D and KDM6A genes, first named MLL2 or MLL4, which occur in 50% to 80% of cases. This etiology was described only 30 years after the discovery of the disease.Citation2,Citation6,Citation7
The estimated prevalence in Japan is 1:32,000 individuals.Citation2,Citation3 The estimated prevalence in Australia and New Zealand is at least 1:86,000.Citation8 In Colombia, 8 cases have been reported, but the official number of diagnosed patients is still unknown.Citation2
Oral manifestations are commonly found in Kabuki Syndrome (68% of cases), and the main cited include: ogival palate, cleft lip and palate, supernumerary teeth, posterior crossbite, ectopic first permanent molars, delayed dental eruption pattern, spaced teeth tapered dental elements and hypodontia.
Microdontia, enamel hypoplasia, dental twinning and fusion, and prominent upper incisors have also been reported.Citation9–12
The present report aimed to present the main oral manifestations of Kabuki Syndrome in a nine-year-old patient, highlighting the importance of a correct diagnosis and multidisciplinary care.
Case Report
A female patient aged 09 years and 10 months was diagnosed with Kabuki Syndrome through a genetic sequencing exam at 9 months. During a program to help children with disabilities from low-income families in Guapimirim city in the Rio de Janeiro State, Brazil. The patient was examined for her oral and clinical characteristics.
Initially, an anamnesis was performed with the child and the mother, who reported the absence of complications during the gestational period, and that the birth occurred 36 weeks after a placental abruption. The mother also informed that the patient such as heart disease, kidney problems, low immunity, scoliosis, and a malformation in the feet, which compromised mobility and required the use of a wheelchair. In addition, no other cases of Kabuki Syndrome have been reported in the child’s family. Next, the patient’s intra- and extraoral conditions were examined a panoramic X-ray was requested as a complement.
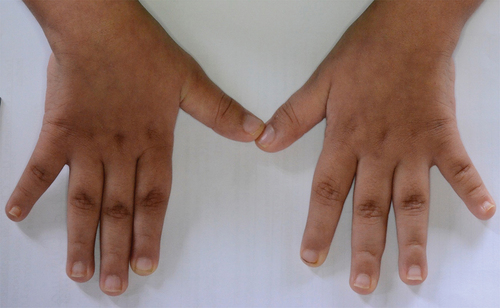
The extraoral examination showed arched eyebrows with an oblique groove, long eyelashes, prominent and recurved ears, and a nose with a wide base and flattened tip (), in addition to a shortened fifth finger (). On intraoral examination, the patient showed a cleft palate, a small “v- shaped” maxillary dental arch, an ogival palate, bilateral posterior crossbite, a diastema, and missing lateral incisors (). A total of 8 maxillary and 11 mandibular teeth were already erupted (3, B, 5, 8, 9, 12, J, 14, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 30) (. Intense accumulation of dental biofilm was evidenced, revealing poor oral hygiene quality ().
Figure 1. Intra and extraoral images: (a) frontal; (b) right side of the face; (c) left side of the face; (d) maxillary teeth; and (e) mandibular teeth.

Figure 2. Right and left hand.
Radiographic findings included 5 unerupted teeth (2, 4, 6, 13, 15) and agenesis of teeth 7, 10, and 11. In the mandibular arch, there were 3 unerupted elements (18, 29, 31), a gyro version of the right and left canines, and taurodontia of elements 20, 21, 28, and 29 ().
Figure 3. Panoramic radiography.
The intraoral examination did not show any carious lesions, but it was possible to observe gingivitis and bacterial plaque in some elements. The patient had the habit of sucking the thumb until the age of 6, which may explain the presence of an anterior open bite. Due to the motor limitations, the parents are responsible for the patient’s oral hygiene.
According to the caregivers, the patient is allergic to chocolate, pork meat, shrimp, and lactose. However, the patient does not have an interest in sweet food, such as candies, juice with sugar, and others, presenting a healthy diet.
Due to the patient’s oral condition, the treatment started with prophylaxis to control plaque and gingivitis, and a periodic follow-up was indicated. Due to the maxillary atresia, and the palatine disjunction, an orthodontic appliance and later closing of the anterior open bite were considered. Weekly follow-up was performed in order to evaluate the patient’s psychological and motor condition. Oral hygiene instructions for the caregiver were also given and encouragement was given regarding the importance of dental treatment to improve the patient’s quality of life.
Discussion
Kabuki syndrome is diagnosed by clustering clinical facial, oral, skeletal, and dermatoglyphic features, growth deficiency, and intellectual disability. Etiologically related to this condition, syndromic patients present heterozygous alterations in KMT2D (13/15, 86.7%) AND KDM6A (2/15, 13.3%) genes that are involved in epigenetic regulation.Citation13 Because she presented all these syndromic features, the patient underwent a genetic sequencing exam that confirmed a mutation in the KMT2D gene, also known as MLL2, confirming the diagnosis of Kabuki Syndrome.
A study of 110 individuals diagnosed with Kabuki Syndrome showed that 81/110 affected individuals (74%) have mutations in the MLL2 gene.Citation14 This result is corroborated by another study that showed alterations in the same gene in 45/62 patients with the syndrome.Citation15 Although these mutations can not be considered pathognomonic for diagnosing the syndrome, these findings have directed the current studies.
The patient in the present case presented the classic craniofacial features described by Niikawa et al.Citation1 and Kuroki et al.Citation4 which are determinants for the diagnosis, such as arched eyebrows, long and curved eyelashes, depressed nasal tip, prominent ears, and short fifth finger as demonstrated in previous reports.Citation10,Citation12,Citation16–18 A study conducted with fourteen Chinese patients genetically diagnosed with Kabuki Syndrome, with ages ranging from 8 months to 11 years, reported that 100% of the patients had arched eyebrows, long eyelashes, external ear deformities, and ogival palate. Delayed motor or language development was observed in 75% of the patients.Citation19
Dental alterations have been described in more than 60% of the cases, and in prominence are the deep and ogival palate, malocclusion (the most observed is the posterior crossbite), short dental arch, microdontia, and hypodontia. Other oral manifestations found in patients were cleft lip or palate, conoid teeth, and screwdriver-shaped incisors.Citation9–12,Citation17 Following patterns reported in the literature, the patient has an ogival palate, cleft palate, short dental arch, and posterior crossbite.
Studies reveal that the most frequently missing teeth in patients affected by the syndrome are maxillary lateral incisors and mandibular central incisors. In the present case, besides the agenesis of the maxillary lateral incisors, the absence of the left maxillary canine was also noted, which is little reported in the literature.Citation9
Other manifestations frequently reported are the predisposition to infections, affecting 60% of the patients, and cardiac problems, present in about 42% of the syndromic patients, being the ventricular septal defect the most common anomaly.Citation1,Citation4 Other frequent cardiac alterations in carriers of the syndrome include aortic coarctation, bicuspid aorta, tetralogy of Fallot, and atrial septal defect.Citation12,Citation18 The patient described has heart disease and low immunity, presenting recurrent episodes of infections.
Because of a malformation of the feet and scoliosis, the patient is a wheelchair user. The patient also presents a shortened fifth finger which is a characteristic of the syndrome. The literature also reports skeletal, ophthalmological, gastrointestinal, and urogenital problems, recurrent infections in childhood, and anomalies of the central nervous system have also been reported.Citation16
Conclusion
The present case report presented the classic features of Kabuki Syndrome in a child without any suspicion during the gestational period. Although rare and with an etiology still not completely understood, its diagnosis is not difficult since facial and oral alterations are characteristic of the syndrome. In this context, the role of the dental surgeon in multidisciplinary teams is highlighted for the correct identification of cases since the facial and intra-oral examinations are decisive for the conclusion of the diagnosis. More specific genetic exams and intrauterine diagnoses need to evolve for earlier detection.
Supplemental Material
Download MS Word (22.6 KB)Disclosure Statement
No potential conflict of interest was reported by the author(s).
Funding
Supported by grants from the Fundação Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de Janeiro (FAPERJ) and Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazilian Governmental Institutions.
Supplemental Material
Supplemental data for this article can be accessed online at https://doi.org/10.1080/19424396.2023.2249028
Additional information
Notes on contributors
Amanda A. Marques
Amanda A. Marques, DDs, is a Specialist in Endodontics at IPPEO Institute.
Sabrina R. Ribeiro
Sabrina Rocha Ribeiro, is a specialist in Orthodontics, specialist in Collective Health and Master in Dentistry from the Methodist University of São Paulo.
Sabrina de C. Brasil
Sabrina de C. Brasil, PhD in Endodontics, UNESA. Professor of the Postgraduate Program in Dentistry, UNIGRANRIO
Flávio R. F. Alves
Flávio R. F. Alves, General Coordinator of the Graduate Program in Dentistry at the University of Grande Rio (Master and Doctorate). PhD in Biological Sciences (Microbiology) from the Federal University of Rio de Janeiro, UFRJ.
References
- Niikawa N, Matsuura N, Fukushima Y, Ohsawa T, Kajii T. Kabuki make-up syndrome: a syndrome of mental retardation, unusual facies, large and protruding ears, and postnatal growth deficiency. J Pediatr. 1981;99(4):565–4. doi:10.1016/S0022-3476(81)80255-7.
- Aristizábal E, Diaz-Ordóñez L, Candelo E, Pachajoa H. A novel intronic KMT2D variant as a cause of Kabuki syndrome: a case report. Appl Clin Genet. 2021;14:409–416. doi:10.2147/TACG.S317723.
- Boniel S, Szymańska K, Śmigiel R, Szczałuba K. Kabuki syndrome-clinical review with molecular aspects. Genes (Basel). 2021;12(4):468. doi:10.3390/genes12040468.
- Kuroki Y, Suzuki Y, Chiyo H, Hata A, Matsui I. A new malformation syndrome of long palpebral fissures, large ears, depressed nasal tip, and skeletal anomalies associated with postnatal dwarfism and mental retardation. J Pedatr. 1981;69(5):99–570. doi:10.1016/S0022-3476(81)80256-9.
- Niikawa N, Kuroki Y, Kajii T, et al. Kabuki make-up (Niikawa-Kuroki) syndrome: a study of 62 patients. Am J Med Genet. 1988;31(3):565–589. doi:10.1002/ajmg.1320310312.
- Bögershausen N, Gatinois V, Riehmer V, et al. Mutation update for Kabuki syndrome genes KMT2D and KDM6A and further delineation of X-Linked Kabuki syndrome subtype 2. Hum Mutat. 2016;37(9):847–864. doi:10.1002/humu.23026.
- Bokinni Y. Kabuki syndrome revisited. J Hum Genet. 2012;57(4):223–227. doi:10.1038/jhg.2012.28.
- White SM, Thompson EM, Kidd A, et al. Growth, behavior, and clinical findings in 27 patients with Kabuki (Niikawa-Kuroki) syndrome. Am J Med Genet A. 2004;127A(2):118–127. doi:10.1002/ajmg.a.20674.
- Porntaveetus T, Abid MF, Theerapanon T, et al. Expanding the oro-dental and mutational spectra of Kabuki syndrome and expression of KMT2D and KDM6A in human tooth germs. Int J Biol Sci. 2018;14(4):381–389. doi:10.7150/ijbs.23517.
- Tuna EB, Marşan G, Gençay K, Seymen F. Craniofacial and dental characteristics of Kabuki syndrome: nine years cephalometric follow-up. J Clin Pediatr Dent. 2012 Summer;36(4):393–400. doi:10.17796/jcpd.36.4.u021164272805116.
- Sattur A, Deshmukh PK, Abrahim L, Naikmasur VG. Kabuki make-up syndrome – a case report with electromyographic study. J ClinDiagn Res. 2014;8(11):ZD03–ZD06. doi:10.7860/JCDR/2014/9804.5122.
- Santos BM, Ribeiro RR, Stuani AS, Silva FWGP, Queiroz AM. Kabuki make- up (Niikawa-Kuroki) syndrome: dental and craniofacial findings in a Brazilian child. Braz Dent J. 2006;17(3):249–254. doi:10.1590/S0103-64402006000300014.
- Di Candia F, Fontana P, Paglia P, et al. Clinical heterogeneity of Kabuki syndrome in a cohort of Italian patients and review of the literature. Eur J Pediatr. 2022;181(1):171–187. doi:10.1007/s00431-021-04108-w.
- Hannibal MC, Buckingham KJ, Ng SB, et al. Spectrum of MLL2 (ALR) mutations in 110 cases of Kabuki syndrome. Am J Med Genet A. 2011;155(7):1511–1516. doi:10.1002/ajmg.a.34074.
- Micale L, Augello B, Fusco C, et al. Mutation spectrum of MLL2 in a cohort of Kabuki syndrome patients. Orphanet J Rare Dis. 2011;6(1):1–8. doi:10.1186/1750-1172-6-38.
- Dupont J, Dias P, Medeira A, Santos H, Cordeiro I. Síndrome de Kabuki: Caracterização de 16 doentes portugueses. Acta Pediátrica Portuguesa. 2010;41:86–91.
- Rocha CT, Peixoto ITA, Fernandes PM, Torres CP, de Queiroz AM. Dental findings in Kabuki make-up syndrome: a case report. Spec Care Dentist. 2008;28(2):53–57. doi:10.1111/j.1754-4505.2008.00011.x.
- Santos A. Características orais e craniofaciais da Síndrome de Kabuki: relato de um caso. Revista de Ciências Médicas e Biológicas. 2013;12(3):385–388. doi:10.9771/cmbio.v12i3.8147.
- Wang Y, Li N, Su Z, et al. The phenotypic spectrum of Kabuki syndrome in patients of Chinese descent: a case series. Am J Med Genet. 2019;182(4):640–651. doi:10.1002/ajmg.a.61467.