

ABSTRACT
Background
The periodontal probe is an essential instrument designed for the purposes of recording clinical periodontal data. As such, accurate periodontal measurements remain a critical factor in providing individualized care to patients. The purpose of this study is to determine the compatibility and accuracy of three different periodontal probes on a periodontal typodont model.
Materials and Methods
Forty-one D3, D4, and DH students were randomly selected to perform a 6-point pocket depth measurement on the mandibular teeth of a previously verified periodontal typodont mounted on a manikin. Each measurement site was outlined with black marking on the tooth to facilitate consistent reproducibility in periodontal probe placement and angulation.
Results
Probing depth measurements between the UNC-15, PCP-126, and Disposable i-PAK® periodontal probe rendered an excellent equivalency (ICC = 0.960) with narrow CI (0.947, 0.971). There is significant difference among these three instruments in their capability to replicate the manufacturer’s suggested probing depth on the periodontal typodont (p < .001). The UNC-15 probe was the most accurate, followed by PCP-126, with the Disposable i-PAK® being the least accurate.
Conclusions
This study demonstrated that the UNC-15, PCP-126, and Disposable i-PAK® yielded equivalent results when measuring probing depths on a periodontal typodont. Furthermore, the UNC-15 was most accurate in its ability to replicate the manufacturer’s suggested pocket depth on the periodontal typodont.
Practical Implications
This study emphasizes the importance in consistency of periodontal probe types in the dental practice.
Introduction
Periodontal disease remains a major public health problem due to its global prevalence with consequences including tooth loss, impaired function, concerns with esthetics, diminished quality of life, and plausible negative impact on general health.Citation1 As such, the early prevention, detection, and treatment of periodontal disease remains a priority for oral healthcare professionals. Periodontal charting is a critical part of the comprehensive periodontal assessment of patients in the dental setting. An important component of charting is the assessment of periodontal probing depths and bleeding on probing, which indicates the level of disease activity and inflammation. Furthermore, clinical attachment levels and recession indicate the current attachment level of the patient and is used in part for periodontal diagnosis and treatment planning.Citation2 The periodontal probe is an essential instrument designed for the purposes of recording clinical periodontal data. Currently, varying diameter, material, graduation markings, and lengths remain some of the observed variabilities that exist among different clinically available periodontal probes. Due to a lack of standardized ISO probes and techniques, we suspect this may lead to measurement variability within the parameters of clinical charting.Citation3 Therefore, accurate periodontal charting utilizing a periodontal probe for detection of clinical parameters remains a critical factor in providing individualized care to patients.Citation4 The purpose of this study is to evaluate the interchangeability and accuracy of three commonly utilized periodontal probe types using a previously verified periodontal typodont.
Several studies have aimed to understand the variation among different generations of periodontal probes when measuring a patient’s clinical attachment loss (CAL), pocket depths (PD), and gingival height (GH). A comparative study by Birte Holtfreter et al. concluded that variation in measurements among different types of manual periodontal probe instruments exists. This particular study aimed to quantify and analyze differences among three different types of manual periodontal probes – PCP-11 (3-3-3-2 mm markings), PCP-2 (2 mm markings), and the PCPUNC-15 (1 mm markings) periodontal probes. Results revealed that pocket depth varied significantly (p < .05) among the three instruments. Such differences in the pocket depth measurement make it appropriate to consider the variation in measurements when using different manual periodontal probes.Citation5
However, other studies such as those conducted by L. Mayfield, et al. reviewed periodontal probe precision between manual and electronic periodontal probes. A comparison was drawn between the manual Hu-Friedy LL-20 probe, Vivacare TPS plastic manual probe, the Vine Valley electronic pressure controlled probe, and the electronic Peri Probe Comp. Results showed that both the manual Hu-Friedy and the electronic Peri Probe Comp recorded deeper pocket depths in contrast to that of the TPS and Vine Valley probe. The main findings of the study concluded that among the four different periodontal probes, the manual instruments displayed the lowest degree of variation as compared to that of the electronic periodontal probes.Citation6
While some studies suggest that variation among manual periodontal probes was lower in comparison to electronic probes, others found that pocket depth and clinical attachment loss measurements can vary with different manual periodontal probes. An in-vitro study by E. Buduneli, et al. assessed accuracy and reproducibility between two manual periodontal probes- the WHO probe (markings that begin at lengths of 3.5, 5.5, 8.5 and 11.5 mm with a 0.5 mm diameter ball at the tip) and the Williams probe (1 mm markings, up to a length of 10 mm) in regards to PD and CAL. Results showed a statistically significant difference (p < .002) between the two manual probes. Findings from the study suggest that the WHO probe possessed superior reproducibility in comparison to the Williams probe. Clinical applications of the study show that the deformation coefficient of the probe material – whether they be metal or plastic material – should be similar to that of the gingival pocket. The study further suggests the significance of calibrating probes as having similar deformation coefficients to the gingival pocket depth may be necessary to test the intra- and inter-examination differences in probing with different periodontal probes.Citation7
Past evidence does not understate the variety of measurements that result from differences in instrument material, markings, and length. Therefore, discrepancies in measurements and thus discrepancies in diagnoses are bound to occur due to a lack of unification of periodontal probe types. By conducting an in-vitro study on a periodontally representative typodont model using three widely utilized manual periodontal probes – the I-PAK Sterile® 3-in-1 (Disposable i-PAK®), UNC-15 (North Carolina), and the PCP-126 (Marquis) periodontal probe – we hope to determine interchangeability as well as accuracy of these three instruments within the clinical setting. We hypothesized that equivalency among the probes would not exist, and that the UNC15 periodontal probe would yield the most accurate measurements on the periodontal typodont.
Methods and Materials
An in-vitro study was carried out by a total of forty-one participants consisting of a combination of twenty-three third year dental students, sixteen fourth year dental students, and two graduating dental hygiene students. Subjects were randomly selected according to consent and availability on the clinic floor. The Institutional Review Board determined that the study does not meet the definitions of human subject research (IRB #5220297).
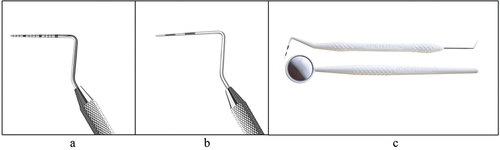
A validated educational research typodont (NISSIN 500HPRO) () was selected to serve as the study’s in-vitro model due to its realistic effects of bone loss, attachment loss, and pocket depths ranging from 4 mm to 10 mm as provided by the manufacturer’s reference probing chart.Citation8,Citation9 The typodont was mounted on a manikin and assembled to a clinical operatory chair in the predoctoral clinic floor under standardized conditions as displayed in . In addition, the periodontal typodont was calibrated in order to minimize the risk of examiner error from the placement and angulation of the periodontal probe. Six surfaces of all teeth (DF, F, MF, ML, L, DL) were outlined with black marking in accordance with the manufacturer’s provided probing chart. provides a visual of the manufactured probing depths ranging from 4 mm to 10 mm. The North Carolina probe (1 mm marking), Marquis probe (3-6-9-12 mm marking), and Disposable i-PAK® (3-6-9-12 mm marking) probe () were placed in a randomized order for each examiner.Citation10–12 A new Disposable i-PAK® was provided to each examiner.
Figure 1. a). Periodontal typodont replicating effects of periodontal disease with pocket depths ranging from 4 mm to 10 mm. b). Lateral perspective of the periodontal typodont mounted on a manikin and assembled on the clinic operatory chair. c). Coronal perspective of the periodontal typodont mounted on a manikin and assembled on the clinic operatory chair. d). Periodontal typodont with uncovered maxillary gingiva to display the construction and variability of probing depths.
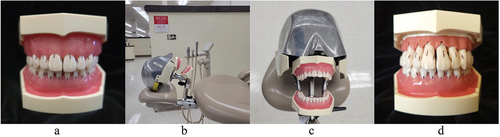
Figure 2. a). Image of North Carolina periodontal probe (UNC-15). b). Image of marquis periodontal probe (PCP126), with 3-6-9-12 mm markings. c). Image of Disposable i-PAK® periodontal probe, with 3-6-9-12 mm markings.
Participants were unaware of the purpose of the study. Prior to examination, the examiner was first instructed to utilize the North Carolina periodontal probe to measure Mesio-Facial surface of #9 and was simultaneously disclosed the according manufactured depth (8 mm). With knowledge of the manufacturer-imparted measurement for MF #9, intent was to have the examiner understand the amount of pressure to be applied on the typodont. Each participant was then instructed through a standardized verbal script to complete a six-point probing depth examination of the mandibular arch (from tooth #18 to #31) on the periodontal typodont. Each examiner performed the study with the three periodontal instruments in one sitting.
Results
A total of forty-one participants probed six surfaces of fourteen mandibular teeth. The sequence was repeated three times with each participant in accordance with a randomized order of the North Carolina, Marquis, and Disposable i-PAK® instruments. Data collection occurred over the course of three weeks and yielded a total of ten thousand, three hundred and thirty-two pocket depth measurements. All tests of significance were two-sided, with the significance level set at α = 0.05.
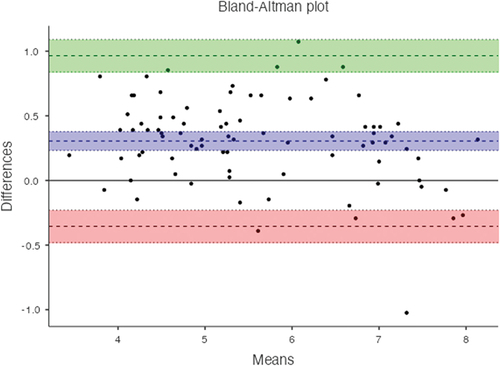
To analyze reliability, the Bland-Altman analysis was utilized in order to observe pairwise comparisons of the North Carolina, Marquis, and Disposable i-PAK® periodontal probes. Three pairwise comparisons were made: North Carolina versus Marquis, Marquis versus Disposable i-PAK®, and North Carolina versus Disposable i-PAK® periodontal probes in respectively. Notably, there was no consistent bias of one approach over the other as evidenced by equal scattering of values above and below 0. Quantitively, the two-way fixed analysis yielded an Intraclass Correlation Coefficient of 0.960, which indicated excellent reliability for the average probing depths of the North Carolina, Marquis, and Disposable i-PAK® to resemble one another.
Figure 3. Bland-Altman plot comparing the North Carolina periodontal probe versus Marquis periodontal probe.
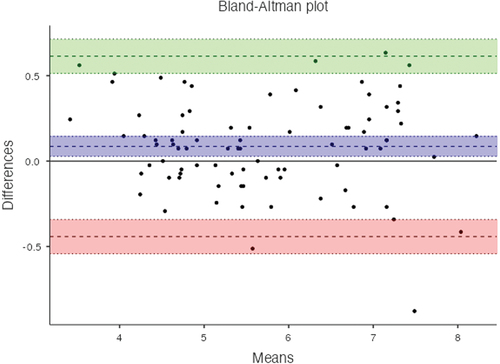
Figure 4. Bland-Altman plot comparing the Marquis periodontal probe versus Disposable i-PAK® periodontal probe.
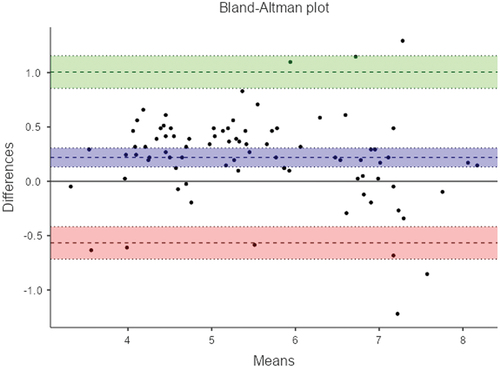
Figure 5. Bland-Altman plot comparing the North Carolina periodontal probe versus Disposable i-PAK® periodontal probe.
There was a statistically significant difference among the three instruments in their ability to replicate the manufacturer’s suggested probing depth on the periodontal typodont, as evidenced by the Repeated Measures ANOVA analysis (p < .001, ). The North Carolina periodontal probe (1 mm markings) performed the most accurate, followed by the Marquis periodontal probe (3-6-9-12 mm markings), with the Disposable i-PAK® (3-6-9-12 mm) periodontal probe performing the least accurate.
Table 1. Repeated measures of ANOVA to test within subjects effects.
The Estimated Marginal Means Technique by type of periodontal probe revealed quantitative differences from the mean probing depth difference, with UNC-15 deviating the least in comparison to PCP126 and Disposable i-PAK® ().
Table 2. Estimated marginal means by type of periodontal probe.
Discussion
The manual periodontal probe is an indispensable instrument in evaluating the periodontal status of patients.Citation13 A wide range of periodontal probes have been created and modified throughout the history of dentistry, for an equally vast spectrum of purposes.Citation14 Because a variety of different periodontal probes exists, reproducible pocket depth measurement is of utmost importance in order to prevent miscommunication among providers. Several studies have attempted to observe the differences in inter-examiner reliability between manual periodontal probes.Citation5,Citation7
Based on the results of this study, we rejected our hypothesis on equivalency. The North Carolina, Marquis, and Disposable i-PAK® periodontal probes were compatible with one other. Furthermore, we supported our hypothesis on accuracy, where the North Carolina periodontal probe was most accurate in replicating the manufacturer’s probing depth, while the Disposable i-PAK® periodontal probe yielded the least accurate pocket depth measurement. The North Carolina periodontal probe may have performed better due to the greater detailed in markings as compared to that on the Marquis and Disposable i-PAK® periodontal probes. It is crucial to note the vast difference in material and weight between the Disposable i-PAK® periodontal probe and the North Carolina as well as Marquis periodontal probe, which may explain why the Disposable i-PAK® periodontal probe performed the worst in terms of the examiner’s ability to match the manufacturer’s suggested probing depth. The flexible material and light weight of the instrument may have prevented the examiner from performing with the usual memory involving tactile experience. There is no current literature supporting the inter-examiner reliability and accuracy between the North Carolina, Marquis, and Disposable i-PAK® periodontal probes, but several studies posed contraindicatory results regarding reliability between several periodontal probes.Citation15
A major strength of the study was the use of a previously validated periodontal typodont model to evaluate equivalency and accuracy of three different periodontal probes in-vitro. The periodontal typodont, mounted in the clinical setting, offered an additional advantage of providing a realistic environment for examiners. Various past studies have constructed their own measurement devices or typodonts to collect data. For example, aluminum blocks with 30 holes of predetermined measurements were created for participants to measure probing depth measurements. This particular in-vitro model provided statistically significant results but may not provide the adequate immersive conditions to replicate the clinical setting such as the variability of periodontal conditions.Citation16
The findings of this study open many avenues for future research studies regarding the reliability and accuracy of periodontal probes. It is crucial to keep in mind several potential areas of improvement to further improve the methodology of the research design. First, one limitation that may have existed is potential error in measurement via the anterior or posterior location of the site.Citation17 However, negligible changes between the relationship between site and performance were observed in our study. Second, the three periodontal probe measurements were conducted consecutively for each participant. Although each order of the probes was randomized, factors such as participant burnout may have had an impact on the results.
Third, the diameter of the periodontal probe may have an influence on the outcome of the measurement depth.Citation18,Citation19 The diameter of the Disposable i-PAK® periodontal probe is marginally larger than that of the North Carolina and Marquis periodontal probe. The diameter of the North Carolina periodontal probe presents as thicker and straighter, whereas that of the Marquis is thinner and slightly more tapered. These differences in shape and size as well as weight, may have affected readings. Fourth, it is important to consider the background of the participants. As most of our study participants consisted of third year dental students, experience levels with utilizing the various periodontal probes may have had an effect on outcomes.
Future research may need to consider the variability of human tissue if pursuing an in-vitro methodology, as the range between healing or inflamed gingiva can significantly alter the reproducibility of investigated sites.Citation20,Citation21 Approximately 1 mm of probing depth error can be acknowledged with each measurement to account for differences in the clinician’s periodontal probing technique. Furthermore, intrabony defects are not always detected radiographically – but if they are, may be underestimated due to the two dimensional nature of radiographs.Citation22 To account for the varied topography of human tissue, it is highly recommended to consider multiple probing measurements in future research methods.
Conclusion
Within the limitations of the study, we conclude that the three types of periodontal probes are compatible with each other, and that the North Carolina periodontal probe is the most accurate in its ability to replicate the manufacturer’s suggested pocket depth on the periodontal typodont.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
Notes on contributors
Rachel Koh
Rachel Koh BA is a dental student at the Loma Linda University School of Dentistry.
Sharon Lee
Sharon Lee BA is a dental student at the Loma Linda University School of Dentistry.
Udochukwu Oyoyo
Udochukwu Oyoyo MPH is an assistant professor at Loma Linda University School of Dentistry.
So Ran Kwon
So Ran Kwon DDS, MS, PhD, MS is a professor and director of the student research program at Loma Linda University School of Dentistry.
Nima D. Sarmast
Nima D. Sarmast, DDS, MS, MPH, MSD is an assistant professor of periodontics at Loma Linda University School of Dentistry.
References
- Papapanou PN, Sanz M, Buduneli N, et al. Periodontitis: consensus report of workgroup 2 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin Periodontol. 2018;45(Suppl 20):S162–6. doi:10.1111/jcpe.12946.
- AAP. The American Academy of Periodontology Glossary of Periodontal Terms. Chicago: The American Academy of Periodontology; 2018.
- Chapple ILC, Mealey BL, Van Dyke TE, et al. Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: consensus report of workgroup 1 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Periodontol. 2018;89(Suppl 1):S74–S84. doi:10.1002/JPER.17-0719.
- Lindhe J, Socransky SS, Nyman S, Haffajee AD, Westfelt E. “Critical probing depths” in periodontal therapy. J Clin Periodontol. 1982;9(4):323–336. doi:10.1111/j.1600-051X.1982.tb02099.x.
- Holtfreter B, Alte D, Schwahn C, Desvarieux M, Kocher T. Effects of different manual periodontal probes on periodontal measurements. J Clin Periodontol. 2012;39(11):1032–1041. doi:10.1111/j.1600-051X.2012.01941.x.
- Mayfield L, Bratthall G, AttStröm R. Periodontal probe precision using 4 different periodontal probes. J Clin Periodontol. 1996;23(2):76–82. doi:10.1111/j.1600-051X.1996.tb00538.x.
- Buduneli E, Aksoy O, Köse T, Atilla G. Accuracy and reproducibility of two manual periodontal probes. J Clin Periodontol. 2004;31(10):815–819. doi:10.1111/j.1600-051x.2004.00560.x.
- Sunaga M, Minabe M, Inagaki K, Kinoshita A. Effectiveness of a specially designed dental model for training, evaluation, and standardization of pocket probing. J Dent Educ. 2016;80(12):1430–1439. doi:10.1002/j.0022-0337.2016.80.12.tb06230.x.
- Harada Y, Sunaga M, Takeuchi Y, et al. Standardization of examiners using a dental model for pocket probe training: adequacy of evaluation with a model and standard accuracy rate of skilled examiners. J Med Dent Sci. 2021;68:49–54.
- PCPUNC156 - Probe UNC #UNC15 hdl #6 Qulix 1-2-3 … .15. n.d. HuFriedy Group.
- PCP126 - Probe #12 hdl #6 Qulix 3-6-9-12. n.d. HuFriedy Group.
- MDSupplies. AD Surgical I-PAK Sterile 3-in-1 Oral Exam Packs Surgical D002-009-P. n.d. MDSupplies.
- Listgarten MA. Periodontal probing: what does it mean? J Clin Periodontol. 1980;7(3):165–176. doi:10.1111/j.1600-051X.1980.tb01960.x.
- Hefti AF. Periodontal probing. Crit Rev Oral Biol Med. 1997;8(3):336–356. doi:10.1177/10454411970080030601.
- Al Shayeb KN, Turner W, Gillam DG. In-vitro accuracy and reproducibility evaluation of probing depth measurements of selected periodontal probes. Saudi Dent J. 2014;26(1):19–24. doi:10.1016/j.sdentj.2013.11.001.
- Heym R, Krause S, Hennessen T, Pitchika V, Ern C, Hickel R. A new model for training in periodontal examinations using manikins. J Dent Educ. 2016;80(12):1422–1429. doi:10.1002/j.0022-0337.2016.80.12.tb06229.x.
- Andrade RFS, Espinoza M, Macedo EA, Espinoza J, Cruz E. Intra- and inter-examiner reproducibility of manual probing depth. Braz Oral Res. 2012;26(1):57–63. doi:10.1590/S1806-83242012000100010.
- Atassi R, Newman HB, Bulman J. Probe tine diameter and probing depth. J Clin Periodontol. 1992;19(5):301–304. doi:10.1111/j.1600-051X.1992.tb00648.x.
- Garnick JJ, Silverstein L. Periodontal probing: probe tip diameter. J Periodontol. 2000;71(1):96–103. doi:10.1902/jop.2000.71.1.96.
- Badersten A, Nilvéus R, Egelberg J. Reproducibility of probing attachment level measurements. J Clin Periodontol. 1984;11(7):475–485. doi:10.1111/j.1600-051X.1984.tb01347.x.
- Lang NP, Wetzel AC, Stich H, Caffesse RG. Histologic probe penetration in healthy and inflamed peri-implant tissues. Clin Oral Implants Res. 1994;5(4):191–201. doi:10.1034/j.1600-0501.1994.050401.x.
- Eickholz P, Hausmann E. Accuracy of radiographic assessment of interproximal bone loss in intrabony defects using linear measurements. Eur J Oral Sci. 2000;108(1):70–73. doi:10.1034/j.1600-0722.2000.00729.x.