

ABSTRACT
Background
Advances in 3D printing are making a significant impact on the future of dentistry. This study evaluated whether the difference in volumetric change of objects printed with the Anycubic and SprintRay 3D printers was clinically or statistically significant.
Methods
A maxillary left 1st premolar typodont tooth was scanned with a TRIOSTM intra-oral scanner and then printed using AnycubicTM (N = 20) and SprintRayTM (N = 20) 3D printers for a total of 40 printed objects. The printed premolars were scanned with a TRIOSTM scanner after complete cure (T1 or baseline). Subsequent scans were made at 3-, 6-, 24-, and 48-hour after the T1 scan. The scans at different time intervals from each scanner were superimposed, and the volumetric change among the scans was analyzed and recorded using a matching software (Geomagic WRAP®). The volumetric changes at different time intervals for both printers were analyzed using a Mann-Whitney U test α = 0.05.
Results
The mean volumetric change of the printed teeth from both AnycubicTM (−1.28 mm3) and SprintRayTM (−3.06 mm3) were minimal and not statistically significantly different from each other at any time points (p > .05).
Conclusions
Both printers showed no clinically significant volumetric change. Although not a statistically significant difference, the AnycubicTM printed objects demonstrated greater stability in comparison to the SprintRayTM printed objects.
Practical Implications
This study showed that clinically acceptable accuracy/outcomes of printed objects can be achieved with a lower-cost option, such as an AnycubicTM 3D printer.
Introduction
Dentistry is continually expanding its reach to provide high-quality care to patients. 3D printing has grown in popularity,Citation1 and has been increasingly integrated into dental practices and orthodontic offices in order to produce quality patient casts used to fabricate dental appliances.Citation2,Citation3 This decision is driven by the recognition that 3D printing offers remarkable efficiency, reproducibility, and cost-effective production of fast and precise outcomes.Citation4 Using digital scans of the mouth also substitutes the need for dental impressions, thus eliminating the traditional usage of dental stone “pour-ups”.Citation5–8 Orthodontists are using 3D materials to make occlusal splints, night guards, indirect bonding trays and much more.Citation2,Citation5,Citation9–11 When using 3D printers, accurate replication of anatomical structures is crucial, as this ensures the ability for 3D printed material to possess the specific mechanical properties necessary for prosthodontic and orthodontic device preparation.Citation12 In contrast to traditional stone models, 3D printed casts have demonstrated comparable, if not superior, mechanical properties and accuracy when utilized as diagnostic tools.Citation12,Citation13 Determining the accuracy of individual 3D printed dental casts compared to dental stone casts, and verifying 3D printers’ ability to deliver highly precise results is paramount for any dental professional as they decide whether or not to incorporate 3D printing technology into their practice.Citation13
At present, the Graduate Orthodontic Clinic at Loma Linda University School of Dentistry utilizes two different 3D printers, Anycubic Photon Mono XTM and SprintRay Pro 95STM Citation14,Citation15 to produce patients’ maxillary and mandibular casts. While both printers possess different features, their notable distinction lies in their respective price. The higher-end option, SprintRay Pro 95STM, is priced at $8,995.00, whereas the lower-end alternative, Anycubic Photon Mono XTM, is priced at $529.00. Consequently, there is an ongoing debate regarding the suitability of these machines and materials for use in contemporary orthodontic practice.Citation10
The Sprintray Pro 95STM is a DLP (Digital Light Processing) printer designed for dental use which uses UV light in the 405 nm range to cure photosensitive resin into the desired object.Citation15–17 The Anycubic MonoXTM is an LCD Liquid-Crystal Display) printer designed for hobbyists and crafters which uses an array of LEDs to shine UV light in the 405 nm range through a monochrome LCD panel to cure photosensitive resin into the desired object.Citation14,Citation16,Citation18
The advantages of DLP based printers are its use of a proven and mature technology, the UV projector is higher intensity than LCD printers which lowers the overall print time and is compatible with a larger range of resins that require the higher intensity to cure properly in a reasonable period of time.Citation19 They can handle more viscous and custom resins with specific properties (e.g. Ceramic Crown resin). Generally, the smaller the printed object the more accurate the DLP products.Citation16 Disadvantages of DLP printers include being more prone to intensity discrepancies between the center and outer edges of the print bed, thus causing X-Y dimensional inconsistencies and possible keystone problems causing distortion. These issues are more apparent in less expensive DLP printers.
The main advantage of LCD printers is the starting price (Anycubic MonoXTM is less than 1/10th the price of the Sprintray Pro 95STM and resins are ¼ to ½ the price).Citation14,Citation15,Citation19 The print quality and X-Y accuracy is fixed and dependent on the density of pixels in the LCD panel (MonoXTM is a 4k resolution LCD panel and newer models can get up to 8k LCD panel).Citation19,Citation20 LCD printers can print larger models with no difference in quality from smaller models.
A disadvantage of LCD printers is that the LCD panels need to be replaced more often than a DLP projector. Monochrome LCD panels last longer than full color panels (the MonoXTM uses a monochrome panel).Citation16 The print speed is usually slower than DLP, although the Anycubic MonoXTM is only about 10% slower than the Sprintray Pro95STM.Citation14,Citation15
As mentioned, one of the main disadvantages of 3D printing is that the final model often shrinks to some degree due to temperature changes and plastic material characteristics. The volumetric change due to resin shrinkage can cause distortion of the model, potentially affecting the clinical fit of the dental appliances fabricated on that model.Citation21 Not all printers and materials have the same shrinkage rate, so determining which printer/material combination offers the most dimensional stability can have significant clinical implications.Citation13
The purpose of this study was to evaluate and compare the volumetric change of printed objects from Anycubic Photon Mono XTM and SprintRay Pro 95STM 3D printers, as these are the two printers currently used in the Loma Linda University Graduate Orthodontic clinic. The null hypothesis stated that there would be no statistically significant difference in volumetric change of the printed objects from either 3D printer.
Materials and Methods
A maxillary left 1st premolar typodont tooth (ANA-4, Frasaco, Germany) was scanned using a TRIOSTM intraoral scanner (3shape TRIOS 3 Wired, Denmark) and exported as an STL (Standard Triangle Language) file. The STL file of the scanned premolar was used for the printing of the experimental objects. To determine a proper sample size for this project, a 2% volumetric difference was used in this study as the indicator of clinical significance. Assuming a 2% standard deviation around a 2% volumetric change, 17 samples per printer were required in order to achieve an 80% power to detect 2% volumetric difference at α = 0.05.To increase the power of the study, 20 objects were printed per printer, for a total of 40 printed objects. The printing steps, program/software and the material used for printing for both printers are shown in .
Table 1. The program/software and materials used for printing experimental objects.
Each printed tooth used was embedded with its own single thick post support at the bottom of the model that held it in a vertical orientation perpendicular to the build platform (root at the bottom, crown at the top). Each model was washed in 99% IPA for 5 minutes in a dirty initial bath before a second clean bath for 5 minutes. The models printed on the Sprintray Pro95TM post-cured in a Sprintray Pro Cure 1 unit using the preset settings for the Sprintray Model White 2 resin which is 50C for 30 min. The Anycubic prints were post-cured in the Sprintray Pro Cure 1 unit at 30C for 6 minutes.
The printed objects were individually numbered and then scanned using a TRIOSTM scanner in chronological order according to the numbers assigned. TRIOSTM scanners were used to scan the printed objects because five scanners were available, allowing all objects to be scanned faster. This allowed less time to pass between scans, reducing variability in the measured volume for each printed tooth. This was considered the baseline (T1) scan. Subsequent scans of each individual printed object were made, again in chronological order, at 3 hrs (T2), 6 hrs (T3), 24 hrs (T4), and 48 hrs (T5) after the T1 scan. The STL files of all scans were exported to a matching software (Geomagic WRAP®, 3D Systems, Rock Hill, SC), for volumetric change analysis.
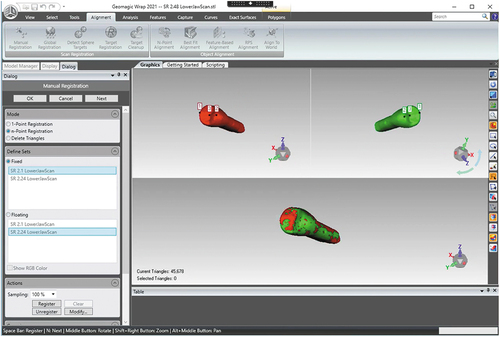
In the Geomagic WRAP® software, the T1 – T5 scans of each printed tooth were superimposed (shown in ) and aligned using the “Best Fit” tool to ensure the greatest accuracy possible. To guarantee precision in every scan, three reference points were selected on the T1 tooth, and the same trio of points was designated in the corresponding location on the T2-T5 teeth to ensure their alignment. After aligning all five scans, the superimposed images (T1 – T5) of each printed tooth were trimmed at the same point at the apical end of the tooth, coronal to the post used for printing. Since each trim was done manually, it was virtually impossible for the trimming to be at the exact same location on each printed tooth. This accounted for the discrepancies observed in the total volumes among the teeth. This study, however, specifically evaluated the change in volume over time, and not the total volume of each tooth. The volumes at all time intervals (T1 – T5) of each printed tooth were analyzed and the volumetric changes from T1 to other time intervals (T2 – T5) were calculated and recorded.
Figure 1. Superimposing two scans in Geomagic Wrap® software.
After all scans were complete and each volume was recorded, a Mann-Whitney U test at a = 0.05 was used to determine volumetric change for each data set using Jamovi v2.3.2.
Results
After data analysis, the average volumetric change in AnycubicTM 3D printed teeth was −1.28 mm3, and the average volumetric change in SprintRayTM printed teeth was −3.06 mm3. These volumetric changes were minimal and were not statistically significantly different from each other at any time points (p > .05). See below for specific p-values.
Table 2. Comparison of mean volumetric change from T1 at different time intervals between objects printed from AnycubicTM and SprintRayTM.
The average volume recorded at each time interval for each printer is displayed as a line graph in . The average volumetric change and standard deviation in mm3 at each time interval compared to the initial scan were also calculated, and can be seen in . The rate of volumetric change in mm3/hr from T2-T5 can be found in .
Figure 2. Volumetric change in mm3 over time.
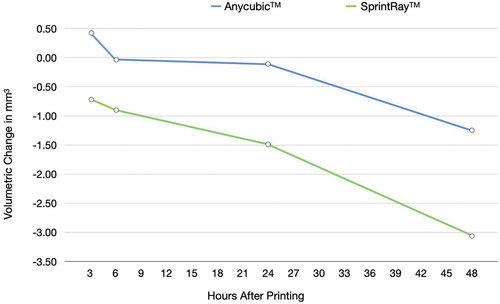
Table 3. Rate of volumetric change at different time intervals between objects printed from AnycubicTM and SprintRayTM.
Discussion
3D printing technology is used widely in dentistry and is a rapidly expanding market continuously introducing enhanced systems and solutions.Citation1 Numerous clinics are electing to adopt 3D printing technology as part of their transition to a fully digital workflow due to the remarkable efficiency, reproducibility, and cost-effective production of fast and precise outcomes.Citation5
Accurate replication of anatomical structures is crucial when creating casts using 3D printers. This ensures the ability to possess specific mechanical properties necessary for prosthodontic and orthodontic device preparation.Citation12 When compared to traditional stone models, 3D printed casts have demonstrated comparable, if not superior mechanical properties and accuracy when utilized as diagnostic tools.Citation12,Citation13 While 3D printing as a whole could be compared to dental stones, it is crucial to assess the accuracy of individual 3D printer technologies due to the inherent variations in their ability to deliver highly precise results.Citation22 Determining whether AnycubicTM and SprintRayTM 3D printers can produce such precise results will greatly impact their use at the Loma Linda University Graduate School of Orthodontics.
These two specific printers were chosen for this study because they are the two printers currently in use at the Loma Linda University Graduate Orthodontic clinic. SprintrayTM printers are currently being used in dental practices and labs around the world and they directly compete with and rival more expensive alternatives. The alternative brands are rapidly improving, but SprintrayTM strives to keep up with current trends and works with many third-party resin manufacturers to remain competitive. AnycubicTM is one example of inexpensive printers that proves that resin-based printers can produce high-quality results while remaining affordable.
The average volumetric change of the 3D printed objects was examined statistically and clinically to determine whether the change was significant or not. The final volumetric change of AnycubicTM teeth was −1.28 mm3, while the final volumetric change of SprintRayTM printed teeth was −3.06 mm3. Statistical analysis results showed that the p-value comparing the final volumetric change of AnycubicTM and SprintRayTM printed teeth was 0.242. A p-value greater than 0.05 confirmed no statistical significance in volumetric change between the two printers. The average volumetric change of the 3D printed teeth was compared to similar studies,Citation7,Citation10,Citation12,Citation13,Citation22 and it was determined that the volumetric change observed was not clinically significant.
During this study, AnycubicTM teeth showed minimal expansion during the first six hours before they started to shrink, and afterward followed a similar trend to SprintRayTM teeth, as depicted in . The volumetric changes observed from both printers were very low, while the average of AnycubicTM 3D printed teeth was −1.28 mm3, and the average of SprintRayTM printed teeth was −3.06 mm3. This change represents a 0.23% and 0.57% volumetric change, respectively (see ). Therefore, both printers produce clinically acceptable models within 48 hours from printing.Citation7,Citation8,Citation10 Further study is needed to evaluate the rate of volumetric change plateaus.
As is depicted in , the slope indicating the rate of volumetric shrinkage increases over time. The shrinkage rate is greater at 48 hours rather than lower, as initially presumed. In regards to orthodontics, the observed shrinkage in this study is unlikely to have any significant clinical impact. Nevertheless, the ability to ascertain the long-term dimensional stability and rate of shrinkage of 3D printed objects/models could prove to be clinically advantageous for other dental disciplines.Citation5,Citation21
Based on the results of our longitudinal cohort study, we accepted our null hypothesis, as there was no significant difference in volumetric change of printed teeth produced by the two 3D printers. Similar studies conducted by Kim et al. and Nulty have compared the trueness and precision of a number of different 3D printer technologies in a similar fashion.Citation8,Citation23 Although neither study compared AnyCubicTM and SprintrayTM against each other as was done in this study, Kim et al. compared the technologies used by both AnyCubicTM (LCD technology) and SprintrayTM (DLP technology). Nulty related the accuracy of nine 3D printers, and compared the affordability of each printer. Both studies found that there was no significant difference in “trueness” and “precision” among the different printers, supporting the findings of this study.Citation8,Citation23
One of the most important principles in the context of printing models for patients is the necessity for precision in replicating the patient’s actual dentition, ensuring that any subsequent dental appliance fabricated from it fits perfectly in the patient’s mouth. Based on the findings of this study, the quality and dimensional stability of printed objects from both tested printers were not discernibly different. However, this study did not evaluate the advanced features that the more expensive printer offers, which may be of greater value to more experienced users of 3D printers.
Limitations of this study included a limited number of TRIOSTM scanners available in a laboratory setting. Due to the small number of scanners, the first scans (T1) recorded were the “1 hour” initial scan. Another limitation was the speed at which the printed teeth could be scanned. As there were only five researchers scanning 40 teeth at each time interval, it was impossible for all printed objects to be scanned at the exact same time point. Calibration of scanners and printers could have also been a limitation, as the researchers did not have control over when or how often the printers and scanners were calibrated.
Future studies could evaluate other brands and models of 3D printers alongside the printers that were compared in this study, thus providing a wide array of options for dental professionals to choose from. Utilizing different printing materials and analyzing their effect on volumetric stability might also be a consideration for future studies. Recording volumetric change over a longer period of time in order to observe the time point at which shrinkage no longer occurs may also be a future consideration.
Conclusion
Within the limitations of the study, we conclude that printed objects from neither printer showed clinically significant volumetric change. Although not statistically significantly different, AnycubicTM printed objects demonstrated slightly greater volumetric stability in comparison to SprintRayTM printed objects over time despite its substantially lower cost. If our school, or a private dental practice, was seeking to use 3D printed technology in their office, they could reasonably do so with high accuracy and lower cost with the AnycubicTM printer as opposed to the SprintrayTM printer.
Acknowledgment
The authors would like to thank Mr. Seth Myhre for his assistance in printing 3D objects at the Graduate Orthodontic Clinic. The authors would also like to thank Dr. Roberto Savignano for his assistance with the Geomagic programs.
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Sarah Batarseh
Sarah Batarseh, BS, is a dental student at Loma Linda University School of Dentistry.
Nathan Goldsberry
Nate Goldsberry, BA, is a dental student at Loma Linda University School of Dentistry.
Carina Handysides
Carina Handysides, BS, is a dental student at Loma Linda University School of Dentistry.
Layla Nemat-Bakhsh
Layla Nemat-bakhsh, BS, is a dental student at Loma Linda University School of Dentistry.
Caleb Valenzuela
Caleb Valenzuela, BS, is a dental student at Loma Linda University School of Dentistry.
Joseph Caruso
Joseph Caruso, DDS, MS, MPH, is a professor in Orthodontics and Dentofacial Orthopedics.
Kitichai Rungcharasaeng
Kitichai Rungcharassaeng, DDS, MS, is in Private Practice, Redlands, CA.
Udochukwu Oyoyo
Udochukwu Oyoyo, MPH, is an assistant professor in dental education services at Loma Linda University School of Dentistry.
References
- van Noort R. The future of dental devices is digital. Dent Mater. 2011;28(1):3–6. doi:10.1016/j.dental.2011.10.014.
- Dawood A, Marti BM, Sauret-Jackson V, Darwood A. 3D printing in dentistry. Nat News. 2015;219(11):521–529. doi:10.1038/sj.bdj.2015.914.
- Wesemann C, Muallah J, Mah J, Bumann A. Accuracy and efficiency of full-arch digitalization and 3D printing: a comparison between desktop model scanners, an intraoral scanner, a CBCT model scan, and stereolithographic 3D printing. Quintessence Int. 2017;48(1):41–50. doi:10.3290/j.qi.a37130.
- Paradowska-Stolarz A, Wezgowiec J, Mikulewicz M. Comparison of two chosen 3D printing resins designed for orthodontic use: an in vitro study. MDPI. 2023;16(6):2237. doi:10.3390/ma16062237.
- Pillai S, Upadhyay A, Khayambashi P, et al. Dental 3D-Printing: transferring art from the laboratories to the clinics. MDPI. 2021;13(1):157. doi:10.3390/polym13010157.
- Banjar A, Chen YW, Kostagianni A, et al. Accuracy of 3D printed implant casts versus stone casts: a comparative study in the anterior maxilla. J Prosthodont. 2021;30(9):783–788. doi:10.1111/jopr.13335.
- Leifert M, Leifert MM, Efstratiadis SS, et al. Comparison of space analysis evaluations with digital models and plaster dental casts. Am J Orthod Dentofacial Orthop. 2009;136(1):e16.1–e16.4. doi:10.1016/j.ajodo.2008.11.019.
- Kim JH, Pinhata-Baptista O, Ayres A, et al. Accuracy comparison among 3D-printing technologies to produce dental models. MDPI. 2022;12(17):8425. doi:10.3390/app12178425.
- Dantagnan C-A, François P, Le Goff S, Attal J-P, Dursun E. Degree of conversion of 3D printing resins used for splints and orthodontic appliances under different postpolymerization conditions - clinical oral investigations. Clin Oral Investi. 2023;27(6):2935–2942. doi:10.1007/s00784-023-04893-8.
- Favero CS, English JD, Cozad BE, et al. Effect of print layer height and printer type on the accuracy of 3-dimensional printed orthodontic models. Am J Orthod Dentofacial Orthop. 2017;152(4):557–565. doi:10.1016/j.ajodo.2017.06.012.
- Gupta DK, Tuli A, Jain A. 3D printed material application in orthodontics. Mater Today. 2020;28(3):1635–1642. doi:10.1016/j.matpr.2020.04.856.
- Czajkowska M, Walejewska E, Zadrożny Ł, et al. Comparison of dental stone models and their 3D printed acrylic replicas for the accuracy and mechanical properties. MDPI. 2020;13(18):4066. doi:10.3390/ma13184066.
- Ellakany P, Al-Harbi F, Tantawi ME, Mohsen C. Evaluation of the accuracy of digital and 3D-printed casts compared with conventional stone casts. J Prosthet Dent. 2020;127(3):438–444. doi:10.1016/j.prosdent.2020.08.039.
- Mono X, Anycubic. Anycubic Photon Mono X. ANYCUBIC. 2023.
- Pro 95s, Sprintray. Pro 95s 3D printer. SprintRay store product. 2023.
- Quan H, Zhang T, Xu H, Luo S, Nie J, Zhu X. Photo-curing 3D printing technique and its challenges. Bioact Mater. 2020;5(1):110–115.
- What is DLP 3D printing? LuxCreo; August 25, 2022. https://luxcreo.com/what-is-dlp-3d-printing-lc/#:~:text=The%20capabilities%20of%20DLP%20printers,finish%2C%20and%20isotropic%20material%20properties.
- Livienna X. What is a LCD 3D printer? Phrozen Technology; April 5, 2023. https://phrozen3d.com/blogs/guides/what-is-a-lcd-3d-printer#:~:text=Advantages%20of%203D%20LCD%20printer&text=3D%20printing%20with%20the%20LCD,accuracy%20than%20traditional%203D%20printers.
- Tsolakis IA, Papaioannou W, Papadopoulou E, Dalampira M, Tsolakis AI. Comparison in terms of accuracy between DLP and LCD printing technology for dental model printing. Dent J (Basel). 2022;10(10):181.
- Tsolakis IA, Gizani S, Panayi N, Antonopoulos G, Tsolakis AI. Three-dimensional printing technology in orthodontics for dental models: a systematic review. Children. 2022;9(8):1106.
- Ling L, Taremi N, Malyala R. A novel low-shrinkage resin for 3D printing. J Dent. 2022;118:103957. doi:10.1016/j.jdent.2022.103957.
- Rungrojwittayakul O, Kan JY, Shiozaki K, et al. Accuracy of 3D printed models created by two technologies of printers with different designs of model base. J Prosthodont. 2019;29(2):124–128. doi:10.1111/jopr.13107.
- Nulty A. A comparison of trueness and precision of 12 3D printers used in dentistry. BDJ Open. 2022;8(1):14. doi:10.1038/s41405-022-00108-6.