

ABSTRACT
Bruxism is characterized by repetitive clenching or grinding of teeth and jaw muscle activity. It is a complex condition with various factors contributing to its development and can exert abnormal loads on the stomatognathic system.
Aim
This scoping review aimed to explore various aspects of bruxism in children, including its causes, prevalence, diagnosis, and multidisciplinary treatment.
Methods
A comprehensive search was conducted in the PUBMED-MEDLINE database focused on studies published from 2018 to 2023.
Inclusion criteria encompassed
Cross-sectional, longitudinal, comparative studies, and randomized and non-randomized clinical trials published in English. Retained full texts were assessed and excluded if inclusion criteria were not met. Methodological quality was assessed using the Joanna Briggs Institute critical appraisal tools for the different types of studies.
Results
Of 498 initial studies, 26 were selected for full reading and 19 met the inclusion criteria. Most studies were cross-sectional (14 studies) and showed a wide prevalence of sleep bruxism.
Conclusion
This scoping review highlights that bruxism is an important issue in children that should be observed by parents/guardians and evaluated by health professionals. Due to its multifactorial nature, a collaborative approach involving a diverse team of professionals is essential for the effective prevention and treatment of bruxism in pediatric patients.
KEYWORDS:
Introduction
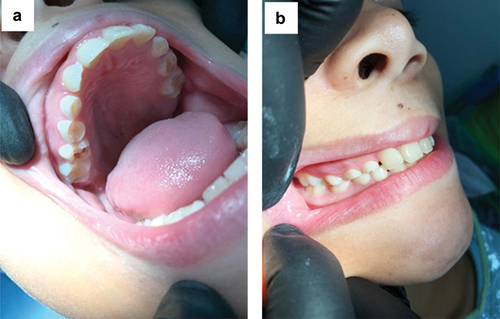
Bruxism is a repetitive masticatory muscle activity involving clenching or grinding teeth or the bracing or thrusting of the mandible.Citation1 It manifests in two circadian phenotypes: sleep bruxism (SB), occurring during sleep, and awake bruxism (AB), observed during wakefulness.Citation2 If left untreated, bruxism can lead to dental damage (), periodontal trauma, muscle hypertrophy, temporomandibular disorders, and pain in the head, facial muscles, or teeth.Citation3,Citation4 Socioeconomic issues like anxiety, depression, and low sleep quality are associated with this parafunctional habit.Citation5–8
Figure 1. Wear in the deciduous dentition in a pediatric patient. (a) occlusal wear in posterior teeth; (b) patient in occlusion showing the wear of the cusps of the deciduous elements.
Bruxism in children is a public health issue, as it can impact their development during this critical period.Citation9 Recent studies have shown an increased prevalence of childhood bruxism, possibly linked to rising anxiety levels and technology usage,Citation10 which were further exacerbated during the COVID-19 pandemic when school closures and excessive technology exposure negatively affected children’s quality of life.Citation8
Scoping reviews are an approach to investigating and providing an overview of the evidence in a variety of fields, including bruxism. They identify key features or factors related to a concept, as a precursor to a systematic review, to identify and analyze knowledge gaps. Scoping reviews are essentially broader and more exploratory in nature compared to systematic reviews.Citation11
Given its multifactorial nature, treating bruxism requires a multidisciplinary approach involving various health care professionals such as pediatric and temporomandibular disorder dentists, pediatricians, psychologists, speech therapists, and physical therapists.Citation12 This study aimed to conduct a scoping review on the etiology, diagnosis, and treatment of bruxism in children.
Materials and Methods
This scoping review was guided by the Johanna Briggs Institute (JBI) Scoping Review Methodology Group.Citation13 This type of study design was chosen because of the broad nature of the research question.Citation11 A quality assessment of the included studies was performed using the critical appraisal tools of the JBI, for cross-sectional, case controls and cohort studies,Citation14 quasi experimental,Citation15 and randomized control trials.Citation16 Each of these check lists contained between eight and 13 items with four possible response categories: “yes,” “no,” “unclear” and “not applicable.” Two reviewers independently assessed the quality of the studies (CA and FA). Differing conclusions were resolved by discussion. An overall score for each study was calculated by summing the number of “yes” responses. A score of ≤ 30% was considered low quality, a score between 31 and 60% was moderate and a score ≥ 61% was high quality. No studies were excluded on the basis of methodological quality.
The main characteristics of the included studies were analyzed descriptively and summarized in a table. It was not possible to perform meta-analyses due to the heterogeneity of the studies.
A systematic search was conducted in the PUBMED-MEDLINE database with the following keywords: “child,” “bruxism,” “etiology,” “diagnosis,” and “treatment.” The inclusion criteria encompassed cross-sectional, longitudinal, comparative studies and randomized or non-randomized clinical trials conducted in children. The search was limited to studies published in English between 2018 and 2023. Specifically, cross-sectional, cohort studies, case-control studies, quasi experimental and randomized clinical trials were included. Case reports, literature and systematic reviews, animal studies, and in vitro studies were excluded to ensure relevance and focus. Additionally, studies involving children with mental or physical disabilities were not considered.
Results
A total of 498 studies were initially found. Among these, 472 studies were excluded based on an assessment of the title and abstract, as they did not meet the inclusion and exclusion criteria. Subsequently, 26 studies were selected for full reading, and ultimately, 19 were included in this scoping review. The characteristics of the included studies and their main results are presented in .
Table 1. Characteristics of the included studies.
Thirteen of the selected studies were conducted in Brazil,Citation3,Citation6–8,Citation17–25 two in Turkey,Citation26,Citation27 and one each in the United States,Citation4 Israel,Citation28 Canada,Citation5 and Africa.Citation29
Among the included studies, 13 were cross-sectional studies,Citation3,Citation4,Citation6,Citation7,Citation17,Citation18,Citation21,Citation23–26,Citation28,Citation29 one was a case-control,Citation20 one was a randomized clinical trial,Citation19 one was on dental treatment,Citation27 one was a prospective longitudinal cohort study,Citation8 one was part of a longitudinal study,Citation5 and one involved clinical and genetic evaluation.Citation22
The age range of the children in the studies varied from 1.5 to 17 years old.Citation3–5,Citation7,Citation8,Citation17–24,Citation26–29 Additionally, two studies included two age groups: one comprising children with primary dentition aged 2 to 5 years old and another group with mixed dentition aged 8 to 10 years old.Citation6,Citation25 Studies have shown that bruxism tends to increase during the child’s initial development and decrease during adolescence and adulthood.Citation5,Citation30 Overall, the included studies did not find a significant statistical difference regarding age.Citation4–6,Citation17–20,Citation22,Citation26,Citation28,Citation29 However, in studies where such differences were observed, they can be explained by factors such as oral habits, lifestyle factors (including sleep duration and chronotype profile), anxiety, and respiratory problems.Citation7,Citation9,Citation24,Citation25
Most of the included studies did not find a significant influence of gender on the prevalence of SB in children.Citation3,Citation4,Citation6,Citation17,Citation18,Citation21,Citation24–26,Citation28,Citation28 However, it is worth noting that some studies suggest the male gender is more susceptible to SB in children,Citation7,Citation23 which could be a potential risk factor.Citation9
In this review, the studies from different countries have reported a prevalence of SB in children ranging from 9.1% to 40.3%.Citation3,Citation4,Citation6,Citation17,Citation18,Citation21–25,Citation28,Citation29 However, two recent studies found an even higher prevalence, with more than 60% of children affected by bruxism.Citation8,Citation26 Furthermore, the prevalence increased to 70% during the COVID-19 pandemic.Citation8
Quality Assessment
Among the cross-sectional studies, only one study that was assessed by the JBI checklist was classified as being of low quality,Citation22 two of moderateCitation23,Citation24 and eleven of high qualityCitation3,Citation4,Citation6,Citation7,Citation17,Citation18,Citation21,Citation25,Citation26,Citation28,Citation29 (see quality score in ). The quasi-experimentalCitation22 study and the randomized controlled trialCitation19 was classified as moderate quality. The case control studyCitation20 and the two cohorts’ studiesCitation5,Citation8 were also classified as moderate quality.
For cross-sectional studies,Citation3,Citation4,Citation6,Citation7,Citation17,Citation18,Citation21–26,Citation28,Citation29 a detailed description of the subjects and the study setting, sufficient coverage of the identified sample or the use of valid methods for identifying bruxism status were generally provided. However, some studiesCitation21–24,Citation29 did not present confounding factors or strategies for dealing with these confounding factors. The quasi-experimentalCitation22 study did not show a control group, a complete follow-up, or an adequate description of the participants who were lost to follow-up. In the randomized controlled trial,Citation19 it was not presented whether the participants and the administration of the treatment were blinded, whether the evaluators were blinded to the results of the treatments, or whether there were reliable measures for follow-up.
For the case-control,Citation20 confounding factors or strategies for dealing with these confounding factors were not presented, as well as whether those involved in collecting data were trained. In the cohort studies,Citation5,Citation8 both had problems with the reliability of the exposure measure, and it was unclear whether the results were measured validly and reliably.
Discussion
The aim of this scoping review was to offer a comprehensive overview of the literature relating to etiology, diagnosis, and treatment of SB and AB.
Etiology
The etiology of bruxism is widely acknowledged as multifactorial, extending beyond the realm of dentistry.Citation2 It is influenced by various factors, including changes in neurotransmitters such as dopamine and a range of biological and psychosocial contributors such as anxiety and personality traits.Citation10,Citation31 Evidence also suggests a hereditary component in SB,Citation26 and specific genetic polymorphisms have been implicated in its development.Citation20 Additionally, associations have been found between bruxism and factors such as malocclusion, nutritional deficiencies, respiratory disorders, allergies, parasitic infections, oral habits, and poor sleep quality.Citation32 Moreover, there may be a genetic predisposition for the co-occurrence of SB and sleep apnea.Citation22,Citation28
Prevalence
In our review, the prevalence of SB showed a high variability between studies, which can be attributed to various factors, including the absence of standardized diagnostic criteria, methodological differences in assessment tools, cultural disparities of the studied population, and parafunctional habits associated, such as object biting or sucking or biting the lips or cheeks. Similarly, Machado et al.Citation10 in their systematic review demonstrated that studies should employ validated and universal diagnostic criteria to ensure accurate assessment and facilitate comparisons between studies.
Two studiesCitation8,Citation26 showed the highest prevalence rates of SB, 40% and 60%. The first used a questionnaire to assess children in Brazil during the pandemic period and revealed an increase in children’s anxiety levels due to withdrawal from social interaction and excessive use of technology.Citation8 The second used a questionnaire and also included a clinical assessment.Citation26 One issue is the lack of consensus on standardized questionnaires, which can lead to disparate results. In addition, the use of clinical evaluation can also increase the reliability of the study. Consequently, evidence-based studies should employ standardized diagnostic criteria to ensure accurate assessment and facilitate comparisons between studies.Citation26
Some authors have also highlighted the association between socioeconomic factors and SB. For instance, lower socioeconomic status and lower parental education levels have been linked to a higher prevalence of SB.Citation8,Citation23,Citation24
Signs and Symptoms
Children with bruxism may exhibit certain characteristics reported by parents/guardians, including audible tooth grinding or clenching sounds during sleep, headaches, orofacial pain upon waking, and discomfort while chewing or opening the mouth. Clinical signs and symptoms of bruxism can manifest as dental wear facets, fractures in restorations, impressions on the cheek mucosa and tongue caused by teeth, tenderness, and pain in the temporal and masseter muscles, head and teeth, which can be evaluated through clinical examinations in children.Citation4,Citation20
Clinical features in children with SB or AB include clenching or grinding of teeth. Oral habits as nails/objects biting, sucking or biting the lips, cheeks, and tongue, finger sucking, and pacifier useCitation4,Citation7,Citation18,Citation19,Citation22 are also observed.
The literature provides evidence for various factors associated with bruxism in children, including emotional factors,Citation23 anxiety,Citation5 higher levels of cortisol, disruption of biological rhythm,Citation19 nocturnal agitation, nightmares,Citation6 and low sleep quality.Citation7
Diagnosis
An established international consensus provides classifications for different levels of diagnosis for SB and AB.Citation2 These categories encompass (a) SB or AB based on self-report alone, (b) probable SB or AB based on self-report and clinical inspection, (c) definite SB or AB based on self-report, clinical inspection, and polysomnography (preferably combined with audio/video recordings), and (d) definite SB or AB based on self-report, clinical inspection, and electromyography (preferably combined with ecological momentary assessment/experience sampling methodology).
Early identification of bruxism is crucial for promptly recognizing clinical features that may pose risks, such as tooth wear, dental damage, fractures, jaw muscle fatigue, and pain.Citation4 In the present review, different diagnostic criteria for SB were utilized across the studies, including the Sleep Disturbance Scale for Children,Citation4,Citation17 Children’s Sleep Habits Questionnaire,Citation22 criteria from the American Association of Sleep Medicine,Citation6,Citation8,Citation23,Citation24,Citation29 Sleep Behavior Questionnaire,Citation18 and Pittsburgh Sleep Quality Index.Citation7 Some studies also employed self-questionnaires.Citation20,Citation21,Citation25,Citation28
Polysomnography is considered the gold standard for diagnosing and assessing SB.Citation3,Citation6,Citation10,Citation19,Citation28 This method is a recognized test preferably combined with audio and video recordings in which the activities of the masticatory muscles are quantified for data from the electromyographic (EMG) channels of the masticatory muscles.Citation33 However, it is challenging to conduct as it requires patients to sleep in a clinic and is an expensive technique.Citation28 Consequently, most studies relied the diagnosis on parent/guardian reports of signs and symptoms during sleep or upon awakening, particularly tooth-grinding sounds during sleep.Citation3,Citation4,Citation6,Citation7,Citation17,Citation18,Citation20,Citation21,Citation23–26,Citation28,Citation29 Another interesting diagnostic alternative is the BiteStrip®, a wireless device that is a precise tool for evaluating the excessive nocturnal activity of the masticatory muscles. It is designed for home use and records signal from forces exceeding an individual’s maximum bite force.Citation10,Citation27
Treatment
Treating bruxism remains a challenge, primarily due to its multifactorial etiology. Various approaches have been explored as alternatives for treating bruxism in children. Acupuncture, a technique that stimulates specific points to promote muscle relaxation, pain relief, and reduction of inflammation, has been utilized.Citation19 Photobiomodulation is a treatment for tissue repair and regeneration that uses low-level laser light therapy (LLLT) and was used on specific acupuncture points as an alternative treatment in the study by Salgueiro et al.Citation19 It was also used because it is a painless technique, improving the children’s acceptance and reported successful outcomes in children with SB, including a reduction in bite forces and decreased reports of headaches.Citation19 Another study that evaluated hard and soft occlusal splints showed that soft occlusal splints could reduce the pain caused by nocturnal bruxism in the muscles and temporomandibular joint.Citation27 However, this method has limitations, especially in children, as it depends on the patient’s cooperation.Citation19
Parents’ and guardians’ involvement and attention during treatment are crucial for the success of any therapy for bruxism in children. Establishing a calm bedtime routine, creating a suitable sleep environment, avoiding electronic games before bedtime, and engaging in daily physical activities with the child are essential supportive measures in the treatment process.Citation7,Citation8
Conclusion
Based on the analyzed literature, some conclusions can be drawn: (a) bruxism is an important issue in children that should be observed by parents/guardians and evaluated by health professionals; (b) early diagnosis and treatment by dental practitioners are crucial to prevent or minimize further damage to the stomatognathic system; (c) bruxism has a multifactorial etiology, necessitating a transdisciplinary approach involving parents/caregivers and different health care professionals for a comprehensive treatment; (d) early intervention is essential to alleviating symptoms, protecting dental structures, and improving the overall well-being of children with bruxism; and (e) continued research and evidence-based practices are necessary to enhance the understanding and treatment of bruxism in children.
Abbrevations
| SB | = | sleep bruxism |
| AB | = | awake bruxism |
| JBI | = | Johanna Briggs Institute |
| LLLT | = | Low-level laser light therapy |
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Cristine da Silva Furtado Amaral
Cristine Amaral – study design, search strategy, data extraction, and article writing.
Jennifer Guedes Sobral
Jennifer Sobral – study design and first-draft writing.
Flávia Cariús Tesch Ferreira Alves
Flávia Alves – figures, writing-reviewing, and editing.
Claudia Maria Pereira
Claudia Pereira – first-draft writing, writing-reviewing, and editing.
Flávio Rodrigues Ferreira Alves
Flávio Alves – first-draft writing, writing-reviewing, and editing.
References
- Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013;40(1):2–8. doi:10.1111/joor.12011.
- Lobbezoo F, Ahlberg J, Raphael KG, et al. International consensus on the assessment of bruxism: report of a work in progress. J Oral Rehabil. 2018;45(11):837–844. doi:10.1111/joor.12663.
- Brancher LC, Cademartori MG, Jansen K, et al. Social, emotional, and behavioral problems and parent-reported sleep bruxism in schoolchildren. J Am Dent Assoc. 2020;151(5):327–333. doi:10.1016/j.adaj.2020.01.025.
- Oh JS, Zaghi S, Ghodousi N, et al. Determinants of probable sleep bruxism in a pediatric mixed dentition population: a multivariate analysis of mouth vs. nasal breathing, tongue mobility, and tonsil size. Sleep Med. 2021;77:7–13. doi:10.1016/j.sleep.2020.11.007.
- Rostami EG, Touchette E, Huynh N, et al. High separation anxiety trajectory in early childhood is a risk factor for sleep bruxism at age 7. Sleep. 2020 13;43(7):zsz317. doi:10.1093/sleep/zsz317.
- Ribeiro MB, Manfredini D, Tavares-Silva C, et al. Association of possible sleep bruxism in children with different chronotype profiles and sleep characteristics. Chronobiol Int. 2018;35(5):633–642. doi:10.1080/07420528.2018.1424176.
- Soares JP, Giacomin A, Cardoso M, Serra-Negra JM, Bolan M. Association of gender, oral habits, and poor sleep quality with possible sleep bruxism in schoolchildren. Braz Oral Res. 2020;16(34):e019. doi:10.1590/1807-3107bor-2020.vol34.0019.
- Lima LCM, Leal TR, Araújo LJS, et al. Impact of the COVID-19 pandemic on sleep quality and sleep bruxism in children eight to ten years of age. Braz Oral Res. 2022;36:e046. doi:10.1590/1807-3107bor-2022.vol36.0046.
- Guo H, Wang T, Niu X, et al. The risk factors related to bruxism in children: a systematic review and meta-analysis. Arch Oral Biol. 2018;86:18–34. doi:10.1016/j.archoralbio.2017.11.004.
- Machado E, Dal-Fabbro C, Cunali PA, Kaiser OB. Prevalence of sleep bruxism in children: a systematic review. Dental Press J Orthod. 2014;19(6):54–61. doi:10.1590/2176-9451.19.6.054-061.oar.
- Munn Z, Peters MDJ, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(143):2–7. doi:10.1186/s12874-018-0611-x.
- Lobbezoo F, van der Zaag J, van Selms MKA, Hamburger HL, Naeije M. Principles for the management of bruxism. J Oral Rehabil. 2008;35(7):509–523. doi:10.1111/j.1365-2842.2008.01853.x.
- Peters MDJ, Godfrey C, McInerney P, et al. Best practice guidance and reporting items for the development of scoping review protocols. JBI Evidence Sythesis. 2022;20(4):953–968. doi:10.11124/JBIES-21-00242.
- Moola S, Munn Z, Tufanaru C, et al. Chapter 7: systematic reviews of etiology and risk. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. https://synthesismanual/jbi.global.
- Tufanaru C, Munn Z, Aromataris E, Campbell J, Hopp L. Chapter 3: systematic reviews of effectiveness. In: Aromataris E, Munn Z, eds. JBI Manual for Evidence Synthesis. JBI; 2020. https://synthesismanual.jbi.global.
- Barker TH, Stone JC, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synth. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430.
- Leal TR, Lima LCM, Perazzo MF, et al. Influence of the practice of sports, sleep disorders and habits on probable sleep bruxism in children with mixed dentition. Oral Dis. 2023;29(1):211–219. doi:10.1111/odi.13917.
- Duarte J, Souza JF, Cavalcante-Leão B, Todero SRT, Ferreira FM, Calixto Fraiz FC. Association of possible sleep bruxism with daytime oral habits and sleep behavior in schoolchildren. Cranio. 2021;39(5):372–378. doi:10.1080/08869634.2019.1661113.
- Salgueiro MCC, Kobayashi FY, Motta LJ, et al. Effect of photobiomodulation on salivary cortisol, masticatory muscle strength, and clinical signs in children with sleep bruxism: a randomized controlled trial. Photobiomodul Photomed Laser Surg. 2021;39(1):23–29. doi:10.1089/photob.2019.4778.
- Küchler EC, Arid J, Palinkas M, et al. Genetic polymorphisms in ACTN3 contribute to the etiology of bruxism in children. J Clin Pediatr Dent. 2020;44(3):180–184. doi:10.17796/1053-4625-44.3.8.
- Lins RM, Cavalcanti MC, Mello Figueiredo LM, Heimer MV, Dos Santos-Junior VE. Probable sleep bruxism in children and its relationship with harmful oral habits, type of crossbite and oral breathing. J Clin Pediatr Dent. 2020;44(1):66–69. doi:10.17796/1053-4625-44.1.12.
- Vieira AR, Scariot R, Gerber JT, et al. Bruxism throughout the lifespan and variants in MMP2, MMP9 and COMT. Pers Med. 2020 27;10(2):44. doi:10.3390/jpm10020044.
- Alves CL, Fagundes DM, Soares PBF, Ferreira MC. Knowledge of parents/caregivers about bruxism in children treated at the pediatric dentistry clinic. Sleep Sci. 2019;12(3):185–9. doi:10.5935/1984-0063.20190083.
- Bach SL, Moreira FP, Goettems ML, et al. Salivary cortisol levels and biological rhythm in schoolchildren with sleep bruxism. Sleep Med. 2019;54:48–52. doi:10.1016/j.sleep.2018.09.031.
- Massignan C, Alencar NA, Soares JP, et al. Poor sleep quality and prevalence of probable sleep bruxism in primary and mixed dentitions: a cross-sectional study. Sleep Breath. 2019;23(3):935–41. doi:10.1007/s11325-018-1771-y.
- Topaloglu-Ak A, Kurtulmus H, Basa S, Sabuncuoglu O. Can sleeping habits be associated with sleep bruxism, temporomandibular disorders and dental caries among children? Dent Med Probl. 2022;59(4):517–522. doi:10.17219/dmp/150615.
- Kolcakoglu K, Dogan S, Oz FT, Aydınbelge M. A comparison of hard and soft occlusal splints for the treatment of nocturnal bruxism in children using the BiteSTRIP®. Clin Pediatr Dent. 2022;46(3):219–224. doi:10.17796/1053-4625-46.3.8.
- Blumer S, Eli I, Kaminsky-Kurtz S, Shreiber-Fridman Y, Dolev E, Emodi-Perlman A. Sleep-related breathing disorders in children – red flags in pediatric care. J Clin Med. 2022;2211(19):5570. doi:10.3390/jcm11195570.
- Rubin PF, Erez A, Peretz B, Birenboim-Wilensky R, Winocur E. Prevalence of bruxism and temporomandibular disorders among orphans in southeast Uganda: a gender and age comparison. Cranio. 2018;36(4):243–249. doi:10.1080/08869634.2017.1331784.
- Manfredini D, Restrepo C, Diaz-Serrano K, Winocur E, Lobbezoo F. Prevalence of sleep bruxism in children: a systematic review of the literature. J Oral Rehabil. 2013;40(8):631–642. doi:10.1111/joor.12069.
- Manfredini D, Serra-Negra J, Carboncini F, Lobbezoo F. Current concepts of bruxism. Int J Prosthodont. 2017;30(5):437–438. doi:10.11607/ijp.5210.
- Barclay NL, Gregory AM. Quantitative genetic research on sleep: a review of normal sleep, sleep disturbances and associated emotional, behavioural, and health-related difficulties. Review Sleep Med Rev. 2013;17(1):29–40. doi:10.1016/j.smrv.2012.01.008.
- Miettinen T, Myllymaa K, Muraja-Murro A, et al. Polysomnographic scoring of sleep bruxism events is accurate even in the absence of video recording but unreliable with EMG-only setups. Sleep Breath. 2020;24(3):893–904. doi:10.1007/s11325-019-01915-2.