

ABSTRACT
The discipline of systems thinking was developed to study and predict outcomes of large multicomponent systems. It provides a lens to examine complex problems, such as global warming or population health. This article applies the basic tenets of systems thinking to the practice of dentistry, looking specifically at patient safety and quality improvement. Using a systems view of the dental office; an argument is made for the development of a quality initiative through the creation of a mechanism for non-discoverable adverse event reporting. This would create a resource for dentists to learn from past adverse events and prevent them from happening again.
Introduction
This article describes systems thinking as it applies to safe care of patients and quality improvement. Through the use of stories, a foundation of system concepts will be built and applied to the health care system. More than that, this article is about dentists and the patients we are privileged to treat.
Dental offices are busy places. Lots of moving parts that interact to produce a result. Managing a dental office is not an easy task. Traditionally, the management of a dental office occurs from top down. The dentist is the captain of the ship. They are trained to the highest level possible and that in itself should prevent any adverse events from happening. This approach has not been entirely effective, since accidents still occur in dental offices. The wrong tooth is extracted, the wrong arch is treated. Perhaps, there is a different way of looking at the workings of a dental office, which might make the dental office safer. This is the question that the discipline of systems thinking embraces. Is there a more comprehensive way of approaching how a dental office functions to improve performance?
What is Systems Thinking
Let’s begin our discussion of systems thinking with the Merrian-Webster definition of a system, which is a regularly interacting or independent group of items forming a unified whole.Citation1 With this definition, we see systems everywhere. The roads and expressways we take to work are a system, the climate is a system and a dental office is a system. Because there are so many moving parts in these examples, they are referred to as complex systems. The prevalence of systems and their importance has led to the creation of the discipline of systems thinking, which looks for ways to approach solving problems involving complex systems. What will the world economy look like 20 years from now or where will climate change have the greatest effect illustrate the scale of systems thinking problems. To understand such complexity, systems thinking has developed a unique vocabulary and diagrams to use as tools in the pursuit of understanding how systems are constructed and behave. Systems thinking also looks to incorporate the variability of human behavior and its effect on the overall system.Citation2–5
Systems thinking started with the work of Bertalanffy in the 1950s, who studied how biologic systems interacted bringing focus to the interaction of the components of the system. His work was termed general systems theory.Citation6 Danielle Meadows further refined the definition of a system as an interconnected set of elements that is coherently organized in a way that achieves something.Citation7 That something is the purpose of the system. In dentistry, that something could be “optimal oral health.”
Systems thinkers examine not only the elements of the system, but how they interact and affect outcomes. Meadows points out that a system is more than the sum of its parts.Citation7 While the least obvious part of a system is often its function or purpose, this is the most important product of the system. Noted for his work in operations research, which was a precursor to systems thinking, Russell Ackoff points out that systems share three characteristics that defines their behavior:
Each part affects the whole.
Each part is necessary, but insufficient for achieving systems aims.
The effect of any part on the system as a whole depends on the behavior of a least one other part.Citation8,Citation9
Using Ackoff’s criteria, what is a system? Grains of sand on a beach are not a system. They do not interact to affect the whole. The aquatic life around coral reefs is a system. Coral reefs are composed of individual parts that interact. Coral reefs provide a habitat for a variety of sea life. The purpose of the coral reef system is to protect coastal areas by reducing the power of the waves hitting the coast.Citation10 At the same time, they provide a crucial source of income for millions of people.Citation11 The second purpose is not as apparent if we limit our examinations to only the elements of the reef. The application of systems thinking attempts to reveal these hidden purposes or unexpected results.
Classically, dentists and other health professionals have been trained to solve problems by looking for direct cause and effect. A affects B equals C is an example of causal thinking. Such a linear approach oversimplifies complex problems. It attempts to reduce the problem to a simple right or wrong, yes or no. A bivalent logic produces two strong opinions, either right or wrong, yes or no.Citation12 This is not how systems work in the real world. For example, the office is busy or it is not. There is traffic on the interstate or not. You are happy or you are not happy. A simple yes or no does not adequately address your state of being. Yes, I feel good, but I am not giddy with happiness. There is traffic, but it is not stop and go. Yes, we have a full schedule, but there is room to see more patients. To fully appreciate the state of a system, a multi-variant logic is needed to fully describe these systems. This is where systems thinking comes in, as it attempts to describe and examine the environmental influences that the problem occurred in.
A simple representation of a systems error could be the following. An emergency patient with gingival swelling is put on the schedule at the end of the day. The dentist asks for a periodontal probe and the assistant must leave the room to get one, as the probe is not on the tray that was brought into the operatory. Using linear thinking, the problem is simply that the instrument was missing from the tray. Solving this problem starts at no probe on the tray. The fix is usually to remind all assistants that an emergency tray requires a periodontal probe, even going so far as to posting pictures of a completed tray with a periodontal probe on it.
If we look at this same scenario from a systems view, what occurred was that an emergency patient was put on the schedule at the end of a busy day. Because of the high volume of patients, an assistant had to create a new tray, while assisting with other patients. In addition, the patient visits were so high that all the periodontal probes were being sterilized. The instrument was not available to put on the tray. The solution this time is totally different than reminding assistants what is the correct tray set-up. Now the solution is to purchase more periodontal probes and have more emergency trays set up and ready for the day. The system affected the outcome. Busy day, not enough periodontal probes and busy dental assistants leading to an unplanned event. Systems thinking looks at how different components interact, which is why it has been described as a holistic theory.Citation13 This is a way of seeing that parts of something are interconnected and can be explained only by reference to the whole. We have all heard the term “holistic medicine.”
Lucian Leape in his iconic commentary “Error in Medicine” in the Journal of the American Medical Association in 1994, became one of the first physicians to see that the systems we practice in affect the quality of care we deliver.Citation14 Dr. Leape looked at the then current safety literature, which demonstrated that 20% of patients in a large hospital (now called a health care system) suffered iatrogenic injuries. Of those injured, 20% died. Leape realized that the physicians in the studies were well trained and at the top of their profession. Yet, there were still unintended adverse events and deaths. He understood that the system in which the physicians practiced was part of the problem. Below are excerpts from Leap’s summary:
Finally, total quality management calls for grassroots participation to identify and develop system modifications to eliminate the underlying failures.
Like total quality management, systems changes to reduce errors require commitment of the organization’s leadership. None of the aforementioned changes will be effective or, for that matter, even possible without support at the highest levels (hospital executives and departmental chiefs) for making safety a major goal of medical practice.
But it is apparent that the most fundamental change that will be needed if hospitals are to make meaningful progress in error reduction is a cultural one. Physicians and nurses need to accept the notion that error is an inevitable accompaniment of the human condition, even among conscientious professionals with high standards. Errors must be accepted as evidence of system flaws, not character flaws. Until and unless that happens, it is unlikely that any substantial progress will be made in reducing medical errors.Citation14
For example, requiring a resident to work a 24-hour shift would certainly put that physician at increased risk to make a mistake.Citation15 Leape encouraged physicians to look at the system and how it affected their ability to make good decisions. Systems thinking is more than just looking at the bigger picture, it is an approach to addressing problems using a specific vocabulary. Unfortunately, this is where the system thinking theorist loses the average health care provider’s interest. Part of this vocabulary is the use of diagrams as a way to visualize patterns within the system.
Causal Diagrams
Let’s begin with our first systems tool, a simple diagram of a causal loop (see ). The line projections are an attempt to capture the dynamic relationships among interacting components of the system. The system diagram attempts to move the observer from “elements interacting” to “how do the elements interact?” Citation16
Figure 1. Casual loop diagram.
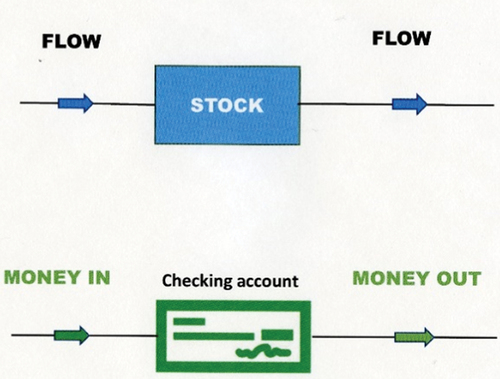
This first diagram depicts the flow of money into a checking account. In system speech, the checking account amount is labeled a “stock,” which is the element of a system that you can see and measure. It is something that has accumulated over time. Recording the behavior of the stock over time plays a large role in system thinking. Your checking account has a history, which can be graphed. We could have substituted water in a bathtub as a stock with water flowing in and out.
Using systems vocabulary, the line with an arrow in is called a “flow.” It shows the passage of something, which could be information, good will or (in our case) money into a checking account. Both stocks and flows can be measured over time and plotted on graphs which are used to observe the function of the system over time. If the checking account flow of money out is greater than the flow in, there will soon be a zero balance. Diagram 1 is a depiction of a causal loop diagram which attempts to visualize how the variables in a system interact.
When a stock grows quickly or is locked to a certain range of quantity, there is likely another factor in play, a modifier to the system. This modifier acts as a control mechanism operating through a feedback loop.
A feedback loop is a closed chain of causal connections from a stock, through a set of decisions or rules or physical laws or actions that are dependent on the level of the stock and back again through a flow to change the stock.Citation17
In , the new line represents the action of adding a modifier, an interest-bearing account from a bank. The interest paid is determined by the amount of dollars in the checking account.
Figure 2. Feedback loop.
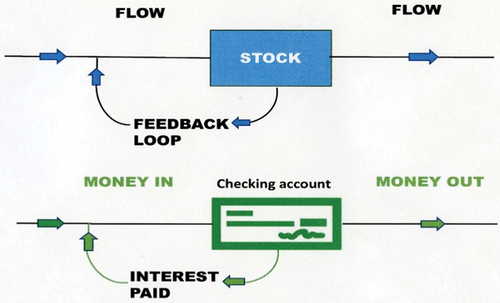
The flow from the interest paid goes back to the account and increases the balance. This is a feedback loop, which is one of the most powerful concepts in system thinking. There are two different forms of feedback loops: the amplifying/reinforcing feedback loop that generates more stock than was there previously, and the stabilizing/balancing feedback loop that decreases the stock from its current level. Interest paid is an example of a reinforcing loop, while an example of a balancing loop would be a thermostat. As the temperature of the room changes, the thermostat will signal devices to heat or cool the room within desired parameters. With a checking account, it might be setting a limit on how low the account can go. The feedback loop purpose is to account for the behavior of the modified stock over time.
Mental Models
Now that we have the basic tools to draw a causal loop diagram, we need to add another piece of our systems speak vocabulary, which is mental modeling. Mental models represent the perspective of the builder or observer of the system. Each observer brings their own experiences to frame their understanding on how and why the system functions. An economist brings a different perspective than a psychologist. A mental model is defined as an interrelated set of beliefs that shape how a person forms expectations for the future and how the world works.Citation18 Monat and Gannon point out that:
System thinking requires that we recognize that in human-designed systems, repeated events or patterns derive from systemic structures which, in turn derive from mental models.Citation19
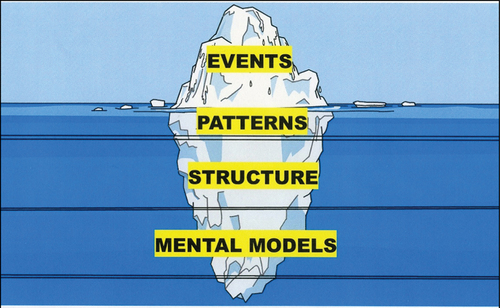
The iceberg model was created to visualize the underlying influences on events by the patterns, structure and mental models associated with the event (see ).Citation20,Citation21 The events that we see are affected by elements that are not so apparent. On the surface, we see events in the system. We see traffic going to work, but below the surface, there are unseen interacting patterns and trends that affect the traffic. To understand, how the parts of the iceberg model connect, observe the increase of local traffic when school is back in session. On the events level, the schools are in session. At the trend level, there is increased traffic due to the students traveling to school. Beneath the trends lies the system structure wherein you take the same roads as the school buses to get to work. Beneath the system structure lies your mental model. You choose this route because it is usually the fastest route you can take to the office, so you get stuck in traffic. The iceberg model is about the interconnectivity of things, which is the fundamental premise of systems thinking.
Figure 3. Iceberg model.
Learning Organizations
Before exploring system thinking applied to healthcare, there is one more knowledge stop to make along the way. It doesn’t take a great leap of imagination to see that the modern corporation can be viewed through the complex system’s lens. In his book, “The Fifth Discipline,” Peter Senge examined the principles of systems thinking as applied to corporate management, specifically how corporations could learn and improve their performance. What he recognized was that for a corporation to expand its capacity, it had to adopt a non-linear form of management. The CEO could not be the only person in the organization solving problems. A quick example from a dental office would be a dental assistant gently reminding the dentist that they are about to drill on the wrong tooth.
Senge wrote:
The tools and ideas presented in this book are for destroying the illusion that the world is created of separate, unrelated forces. When we give up this illusion – we can then build ‘learning organizations,’ organizations where people continually expand their capacity to create the results, they truly desire, where new and expansive patterns of thinking are nurtured, where collective aspiration is set free and where people are continually learning how to learn together.
As the world becomes more interconnected and business become more complex and dynamic, work must become more ‘learningful.’ It is no longer sufficient to have one person learning for the organization, a Ford, or a Sloan, or a Watson or a Gates. It’s just not possible to figure it all out from the top and have everyone following the orders of the ‘grand strategist.’ The organization that will truly excel in the future will be organizations that discover how to tap people’s commitment and capacity, to learn at all levels in an organization.Citation22
Senge describes how learning organizations work in an exercise called “the beer game”, which was invented at the Massachusetts Institute of Technology to teach students how to manage supply chain problems. In this exercise, individuals make decisions at various points along a supply chain with the object being to teach the importance of information sharing, supply chain management and collaboration through the process. Of direct relevance to the health care system is information sharing. Senge makes the point that to build a learning organization five technologies must be addressed:Citation23
Systems thinking
Personal mastery
Mental models
Building a shared vision
Team learning
Let’s discuss the three we have not addressed yet.
Personal Mastery
In this context, personal mastery does not mean technical dominance. It is the drive to obtain clarity in our personal vision of ourselves, to see things more objectively and to decrease the personal bias in our observations.
Building a Shared Vision
This refers to an organization in which people are bound together by a common identity and sense of destiny. It is not parroting a mission statement; it is an inward, personal commitment to a cause. An example would be a dental team that collectively puts the welfare of the patient above personal gains.
Team learning
How can a team of committed managers with individual IQ’s above 120 have a collective IQ of 63?Citation24
Serge points out that dialogue is the key to team learning. Each member needs to be open to hearing new ideas. Team members must be on the alert for “defensiveness”, as that can destroy team learning. The fundamental component of business organizations is the team, not the individual.
In summary, organizations learn not by linear thinking, but by the collective learning interactions of all the people of the organization. That process is a collective feedback loop.
Application of System Thinking to Health Care
We described two building blocks: systems thinking and learning organizations. The last piece and reason for this article is the application of these concepts to health care. The three publications discussed next will provide an overview of systems thinking applied to health care.
The most accessible article is the World Health Organization (WHO) report from the Alliance for Health Policy and Systems Research, entitled Systems Thinking for Health Systems Strengthening. (2008).Citation25 This report presents an overview of applying system thinking to large health care systems with the goal of increasing performance in producing health with equity. It examines several projects, including tobacco control, obesity, and tuberculosis. In the executive summary, the authors point out that system thinking identified challenges to the health care system by:
Exploring these problems from a systems perspective
Show potentials of solutions that work across subsystems
Promote dynamic networks of diverse stakeholders
Inspire learning
Foster more system-wide planning, evaluations and research
In the second article, Leischow, et al. published Systems Thinking to Improve Public Health (2008), which emphasized the need for a cross discipline approach to problem solving.Citation26 Transdisciplinary research is described as a:
process in which team members representing different fields work together over extended periods to develop shared conceptual and methodologic frameworks that not only integrate but also transcend their respective disciplinary perspectives
The article points out that most disease causation is multifactorial, dynamic and non-linear. It stresses that scientific silos, or compartmentalized knowledge, have the potential to impede understanding of the complex inter-relationships among disease variables. Emphasizing the migration from a top-down approach to an organizational wide sharing of information.
Lastly, in Development and Application of Systems Thinking Principles for Quality Improvement, Duncan McNab, et al. interpreted a white paper on aviation safety published by the European Organization for the Safety of Air Navigation.Citation27 This white paper was entitled: System Thinking for Safety: Ten Principles.Citation28 McNab found that, like aviation, most healthcare problems are systemic problems and conversely the solutions are usually systemic solutions. In their conclusion, five principles for patient safety were proposed:
Seek multiple perspectives to understand patient safety.
Consider the influence of prevailing work conditions, demand capacity, resources and constraints.
Analyze interactions and work flow within the system.
Try to understand why professional decisions were made at the time.
Explore everyday work, including adjustments made to achieve success in changing system conditions.
These articles emphasize how parts of the healthcare system interact to identify points of leverage where change can be made.
An Example of Applying System Thinking to the Dental Office
The final topic is the application of the tools of system thinking to dental office procedural sedation, which is an extremely complex subject of great importance and emotional content. Under the current sedation system, adverse events do occur in dental offices during sedation.Citation29,Citation30 The systems question is why and what can we do about these adverse events?
If we start to create our mental model of what makes up the dental office sedation system, we find a large complex system with multiple feedback loops involving information transfer, provider training, proficiency, experience and human engineering, all of which originate on the staff side. The facility encompasses technology, instrument systems and human engineering. Patients and their families bring in variables of the human condition adding to the many moving parts of this system. The purpose of the system is to safely perform dental procedures, while the patient is under the effect of sedation drugs, specifically to do no harm to the patient. Even with current safeguards and training, adverse events do occur.
What can be done about this? One solution tried in the past was to increase the amount of training required to perform procedural sedation.Citation31–33 If we draw a causal diagram of this solution or fix (see ), our problem/symptom is adverse sedation events in dental offices. The fix is to increase credentialing requirements. This solution decreases the number of adverse events by eventually decreasing the number of dentists who can do procedural sedation. The unintended consequence is that there are less new dentists with a sedation permit exacerbating an already acute problem of access to care for a vulnerable patient population. This is what occurred in a midwestern state.
Figure 4. System archetype “fixes that fail”.
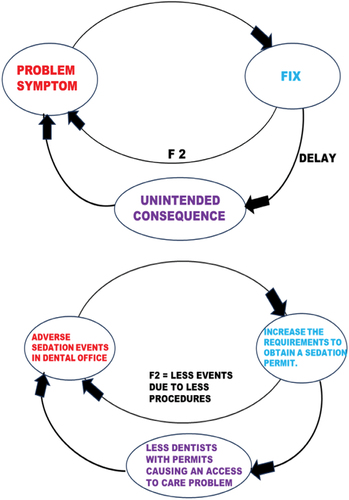
That state’s dental board proposed to change the requirements for an oral sedation permit to require the applicants to have a prescribed number of intravenous sedations in their training program. The proposal went beyond the levels set by the Council of Dental Accreditation (CODA) for the training of pediatric dentists. While the current holders of the oral sedation permit would be allowed to keep the permit license, no new pediatric dentist could meet the standards because of the lack of training in their graduate programs. is a causal diagram of this proposed credentialling change. The problem is adverse sedation events. The fix is to increase credentialling requirements. The solution eventually decreases adverse events. The unintended consequence is an increased access to care issue.
In the systems thinking vocabulary, there are archetypical examples, which describe common problem patterns that affect system behaviors. The eight common archetypes are: drifting goals, escalation, fixes that fail, growth and underinvestment, limit to success, shifting the burden/addiction, success to the successful and tragedy of the commons.Citation4 Improperly increasing the requirements to practice oral sedation can fall under “fixes that fail”Citation34
Is there another solution we could apply to the adverse sedation events problem from the organizational learning perspective? Let’s start with the premise that each dental office is part of a larger health care system. All offices are connected and interact with the larger complex system. Picture your office embedded with other offices in your community, which are embedded within the city you practice in, which are embedded with the dental offices of your state, which are embedded within the dental industry in the United States, which are embedded within the global dental industry. Each embedded system contributes valuable information to the dental health care system.
One can picture an infinite number of feedback loops of information crisscrossing the health care system universe. Each loop interacting with the other loops in the system. You have to wonder if it is even possible to observe the system as a whole. Let’s pull back to a wider perspective. From this vantage point, would we say that the system is a learning system? Is learning fundamental to our dental health care system? The answer is yes!
The health care system learns by the use of a simple reinforcing feedback loop (see )Footnote1.
Figure 5. PDSA cycle.
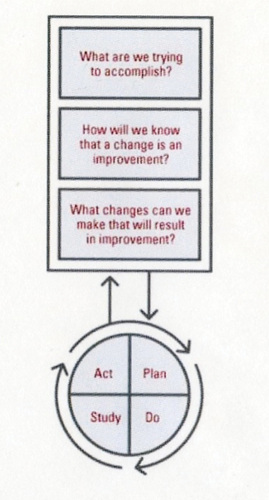
Something happens, it gets examined and changes are made. It’s how the system improves its function and performance. The Plan-Do-Study-Act (PDSA) cycle is how organizations and dentists learn and acquire knowledge.Citation35 Organized dentistry, universities and others offer continuing education courses and state dental boards share valuable information, which we evaluate and act upon. This information changes the way dentistry is practiced. The transfer of information is the first step to quality improvement. Someone finds a better way and shares the information with the profession. The key here is information sharing.
As noted in our healthcare systems thinking articles, information transfer is critical to a learning organization. In the two major space shuttle catastrophes, the National Aeronautics and Space Administration (NASA) had the information to prevent the accidents, but did not act upon it.Citation36,Citation37 The learning loop was broken by flaws in communication and decision making within the organization. Both accidents originated in poor information transfer within NASA.
Consider another very simple example looking at information and communication. Picture a field where a farmer has dug several large holes about 8 feet deep, which present a physical risk if you fell in. This night, you are given the task to cross the field. There is no moon and it is pitch black outside. You are given a choice to use a flashlight or not. You choose to use a flashlight. The information provided by the flashlight makes it easier to see the holes and safely cross the field. If you have fellow travelers, you can tell them where the holes are. Pretty simple. The more you know, the safer the trip.
Let’s consider what happens when there is an adverse event in a dental office. Individual dentists usually hear about an adverse event through mass media with few details shared. An investigation by the state dental board, looks to uncover the root cause of the event, but even that information is hard to access and is limited in its distribution. The profession is proverbially in the dark. If we think of each individual dental office interacting within the dental industry, we certainly would want that industry/system to warn us if there is a flaw or hole in the way we practice. Not pointing out such events would increase the likelihood for harm to happen again. By warning the dental community where the “holes in the field” are, we become a “learning organization,” acting as an accumulating feedback loop by sharing information to improve our walk/quality of care. Information is our flashlight; it shows us what to do and what not to do.
As we have pointed out when there is an adverse event in dentistry, there is little to no sharing of information. As a community, we are deprived of the opportunity to know what happened, learn from it, and institute appropriate measures so such an event does not happen in our office. We cannot apply the PDSA learning cycle because we do not have enough information to make an informed decision. If we recognize that the key to having an efficient and effective learning organization is communication, we must acknowledge that there is an obvious flaw in our system. There is an obstruction to the free flow of information and the system is deprived of an opportunity to learn from a mistake.
How do we fix this problem to open up the flow of information about adverse events to the profession? How do we eliminate the siloing of safety information to a few designated individuals? Fortunately, there is a tool to accomplish this task. It is a tool used in aviation and it is called “non-discoverable incident reporting.”
The Aviation Safety Reporting System (ASRS) is a voluntary, confidential reporting system, which is operationalized by NASA acting as an independent neutral third party.Citation38 A pilot or an airline files a report to the Federal Aviation Agency. The FAA sends the report to NASA, who de-identifies the report. The de-identified report is sent back to the FAA, where FAA experts examine the event for a root cause and prevention. The results are then released to the entire aviation industry. Under the ASRS, the FAA cannot use the information for any enforcement acts, except criminal actions. You can get a feel on how the aviation industry feels about the reporting system from this quote from the FAA website on mandatory and voluntary incident reporting:
Incident Reporting Saves Lives! It is critically important that all injuries and accidents, including near misses, are reported so that the causes can be determined and the risk eliminated. Reporting hazards helps prevent additional injuries and increases safety.Citation39
The dental reporting system would work similarly to the aviation system. When a severe adverse event or a sentinel event occurs in a dental office, the dentist would voluntarily send a report to an agency that would de-identify the report, analyze it, compare it with similar events and publish a summary. This could be done through a Patient Safety Organization (PSO) specific to dentistry.Citation40,Citation41 Once published, all dentists would have access to the information and have an opportunity to learn from it. Just like the aviation industry, dental professionals could grow their knowledge base through increased communication to bring the profession to new heights of safety and care.
Summary
In summary, the discipline of systems thinking is a way to approach problems of size. Large complex systems, like the dental industry, have multiple interacting components. Systems thinking through the use of specialized vocabulary and diagrams, attempts to understand the function and purpose of a large system. Through this study, a hoped-for result would be to identify points of leverage to influence the outcomes of the system. One of the functions of a complex system is the ability to learn. Through the work of Senge, the attributes of a learning organization are applied to organized dentistry to improve performance through quality improvement. By using systems thinking, a correctable flaw in the dental health care system was identified. The solution is non-discoverable incident reporting. Its use would improve the dissemination of adverse events information to the dental profession. This would enhance the dental health care system’s ability to learn from these tragic events and improve outcomes. If such reporting results in one less adverse event, it would be worth the effort.Citation42
Disclosure Statement
No potential conflict of interest was reported by the author(s).
Additional information
Notes on contributors
Charles S. Czerepak
Charles S. Czerepak is a Board-Certified Pediatric Dentist working at Pine Dental Care, a private practice in Chicago, Illinois. He is an Attending Dentist at the Ann & Robert H. Lurie Children’s Hospital of Chicago and an Assistant Clinical Professor at Northwestern University Feinberg School of Medicine. He currently serves on the ADA Medicaid Advisory Committee and the AAPD Pediatric Dental Medicaid and CHIP Advisory Committee. He is currently on the AAPD safety committee and is one of the moderators of the AAPD Special Interest Group on safety. He participated on the ADA task force on safety. He and his wife MaryAnn have two wonderful children and two fabulous grandchildren.
Notes
1. Copied from the AHRQ website on Health Literacy Universal Precautions Toolkit, 2nd Edition.
References
- System. Merriam-Webster.com 2023. https://www.merrian-webster.com Accessed November 27, 2023.
- Monay JP, Gannon T. What is Systems Thinking? A Review of Selected Literature Plus Recommendations. Am J Syst Sci. 2015;4:11–8.
- Ackoff RL, Addison HJ, Carey A. Systems Thinking for Curious Managers. Arminster, U.K: Triarchy Press Limited; 2010.
- Kim DH. Systems Thinking Tools, a User’s Reference Guide. Watham, MA: Pegasus Communications Inc. USA, 1994; 2000.
- Skochelak SE, Hammond MM, Lomis KD, et al. Health Systems Science. 2nd ed. Philadelphia, PA: Elsevier; 2022.
- Bertalanffy LV. An outline of general systems theory. British J Philos Sci. 1950;1(2):134–165. doi:10.1093/bjps/I.2.134.
- Meadows D. Thinking in Systems: A Primer. White River Junction, VT: Chelsea Green Publishing; 2008.
- Ackoff R. Redesigning the Future: A Systems Approach to Societal problems. New York, NY: John Wiley & Sons; 1974.
- Ackoff R. The Democratic corporation: A radical Prescription for Recreating Corporate America and Rediscovering Success. New York, NY: Oxford University Press; 1994.
- Razek L. 6 Reasons Coral Reefs Deserve Protection. Philadelphia, PA: Project: Protecting Coastal Wetlands and Coral Reefs, the PEW Charitable Trusts; 2022.
- United Nations Environment Programme, International Sustainability Unit & International Coral Reef Initiative. The coral reef economy: The business case for investment in the protection, preservation and enhancement of coral reef health; 2018. https://wedocs.unep.org/20.500.11822/26694.
- Cabrera D, Cabrera L. Systems Thinking Made Simple, New Hope for Solving Wicked Problems. 2nd ed. New York, NY: Plectica Publishing; 2015: 126–127.
- Atkins A. Holistic Change: Creating Organizational and Individuals Alignment at Genuity. Waathan, MA: The Systems Thinker, Pegasus Communication 2015.
- Leape LL. Error in medicine. JAMA. 1994;272(23):1851–1857. doi:10.1001/jama.1994.03520230061039.
- Weaver MD, Landrigan CP, Sullivan JR, et al. The association between resident physician work hour regulations and physician safety and health. Am J Med Jul. 2020;133(7):e343–e354. doi:10.1016/j.amjmed.2019.12.053.
- Meadows DH. Thinking in Systems: A Primer. White River Junction, VT: Chelsea Green Publishing; 2008: 18.
- Meadows DH. Thinking in Systems: A Primer. White River Junction, VT: Chelsea Green Publishing; 2008: 27.
- Holtrop JS, Scherer LD, Matlok DD, Glasgow RE, Green LA. The importance of mental models in implementation science. Front Public Health. 2021, Jul 6;9:680316. doi:10.3389/fpubh.2021.680316.
- Monat JP, Gannon TF. What is systems thinking? A review of selected literature plus recommendations. Am J Syst Sci. 2005;4:11–26.
- Monat JP, Gannon TF. The meaning of “structure” in Systems Thinking. Systems. 2023;11(2):92. doi:10.3390/systems11020092.
- Maani K, Cavana R. Systems Thinking and Modelling – Managing Change and Complexity. 2nd ed. Hoboken, NJ: Pearson Education, Prentice Hall; 2007.
- Senge P. The Fifth Discipline. The Art and Practice of Learning Organizations. New York, NY: Crown Business; 2006.
- Senge P. The Fifth Discipline. The Art and Practice of Learning Organizations. New York, NY: Crown Business; 2006: 6.
- Senge P. The Fifth Discipline. The Art and Practice of Learning Organizations. New York, NY: Crown Business; 2006: 9.
- de Savigny D, Adamo T, eds. Systems Thinking for Health Systems Strengthening. Geneva, Switzerland: Alliance for Health Policy and Systems Research, WHO; 2009.
- Leischow SJ, Best A, Trochim WM, et al. Systems Thinking to Improve the Public Health. Am J Prev Med. 2008 August;35(20):S196–S203. doi:10.1016/j.amepre.2008.05.014.
- McNab D, McKay Sorrock JS, Bowie S, Luty P. Development and application of ‘systems thinking’ principles for quality improvement. BMJ Open Qual. 2020;9(1):e000714.
- EUROCONTROL. Systems Thinking for Safety: Ten Principles (A White Paper). Brussels, Belgium: EUROCONTROL; 2014.
- Obadaro EM, Ramoni RB, Kalenderian E. Lessons learnt from dental patient safety case reports. J Am Dent Asso. 2015 May;146(5):318–326.e2. doi:10.1016/j.adaj.2015.01.003.
- Rafetto LK. Safety in the Dental Office. Dela J Public Health. 2023 Apr;9(1):52–55. doi:10.32481/djph.2023.04.012.
- Diomme RA. Proposed guideline revisions for dental sedation and general anesthesia: why target the safest level of sedation? Compendium. 2016 Sept;37(8):546–52.
- Boynes SG, Bastin MR. Sedation regulations changes and their impact on dental practice. Decisions in Dentistry. 2018 March;4(3):15–16,18,21.
- Kleinpell R, Myers CR, Schorn MN. Addressing barriers to APRN practice: policy and regulatory implications during COVID-19. Journal of Nursing Regulations. April 2023;14(1):13–20. doi:10.1016/S2155-8256(23)00064-9.
- Clancy T. Systems thinking: three system archetypes every manager should know. IEEE Engineering Management Review. Vol. 46, No. 2, Second Quarter, June 2018. IEEE. doi:10.1109/EMR.2018.2844377.
- Plan-Do-Study-Act (PDSA). Directions and Examples: in Health Literacy Universal Precautions Tool Kit. 2nd ed. Agency for Healthcare Research and Quality (AHRQ). www.ahrq.gov/health-leteracy/improve/precautions/tools2b.html
- Report of the Presidential Commission of the Space Shuttle Challenger Accident, Jun 6, 1986. Washington Government Printing Office, Vol. 1; 1986.
- Columbia Accident Investigation Board Report Vols. 1–5; August 2003. Washington DC: Government Printing Office.
- Aviation Safety Reporting System (ASRS). Washington, DC: Federal Aviation Agency; 2024. http://faa.gov/aircraft/safety/report
- Aviation Safety Hazmat Reporting. Wahington, DC: Federal Aviation Agency; 2024. http://faa.gov/hazmat/incident-reporting
- Patient Safety Organization (PSO). Washington, DC: Agency for Healthcare Research and Quality; 2024. http://pso.ahrq.gov
- Dental Patient Safety Foundation PSO. Orland Park, IL: Dental Patient Safety Foundation; 2024. www.dentalpatientsafety.org
- Kalenderian E, Walji MF, Tavares A, Ramoni RB. An adverse event trigger tool in dentistry. A new methodology for measuring harm in the dental office. JADA. 2013 July;144(7):808–814. doi:10.14219/jada.archive.2013.0191.