
Abstract
The quality and reliability of a nation's healthcare system is often driven by the number and diversity of its healthcare professionals. Unfortunately, many developing nations have constrained segments of highly skilled labor and must “import” this human capital. Volatility in key healthcare professions can threaten reliable and sustainable healthcare delivery. This article considers the development of a healthcare human resources sector in a quickly developing nation as an enterprise transformation problem. In this article, the axiomatic design large flexible system modeling framework is used to assess healthcare delivery capability in Abu Dhabi, UAE. Here, each profession type is modeled as a functional requirement, and the physical hierarchy is modeled at individual, healthcare facility, and regional levels. The knowledge base is filled with the associated number of professionals of a given type provided by the corresponding design parameters. The Abu Dhabi case study shows significant volatility in the healthcare labor market. The work demonstrates that te axiomatic design theory as applied to large flexible systems can be applied to data-centric methods in human resources management in the context of skills shortages and high attrition rates.
1. INTRODUCTION
1.1 Motivation
The progress of a developing nation is often measured by the advancement of their infrastructure. While “hard” infrastructure, such as water, power, and transportation, is often easy to assess, “soft” infrastructure (Niskanen, Citation1991), such as healthcare systems, is often more challenging. Fundamentally, healthcare is a labor-intensive system, the quality and reliability of which are driven by the number and diversity of its healthcare professionals. Therefore, ensuring a nation's development can be seen to depend as equally on the retention of knowledge-based healthcare professionals as it does on the maintenance of water, power, and transportation capital.
Moving from a macroeconomic scale to a microeconomic scale, recent research has shown the critical role of knowledge workers in the strategic development of organizations (Grant, Citation1996; Pettigrew, Thomas, and Whittington, Citation2006; Spender, Citation1996). This is due in large part to the workers’ possession of tacit knowledge (Nonaka and Nishiguchi, Citation2001; Nonaka and Takeuchi, Citation1995), which has received much attention in the context of the resource-based view (Barney, Citation1991; Wernerfelt, Citation1995), competence-based competition (Leonard-Barton, Citation1992; Nonaka and Takeuchi, Citation1995), dynamic capabilities (Brown and Eisenhardt, Citation1998; Spender, Citation1996; Teece, Pisano, and Shuen, Citation1997), and knowledge-based view (Grant, Citation1996; Sveiby, Citation2001). Ultimately, human resources management (HRM) is the key factor in the successful growth of enterprises (Shah, Nazir, Zaman, and Shabir, Citation2013).
The strategic importance of knowledge workers has subsequently led to supporting HRM practices. In one work, the impacts of HRM practices are studied from an operations management perspective (Pathirage, Amaratunga, and Haigh, Citation2007). In another, experienced and well-trained police and fire personnel made fewer mistakes and performed faster in the delivery of their critical services (Taylor, Murphy, and Price, Citation2006). Such results are likely extensible to first-response healthcare professionals. HRM has also shown to be central to the development of a leadership-centric business vision (Roepke, Agarwal, and Ferratt, Citation2000). Recent work has also shown the importance of HRM to the knowledge management of an organization (Whelan and Carcary, Citation2011) and its criticality in the development of learning organizations (Lee-Kelley, Blackman, and Hurst, Citation2007), especially as it develops key capabilities in corporate social responsibility and sustainability (Nicolopoulou, Citation2011).
Unfortunately, many nations suffer from very constrained segments in their highly skilled, knowledge-centric labor market (Jin and Li-ying, Citation2003). Given the relative ease of attrition and relative difficulty to train, the HRM literature has given a great deal of attention to IT professionals (Ang and Slaughter, Citation2004; Roepke et al., Citation2000; Zheng and Hu, Citation2008). One author also highlighted the critical service role of IT professionals in the healthcare sector (Boland, Citation1998). Similarly, HRM research has addressed the challenges of maintaining a capable R&D staff (Han and Froese, Citation2010), including the needs posed by its female members (Cuny and Aspray, Citation2002; Servon and Visser, Citation2011). The retention of army officers is also a particularly interesting workforce segment given that their practical field experience represents decades of tacit knowledge (Dabkowski, Huddleston, Kucik, and Lyle, Citation2011). Similarly, HRM practices have recognized the important role of senior workers (Armstrong-Stassen and Schlosser, Citation2011; Wong and Kimura, Citation2009). Finally, there is growing recognition that knowledge workers also includes skilled manual labor in manufacturing (Foy and Iwaszek, Citation1996; Zheng, Soosay, and Hyland, Citation2008) and construction (Clarke and Herrmann, Citation2007; Gow, Warren, Anthony, and Hinschen, Citation2008).
These human resources challenges are particularly exacerbated in developing and emerging economies, where either human capital has not had a chance to accumulate or the growth rate of the economy outstrips efforts at human capital development (Beulen, Citation2009; Kapoor and Sherif, Citation2012). Geography-specific studies have addressed the large-scale issues found in China and India (Beulen, Citation2009; Doh, Smith, Stumpf, and Tymon, Citation2011; Kapoor and Sherif, Citation2012; Zheng et al., Citation2008). In similar studies, Horwitz (Citation2011) showed the lingering impacts of centrally planned political economies on HRM in eastern and central Europe, while Zheng and Hu (Citation2008) described the effects of economic restructuring in Singapore and Taiwan. Further attention has been given to Gulf Cooperation Council (GCC) countries where the absence of well-established indigenous human capital combined with fast economic and population growth has led to dramatic needs in HRM (Doh et al., Citation2011; Horwitz, Citation2011).
1.2 Contribution and Potential Application
Given these exacerbated conditions in the GCC, and the importance of retaining knowledge-centric healthcare professionals to a nation's development, this article views healthcare HRM as a dynamic process of enterprise transformation where the enterprise is the national healthcare delivery sector. This paradigm is valid within the GCC as the national healthcare authority is run as a large semi-private enterprise with a near monopoly over the local healthcare sector. In a sense, it is a directed system-of-systems (Maier, Citation1998; Wenger, Antoniev, and Gorod, Citation2013) that must operate in an environment of rapid economic and population growth.
Unlike many traditional applications of HRM, where organization size is either stable or modestly growing, this application requires HRM techniques to track a steep growth trajectory. As such, and from a methodological perspective, this article departs from classical survey-based human resources retention and attrition management in favor of a big data analytics approach. This approach is based upon the axiomatic design theory for large flexible systems but is extended in such a way that its knowledge bases evolve dynamically in time to track population growth rates.
This article also contributes a case study with a descriptive analysis of the volatility and the retention caused by healthcare HRM practices in the emirate of Abu Dhabi. To our knowledge, this is the first such public study of its kind. As such, the study presented here can highlight areas of deficiency that human resources managers can either resolve or investigate root causes.
1.3 Article Outline
These contributions are made over six sections. The background section provides the methodological background to this study in terms of existing HRM research methods and the relevant aspects of axiomatic design. The methodology section provides a methodological contribution by describing how an axiomatic design knowledge base can be used to model the healthcare labor pool as a large flexible system. The remainder of the article introduces the Abu Dhabi case study and its results. The work concludes with the general implication on data-intensive HRM.
2 METHODS
The methodological background for the study is presented. Existing human research management methods are first reviewed so they can be contrasted to how an axiomatic design based approach can be applied. Next, the axiomatic design knowledge-based models are applied to data-centric HRM of healthcare professionals.
2.1 Existing HRM Research Methods
In the context of this discussion, HRM research methods have centered around two broad classes of research questions: (1) What are the causal factors driving an individual's decision to join and stay within an organization (Afifi, Citation1991; Ang and Slaughter, Citation2004; Armstrong-Stassen and Schlosser, Citation2011; Budhwar, Varma, Malhotra, and Mukherjee, Citation2009; Ghosh and Sahney, Citation2010)? (2) What HRM strategies can be implemented to prolong the retention of this individual in an organization (Beulen, Citation2009; Chew and Chan, Citation2008; Finegold, Levenson, and Van Buren, Citation2005; Kaliprasad, Citation2006; Lockwood and Ansari, Citation1999)? In the majority of this work, the research methods relied on semi-structured interviews and surveys to study the attrition intention of currently employed individuals. Such a research methodology presents two biases. First, it is not clear if the intention to resign is fleeting or if it is severe enough to be actionable. Second, the individuals who have already resigned are not included in either the interviews or surveys. From the perspective of continuous improvement, these individuals present the greatest learning opportunities.
In contrast, some of the more recent research has taken the strategy of directly studying organizations’ human resources databases (Dabkowski et al., Citation2011; Holtbrugge, Friedmann, and Puck, Citation2010; Zheng and Hu, Citation2008). Such a research methodology resolves the two previously mentioned concerns. Furthermore, it allows for rigorous diagnostic capabilities based upon data-mining techniques (Chien and Chen, Citation2008; Dabkowski et al., Citation2011). For example, recent work has proposed the usage of geographic information system (GIS) technology to study the impact of location on human resources retention (Hanewicz, Citation2009). Other work presents the development of work flexibility to manage the disturbances caused by worker attrition (Fry, Kher, and Malhotra, Citation1995). These types of practices lend themselves to the knowledge base-centric capabilities assessments used in the axiomatic design of large flexible systems.
2.2 Axiomatic Design Theory for Large Flexible Systems
Prior to proceeding with the application of axiomatic design for large flexible systems in the next section, an introduction is provided here to guide the reader. At its heart, axiomatic design addresses the mapping between the functional domain and the physical domain. At a given level of hierarchy or decomposition, this mapping is described as a matrix design equation (Suh, Citation2001):
(1) where FR represents the functional requirements, DP represents the design parameters (i.e., system parameters, components, modules, or artifacts), DM is a binary design matrix, and the = symbol means “fulfilled by” (Farid, Citation2007; Suh, Citation2001). The goal of axiomatic design is to fulfill the independence axiom and create an uncoupled design (Suh, Citation2001). In practice, this requires a one-to-one mapping between elements in FR and DP and occurs when DM is square and diagonal (Suh, Citation2001). Upper triangle forms of DM are also considered admissible designs and are said to be decoupled (Suh, Citation2001). For the sake of mathematical rigor, EquationEq. (1)
(1) has multiple meanings. Very low in the functional/physical dual hierarchy, FR and DP are real numbers and the * operator signifies traditional matrix multiplication (Suh, Citation2001). At higher levels of the dual hierarchy, FR and DP are represented by sets of functions and objects, respectively, and the * symbol signifies an aggregation operator (Farid, Citation2007; Farid and Khayal, Citation2013; Farid and McFarlane, Citation2008).
Definition 1. Aggregation Operator * (Farid, Citation2007; Farid and Khayal, Citation2013; Farid and McFarlane, Citation2008): Given an arbitrary element sj ∈ S, an arbitrary parent group s k ∈ S, and a binary aggregation matrix A for which elements akj equal 1 if sj ∈ sk, then (Farid, Citation2007; Farid and Khayal, Citation2013; Farid and McFarlane, Citation2008)
(2)
For the purposes of recursively representing the axiomatic design functional and physical hierarchies,
(3)
Finally, it must be noted that the application of EquationEq. (1)(1) implies that FR and DP are taken as fixed sets and is called the axiomatic design for large fixed systems (Suh, Citation2001). A deep introduction to this theory is provided in Chapter 4.4 of the classical text (Suh, Citation2001).
Given that this article concerns enterprise transformation from a human resources perspective, the assumption that FR and DP are fixed sets must be relaxed. For this, Suh, in his classical text (2001, pp. 202–207), developed axiomatic design for large flexible systems. Suh (Citation2001) defined large flexible systems as systems with many functional requirements that not only evolve over time but each functional requirement can be fulfilled by any one of a number of design parameters. This is such a fundamentally different mapping of FR to DP that DM is replaced by a knowledge base. Consider the example provided in the classical text (Suh, Citation2001):
(4)
Here, Suh (Citation2001) stated that “FR1 can be satisfied (indicated by $) by DPa1 or DPb1 or DPc1” (p. 203). It is important to note the usage of the word or and not and to describe the design. First, it implies that there is no longer a one-to-one mapping of FR to DP. It also implies that, in the axiomatic design for large flexible systems, the independence axiom is still fulfilled because DPa1 (alone and in its entirety) fulfills FR1 in exactly the same way that a one functional requirement fixed system design fulfills the independence axiom. The same holds true for DPb1 or DPc1. The simultaneous presence of other DPs that are able to do the same does not violate the independence axiom (Farid, Citation2007; Farid and McFarlane, Citation2008).
Although Suh (Citation2001) did not further revisit the subject of the axiomatic design of large flexible systems, it has since been applied in the design of reconfigurable manufacturing systems (Farid, Citation2007, 2008, Citation2013, 2014a; Farid and McFarlane, Citation2008; Farid and Ribeiro Citation2014), reconfigurable transportation systems (Baca, Farid, Tsai, and Viswanath, Citation2013; Viswanath, Baca, and Farid, Citation2013), transportation-electrification (Viswanath and Farid Citation2014), temporary housing (Gilbert, Farid, and Omar, Citation2013), power systems (Farid, 2014b), water infrastructure (Farid, Citation2014c), energy–water nexus (Lubega and Farid Citation2014), and HRM (Farid and Khayal, Citation2013; Khayal and Farid, Citation2013). In all of these works, EquationEq. (3)(3) is rewritten in terms of a matrix equation using a Boolean knowledge base matrix J:
(5) where the A · B operation represents the Boolean equivalent of matrix multiplication:
(6) and where Vj is the array-OR operation similar to the familiar sigma (summing) notation for real numbers (Farid and McFarlane, Citation2008).
All of these applications of axiomatic design for large flexible systems also advanced the concepts of system degrees of freedom, functional redundancy, and design parameter flexibility (Baca et al. Citation2013; Farid, Citation2007, Citation2008, Citation2013, 2014a, 2014b, 2014c; Farid and Khayal Citation2013; Farid and McFarlane, Citation2008; Farid and Ribeiro, Citation2014; Gilbert et al., Citation2013; Khayal and Farid Citation2013; Lubega and Farid Citation2014; Viswanath and Farid Citation2014; Viswanath et al., Citation2013). A generalized definition of a large flexible system's degrees of freedom is:
(7)
From this, it follows that redundancy Ri of the ith functional requirement is
(8) and the flexibility of the jth design parameter is
(9) because the independence axiom is already fulfilled in large flexible systems, the focus of the design questions turns to how much functional redundancy and physical flexibility is required.
The quantification of the knowledge base as a description of a large flexible system also allows the rigorous description of its change in time through a reconfiguration process (Farid and Covanich, Citation2008). Given a reconfiguration process R that occurs over a time interval T, the resulting discrete time difference equation describes the time evolution of the knowledge base:
(10)
Given that J represents independent degrees of freedom, it is valid to vectorize it with the vec() operator (Abadir and Magnus, Citation2005) as is typically implemented in MATLAB with the (:) operator. It follows that the knowledge base differential ΔJ caused by a reconfiguration process R is given by
(11)
These measures are applied to the development of a healthcare human resources knowledge base in the following section.
3 MODELING HEALTHCARE SYSTEMS WITH AXIOMATIC DESIGN
In this section, the axiomatic design theory for large flexible systems is applied to model the (licensed) healthcare workforce in a national healthcare system. This is distinguished from the HRM system, which could potentially act to change the size, composition, and placement of this healthcare workforce. That said, the chosen modeling technique describes the system architecture (Farid, Citation2007; Oliver, Kelliher, and Keegan, Citation1997) that is a necessary aspect of enterprise transformation (Basole et al., Citation2013).
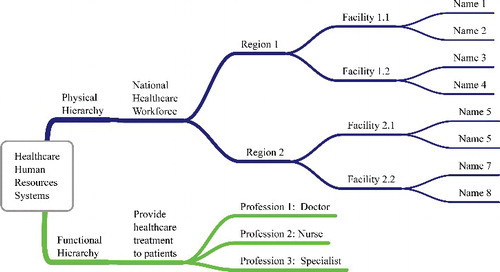
The functional requirements and design parameters are established as follows. The set of functional requirements is defined as the set of healthcare professions; FR = {Healthcare Professions} (e.g., general practitioner profession, nursing profession). In systems engineering, functional requirements are traditionally written in a “verb + operand” construction (Oliver et al., Citation1997); however, in HRM, human resource functions actually refer to certain job descriptions or roles that a given employee must do (e.g., accounting, engineering, maintenance). Therefore, it is important to interpret FR above not as people that execute healthcare professions but rather the professions themselves that must be done. Consequently, the design parameters are the set of individuals’ names; DP = {Individual Names}.
Physical hierarchies based upon aggregation appear in all systems of significant size, and the design parameters may be organized accordingly. Here, further analyses can be conducted if each individual belongs to a healthcare facility; DP = {Healthcare Facilities}. Finally, these healthcare facilities can be viewed in terms of the geographic regions in which they are located; DP = {Regions}. Although the design parameters in axiomatic design for large flexible systems are assumed to change, their aggregations as healthcare facilities and regions are assumed to remain stable.
This work does not introduce a functional hierarchy. The axiomatic design for large fixed systems does require the physical and functional hierarchies be decomposed to equal levels (Suh, Citation2001). However, doing so in large flexible systems can be problematic. The axiomatic design for large flexible systems assumes that the set of functional requirements will change in time (Suh, Citation2001, p. 204). Consequently, the functional hierarchy is likely to change as well. Furthermore, physical aggregation and functional aggregation do not have the same meaning and do not necessarily imply each other (Dori, Citation2002). Consider for example, a functional hierarchy that mirrors the physical hierarchy previously described. The healthcare professions would then be organized into neighborhoods (around facilities) and then regions. However, such a hierarchical approach would ultimately fix the composition of healthcare professions in each neighbourhood or region and may result in a highly rigid top–down structure. Any time the set of functional requirements changed, the functional hierarchy would likely change as well. Furthermore, in this application domain, such a fixed functional hierarchy would not recognize that patients will go to any region they feel best serves their healthcare, and this can indeed easily change. Mismatched functional and physical have been previously found in the axiomatic design for large flexible systems (Baca et al., Citation2013; Farid and Khayal, Citation2013; Farid and Ribeiro, Citation2014; Khayal and Farid, Citation2013; Viswanath et al., Citation2013).
The resulting axiomatic design dual hierarchy is pictured in . The independence axiom is fulfilled at the leaves of the hierarchy. Any given profession is fulfilled by an individual qualified to execute that profession. As mentioned in section 2.2, the axiomatic design for large flexible systems allows the redundancy of individuals to fulfill a given profession without violating the independence axiom. Furthermore, this decomposition can easily be integrated into existing frameworks for enterprise modeling and simulation previously applied to the healthcare sector (Barjis, Citation2011).
The relationships between the healthcare professions in the functional hierarchy and the various aggregations of the physical system can be captured in the healthcare human resources knowledge base. At the lowest level, J is the binary map between the ith healthcare profession and the jth individual name. At a higher level of aggregation, JP is defined as an integer knowledge base for which the elements equal the number of individuals with a given profession at a given healthcare facility; it then follows that
(12)
EquationEquation (12)(12) may be used recursively for the regional analysis.
The calculation of the number of healthcare human resources degrees of freedom follows straightforwardly from EquationEq. (7)(7) ; it represents the total number of healthcare professionals in the system at a given time. The redundancy Ri of the ith healthcare profession is given by EquationEq. (8)
(8) , or in the special case that all healthcare professionals work for a single healthcare facility or region, then
(13)
Similarly, EquationEq. (9)(9) gives the functional flexibility Fj of the jth design parameter. It represents the number of professions for which an individual is licensed. Typically, this is only 1. The functional flexibility Fk of the kth healthcare facility exhibits the same form provided that JP is taken in binary rather than integer form:
(14)
The healthcare system properties of profession redundancy and facility flexibility are particularly important system properties. The former is often related to a healthcare system's quality of service (QoS), especially when normalized by the size of the patient population (e.g., number of doctors/patients). The latter is often related to a healthcare facility's convenience in that if a particular profession is present at a given facility, it then eliminates the need for a patient to go elsewhere. Such a convenience measure addresses patient conditions that are time critical one-offs (e.g., emergency services) as well as more routine services (e.g., the neighborhood pharmacist).
In this context, HRM recruiting practices that counter natural rates of professional attrition can be modeled as reconfiguration processes acting upon the system knowledge base. Given a recruiting (reconfiguration) process RR and an independent attrition (reconfiguration) process RA that occur over a time interval T, the healthcare human resources knowledge base evolves by a differential:
(15)
One novelty in this work is the extension of the knowledge base differential to a proper differential equation. If the recruiting and attrition processes are taken to be time-invariant processes that occur over successive time intervals, then EquationEq. (15)(15) can be rewritten as a familiar first-order differential equation:
(16)
The efficacy of HRM practices can then be measured in terms of the time constant matrix (RR – RA)/T. In a sense, EquationEq. (16)(16) describes the rate of change of the healthcare human resources system architecture for which its control is the region's aggregate human resources practices. The rate of change is also particularly important in the context of rapid population growth, as the normalization by population is closely linked with QoS.
4 CASE STUDY RESULTS—EVOLUTION OF ABU DHABI HEALTHCARE HUMAN RESOURCES KNOWLEDGE BASE
In this section, the models presented in section 3 are applied to an emirate of Abu Dhabi data set of healthcare professionals to draw some conclusions about the emirate's HRM practices. Section 4.1 describes the data in detail, while section 4.2 presents the results from the two perspectives highlighted in section 3: QoS and convenience of service (CoS).
4.1 Data
The Abu Dhabi emirate is the largest of the seven emirates in the United Arab Emirates and makes up 80% of the UAE land area. Abu Dhabi city is the capital of the UAE (Anonymous, 2013). According to the Statistics Centre of Abu Dhabi (SCAD), in 2011, UAE nationals made up approximately 20% of the population, while the remaining 80% were expatriates. This illustrates the UAE as a country in need of importing much of its healthcare human capital into the labor market.
The data used in this article include a publicly available list of all clinician licenses issued in the emirate of Abu Dhabi (Health Authority of Abu Dhabi, 2013). The license list was cleaned and organized with the following attributes used in this case study: physician name, profession, facility licensed at, region (of the Abu Dhabi emirate), start date, and end date. The data used in this analysis spanned from 1967 to 2012, with 35 professions in 1,769 facilities in 15 regions.
The numbers of clinicians per year were normalized across the 45 years by dividing by the population in Abu Dhabi. They are presented in units of number of clinicians per million people. The population data was derived from SCAD's published report “Abu Dhabi Development Statistics-Population and Labour Force” (Statistics Center of Abu Dhabi, 2013).
4.2 Results
The provided data were analyzed using the axiomatic design models and measures provided in the methodology (Farid and Khayal, Citation2013). The results are presented in terms of healthcare system QoS and CoS.
4.2.1 QoS—Profession Redundancy
In this section, QoS is assessed in terms of profession redundancy normalized to the actual population. , , and present the evolution of healthcare professional recruiting, attrition, and net in Abu Dhabi from 1967 to 2012 on a semi-log scale. All three figures show a decreasing envelope trend, where the exponential population growth is occurring at a faster rate than the process of recruitment or attrition. That said, all three figures show general upward trends, suggesting that the healthcare enterprise is very much in a growth phase. One interesting question outside the scope of this work is the ideal number of clinicians per population to which each of these healthcare functions must ultimately stabilize. The overall growth trends, even when normalized by the population, suggests that the emirate of Abu Dhabi as a whole has not reached these final healthcare service targets.
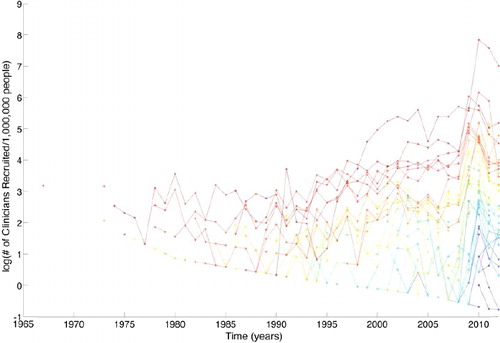
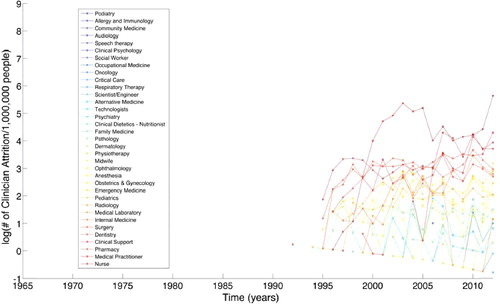
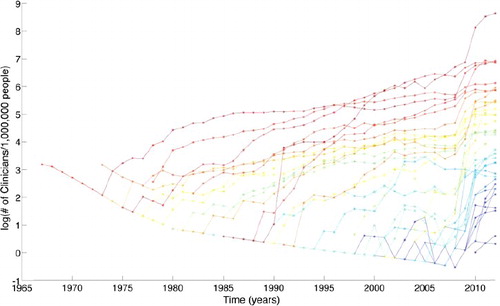
In addition to the baseline growth trend, the data also show a number of other interesting phenomena. First of these is a significant systematic change in healthcare recruiting between 2008 and 2010. The figures also show varying trends between professions that have been established the longest and those that have been available for the shortest period of time in Abu Dhabi. The oldest healthcare professions, such as medical practitioners, pharmacists, and dentists, tend to show more stable evolutions. These older healthcare professions also show minimal to no attrition before the 1990s. The recruitment and attrition of professionals appear to be very volatile, while the net seems to be much more stable. This shows specific effort toward attempting to maintain and minimize volatility over the years, given patterns of high and variable attrition.
presents the statistical measures of the QoS. The statistic measures of the coefficient of variation; the regression line slopes bR, bA, and b; and the coefficient of determination (goodness of fit) R2 give complementary views of the evolution of healthcare professionals. The highest coefficients of variation of professions include nurses and family medicine; these are professions that have been established for approximately 30 years yet show large volatility. The values show that there is very large volatility in these much-needed areas. Meanwhile, the regression line slopes demonstrate that the Abu Dhabi healthcare system is still very much in a ramping-up phase indicative of a developing nation. Nearly all professions are growing at many multiples of the population growth rate, with the strongest trends in social workers, critical care, and respiratory therapy. Finally, the correlation coefficients show the greatest volatility in healthcare professions with the least redundancy, suggesting the need for further recruiting to maintain QoS.
TABLE 1 Statistical Measure of QoS
4.2.2 CoS—Functional Flexibility of Facilities
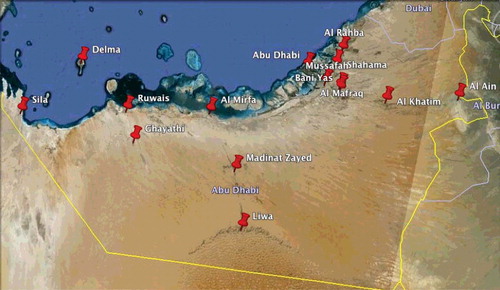
In this section, CoS is assessed in terms of functional flexibility for facilities as well as regions. shows the evolution of facility diversity over time for the 1,769 facilities. shows the evolution of region diversity over time for the 15 regions in the Abu Dhabi emirate. illustrates the geolocation of the regions in the Abu Dhabi emirate.
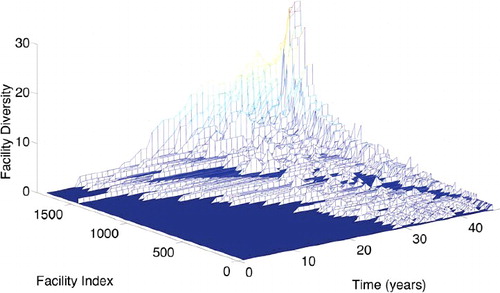
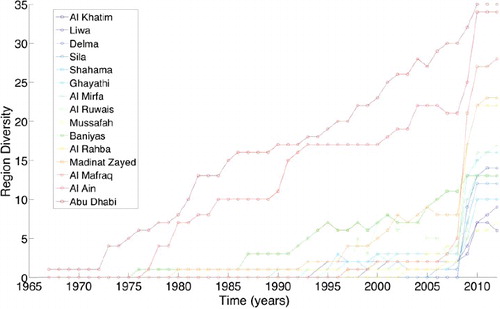
and show similar trends and different levels of detail. highlights the tremendous diversity in the services offered from facility to facility. Naturally, some facilities are larger than others and offer more services. A more interesting picture emerges when these data are aggregated by region, as shown in . Relatively well-established regions (e.g., Abu Dhabi, Al-Ain) lead with a greater diversity of services than the comparatively basic services offered in rural regions. The region diversity can be described as having a linear trend. However, there appears to be a drastic increase in region diversity for most regions starting in 2009.
presents the statistical measures of the CoS. The statistical measures show the most consistent expansion in healthcare services in Abu Dhabi, Al Ain, and Baniyas as compared to the other regions that undertook the 2008 regional diversity expansion.
TABLE 2 Statistical Measures of CoS
5 DISCUSSION: TRANSFORMATION OF THE HEALTHCARE SECTOR ENTERPRISE IN A RAPIDLY DEVELOPING NATION
Given the results provided in the previous section, this section seeks to add to the developing literature on enterprise transformation in the healthcare sector (Basole, Braunstein, and Rouse, Citation2012). In particular, this work is interested in rapid healthcare human resources growth in a developing nation. This discussion is organized into five parts based upon four insights. First, human resource capacity must be viewed functionally as well as regionally to address both QoS and CoS. That given, the HRM problem must first focus on simply building capacity at the necessary growth rate for all functions in all regions. Third, even if the right growth rate for each function and region is achieved, the volatility in this growth rate must also be minimized to maximize the efficiency of the enterprise transformation. Finally, the authors recognize that a well-controlled growth rate underestimates the stock of unquantifiable implicit knowledge that retained healthcare professionals possess. A physician with 15 years of experience abroad is not likely to contribute as well as a physician with 15 years of local experience. The discussion proceeds around each of these points in turn.
5.1 Building Healthcare Functional Capacity
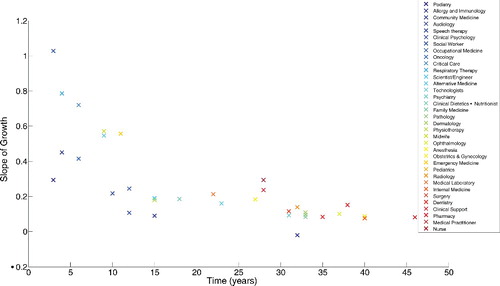
This subsection quantifies how well Abu Dhabi is building healthcare functional capacity. shows theslope of growth for healthcare professions as a function of how long the profession has existed within the emirate. Interestingly, the slope of the functional growth depends very heavily on how long the function has existed. Healthcare functions that have existed for greater than approximately 15 years have modest normalized growth rates of approximately 0.1 log(clinicians/population). A normalized log growth rate of zero corresponds to a steady ratio of clinicians per population. In contrast, 12 new functions entered the healthcare system within the last 15 years. In these cases, the growth rates are significantly more aggressive. This analysis suggests that the HRM problem simultaneously requires a rapid diversification of functionality while maintaining a steady maintenance of established functionality.
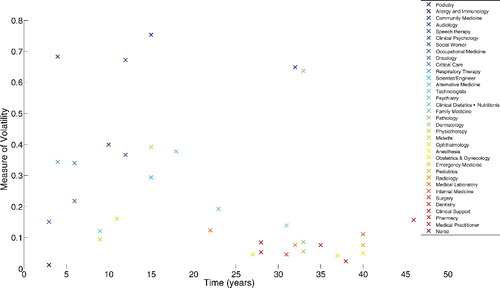
5.2 Controlling Healthcare Human Resources Functional Capacity
While Abu Dhabi continuesto maintain existing healthcare functionality and rapidly introduce new diverse functionality, the efficacy of this process can be measured by the volatility in these growth rates. In a sense, the healthcare enterprise, over time, should be developing HRM practices that become increasingly adept at holding the growth rate constant to a desired level. shows that while the volatility for many professions that have existed for more than 25 years has stabilized to below 0.1 log(clinicians/population), other professions still exhibit considerable volatility. In most cases, the professions that have existed for less than 20 years exhibit volatility measures between two to eight times the stabilized rate. Finally, practitioners of family medicine and allergy/immunology exhibit extremely high volatility despite their presence in the emirate for more than 3 decades. These results suggest that the healthcare enterprise is unable to stabilize its healthcare functional capacity until at least 2 decades have passed. More focused efforts can be made to retain existing professionals while also streamlining the recruiting process relative to their attrition.
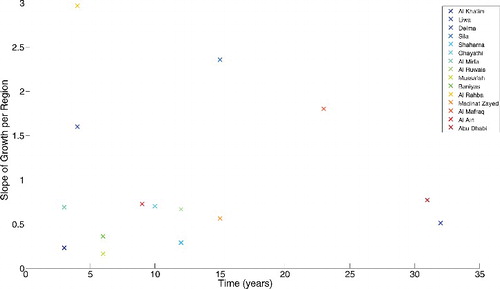
5.3 Building Healthcare Human Resources Regional Capacity
This subsection quantifies how well Abu Dhabi is building healthcare regional capacity. gives a telling picture of rapid growth. While the previous subsections showed that the growth in some healthcare professions had stabilized, all regions in the emirate of Abu Dhabi are rapidly developing healthcare capacity. In cases like Delma and Sila, these figures can be interpreted as a concerted effort to bring convenient healthcare services toless populated areas. And yet, even the more established cities of Abu Dhabi and Al Ain are continuing to develop and mature their healthcare services.
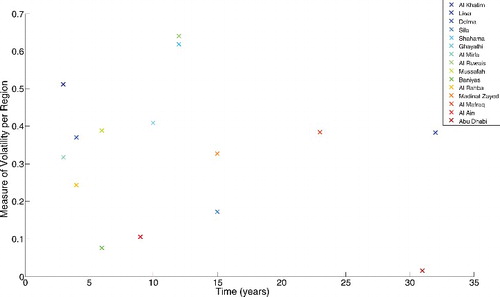
5.4 Controlling Healthcare Human Resources Regional Capacity
Naturally, with such aggressive growth rates in all regions, it is not surprising that shows elevated volatility measures in nearly all regions. Two notable exceptions are the city of Abu Dhabi and the neighboring Baniyas. In these two regions, HRM practices seem to have matured sufficiently to be able to control the volatility in regional capacity to a very low rate. The root cause factors behind these low volatility values should be thoroughly investigated so that the associated best practices can be transplanted to other regions.
5.5 Retention of Healthcare Knowledge
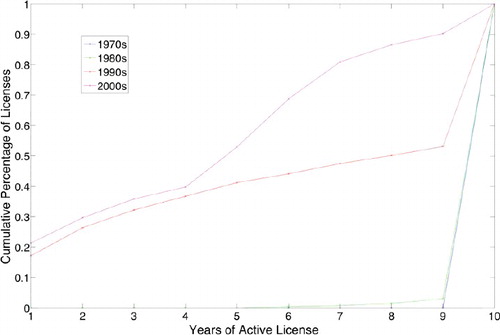
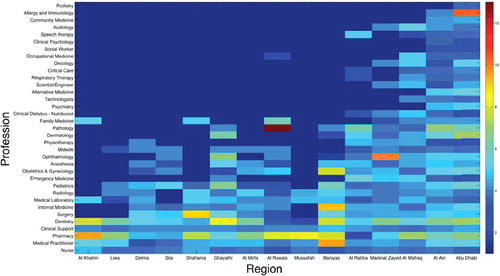
In this subsection, retention of healthcare knowledge is assessed in terms of the average number of active license times. While the previous subsections addressed the growth rate and volatility of healthcare professionals, it is equally important to address the specific issue of retention of local human capital. shows the turnover of healthcare human resources per decade. presents the average license times for each profession per region.
There appear to be very different patterns of turnover between the oldest decades of the 1970s and 1980s and the newest decades of the 1990s and 2000s. The older decades retained healthcare professionals very well, while the more recent decades have progressively shorter active license times. Quantitatively, since the 1990s, approximately 25% of healthcare professionals decide to leave within 2 years of service in the emirate of Abu Dhabi. Put in context with the previous discussions, these figures suggest that the more recent attempts toward functional and regional diversification may actually prove less effective—with more recent healthcare professionals deciding to stay for relatively shorter periods of time.
The retention picture may also be addressed regionally. Pharmacy has the highest average license times across the regions of the Abu Dhabi emirate, closely followed by dentistry. These are the two professions that appear in all regions. Interestingly, the less urban areas of Al Khatim, Baniyas, Liwa, and Ghayathi appear to retain their healthcare professions longer than the more urban regions. The healthcare enterprise can investigate what makes these regions more successful in retaining their healthcare professionals relative to others.
6 CONCLUSIONS AND FUTURE WORK
In conclusion, this article has modeled healthcare professionals in the emirate of Abu Dhabi as a large flexible system, the functions of which are healthcare professions. The physical hierarchy was modeled at the level of individuals, then aggregated to healthcare facilities, and then aggregated further to the regional level. Recruiting and attrition were modeled as reconfiguration processes that allowed for a discrete-time evolution of the system knowledge base. The results showed Abu Dhabi's aggressive efforts to develop its healthcare human resources capital and improve the QoS despite high attrition rates and the quickly growing population. The results also showed a trend toward improving the flexibility of facilities, consistently in larger cities while abruptly in recent years in more rural areas. The data also showed a continually deteriorating ability to retain healthcare professionals in recent decades, especially in more urban areas. The precision of these results can be instructive from the enterprise transformation perspective and should serve decision makers to develop HRM policies that stabilize healthcare QoS, facility convenience, and human resources retention where it is needed most.
The article's results demonstrate the significant potential of the axiomatic design knowledge bases in the application of HRM. The knowledge base, when viewed at multiple levels of physical hierarchy and dynamically over time, allows for data-centric methods that can support enterprise transformation in an environment of rapid growth.
REFERENCES
- Abadir, K.M., and Magnus, J.R. (2005). Matrix algebra. Econometric exercises. Cambridge, UK: Cambridge University Press.
- Afifi, S.S. (1991). Factors affecting professional employee retention. Journal of Management in Engineering, 7(2), 187–202.
- Ang, S., and Slaughter, S. (2004). Turnover of information technology professionals: The effects of internal labor market strategies. Data Base for Advances in Information Systems, 35(3), 11–27.
- Anonymous. (2013). Abu Dhabi. Retrieved from http://en.wikipedia.org/wiki/Abu_dhabi
- Armstrong-Stassen, M., and Schlosser, F. (2011). Perceived organizational membership and the retention of older workers. Journal of Organizational Behaviour, 32(2), 319–344.
- Baca, E.E. S., Farid, A.M., Tsai, I.-T., and Viswanath, A. (2013). An axiomatic design approach to passenger itinerary enumeration in reconfigurable transportation systems. Proceedings of the Seventh International Conference on Axiomatic Design (ICAD2013) (pp. 1–10), Worchester, MA, June 26–28.
- Barjis, J. (2011). Enterprise modeling and simulation within enterprise engineering. Journal of Enterprise Transformation, 1(3), 185–207.
- Barney, J. (1991). Firm resources and sustained competitive advantage. Journal of Management, 17(1), 99–120.
- Basole, R.C., Bellamy, M., Clear, T., Dabkowski, M., Monreal, J., Park, H., Valerdi, R., and Van Aken, E. (2013). Challenges and opportunities for enterprise transformation research. Journal of Enterprise Transformation, 3(4), 330–352.
- Basole, R.C., Braunstein, M.L., and Rouse, W.B. (2012). Enterprise transformation through mobile ICT: A framework and case study in healthcare. Journal of Enterprise Transformation, 2(2), 130–156.
- Beulen, E. (2009). The contribution of a global service provider's human resources information system (HRIS) to Staff retention in emerging markets: Comparing issues and implications in six developing countries. Information Technology & People, 22(3), 270–288.
- Boland, A.S. (1998). Recruiting and retaining IT staff. Health Management Technology, 19(5), 74–77.
- Brown, S.L., and Eisenhardt, K.M. (1998). Competing on the edge: Strategy as structured chaos. Boston, MA: Harvard Business School Press.
- Budhwar, P.S., Varma, A., Malhotra, N., and Mukherjee, A. (2009). Insights into the Indian call centre industry: Can Internal marketing help tackle high employee turnover?” Journal of Services Marketing, 23(5), 351–362.
- Chew, J., and Chan, C.C. A. (2008). Human resource practices, organizational commitment and intention to stay. International Journal of Manpower, 29(6), 503–522.
- Chien, C.-F., and Chen, L.-F. (2008). Data mining to improve personnel selection and enhance human capital: A case study in high-technology industry. Expert Systems with Applications, 34(1), 280–290.
- Clarke, L., and Herrmann, G. (2007). Skill shortages, recruitment and retention in the house building sector. Personnel Review, 36(4), 509–527.
- Cuny, J., and Aspray, W. (2002). Recruitment and retention of women graduate students in computer science and engineering: Results of a workshop organized by the Computing Research Association. SIGCSE Bulletin, 34(2), 168–174.
- Dabkowski, M.F., Huddleston, S.H., Kucik, P., and Lyle, D.S. (2011). Shaping senior leader officer talent: Using a multi-dimensional model of talent to analyze the effect of personnel management decisions and attrition on the flow of army officer talent throughout the officer career model. Proceedings of the 2011 Winter Simulation Conference (WSC 2011) (pp. 2466–2477). Fort Leavenworth, KS, December 11–14, 2011.
- Doh, J.P., Smith, R.R., Stumpf, S.A., and Tymon Jr., W.G. (2011). Pride and professionals: Retaining talent in emerging economies. Journal of Business Strategy, 32(5), 35–42.
- Dori, D. (2002). Object–process methodology: A holistics systems paradigm. Berlin, Germany: Springer.
- Farid, A.M. (2007). Reconfigurability measurement in automated manufacturing systems. University of Cambridge Engineering Department Institute for Manufacturing. Retrieved from http://amfarid.scripts.mit.edu/resources/RMS-T01.pdf
- Farid, A.M. (2008). Product degrees of freedom as manufacturing system reconfiguration potential measures. International Transactions on Systems Science and Applications, 4(3), 227–242. Retrieved from http://amfarid.scripts.mit.edu/resources/RMS-J03.pdf
- Farid, A.M. (2013). An axiomatic design approach to non-assembled production path enumeration in reconfigurable manufacturing systems. 2013 IEEE International Conference on Systems Man and Cybernetics (pp. 1–8). Manchester, UK, October 13–16.
- Farid, A.M. (2014a). Axiomatic design & design structure matrix measures for reconfigurability & its key characteristics in automated manufacturing systems. International Conference on Axiomatic Design (pp. 1–8). Campus de Caparica, Portugal, September 24–26.
- Farid, A.M. (2014b). Multi-agent system design principles for resilient operation of future power systems. IEEE International Workshop on Intelligent Energy Systems (pp. 1–7). San Diego, CA, October 8.
- Farid, A.M. (2014c). Static resilience of large flexible engineering systems: Part I—Axiomatic design model. 4th International Engineering Systems Symposium (pp. 1–8). Hoboken, NJ, June 8–11. Retrieved from http://amfarid.scripts.mit.edu/resources/CESUN1.pdf
- Farid, A.M., and Covanich, W. (2008). Measuring the effort of a reconfiguration process.IEEE International Conference on Emerging Technologies and Factory Automation (ETFA) (pp. 1137–1144). Hamburg, Germany, September 15–18.
- Farid, A.M., and Khayal, I.S. (2013). Axiomatic design based volatility assessment of the Abu Dhabi healthcare labor market: Part I—Theory. Proceedings of the Seventh International Conference on Axiomatic Design (ICAD 2013) (pp. 1–8). Worcester, MA, June 26–28.
- Farid, A.M., and McFarlane, D.C. (2008). Production degrees of freedom as manufacturing system reconfiguration potential measures. Proceedings of the Institution of Mechanical Engineers, Part B (Journal of Engineering Manufacture), 222(B10), 1301–1314.
- Farid, A.M., and Ribeiro, L. (2014). An axiomatic design of a multi-agent reconfigurable manufacturing system architecture. International Conference on Axiomatic Design (pp. 1–8). Lisbon, Portugal, September 15–18.
- Finegold, D., Levenson, A., and Van Buren, M. (2005). Access to training and its impact on temporary workers. Human Resource Management Journal (UK), 15(2), 66–85.
- Foy, F.P., and Iwaszek, G. (1996). Workforce development-building the public education pipeline to meet manufacturing technician hiring needs. IEEE/SEMI 1996 Advanced Semiconductor Manufacturing Conference and Workshop (pp. 451–454), Cambridge, MA, November 12–14.
- Fry, T.D., Kher, H.V., and Malhotra, M.K. (1995). Managing worker flexibility and attrition in dual resource constrained job shops. International Journal of Production Research, 33(8), 2163–2179.
- Ghosh, K., and Sahney, S. (2010). Organizational sociotechnical diagnosis of managerial retention in an IT organization: SAP-LAP framework. International Journal of Organizational Analysis, 18(1), 151–166.
- Gilbert III, L., Farid, A.M., and Omar, M. (2013). An axiomatic design based approach for the conceptual design of temporary modular housing. Proceedings of the Seventh International Conference on Axiomatic Design (ICAD 2013) (pp. 146–153). Worcester, MA, June 26–28.
- Gow, K., Warren, C., Anthony, D., and Hinschen, C. (2008). Retention and intentions to quit among Australian male apprentices. Education + Training, 50(3), 216–230.
- Grant, R.M. (1996). Toward a knowledge-based theory of the firm. Strategic Management Journal, 17(SI), 109–122.
- Han, Z., and Froese, F.J. (2010). Recruiting and retaining RD professionals in China. International Journal of Technology Management, 51(2–4), 387–408.
- Hanewicz, C. (2009). Identifying student retention patterns using GIS technology. Portland International Conference on Management of Engineering and Technology, Orem, UT, August 2–6.
- Health Authority of Abu Dhabi. (2013). Clinical Licenses. Shafafiya Website. Retrieved from http://www.shafafiya.org/dictionary/portal
- Holtbrugge, D., Friedmann, C.B., and Puck, J.F. (2010). Recruitment and retention in foreign firms in India: A resource-based view. Human Resource Management, 49(3), 439–455.
- Horwitz, F.M. (2011). Future HRM challenges for multinational firms in eastern and central Europe. Human Resource Management Journal, 21(4), 432–443.
- Jin, C., and Li-ying, W. (2003). Flow and retention of intellectual employees in hi-tech companies. Proceedings. Managing Technologically Driven Organizations: The Human Side of Innovation and Change (IEMC ‘03). Zhejiang University, China, November 2–4.
- Kaliprasad, M. (2006). The human factor I: Attracting, retaining, and motivating capable people. Cost Engineering, 48(6), 20–26.
- Kapoor, B., and Sherif, J. (2012). Global human resources (HR) information systems. Kybernetes, 41(1–2), 229–238.
- Khayal, I.S., and Farid, A.M. (2013). Axiomatic design based volatility assessment of the Abu Dhabi healthcare labor market: Part II—Case study. Proceedings of the Seventh International Conference on Axiomatic Design (ICAD) (pp. 1–8). Worcester, MA, June 26–28.
- Lee-Kelley, L., Blackman, D.A., and Hurst, J.P. (2007). An exploration of the relationship between learning organisations and the retention of knowledge workers. Learning Organization, 14(3), 204–221.
- Leonard-Barton, D. (1992). Core capabilities and core rigidities: A paradox in managing new product development. Strategic Management Journal (1986–1998), 13(special issue), 111–125.
- Lockwood, D., and Ansari, A. (1999). Recruiting and retaining scarce information technology talent: A focus group study. Industrial Management + Data Systems, 99(6), 251–256.
- Lubega, W.N., and Farid, A.M. (2014). A reference system architecture for the energy–water nexus. IEEE Systems Journal, PP(99), 1–11.
- Maier, M.W. (1998). Architecting principles for systems-of-systems. Systems Engineering, 1(4), 267–284.
- Nicolopoulou, K. (2011). Towards a theoretical framework for knowledge transfer in the field of CSR and sustainability. Equality, Diversity and Inclusion: An International Journal, 30(6), 524–538.
- Niskanen, W.A. (1991). The soft infrastructure of a market economy. Cato Journal, 11(2), 233–238.
- Nonaka, I.O., and Nishiguchi, T. (2001). Knowledge emergence: Social, technical, and evolutionary dimensions of knowledge creation. Oxford, UK: Oxford University Press.
- Nonaka, I.O., and Takeuchi, H. (1995). The knowledge-creating company: How Japanese companies create the dynamics of innovation. Oxford, UK: Oxford University Press.
- Oliver, D.W., Kelliher, T.P., and Keegan, J.G. (1997). Engineering complex systems with models and objects. New York, NY: McGraw-Hill.
- Pathirage, C.P., Amaratunga, D.G., and Haigh, R.P. (2007). Tacit knowledge and organisational performance: Construction Industry Perspective. Journal of Knowledge Management, 11(1), 115–126.
- Pettigrew, A.M., Thomas, H., and Whittington, R. (2006). Handbook of strategy and management. London; Thousand Oaks, CA: Sage Publications.
- Roepke, R., Agarwal, R., and Ferratt, T.W. (2000). Aligning the IT human resource with business vision: The leadership initiative at 3M. MIS Quarterly: Management Information Systems, 24(2), 327–353.
- Servon, L.J., and Visser, M.A. (2011). Progress hindered: The retention and advancement of women in science, engineering and technology careers. Human Resource Management Journal, 21(3), 272–284.
- Shah, S.F. H., Nazir, T., Zaman, K., and Shabir, M. (2013). Factors affecting the growth of enterprises: A survey of the literature from the perspective of small- and medium-sized enterprises. Journal of Enterprise Transformation, 3(2), 53–75.
- Spender, J.C. (1996). Making knowledge the basis of a dynamic theory of the firm. Strategic Management Journal, 17(SI), 45–62.
- Statistics Center of Abu Dubai (SCAD). (2013). Abu Dhabi Development Statistics-Population and Labour Force: Population and Demography. Abu Dhabi, UAE.
- Suh, N.P. (2001). Axiomatic design: Advances and applications. Oxford, UK: Oxford University Press.
- Sveiby, K.-E. (2001). A knowledge-based theory of the firm to guide in strategy formulation. Journal of Intellectual Capital, 2(4), 344–358.
- Taylor III, L.J., Murphy, B., and Price, W. (2006). Goldratt's thinking process applied to employee retention. Business Process Management Journal (UK), 12(5), 646–670. doi 10.1108/14637150610691055
- Teece, D.J., Pisano, G., and Shuen, A. (1997). Dynamic capabilities and strategic management. Strategic Management Journal, 18(7), 509–533.
- Viswanath, A., Baca, E.E. S., and Farid, A.M. (2013). An axiomatic design approach to passenger itinerary enumeration in reconfigurable transportation systems. IEEE Transactions on Intelligent Transportation Systems, 15(3), 915–924.
- Viswanath, A., and Farid, A.M. (2014). A hybrid dynamic system model for the assessment of transportation electrification. 2014 American Control Conference (pp. 1–7). Portland, OR, June 4–6.
- Wenger, N., Antoniev, A., and Gorod, A. (2013). The international space station: Applying system of systems methodology. 2013 8th International Conference on System of Systems Engineering (pp. 235–242). Maui, HI, June 2–6.
- Wernerfelt, B. (1995). The resource-based view of the firm: Ten years after. Strategic Management Journal (1986–1998), 16(3), 171.
- Whelan, E., and Carcary, M. (2011). Integrating talent and knowledge management: Where are the benefits? Journal of Knowledge Management (UK), 15(4), 675–687.
- Wong, D., and Kimura, R. (2009). Replenishing the aging work force in the power industry. 2009 IEEE Power Energy Society General Meeting (PES), July 26–30.
- Zheng, C., and Hu, M.-C. (2008). Challenge to ICT manpower planning under the economic restructuring: Empirical evidence from MNCs in Singapore and Taiwan. Technological Forecasting and Social Change, 75(6), 834–853.
- Zheng, C., Soosay, C., and Hyland, P. (2008). Manufacturing to Asia: Who will win the emerging battle for talent between dragons and tigers? Journal of Manufacturing Technology Management, 19(1), 52–72. doi 10.1108/17410380810843453