
ABSTRACT
This study evaluated the technical quality of root canal treatment (RCT) and detected iatrogenic errors in an undergraduate dental clinic at the College of Dentistry, Taibah University, Saudi Arabia. Dental records of 280 patients who received RCT between 2013 and 2016 undertaken by dental students were investigated by retrospective chart review. Root canal obturation was evaluated on the basis of the length of obturation being ≤2 mm from the radiographic apex, with uniform radiodensity and good adaptation to root canal walls. Inadequate root canal obturation included cases containing procedural errors such as furcal perforation, ledge, canal transportation, strip perforation, root perforation, instrument separation, voids in the obturation, or underfilling or overfilling of the obturation. In 193 (68.9%) teeth, RCT was adequate and without procedural errors. However, in 87 (31.1%) teeth, RCT was inadequate and contained procedural errors. The frequency of procedural errors in the entire sample was 31.1% as follows: underfilling, 49.9%; overfilling, 24.1%; voids, 12.6%; broken instruments, 9.2%; apical perforation, 2.3%; and root canal transportation, 2.3%. There were no significant differences (p > 0.05) in the type or frequency of procedural errors between the fourth- and fifth-year students. Lower molars (43.1%) and upper incisors (19.2%) exhibited the highest and lowest frequencies of procedural errors, respectively. The technical quality of RCT performed by undergraduate dental students was classified as ‘adequate’ in 68.9% of the cases. There is a need for improvement in the training of students at the preclinical and clinical levels.
Responsible Editor Omran Bakoush, Sweden
1. Introduction
Nonsurgical root canal treatment (RCT) is an important element of comprehensive dental healthcare [Citation1,Citation2]. Previous studies have reported success rates >90% for nonsurgical RCT under controlled conditions [Citation3,Citation4]. However, this high success rate has been reported to decrease to 40–65% in cases where RCT is performed by general practitioners[Citation5]. This decrease can be attributed to the inadequacy of educational programs and lack of self-confidence in performing root canal procedures [Citation6,Citation7]. Therefore, it is important to improve undergraduate programs, where it is possible to recognize the reasons that affect the success of dental treatments [Citation8,Citation9].
Radiographic evaluation is a common method for assessing the technical quality of RCT [Citation10,Citation11]. This assessment process is important because the quality of root canal obturation greatly affects the prognosis of therapy [Citation9,Citation12]. Several factors determine the technical quality of root canal obturation, including the distance between the end of the root canal obturation material and the root apex, density, presence of voids, and taper. Radiographic evaluation of root canal obturation depends on these factors [Citation13,Citation14]. The radiographic appearance of an appropriate root canal obturation is characterized by a uniformly tapered canal from the coronal to apical ends, a dense root canal obturation without voids, and presence of filling materials 0.5–2 mm below the radiographic apex [Citation15]. In root canal obturation, each 1-mm loss of working length in teeth with apical periodontitis increases the failure rate by 14% [Citation16]. Underfilling and overfilling of a root canal obturation will also compromise the success rate of RCT [Citation17]. In addition, other iatrogenic errors such as instrument fracture, ledge formation, and apical perforations can cause failure of nonsurgical RCT [Citation4,Citation18].
Several studies have reported the adequacy of RCT performed by undergraduate students as varying between 33% and 70% [Citation13,Citation19]. Assessment of treatment quality and frequency of procedural errors will help improve educational programs and enhance health services [Citation14,Citation20].
Dental students at Taibah University undertake a preclinical full-year endodontic course in the third year of their six-year Bachelor of Dental Surgery course. The endodontic course involves 28 h of theoretical lectures and 56 h of laboratory training during which the students perform technical procedures of RCT on extracted teeth. The clinical course is a one-semester clinical endodontic course in the fourth year; it involves 14 h of theoretical lectures and 42 h of clinical sessions during which students treat single- and multi-rooted teeth. In this course, the students perform three to six cases (one to two interior teeth, one to two premolars, and one to two molars). In the fifth year, endodontic treatments are performed as part of a comprehensive dentistry-care course under the supervision of specialists.
This study radiographically evaluated the technical quality and frequency of complications in RCTs performed by undergraduate dental students at the College of Dentistry, Taibah University, Saudi Arabia, between 2013 and 2016.
2. Materials and methods
2.1. Case selection
This study was approved by the Research Ethics Committee of the College of Dentistry, Taibah University (reference no. TUCDREC/20,160,217/ALRAHABI).
The dental records of 280 patients who received RCT performed by dental students (fourth-year students, 131 patients; fifth [final]-year students, 149 patients) at the College of Dentistry were investigated by performing a retrospective chart review. The study sample was randomly selected from records between 2013 and 2016.
RCTs were performed with the step-back instrumentation technique using stainless steel K-files of 0.02 taper. Root canals were irrigated with 2.5% sodium hypochlorite. Root canal obturation was performed with the lateral condensation technique. Radiographs were exposed using the bisecting-angle technique.
2.2. Evaluation of complications of RCT
Two endodontists with >7 years of experience evaluated the technical quality and procedural errors of RCT in the records. In case of controversy, a third investigator was asked to evaluate the radiographs, and a final decision was reached. The examiners used the following criteria for evaluation: adequate root canal obturation – length of root canal obturation ≤2 mm from the radiographic apex, with uniform radiodensity and good adaptation to root canal walls; inadequate root canal obturation – any case containing a procedural error was considered inadequate.
RCT complications were classified as follows. For errors during access cavity preparation, furcal perforation was identified when obturation material extruded through the furcation area and was radiographically detected in multi-rooted teeth. For errors during root canal instrumentation, ledges were identified when the root canal obturation did not follow the original shape of the canal in teeth with curved root canals. Transportation was identified when obturation material extruded away from the curve of the canal. Strip perforation was identified when obturation material extruded in the lateral (inner) wall of both buccal roots of maxillary molars, mesial and distal roots of mandibular molars, and in any root of other teeth. Root perforation was identified when obturation material extruded in any area of a root except the furcation area in multi-rooted teeth. Instrument separation was identified when a radiopaque fractured instrument segment was detected in the root canal or extended into the periapical area in X-ray radiographs. For errors during root canal obturation, voids were identified when visible voids within the root canal obturation mass could be detected on X-ray radiographs. Overfilling was determined when root canal obturation material extruded beyond the apex. Underfilling was determined when root canal obturation was shorter than the radiographic apex by ≤2 mm.
2.3. Statistical analysis
Statistical analyses of data were performed using IBM SPSS Statistics for Windows v20 (IBM Corp., Armonk, NY). Statistical significance was set at p < 0.05. The chi-square test was used to determine statistically significant differences in the technical quality of RCTs and frequency of procedural errors between the two academic levels and among tooth types.
3. Results
3.1. Technical quality of root canal obturation
A total of 280 records of endodontically treated teeth were evaluated. In all of these cases, RCT was performed by undergraduate dental students at Taibah University during the academic years 2013–2016. presents the distribution of cases according to academic level and tooth type.
Table 1. Distribution of treated teeth according to academic level
In 193 (68.9%) teeth, RCT was determined to be adequate and without procedural errors. However, in 87 (31.1%) teeth, the treatment was inadequate and contained procedural errors. Among the teeth treated by fourth-year students, 90 (68.7%) had received adequate treatment, whereas 41 (31.3%) teeth exhibited procedural errors. Among teeth treated by fifth-year students, 103 (69.1%) had received adequate treatment, whereas 46 (30.9%) teeth exhibited procedural errors. presents the results of technical quality assessment of endodontically treated teeth.
Table 2. Technical quality of treated teeth according to tooth type and academic level
3.2. Iatrogenic errors
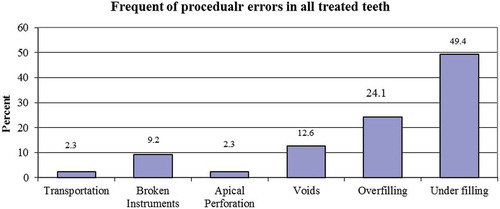
The overall frequency of procedural errors was 31.1%. The frequencies of procedural errors were as follows: underfilling of the obturation, 49.9%; overfilling of the obturation, 24.1%; voids in the obturation, 12.6%; broken instruments, 9.2%; apical perforation, 2.3%; and root canal transportation, 2.3%. presents the frequencies of procedural errors in all of the treated teeth.
Figure 1. Frequency of procedural errors in all treated teeth.
3.3. Effect of academic level on frequency and type of procedural errors
The frequencies of procedural errors among teeth treated by the fourth- and fifth-year students were 30.9% and 31.1%, respectively. Underfilling of root canal obturation was the most frequent error among both the fourth- (51.2%) and fifth-year (47.8%) students. Apical perforation and transportation were the least frequent procedural errors among both the fourth- (2.4%) and fifth-year (2.2%) students. Procedural errors in lower incisors were significantly more frequent among the fifth-year students (66.7%) than among the fourth-year students (p < 0.01). There were no significant differences (p > 0.05) between the two groups of students in the type or frequency of procedural errors in the overall sample. presents the frequency and type of procedural errors among the fourth- and fifth-year students.
Table 3. Frequency and type of procedural errors according to academic level
3.4. Effect of tooth type on frequency and type of procedural errors
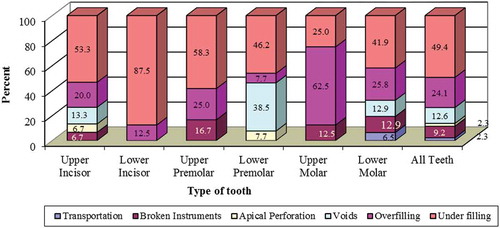
In the overall sample, lower molars exhibited the highest frequency of procedural errors (43.1%), while upper incisors exhibited the lowest frequency (19.2%). Relative to other teeth, upper molars exhibited a significantly higher frequency (p < 0.05) of overfilling of root canal obturation. There were no significant differences in procedural error frequencies among the other teeth. presents the frequencies and types of each procedural error in each tooth type.
Figure 2. Types and frequencies of procedural errors in each tooth type.
4. Discussion
This study was conducted to evaluate the technical quality and complications of RCT performed by undergraduate dental students at the author’s institution between 2013 and 2016. Evaluations were made using postoperative periapical radiographs. Radiographs exhibiting superimposition of tooth structure on root canal obturation and anatomical structures were excluded from the study sample to ensure that there was no confusion in radiographic interpretation. Radiographic criteria for quality of RCT were established in accordance with the European guidelines and previous studies on outcome of RCT performed by dental undergraduates [Citation9,Citation21]. In 68.9% of the cases in the present study, RCT was without procedural errors and exhibited technically adequate root canal obturation. This result differs somewhat from the results of other studies, where the proportion of technically adequate root canal obturation varied from 13% to 60.4% [Citation22,Citation23]. These differences might be the result of differences in evaluation criteria, materials, educational system, methodology, and sample size between the present and previous studies. In addition, 31.1% of the treated teeth in the present study exhibited procedural errors. There were no significant differences between the fourth- and fifth-year students in the quality of root canal obturation or frequency of procedural errors in the present data set. This indicates that the outcome was not affected by the academic level. Similar results were reported by Khabbaz et al. in Greece [Citation9] and Unal et al. in Turkey [Citation13].
In the present study, the fifth-year students exhibited a higher frequency of procedural errors in lower incisors than the fourth-year students. This might have been because the number of lower incisors treated by the fifth-year students was higher than that treated by the fourth-year students. This difference might also have resulted from the fifth-year students having less experience with lower incisors in preclinical training.
Upper incisors exhibited the lowest frequency of procedural errors (19.2%). Similar results were found in other studies [Citation21,Citation24]. This high rate of adequate RCT in upper incisors might simply be attributable to the anatomy of the upper incisor and its anterior position, which make isolation and treatment relatively easy. Alternatively, this result might have been because of intensive training in the preclinical stage. Procedural errors were the most frequent in lower molars (43.1%). Other studies have also reported molars, particularly lower molars, as generally exhibiting the lowest percentage of adequate RCT and more frequent procedural errors [Citation9,Citation25]. This might be attributable to the anatomical complexity of molars or insufficient training in the preclinical stage. Therefore, there is a need to review current educational programs to improve student skills in RCT for molars.
Underfilling of root canal obturation was the most frequent procedural error (49.4%) in the present study. This error resulted from inaccuracies in working length determination, where the students determined the working length on the basis of X-ray findings alone, without using an electronic apex locator. Several studies have reported that the accuracy of electronic apex locators has reached 97% [Citation26,Citation27]. The techniques taught for cleaning and shaping included the step-back technique with stainless steel K-files and lateral condensation for root canal obturation. The sequence of application of stainless steel instruments starts from the apical end of the canal and proceeds to the coronal part, which can lead to iatrogenic damage to the original canal. It may also cause instrumentation mishaps such as ledges, blocking, and root canal transportation, which will reduce the efficiency of cleaning and shaping, increase the probability of underfilling root canal obturation [Citation28], and cause adverse effects on prognosis [Citation25]. Nickel–titanium (NiTi) rotary instruments for endodontic practice have been considered revolutionary. Today, NiTi instruments are preferred over stainless steel hand files because of the ability of the former to maintain the original curvature of the canal [Citation29]. Because of the relatively high incidence of procedural errors when using stainless steel files, the success rates of procedures performed with stainless steel instruments are also lower than those of procedures performed with NiTi rotary files [Citation25,Citation30].
In the present study, upper molars were overfilled more frequently than other teeth. In contrast, other studies have reported the quality of root canal obturation of maxillary teeth to be better than that of mandibular teeth [Citation1]. Overfilling can result from missing the apical stop during cleaning and shaping because of the lack of length control on stainless steel files. Modification of the endodontic curriculum and increasing the number of specialized staff members and training time for preclinical and clinical endodontic courses are important elements for improving student competency in endodontics. It will be useful to reevaluate the technical quality and procedural errors of RCTs performed by undergraduate dental students in the future to determine the effects of educational program modifications.
5. Conclusions
In this study, the technical quality of RCT performed by undergraduate dental students was classified as ‘adequate’ in 68.9% of cases. The overall frequency of complications in RCT was 31.1%. The most frequent error was underfilling of root canal obturation, and the tooth type with the highest number of procedural errors was the lower molar. There were no significant differences between the fourth- and fifth-year students in the type or frequency of procedural errors. It is suggested that these issues be addressed in the dentistry program at the College of Dentistry, Taibah University, to improve the training of students at the preclinical and clinical levels. In addition, this research should be repeated to assess the effects of any changes that are made in the future.
Acknowledgments
This study was supported by the Department of Restorative Dentistry Science, College of Dentistry, Taibah University, Saudi Arabia. The author thanks Drs. Ayman Alkady and M Sohail Zafar for their help in evaluating X-ray radiographs.
Disclosure statement
No potential conflict of interest was reported by the author.
References
- Barrieshi-Nusair K, Al-Omari M, Al-Hiyasat A. Radiographic technical quality of root canal treatment performed by dental students at the Dental Teaching Center in Jordan. J Dent. 2004;1132(4):1–6.
- Er O, Sagsen B, Maden M, et al. Radiographic technical quality of root fillings performed by dental students in Turkey. Int Endod J. 2006;39(11):867–872.
- Friedman S, Mor C. The success of endodontic therapy—healing and functionality. J Calif Dent Assoc. 2004;32(6):493–503.
- Imura N, Pinheiro ET, Gomes BP, et al. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007;33(11):1278–1282.
- Sunay H, Tanalp J, Dikbas I, et al. Cross-sectional evaluation of the periapical status and quality of root canal treatment in a selected population of urban Turkish adults. Int Endod J. 2007;40(2):139–145.
- Jenkins S, Hayes S, Dummer P. A study of endodontic treatment carried out in dental practice within the UK. Int Endod J. 2001;34(1):16–22.
- Stewardson D. Endodontics and new graduates: part I, practice vs. training. Eur J Prosthodont Restor Dent. 2002;10(3):131–137.
- Moor R, Hülsmann M, Kirkevang LL, et al. Undergraduate curriculum guidelines for endodontology. Int Endod J. 2013;46(12):1105–1114.
- Khabbaz M, Protogerou E, Douka E. Radiographic quality of root fillings performed by undergraduate students. Int Endod J. 2010;43(6):499–508.
- Hansrani V. Assessing root canal fillings on a radiograph–an overview. Br Dent J. 2015;219(10):481–483.
- Tsuneishi M, Yamamoto T, Yamanaka R, et al. Radiographic evaluation of periapical status and prevalence of endodontic treatment in an adult Japanese population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;100(5):631–635.
- Moussa-Badran S, Roy B, Bessart du Parc A, et al. Technical quality of root fillings performed by dental students at the dental teaching centre in Reims, France. Int Endod J. 2008;41(8):679–684.
- Unal GC, Kececi AD, Kaya BU, et al. Quality of root canal fillings performed by undergraduate dental students. Eur J Dent. 2011;5(3):324–330.
- Abu-Tahun I, Al-Rabab’ah MA, Hammad M, et al. Technical quality of root canal treatment of posterior teeth after rotary or hand preparation by fifth year undergraduate students, The University of Jordan. Aust Endod J. 2014;40(3):123–130.
- Loest C. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921–930.
- Chugal NM, Clive JM, Spångberg LS. Endodontic infection: some biologic and treatment factors associated with outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;96(1):81–90.
- Kabak Y, Abbott P. Prevalence of apical periodontitis and the quality of endodontic treatment in an adult Belarusian population. Int Endod J. 2005;38(4):238–245.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30(8):559–567.
- Rafeek RN, Smith WA, Mankee MS, et al. Radiographic evaluation of the technical quality of root canal fillings performed by dental students. Aust Endod J. 2012;38(2):64–69.
- Motamedi MRK, Davoodi SHR, Saeidi A, et al. Technical quality of root canal therapies performed by novice dental students in preclinical practice. Dent Res J. 2015;12(4):365–371.
- Eleftheriadis G, Lambrianidis T. Technical quality of root canal treatment and detection of iatrogenic errors in an undergraduate dental clinic. Int Endod J. 2005;38(10):725–734.
- Balto H, Al Khalifah S, Al Mugairin S, et al. Technical quality of root fillings performed by undergraduate students in Saudi Arabia. Int Endod J. 2010;43(4):292–300.
- Elsayed RO, Abu-Bakr NH, Ibrahim YE. Quality of root canal treatment performed by undergraduate dental students at the University of Khartoum, Sudan. Aust Endod J. 2011;37(2):56–60.
- Lynch C, Burke F. Quality of root canal fillings performed by undergraduate dental students on single-rooted teeth. European J Dent Educ. 2006;10(2):67–72.
- Cheung GS, Liu CS. A retrospective study of endodontic treatment outcome between nickel-titanium rotary and stainless steel hand filing techniques. J Endod. 2009;35(7):938–943.
- Pascon EA, Marrelli M, Congi O, et al. An ex vivo comparison of working length determination by 3 electronic apex locators. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(3):e147–51.
- Bernardes RA, Duarte MA, Vasconcelos BC, et al. Evaluation of precision of length determination with 3 electronic apex locators: root ZX, Elements Diagnostic Unit and Apex Locator, and RomiAPEX D-30. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(4):e91–4.
- Kfir A, Rosenberg E, Zuckerman O, et al. Comparison of procedural errors resulting during root canal preparations completed by senior dental students in patients using an ‘8-step method’ versus ‘serial step-back technique’. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004;97(6):745–748.
- Taşdemir T, Aydemir H, Inan U, et al. Canal preparation with Hero 642 rotary Ni–Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J. 2005;38(6):402–408.
- Schäfer E, Bürklein S. Impact of nickel–titanium instrumentation of the root canal on clinical outcomes: A focused review. Odontology. 2012;100(2):130–136.