ABSTRACT
Background: The gold standard for COVID-19 diagnosis relies on quantitative reverse-transcriptase polymerase-chain reaction (RT-qPCR) from nasopharyngeal swab (NPS) specimens, but NPSs present several limitations. The simplicity, low invasive and possibility of self-collection of saliva imposed these specimens as a relevant alternative for SARS-CoV-2 detection. However, the discrepancy of saliva test results compared to NPSs made of its use controversial. Here, we assessed Salivettes®, as a standardized saliva collection device, and compared SARS-CoV-2 positivity on paired NPS and saliva specimens.
Methods: A total of 303 individuals randomly selected among those investigated for SARS-CoV-2 were enrolled, including 30 (9.9%) patients previously positively tested using NPS (follow-up group), 90 (29.7%) mildly symptomatic and 183 (60.4%) asymptomatic.
Results: The RT-qPCR revealed a positive rate of 11.6% (n = 35) and 17.2% (n = 52) for NPSs and saliva samples, respectively. The sensitivity and specificity of saliva samples were 82.9% and 91.4%, respectively, using NPS as reference. The highest proportion of discordant results concerned the follow-up group (33.3%). Although the agreement exceeded 90.0% in the symptomatic and asymptomatic groups, 17 individuals were detected positive only in saliva samples, with consistent medical arguments.
Conclusion Saliva collected with Salivette® was more sensitive for detecting symptomatic and pre-symptomatic infections.
Notes on contributions
Conceived and designed the experiments: LA. Performed the experiments: MMC, NB, LA. Analyzed the data: LA, SG, MMC. Contributed with reagents/materials/analysis tools: MMC, SG, JD, RA, NG, HTD, MM. Sample collections: LA, JD, RA, NG. Drafted the paper: LA. Revised critically the paper: all the authors.
Acknowledgments
We would like to acknowledge the IHU Mediterranean Infection nurse staff for their reception in the routine test rooms and all the participants who accepted to donate saliva. We also acknowledge Catherine Verret and Carine Malle (DFRI, SSA, Paris) for their help in the redaction of the ethical statement folder.
Disclosure statement
The authors declare that they have no competing interests.
List of abbreviations
NPS: nasopharyngeal swab; PCR: Polymerase Chain Reaction; Ct: Cycle threshold; RT-qPCR: Reverse transcription quantitative real-time PCR; SARS-CoV-2: Severe Acute Respiratory Syndrome Coronavirus 2; COVID-19: Coronavirus Disease 2019: PPA: positive percent agreement.
Supplementary material
Supplemental data for this article can be accessed here
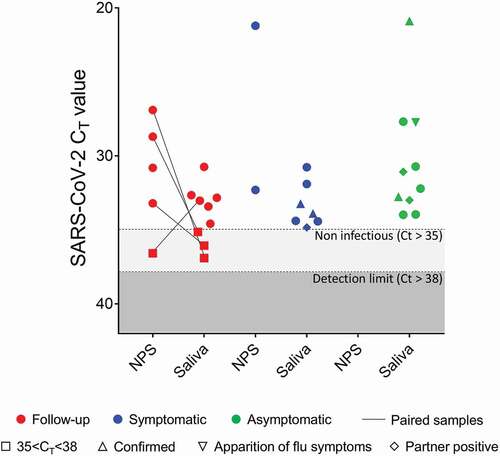
Additional File 1. SARS-CoV-2 Ct values from discordant results of paired NPS and saliva samples according to clinical history or symptoms. Paired samples with Ct > 38 were not presented. Paired samples detected at a non-infectious level (35 < Ct < 38) are indicated by squares. Triangles represent participants with influenza symptoms apparition with (arrow up) or without (arrow down) confirmed SARS-CoV-2 positive test. The participants for who his/her partner were declared SARS-CoV-2 positive few days before are represented by a diamond.
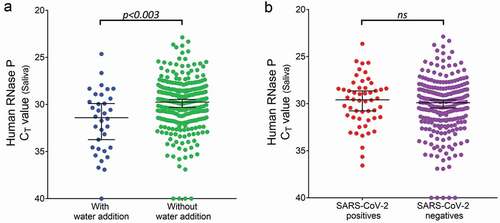
Additional File 2. Consequences of water addition to saliva samples on RNA detection. (A) Comparison of human RNase P Ct values between saliva samples with (n=34) and without (n=269) water addition (p < 0.003, Mann–Whitney test). (B) Comparison of human RNase P Ct values between positive (n=52) and negative (n=251) SARS-Cov-2 saliva samples (p>0.05, Mann–Whitney test). Bars represent the median and 95% CI.