
Abstract
Objective
Hand surgery makes up a large proportion of procedures, ranging from simple to complex. Increased complexity places greater demand on hand surgery competence. Furthermore, when surgical expertise is not matched to the procedure complexity, treatment injuries might occur. The purpose of this study was to assess patient-reported claims submitted to The Norwegian System of Patient Injury Compensation (NPE).
Methods
We examined all hand surgery claims submitted to NPE between 1 January 2007 and 30 June 2017. NPE records patient demography and variables, such as diagnosis, type of injury, injury location, the reason for the compensation claim, and whether a claim was accepted or rejected.
Results
NPE received 1321 claims related to treatment injuries from hand surgery at a steady rate throughout the study period. A total of 532 claims were accepted (40.3%). The approval rate for trauma cases was significantly higher than for elective cases (45.5 vs. 34.2%, p < .05). The most common diagnoses were hand fractures, dislocations and ligament injuries, carpal tunnel syndrome and arthrosis of the first carpometacarpal joint. Tendon injuries had the highest percentage of accepted claims (52.6%). The most common reason for claims being accepted was ‘failure of treatment’. 19.7% of these involved a disability percentage >15%. Elective surgery accounted for ⅔ of the approved disability cases.
Conclusions/interpretation
This is the first national study of patient-reported injuries after hand surgery treatment in Norway. The proportion of accepted claims is similar to that seen for orthopaedics. Acceptance levels were, however, higher for hand trauma cases than for disorders treated electively.
Abbreviations
NPE: Norwegian system of patient injury compensation; SD: standard deviation; CT: computed tomography; MRI: magnetic resonance imaging; UiT: University of Tromsø – Arctic University of Norway.
Introduction
The field of hand surgery includes hand trauma and electively treated hand disorders. Hand surgery accounts for a large number of cases. Statistics from Scandinavia and Europe show that hand injuries are one of the most common emergency room injuries, accounting for 1/5 − 1/3 of cases [Citation1–3]. Many patients also receive elective treatment for hand disorders. There has been a steady increase in the overall number of patient-reported claims submitted to the Norwegian System of Patient Injury Compensation (NPE). It is unknown to what extent this increase applies to treatment injuries after hand injuries or disorders, but it is likely that hand surgery claims have shown similar increases. Hand surgery treatment ranges from simple to complex procedures. Increased complexity places greater demands on hand surgery competence. Treatment injuries may potentially occur where expertise is not matched to procedure complexity.
NPE is a government agency under the Ministry of Health and Care Services. NPE examines claims from patients who believe they have sustained an injury as a result of treatment failure in the health service [Citation4]. The agency was established in 1988 to strengthen the legal rights of patients. These rights have been a part of the Norwegian law since 2003 [Citation5,Citation6]. All public health services are included in the scheme, private health services being included in 2009 [Citation6]. Five criteria must be fulfilled to qualify for compensation (). The right to receive compensation for a treatment injury is only attributed if an error or omission in treatment was made by the health services. This includes errors or omissions in medical investigation, diagnosis or follow-up. The error or omission is not required to be linked to a lack of caution or the negligence of health personnel, but rather whether the reasonable health service expectations of a patient are met or not. A patient must prove connection between the treatment and/or diagnosis and the alleged injury. The patient is compensated regardless of whether the system or an individual is to blame [Citation5,Citation7]. Medical treatment is rarely risk free, and sometimes severe injuries occur despite appropriate treatment. If the patient suffers a major or particularly unexpected injury which was unavoidable, the patient can be eligible for compensation [Citation5,Citation7]. A fundamental condition for compensation in Norway (as in most other countries) is that the injury must have caused a financial loss, for example of earnings and/or future income [Citation7]. The financial loss must exceed NOK 10,000 to qualify. If the patient has sustained a permanent and significant injury, i.e. warranting a medical disability rating of more than 15%, compensation may be paid even if the patient did not suffer a financial loss [Citation7,Citation8]. Medical disability compensation is intended as a financial compensation for the diminished quality of life and reduced functional capacity caused by the injury [Citation7–9]. Disability tables are used to assess medical disability. Examples of 15% disability include thumb amputation at midlevel of the proximal phalanx, fusion of the wrist in 0–20 degree of extension and normal forearm rotation or ulnar nerve injury in the hand with both motor and sensory loss. NPE decides whether a claim for compensation is accepted or rejected through the aid of appropriate experts. NPE also determines the size of compensation. If the patient disagrees with a decision, they can appeal through a court lawsuit against the state.
Table 1. Criteria for patient compensation due to ‘treatment injury’.
The purpose of this study was to gain information which can be used to improve the quality of hand surgery. The primary aim was to assess compensation claims submitted to the NPE that relate to hand surgery treatment, to obtain an overview of the total number of treatment injuries and their characteristics. A secondary aim was to examine whether claims for some diagnoses were more prevalent than others and whether there were differences between claims after hand injuries and hand disorders.
Materials and methods
We were given access to anonymised data for hand surgery treatment for the period 1 January 2007–30 June 2017. Hand surgery was defined as being the surgery of soft tissue and bones in the hand, including carpal bones, but not the distal radius or forearm fracture or its sequela (posttraumatic osteoarthritis after, e.g. intraarticular distal forearm), all soft tissue in the forearm, and nerve injuries from the hand and proximally, but not including injuries of the brachial plexus.
We were given access to variables such as diagnostic codes specified by the International Classification of Diseases version 10 (ICD-10), type of injury, information on whether the claims were accepted or rejected, the reason for treatment and diagnostic failure (available for injuries after 2012), whether the patient received medical disability compensation, and text describing the treatment and injury. The diagnoses included in the study are shown in . Diagnostic codes with fewer than 24 cases were grouped into two groups; a miscellaneous group for trauma cases and a miscellaneous group for elective cases. We assume that they individually would make no significant difference. They, however, appear in some of the diagrams and figures.
Table 2. Total number of complaints and percentage of granted cases distributed in trauma and elective claims sent to NPE in the period 1 January 2007–30 June 2017.
Statistical analysis
Microsoft Excel was used to present the data material in tables. Frequency analysis of registered patient cases was therefore conducted. Descriptive statistics were used to analyse demographic data such as age and gender. Continuous variables were given as mean and SD, categorical data being given as percentages. Groups were analysed using cross tables. A p value < .05 was considered to be statistically significant. A claim can be submitted within 3 years (limitation period) after an injury occurred. We have not applied advanced statistical methods to assess trends over time because of this delay in the reporting of claims.
Ethics/approvals
The Archives Act permits NPE to retain patient data after consent for this has been obtained from the patient seeking compensation [Citation10]. The lead author was granted access to anonymised data from the NPE database.
Results
The total material
NPE made 1321 decisions on claims in the study period that related to our definition of hand surgery. An average of 125.8 decisions relating to hand surgery was made each year. This number was falling markedly from 2016. There was no significant difference in the numbers of each sex in the complete data set (701 women and 624 men, p > .05). Average age at the time of injury in the complete data set was 44.3 years (SD 16.0). There was no significant age difference between women and men.
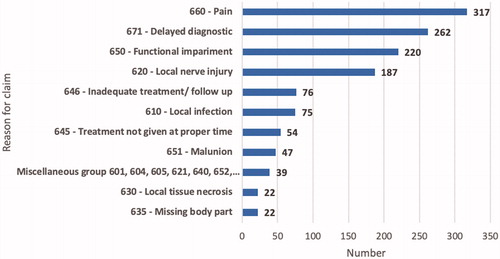
Of 40.3% of the 1321 claims submitted to NPE in the study () were accepted and 59.7% were rejected. The most frequent causes for patient claims were pain, delayed diagnostic, impaired function and local nerve injury (). Delayed diagnosis (27.8%) was the most common cause for accepted claims, while pain (33.5%) and functional disorders (19.8%) were the most common causes for rejected cases.
Figure 1. Reasons for the 1321 patient claims in hand surgery submitted to NPE in the period 1 January 2007–30 June 2017.
Trauma cases
Of 45.5% of the 712 trauma claims were accepted, varying from 8 to 52.9% (). The proportion of men was much greater than women (63.6 vs. 36.4% p < .05). Mean age was 38.7 years (SD 15.5). Around 1/5 of the claims were falling into each of the age groups of 20–29, 30–39, 40–49 and 50–59 years. Diagnosis ‘S62 – Fracture at wrist and hand level’ dominated, accounting for almost half of the accepted trauma claims. Note that this diagnosis code does not include distal radius or ulna fractures. Almost ¼ of the claims for hand fractures were due to ‘S62.0 – Fracture of scaphoid bone of wrist’. Of 63% of these were accepted, which is almost 15% higher than for all hand fractures. The second-largest trauma diagnosis was ‘S63 – Dislocation, sprain and strain of joints and ligaments at wrist and hand level’ at 17% (). ‘S66 – Injury of muscle and tendon at wrist and hand level’ had the highest percentage of accepted claims (52.6%), accounting for 12.7% of accepted trauma claims. The grounds for acceptance were almost equally distributed between ‘treatment failure’ and ‘diagnostic failure’ (). However, 2/3 of all accepted hand fracture claims were based on treatment failure, but more than 2/3 of accepted scaphoid fracture claims were based on diagnostic failure. The reasons for failure in treatment or diagnostics are shown in and Citation4.
Figure 2. Numbers in each claim category for trauma and elective claims in hand surgery submitted to NPE in the period 1 January 2007–30 June 2017.
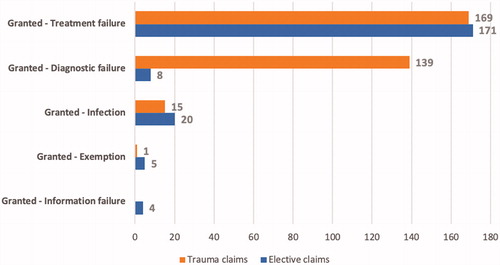
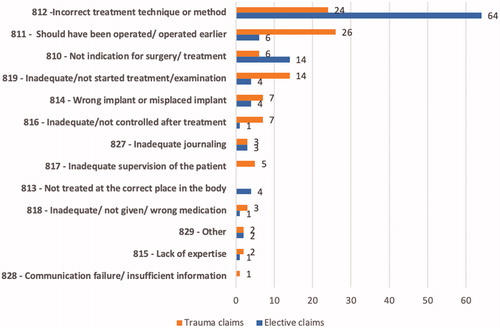
Figure 3. Reason for granting cases due to failure of treatment for trauma and elective claims submitted to NPE in the period 1 January 2012–30 June 2017.
Elective cases
Of 34.2% of the 609 diagnoses treated electively were accepted. Women predominated in relation to men (59.3 vs. 40.7%, p < .05). The mean age of the elective group was 50.8 years (SD 13.9). Age distribution was 29.6% in the 50–59 years group, 22.8% in the 40–49 years group and 19.4% in the 60–69 years group. The diagnosis ‘G56 – Mononeuropathies of upper limb’ dominated, accounting for 40% of the accepted claims for elective hand surgery (). ‘G56.0 – Carpal tunnel syndrome’ accounted for 86.9% of these and ‘G56.2 – Lesion of ulnar nerve’ for 10.7%. The second-largest elective diagnosis was ‘M18 – Arthrosis of first carpometacarpal joint’, accounted for 16%. ‘M65 – Synovitis and tenosynovitis’ accounted for 11.1% of accepted claims, but this diagnosis had the highest rate of acceptance for elective cases at 41.8%. ‘M 72 – Fibroblastic disorders’ accounted for 11% of accepted claims for elective hand surgery. ‘M72.0 – Palmar fascial fibromatosis [Dupuytren]’ accounting for 97.5% of this diagnosis, but at a low acceptance rate. 82.2% of elective cases were accepted based on ‘failure in treatment’ ( and Citation3).
Compensation
A total of 105 of the 532 accepted claims were awarded compensation, based on the degree of medical disability >15%. This accounts for 19.7% of the total number of accepted claims. Trauma cases accounted for 36.2% of these, and elective cases for 63.8% (p < .05). Hand fractures accounted furthermore for 39.5% and dislocations and ligament injuries 21.1% of the trauma claims awarded compensation. Twice as many scaphoid fracture claims were awarded compensation as all hand fractures. Mononeuropathies accounted for 49.3% of elective claims, followed by arthrosis of first carpometacarpal joint at 22.4%.
Discussion
In the defined study period, NPE received 1321 claims by our definition of hand surgery. This includes hand trauma and electively treated hand disorders. We excluded distal radius fractures in this study, as these have been studied previously and have shown around 40% claim acceptance, which is the same rate as for the remainder of orthopaedics [Citation11,Citation12].
The total number of claims and accepted claims were evenly distributed across the first 8 years of the study period but declined from 2015. This can be explained by the limitation period of 3 years for filing a claim, and by missing data for the last 6 months of 2017. The total number of claims submitted to NPE for all medical fields increased significantly in the 10-year period [Citation13]. Hand surgery claims were, however, almost constant. Hand surgery therefore declined compared to the total number of NPE claims.
Gender was evenly distributed for accepted and rejected claims. Young men, however, dominated in trauma cases and elderly women in elective cases. This gender and age distribution for hand trauma and hand disorders is a known epidemiology in hand surgery [Citation3,Citation14,Citation15]. Further studies on the economic impact of trauma cases would be of interest, as a higher rate of claim acceptance for men of working age is a scientifically proven trend.
The most common grounds for claims were pain, dysfunction or delayed treatment (), irrespective of whether the claim was accepted or rejected. The patient expectation that treatment would relieve pain was greatest among the rejected cases. These rejected cases indicate that NPE acknowledge that some pain or dysfunction is expected after treatment. We argue that the incorporation of high quality oral and written information and shared decision-making into daily practice will modulate the patient’s expectation and is essential in reducing ‘treatment injury’ claims to a more correct level.
Hand surgery includes a large number of different types of treatments that range from simple to more complex. This leads us to believe that the proportion of accepted claims varies with the complexity of the diagnosis. However, 2/3 of the approved claims were for hand fractures, joint and ligament injuries, carpal tunnel syndrome and arthrosis of first carpometacarpal joint, the majority of treatment for all these diagnoses involving less complex procedures.
The percentage of accepted claims for the entire field of hand surgery in this study was 40.3%. This is equal to the approval rate for orthopaedics as a whole [Citation11,Citation12]. This may indicate that hand surgery is handled as well as orthopaedics. The approval rate is however, 12% higher than for 10 other medical fields in Norway [Citation13], which may indicate that treatment quality can be improved.
The acceptance rates for trauma cases were significantly higher than for elective cases (45.5 vs. 34.2%, p < .05), which may indicate a special need to focus on treatment of trauma cases. Complexity may also vary within a diagnostic group. For example, 63% of the claims for scaphoid fractures were accepted compared to 49.5% for all hand fractures. In mononeuropathies, however, only 36.1% of the cases were accepted (). This diagnosis accounts for almost 1/5 of the total number of claims, and more than 1/3 of the accepted elective claims and was the most common diagnosis to receive medical disability compensation. Even though the acceptance rate is low, the impact of treatment injuries in mononeuropathies in total is high due to the high number of cases and the medical disability cases. Treatment of this diagnosis therefore also needs special focus. Further studies that incorporate the use of national registry data on how many cases are treated, may further clarify whether these diagnoses have higher incidences of treatment injuries or whether this is due to the high volume of cases treated.
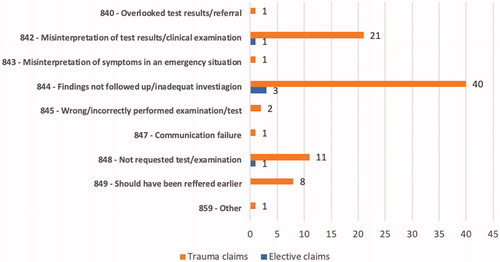
The causal categories for accepted claims are shown in . This shows that trauma cases were almost evenly distributed between ‘failure in treatment’ and ‘failure in diagnostics’. Scaphoid fractures differed from this, with 65% of accepted cases being based on ‘delayed diagnostic’ and 30.4% on ‘failure in treatment’. ‘Failure in treatment’ was the cause of accepted claims in 82.2% of elective cases. NPE introduced specific causal codes describing the causes of categories in 2012. Specific causes of treatment failure are therefore only available for half the cases ( and Citation4). ‘Should have been operated earlier’ was the most common for trauma cases, while ‘incorrect treatment technique’ was the most common treatment failure for elective cases. The causal code ‘should have been operated earlier’ may be due to an individual’s misjudgement when assessing the degree of urgency and severity. It may also be due to the lack of capacity to operate the patient within the recommended waiting time. The code ‘wrong treatment technique’ is at the individual level, the surgeon either choosing the wrong treatment technique or performing the procedure incorrectly. It can also be due to a system error, for example a work schedule planning that allows a surgeon who is not sufficiently trained to carry out hand surgery or treatment. This may account for the 12% higher risk of treatment injury for a hand trauma than for an elective hand condition. The most common causal codes for diagnostic failure were ‘findings not followed up/inadequate investigation’ and ‘misinterpretation of test result/clinical examination’ (). Failure in diagnostics most often occurs at the individual level. Training in proper clinical examination can, for example indicate a suspected scaphoid fracture, and a cost-effective work-up is then to perform immediate computed tomography (CT) or magnetic resonance imaging (MRI) in case of normal radiographs.
Figure 4. Reason for accepting claims submitted to NPE due to failure in diagnostic, for trauma and elective claims, in the period 1 January 2012–30 June 2017.
Almost 20% of all patients whose claims were accepted were given compensation for a medical disability of >15%, 2/3 being elective cases. Arthrosis of first carpometacarpal joint and mononeuropathies were the most frequent elective diagnoses that received this form of compensation (50 and 40%, respectively). Hand fractures, dislocations and ligament injuries were the most frequent trauma case diagnoses that received this form of compensation (39.5 and 21.1%, respectively). This indicates a trend of less complex diagnoses leading to medical disability. Further studies of the prevalence of the defined ICD-10 diagnoses are however needed to clarify whether some treatments more frequently result in medical disability than others.
Strengths and weaknesses of the study
NPE is not a reporting or injury register. The data from NPE is based on patient-reported claims. How many patients who are not submitting claims after sustaining a treatment injury are to the best of our knowledge unknown. The real total number of treatment injuries is likely to be higher than shown in our study. Our results provide an overview of the total number of claims and do not include data on the total number of treatments carried out per year. We therefore do not give incidence rates for treatments injuries in the field of hand surgery, or the variation in injury rates between treatment levels or between regional health authorities for each diagnosis. A weakness of the data is that claims are reviewed through the aid of appropriate experts. There will always be some variation between how the different experts conclude, due to individuality.
Conclusion
This is the first national study on patient-reported injuries after treatment in the field of hand surgery in Norway. The number of treatment injuries has remained steady despite a general increase in claims submitted for all medical fields. The proportion of accepted claims is similar to that seen for orthopaedics but is higher for hand trauma cases than hand disorders treated electively.
Acknowledgements
The authors would like to thank senior advisor Sølvi Flåte at the Norwegian System of Patient Injury Compensation for her excellent help with extracting data from NPE’s database. The article is based on parts of the findings of the unpublished Master thesis of the first two authors in Medicine at UiT in 2019, supervised by the last two authors.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Clark DP, Scott RN, Anderson WR. Hand problems in an accident and emergency department. J Hand Surg. 1985;10(3):297–299.
- Angermann P, Lohmann M. Injuries to the hand and wrist. A study of 50,272 injuries. J Hand Surg Br. 1993;18(5):642–644.
- Larsen CF, Mulder S, Johansen AM, et al. The epidemiology of hand injuries in The Netherlands and Denmark. Eur J Epidemiol. 2003;19(4):323–327.
- Norsk Pasientskadeerstatning. Om NPE. 2020. (07–30). Available from: https://www.npe.no/no/Om-NPE/
- Kongsgaard UE, Fischer K, Pedersen TE, et al. Complaints to the Norwegian system of patient injury compensation 2001–14 following nerve blockade. Tidsskr Laegeforen. 2016;136(23–24):1989–1992.
- Norsk Pasientskadeerstatning. Norsk pasientskadeerstatning gjennom 30 år. 2020. (07–30). Available from: https://www.npe.no/no/Om-NPE/Organisasjon/historien-til-norsk-pasientskadeordning/
- Molven O, Julia F. Healthcare, welfare and law. Health legislation as a mirror of the Norwegian welfare state. Oslo, Norway: Gyldendal Akademisk; 2011.
- Norsk Pasientskadeerstatning. [Internett]. Hva skal til for år erstatning for en pasientskade? Oslo: 2017. [2017-09-28]. Available from: https://www.npe.no/no/Erstatningssoker/Soke-erstatning/Hva-skal-til-for-erstatning-pasientskade/
- Syse A, Kjelland M, Jørstad RG. Pasientskaderett. 1. Utg. Oslo, Norway: Gyldendal Norsk Forlag; 2011. p. 536.
- Norsk Pasientskadeerstatning. Personvernerklaering. 2020. (07–30). Available from: https://www.npe.no/no/Om-NPE/personvernerklaering/
- Norum J, Balteskard L, Thomsen MW, et al. Wrist malpractice claims in Northern Norway 2005–2014. Lessons to be learned. Int J Circumplar Health. 2018;77(1):1483690.
- Clementsen S, Hammer OL, Engebretsen E, et al. Compensation after distal radius fractures. A review of 800 claims to the Norwegian system of patient injury compensation 2000–2013. Open Orthop J 2018;12:419–414.
- Norsk Pasientskadeerstatning. Statistikk for regionale helseforetak 2013–2017 (Internett). Oslo: NPE. 2017. [2020-03-13]. Available from: https://www.npe.no/globalassets/dokumenter-pdf-og-presentasjoner/rapporter/rhf_rapport_2017_web.pdf
- Skadeforebyggende Forum. [Internett]. Oslo; Fakta Om Personskader. 2019. [2019-04-26]. Available from: https://www.skafor.org/fakta/
- Elberg JJ, Jorgensen HR, Larsen CF. Hand injuries. Epidemiology, medical and economic consequences. Ugeskr Laeger. 1987;149(16):1096–1099.