
ABSTRACT
Background: Suicide is a leading cause of death, and rates of attempted suicide have increased during the COVID-19 pandemic. The under-diagnosed psychiatric phenotype of dissociation is associated with elevated suicidal self-injury; however, it has largely been left out of attempts to predict and prevent suicide.
Objective: We designed an artificial intelligence approach to identify dissociative patients and predict prior suicide attempts in an unbiased, data-driven manner.
Method: Participants were 30 controls and 93 treatment-seeking female patients with posttraumatic stress disorder (PTSD) and various levels of dissociation, including some with the PTSD dissociative subtype and some with dissociative identity disorder (DID).
Results: Unsupervised learning models identified patients along a spectrum of dissociation. Moreover, supervised learning models accurately predicted prior suicide attempts with an F1 score up to 0.83. DID had the highest risk of prior suicide attempts, and distinct subtypes of dissociation predicted suicide attempts in PTSD and DID.
Conclusions: These findings expand our understanding of the dissociative phenotype and underscore the urgent need to assess for dissociation to identify individuals at high-risk of suicidal self-injury.
HIGHLIGHTS
Dissociation, feelings of detachment and disruption in one's sense of self and surroundings, is associated with an elevated risk of suicidal self-injury; however, it has largely been left out of attempts to predict and prevent suicide.
Using machine learning techniques, we found dissociative identity disorder had the highest risk of prior suicide attempts, and distinct subtypes of dissociation predicted suicide attempts in posttraumatic stress disorder and dissociative identity disorder.
These findings underscore the urgent need to assess for dissociation to identify individuals at high-risk of suicidal self-injury.
Antecedentes: El suicidio es una de las causas principales de muerte y las tasas de intentos suicidas han aumentado durante la pandemia de COVID-19. El fenotipo psiquiátrico sub-diagnosticado de disociación se asocia con autolesiones suicidas elevadas; sin embargo, en gran medida se ha dejado fuera de los intentos para predecir y prevenir el suicidio.
Objetivo: Diseñamos un enfoque de una inteligencia artificial para identificar a los pacientes con trastornos disociativos y predecir intentos suicidas previos en una forma imparcial y basada en datos.
Método: Los participantes fueron 30 mujeres controles y 93 pacientes con trastorno de estrés postraumático (TEPT) y niveles variados de disociación que buscaban tratamiento, incluyendo algunas con TEPT subtipo disociativo y algunas con trastorno de la identidad disociativo (TID).
Resultados: Los modelos de aprendizaje no supervisados identificaron pacientes a lo largo de un espectro de disociación. Además, los modelos de aprendizaje supervisados predijeron con precisión los intentos suicidas previos con una puntuación de hasta 0.83. El TID tuvo el riesgo más alto de intentos suicidas previos y los distintos subtipos de disociación predijeron intentos suicidas en TEPT y TID.
Conclusiones: Estos hallazgos expanden nuestra comprensión del fenotipo disociativo y subrayan la necesidad urgente de evaluar la disociación para identificar a las personas con alto riesgo de autolesiones suicidas.
背景:自杀是导致死亡的主要原因,自杀未遂率在 COVID-19 疫情期间有所增加。未得到充分诊断的精神病学解离表型与自杀性自伤的升高有关;然而,它在很大程度上被排除在预测和预防自杀的尝试之外。
目的:我们设计了一种人工智能方法来识别解离患者并以无偏见的数据驱动方式预测先前的自杀意图。
方法:参与者是 30 名对照和 93 名寻求治疗的患有创伤后应激障碍 (PTSD) 和不同程度解离的女性患者,包括一些患有 PTSD 解离亚型和一些患有解离性身份障碍 (DID) 的女性。
结果:无监督学习模型识别出一系列解离患者。此外,监督学习模型准确地预测了先前的自杀意图,得分高达 0.83。 DID 具有最高的先前自杀意图的风险,并且不同的解离亚型预测了 PTSD 和 DID 的自杀意图。
结论:这些发现拓展了我们对解离表型的理解,并强调了评估解离以识别具有自杀性自伤高风险个体的迫切需要。
1. Introduction
Suicide is a leading cause of death globally (World Health Organisation, Citation2014). While the economic cost of self-injury, suicide attempts and suicides in the United States alone was estimated to be greater than $90 billion in 2013 (Shepard et al., Citation2016), the psychological costs to individuals and bereaved families are devastating and not easily quantifiable. Moreover, there has been minimal progress in reducing these types of deaths, despite the urgent need (World Health Organisation, Citation2014) – now made more urgent with increased rates of suicidal thinking and attempts for many groups during the COVID-19 pandemic (Fortgang et al., Citation2021; Holland et al., Citation2021; Yard et al., Citation2021).
Traumatic stress exposure during childhood is strongly associated with suicidal ideation and behaviours (Afifi et al., Citation2008; Bruffaerts et al., Citation2010; Dube et al., Citation2001). In addition, individuals with trauma-related psychiatric disorders such as posttraumatic stress disorder (PTSD), the dissociative subtype of PTSD (PTSD-DS), and dissociative identity disorder (DID) have increased frequency of self-injury, suicidal ideation and suicide attempts across the lifespan (Calati et al., Citation2017; Eidhof et al., Citation2019; Foote et al., Citation2008; Ford & Gómez, Citation2015). Importantly, symptoms of dissociation are key aspects of the diagnostic criteria for each of these disorders (American Psychiatric Association, Citation2013). Dissociation is characterised by disruptions and discontinuities in the typical integration of psychological functioning (American Psychiatric Association, Citation2013; Dell, Citation2006). Dissociative symptoms are associated with increased suicide attempts (Calati et al., Citation2017; Vine et al., Citation2020) and, therefore, could be leveraged for early identification of individuals at elevated risk of suicidal self-injury. However, dissociative symptoms remain understudied and under-diagnosed due to a relative lack of understanding in general psychiatric practice (Sar & Ross, Citation2006).
Given that dissociation is underappreciated in clinical research and practice, it would be clinically beneficial to develop techniques to (1) quickly and efficiently identify patients suffering from dissociation and related symptoms, and (2) determine among these high-risk individuals, what specific dissociative symptoms may predict suicidal self-injury. Artificial intelligence (AI) and machine learning techniques use algorithms to identify patterns in data with minimal human intervention – thus ideally reducing human bias in how patterns and predictors are identified (Dwyer et al., Citation2018). Machine learning has recently been applied to the challenging problem of predicting self-injurious and suicidal behaviours (Burke et al., Citation2019; Torous et al., Citation2018), however, dissociation has not yet been considered in these models.
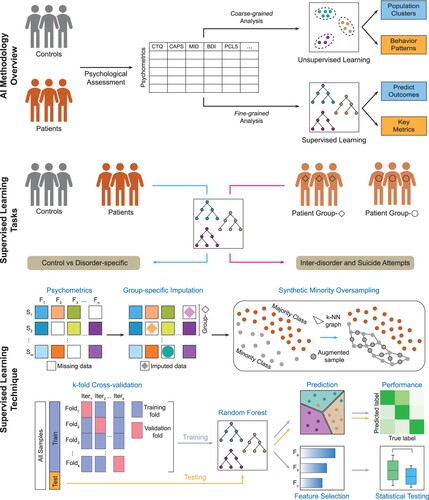
To address this critical gap, we designed and applied complementary AI techniques to identify patterns and make predictions for a sample of women with PTSD and various levels of dissociation, including PTSD-DS, dissociative disorder not otherwise specified type 1 (DDNOS), and DID (). The participant data for our models included self-report and clinical interviews of childhood trauma, PTSD, depression, and dissociation. First, we hypothesised that we could analyse and visualise coarse-grained structures in the psychometric self-report and clinical interview data in an unbiased manner. We therefore applied unsupervised machine learning algorithms that do not require labels for training. Second, to obtain a fine-grained view of the assessment data, we designed a robust supervised learning technique combining metrics with target labels for training to predict clinical groups and past suicide attempts. We hypothesised that these methods would accurately predict diagnostic groups and patterns in suicidal self-injury.
Figure 1. Overview of the Multigranular Artificial Intelligence (AI) approach. Participant data were analyzed using two complementary AI approaches: Unsupervised Learning and Supervised Learning. The unsupervised learning tasks were designed for categories of clinical interest (i.e. diagnostic categories, suicide attempt). The supervised learning technique included five stages: feature engineering, class balancing by synthetic oversampling, k-fold cross-validation, model training, and testing. Model training included feature ranking and selection, and statistical testing of the top features. Of note, variables are called features in machine learning.
2. Methods
We developed an integrated AI approach and applied it to a clinical dataset of participants enrolled at McLean Hospital, where each patient's data were represented as a numeric feature (variable) vector consisting of self-report and clinical interview psychometrics. The unsupervised and supervised AI methods were utilised to study patterns and categorise the high-dimensional data, and to identify psychometric signatures in the heterogeneous patient sample ().
2.1. Study design and participants
The study cohort was recruited at a psychiatric hospital in the Northeastern United States and included 123 female sex assigned at birth participants (93 patients and 30 controls), between 18–62 years old (M = 33.1 years). All patients were diagnosed with PTSD and various levels of dissociation, including some with PTSD-DS, and some DID or DDNOS (). Patients were excluded if they had a current alcohol or substance use disorder within the past month or a history of or current psychotic spectrum disorder. Control participants had no lifetime or current psychiatric diagnoses. A set of quantitative self-reports and interviews were administered to each participant, including the PTSD Checklist for DSM-5 (PCL-5) (Weathers et al., Citation2013), Clinician-Administered PTSD Scale for DSM-5 (CAPS-5) (Weathers et al., Citation2018), Childhood Trauma Questionnaire (CTQ) (Bernstein et al., Citation1994), Dissociative Experiences Scale-II (DES-II) (Carlson & Putnam, Citation1993), Structured Clinical Interview for DSM-IV Dissociative Disorders revised (SCID-D) (Steinberg, Citation1994), Multidimensional Inventory of Dissociation (MID) (Dell, Citation2006) and Beck Depression Inventory-II (BDI-II) (Beck et al., Citation1996). The average scores from the various assessments are listed in . This study was approved by the Mass General Brigham institutional review board and complied with all relevant ethical regulations in accordance with the principles stated in the Declaration of Helsinki. Informed consent was obtained from all research participants.
Table 1. Summary of demographics and clinical data.
2.2. Feature engineering
The psychometric data were divided into two primary sections, (1) numerical/input data: which consisted of assessment scores, and (2) categorical/output data: which consisted of outcomes of clinical interest, such as final diagnosis (e.g. PTSD, PTSD-DS, etc.), suicide attempts (Yes/No) and severity labels for specific assessments (e.g. childhood trauma severity for CTQ, depression severity for BDI-II, etc.). The numerical data had 441 variables in total, which were further divided into two groups: (1) summary subscale scores of the assessments (101 features) and (2) individual items of the assessments (340 features). See the supplemental materials for further detail.
2.3. Unsupervised learning
We employed an unsupervised learning approach (Theodoridis & Koutroumbas, Citation2008) to identify clusters of data points sharing common patterns and then describe the relationships among the clusters to assess clinical behaviours and categories of interest. For this approach, only the numeric features were used. To discern these patterns, we employed clustering and dimensionality reduction techniques, to map and visualise high-dimensional data into two-dimensional (2D) spaces while preserving the similarity between the data points. Specifically, we applied t-Distributed stochastic neighbour embedding (t-SNE) (Van der Maaten & Hinton, Citation2008), a technique commonly used to analyse biological data. This technique efficiently captures critical parts of the local structure of high-dimensional data and maps it into 2D space. It can also determine clusters without prior knowledge of cluster number or sizes. The 2D points were then annotated according to the categories of interest (categories that were initially excluded), revealing the pattern of correlation between data structures and clinical labels.
Next, we used a more generalisable dimensionality reduction method with deep learning architecture, Denoising Autoencoder with Neuronal Approximator (DAWN) (Srinivasan et al., Citation2020), to uncover additional high-dimensional relationships in the patient sample.
2.4. Supervised learning
For a higher resolution analysis that would enhance the distinction between groups, we used supervised learning (Kotsiantis, Citation2007). To avoid potential classification bias and obtain robust models with consistent predictions and predictors, we first addressed a class imbalance problem in our data in which the size of the control group did not match the patient group. We used a data augmentation technique to add control samples, known as synthetic minority over-sampling technique (SMOTE) (Chawla et al., Citation2002). Samples were added by creating intermediate points in the existing feature space of the k-nearest neighbours (i.e. k-NN graph) (Fukunaga & Narendra, Citation1975) of each control sample. These augmented and balanced data were used for all further steps.
Next, we completed two types of classification tasks (): (1) categorising control and patient diagnostic groups, and (2) modelling the risk of a prior suicide attempt in the patient sample. We used the multi-class Random Forest (RF) algorithm (Liaw & Wiener, Citation2002) to complete these tasks. See the supplemental materials for further details. In brief, this algorithm first undergoes training on the paired input-output data, where the input corresponds to psychometrics and output corresponds to categories of interest, for example, PTSD status, final diagnosis, risk of attempting suicide.
For predicting suicide attempt in the patients, we used the patient responses for the question ‘Have you ever attempted suicide?’ with yes/no answers as the output labels, that would be predicted by our supervised learning model. As the MID tool accounted for the majority (∼64%) of the collected data, we modelled the specificity of these metrics in predicting suicide attempt. We used the 218 questions in the MID assessment to calculate 56 summary-level metrics according to the MID manual (Dell et al., Citation2017). Since the DDNOS group contained only three patients, the low sample size prohibited accurate application of a supervised learning algorithm and was excluded from this analysis.
2.5. Statistical testing
The classification models identified a set of predictors that were indicative of clinical symptomatology that was enhanced in one category versus another. In addition to ascertaining the generalizability of selected features, we verified whether a specific predictor had significant differences among the modelled categories by performing non-parametric statistical hypothesis testing using the Wilcoxon test (Wilcoxon, Citation1992).
Additionally, since the exposure factors of childhood trauma and several categories of interest, such as depression severity, were highly associated with suicidal self-injury (Copeland et al., Citation2018), we performed odds ratio and risk ratio analyses to determine the strength of these relationships in the study cohort (Szumilas, Citation2010). For both analyses, we used the Wald test (Buse, Citation1982) with a confidence interval of 95% to assess effect size and the chi-squared test with the threshold p-value < .05 to reject the null hypothesis (i.e. there was no association between exposure and suicide attempt). Significance tests were two-tailed.
3. Results
3.1. Unsupervised learning revealed patient sub-clusters and a spectrum of dissociation symptoms across diagnoses
First, we performed t-Distributed stochastic neighbour embedding (t-SNE) based clustering on the self-report and interview-based subscales (summary-level variables or ‘features’), using the inter-cluster distance ((A)). We found two primary clusters belonging to control and patient groups, which intrinsically captured the large dissimilarity between these two groups. Within the large patient cluster, there were smaller patient sub-clusters, indicating patient heterogeneity. We identified small and mixed clusters of PTSD, PTSD-DS, and DDNOS patients and a distinct cluster for DID (67% of patients with DID). To identify factors contributing to the patient cluster structure and the uniqueness of the DID cluster, we overlayed two categorical features, the childhood trauma questionnaire (CTQ) total severity (minimal, moderate, severe, extreme) and Beck Depression Inventory-II (BDI-II) depression severity (minimal, mild, moderate, severe; (B,C)) onto the clusters. Next, we mapped the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D) symptom severity for depersonalisation, derealization, amnesia, identity alteration and identity confusion onto the clusters, finding that PTSD-DS, DDNOS and DID patients had the highest severity for all five scales (Supplementary Figure 1). We also assessed whether unbiased analyses of all the question-level metrics (340 features) could uncover more distinct clusters (Supplementary Figure 2), but the clustering provided a marginal distance change exclusively in the ‘DID cluster’. This cluster had a higher proportion of individuals that attempted suicide ((D)).
Figure 2. Unsupervised learning reveals patient sub-clusters and spectrum of dissociative symptoms. (A) Two-dimensional t-SNE embedding of summary psychometrics on arbitrary X and Y axes, annotated with diagnosis labels, shows patient heterogeneity patterns with a distinct ‘DID cluster’ of 26 individuals (circled). (B and C) Embedding annotated with CTQ and BDI-II severity respectively, shows the ‘DID cluster’ has a high rate of extreme trauma and severe depression. (D) Annotation of individuals who attempted suicide where we found past suicide attempt was more prevalent in the ‘DID cluster.’ (E) DAWN 2D embedding of only the patients on arbitrary X and Y axes demonstrated the presence of a spectrum of dissociative symptoms with clustering of individuals who attempted suicide. (F) Bubble plot showing the relationship between childhood trauma and depression severity and prevalence of individuals who attempted suicide. t-SNE, t-Distributed stochastic neighbour embedding; CTQ, Childhood Trauma Questionnaire, BDI-II, Beck Depression Inventory-II, DAWN 2D, Denoising Autoencoder with Neuronal Approximator.
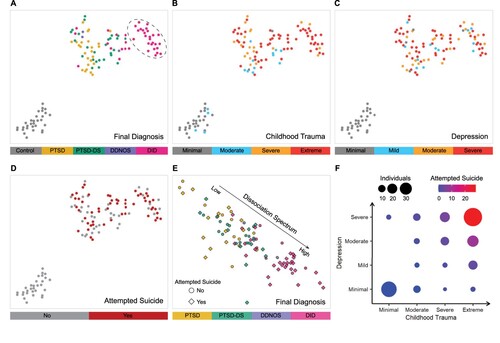
Next, we explored clustering in the data using Denoising Autoencoder with Neuronal Approximator (DAWN Srinivasan et al., Citation2020). The embedding generated by DAWN showed a spectrum of dissociative symptoms ((E) and Supplementary Figure 3): PTSD patients with the lowest dissociative scores were mapped on the left, PTSD-DS and DDNOS patients with moderate dissociation were positioned in the centre and DID patients with severe symptoms were mapped on the right. We also identified a more prominent clustering of the individuals with suicide attempts that were at the extreme end of the spectrum of dissociative symptoms. Lastly, the analysis revealed a strong relationship between suicide, childhood trauma, and depression ((F)), where the most severe group has the highest proportion of individuals who attempted suicide: 37 individuals, of whom ∼60% were patients with DID and 76% attempted suicide. Similar patterns were observed when considering diagnosis and current level of psychiatric care . We also examined the severity of suicidal ideation, i.e. BDI-II Q.9 responses, according to diagnosis and current level of psychiatric care, (Supplementary Figure 5(A,B)). Patients with DID and PTSD-DS had higher levels of suicidal ideation than other groups.
3.2. Supervised learning models identified key patient metrics and past suicide attempts
Classifying Diagnostic Groups. Supervised learning models were created to classify individuals based on diagnosis and to extract important distinguishing psychometrics. illustrates the accuracy for each patient inter-group classification model trained on summary-level psychometrics, that is, subscale totals on each questionnaire or interview. These models were highly stable during training and accurate on the unseen test data during testing, reaching an F1 score of 0.95. Separate models were developed to determine the utility of the question-level item data (Supplementary Table 2).
Table 2. Results of the supervised learning modelling tasks using summary psychometrics.
Of note, for the binary classification of control/patient, only two features were sufficient to make this classification (Supplementary Table 1). The top feature was the PTSD checklist for DSM-5 (PCL-5) Criterion E severity, indicative of alterations in arousal and reactivity. This result had a highly significant difference in differentiating controls vs. patients, obtained from Wilcoxon test ((A)) as a raincloud plot (visualisation that includes raw data, summary statistics as a box plot and probability density) (Allen et al., Citation2019). Moreover, to categorise individuals to either the control group or a disorder group (PTSD, PTSD-DS, DID), only a single feature was necessary (Supplementary Table 1 and Supplementary Figure 6). Modelling question-level metrics did not improve the test accuracies (Supplementary Table 2).
Figure 3. Hybrid supervised learning identifies markers and distinct symptom landscape. (A) Raincloud plot with p-value showing the primary symptom that distinguished the patient and control groups. (B and C) CTQ: Sexual abuse and SCID-D Dissociative Symptoms: Depersonalisation were the top-two metrics that distinguished between the tertiary classification of the three patient groups. On average, individuals with DID reported the most severe histories of childhood sexual abuse and the most extreme depersonalisation symptoms, followed by individuals with PTSD-DS. (D) A scatter plot demonstrated the spectrum of dissociation in patients when MID metrics of Pathological Dissociation: Severe Dissociation and Partially Dissociated Intrusions: Made/Intrusive Actions were considered. Probability densities are displayed on the top and right for each metric. (E) MID Fully-Dissociated Actions: Fugues was identified as the top metric for predicting past suicide attempts. (F) Scatter plot of the top-two metrics for suicide attempts. Thresholds or decision boundaries are displayed with a dashed line. The area greater than the thresholds included most suicide attempts. Probability densities are displayed on the top and right for each metric. MID, Multidimensional Inventory of Dissociation; CTQ, Childhood Trauma Questionnaire; SCID-D, Structured Clinical Interview for DSM-IV Dissociative Disorders revised; PCL-5, PTSD Checklist for DSM 5; PDI, partially-dissociated intrusions; CBP, cognitive and behavioural psychopathology scale.
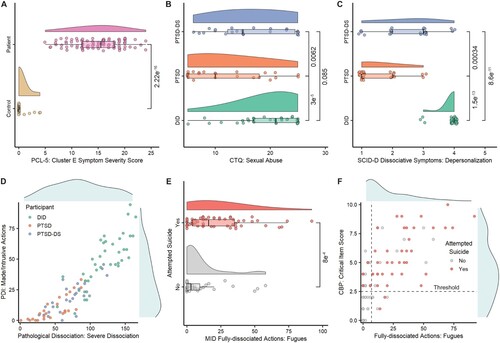
The multi-class prediction assigning individuals to PTSD, PTSD-DS, and DID using summary-level self-report/interview subscales was also highly accurate () and categorised the heterogeneous sample with only eight predictors. Most predictors came from diagnostic interviews; however, one top-ranking predictor measured childhood sexual abuse using the childhood trauma questionnaire. DID and PTSD-DS reported more sexual abuse compared to PTSD ((B)).
When comparing one diagnostic category to another (), we found that patients with DID and PTSD could be accurately assigned to the correct group based on a single feature, the SCID-D Dissociative Symptoms Depersonalisation metric, in which only the DID sample had a high score ((C)). In both metrics selected by the models ((B,C)), the PTSD-DS sample had intermediate scores, compared to lower scores for patients with PTSD, and higher scores for patients with DID. The supervised learning models provided metric-level insights first observed with the unsupervised learning.
Moreover, using supervised learning to classify the three patient samples (PTSD, PTSD-DS, DID) simultaneously, we observed a spectrum of dissociative symptoms that was similar to the unsupervised learning results ((D) and Supplementary Figure 7). The patients with PTSD had the lowest dissociation severity, while PTSD-DS had intermediate severity, and patients with DID had the greatest severity.
Classifying Based on Past Suicide Attempt. Supervised learning models were also created to classify individuals based on past suicide attempt and extract important distinguishing psychometrics. Past suicide attempt was a binary classification (i.e. ‘yes’ vs. ‘no’ history of past attempt). Suicide attempt modelling resulted in training and test accuracy scores ≥ 0.7. The model identified eight features, six of which were from the multidimensional inventory of dissociation (MID; ; (E)). Moreover, we found that the top-two suicide attempt predictors were related to amnesia and harmful or potentially dangerous symptoms (Fully-Dissociated Actions: Fugues; Functionality and Impairment: Critical Items Score) and could be visualised using two thresholds ((F)). This revealed decision boundaries where the area greater than the identified thresholds consisted of most individuals (∼66%) who attempted suicide and only a small number of individuals who did not (∼21%).
Given that most features that predicted suicide attempt were from the MID, we conducted a subsequent analysis focused only on MID data. First, we used the entire patient sample, followed by PTSD-specific modelling (which collapsed across PTSD/PTSD-DS groups) and then finally only the patients with DID (). By focusing only on dissociative symptoms captured by the MID, we observed an improvement in test accuracy for predicting suicide attempt (accuracy delta: 0.03 ≥ ΔF1 ≥ 0.13), especially in the DID sample (score = 0.83).
Table 3. Results of the suicide attempt modelling tasks using MID summary metrics.
For the prediction of suicide attempt in the entire patient sample, three features from the MID Schneiderian First-Rank Symptoms were identified as predictive ((A,B)). For the PTSD/PTSD-DS group, the top-ranking feature was the experience of hearing persecutory voices. We examined how these experiences were related to suicide attempts ((C)), determining thresholds that could delineate ∼65% of suicide attempts. When predicting suicide attempt only within the DID group, we achieved the highest F1 scores.
Figure 4. Predictive subscales from the MID and the odds/risk ratio for suicide attempt in the DID sample. (A and B) Raincloud plots showing the top-two metrics identified by the supervised learning model to predict suicide attempt. (C) Scatter plot of the top-two metrics that predicted suicide attempt in the PTSD/PTSD-DS group. Probability densities are displayed on top and right for each metric. (D) Suicide attempt modelling in the patient sample using question-level responses identified the top metric, Question 186: Discovering that you have attempted suicide but having no memory of having done it. (E) Suicide attempt odds ratio analysis for the DID group with a combined PTSD/PTSD-DS group as the reference. (F) Suicide attempt risk ratio analysis for the DID group with PTSD/PTSD-DS group as the reference. MID, Multidimensional Inventory of Dissociation, PDI, partially-dissociated intrusion.
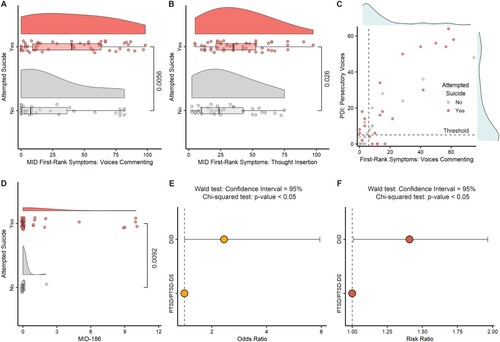
We also explored question-level metrics in the entire patient sample. The top-two ranking features were both related to amnesia for actions: MID – Q.186: ‘Discovering that you have attempted suicide, but having no memory of having done it,’ ((D)) and MID – Q.204: ‘There were times when you ‘came to’ and found pills or a razor blade (or something else to hurt yourself with) in your hand’. Taken together, we found that different types of dissociation predicted past suicide attempt within each diagnostic category with a high level of accuracy, especially for DID.
3.3. Odds ratio and risk ratio analysis of suicide attempts
We observed that approximately 71% of patients with DID attempted suicide, which comprised ∼51% of all the individuals who attempted suicide in the patient sample. Given this, we performed an odds ratio (OR) and risk ratio (RR) analysis to determine odds/risk of suicide attempts as related to diagnostic categories and the dimensional symptoms of depression and childhood trauma. We found that the small sample sizes of the patient groups and severity labels influenced the association in two ways: (1) the high magnitude of the association obtained for the diagnosis groups when using the control group as reference, and (2) the large width of the confidence interval (CI). We note that the range of the CI decreased as the sample size increased, and the magnitude of the association was dependent on the number of suicide attempts in the reference group. All ratios were statistically significant (Supplementary Figure 8); furthermore, we observed that higher severity of childhood trauma and depression increased the OR and RR for suicide attempt. To overcome the above issues with the reference group, we examined the risk of attempting suicide only within the patient sample by considering PTSD/PTSD-DS as a reference group. Compared to the PTSD/PTSD-DS group, the DID group had an estimated OR = 2.4 and RR = 1.4 with 95% CI (p < .05) for increased risk of suicide attempt ((E,F)).
4. Discussion
Dissociation is linked to greater suicidal self-injury (Calati et al., Citation2017) but remains under-diagnosed and underappreciated in psychiatric practice (Sar & Ross, Citation2006) – underscoring a missed opportunity to identify and implement early interventions with individuals at-risk of attempting suicide. AI techniques including supervised and unsupervised machine learning can reveal unique intrinsic structures in complex datasets and can serve to validate front-line clinical reports of underappreciated symptoms using unbiased, data-driven methods. In the current study, AI methods were able to identify clusters of patients along a dissociative continuum. Moreover, with supervised learning techniques we were able to predict diagnostic groups and incidence of a past suicide attempt with a score of up to 0.83 – an accuracy comparable to much larger studies predicting suicide attempts (Delgado-Gomez et al., Citation2016; Edgcomb et al., Citation2021).
Our unsupervised machine learning analyses revealed patient clusters that mapped onto a spectrum of dissociative symptoms using summary scores from self-report and clinician-administered interviews. First, we identified a distinct cluster containing mostly patients with DID. Patients in this cluster had the highest levels of childhood trauma, depression and suicide attempts. Second, this analysis also identified other more heterogeneous clusters of patients. When mapped to diagnostic categories, these clusters were a mix of patients diagnosed with PTSD, PTSD-DS, and DDNOS. The current findings suggest the borders of trauma-related diagnostic categories may not be as discrete as the current diagnostic criteria imply. Finally, we also applied our even more powerful, state-of-the-art unsupervised machine learning method, the deep cluster method DAWN, to the summary scores from self-reports and interviews. In these types of models, algorithms are structured in layers to create a network that can ‘learn’ on its own. Like our prior models, this analysis also revealed and visualised a distinct continuum of dissociation symptoms in the patient sample, replicating reports of dissociative subtypes in PTSD cohorts (Wolf et al., Citation2012), but now through a powerful and unbiased data-driven method.
Given DSM-5 diagnostic categories remain dominant in the field, we also completed a series of supervised learning analyses in which we provided the algorithm with our diagnostic categories of interest. These models identified the smallest number of questions or ‘features’ necessary to distinguish between diagnostic groups. Most top features in these models were scales from interviews designed to distinguish between these diagnostic categories. Interestingly, however, there was one top-ranking feature related to childhood sexual abuse. Individuals with DID and PTSD-DS reported more childhood sexual abuse compared to individuals with conventional PTSD. Prior work consistently links trauma and childhood maltreatment with dissociation (Dalenberg et al., Citation2012). Findings are typically more mixed when focused on a particular type of childhood trauma and its association with dissociation, however. For example, some studies link dissociation with greater childhood sexual abuse exposure and some do not (Hill et al., Citation2020). Taken together, our supervised learning results validated diagnostic interviews/self-reports with data-driven machine learning and highlighted childhood sexual abuse as a common exposure associated with adult dissociation symptoms.
Our primary aim was to leverage patient history, symptoms, and diagnoses to predict an incidence of a past suicide attempt. First, we were interested in how childhood trauma and symptoms of depression impacted the odds and risk of suicide attempts. As expected, individuals with severe depression and extreme childhood trauma were at highest risk of having attempted suicide. A significant literature links more severe depression (Hawton et al., Citation2013) and childhood adversity with higher likelihood of suicide attempts (Bruffaerts et al., Citation2010) Next, we explored how diagnostic category impacted suicide attempt. Compared to our PTSD groups, individuals with DID had the greatest number of attempts: 71% had attempted suicide. Moreover, in comparing the DID and PTSD/PTSD-DS groups, the odds of a suicide attempt were 140% higher in patients with DID. Further, patients with a DID diagnosis had a 40% increased risk of a suicide attempt compared to those with a PTSD/PTSD-DS diagnosis. These results are consistent with previously reported high prevalence rates of suicide attempts in patients with DID compared to other disorders (Foote et al., Citation2008). These findings highlight the urgent need to include individuals with DID in studies of suicidal self-injury.
The aforementioned suicide-attempt analyses examined dissociation at a coarse-grained diagnostic level, however, there are many dimensional subtypes of dissociation and no prior research had explored the relationship between suicide attempt and specific types of dissociative experiences. Thus, we used supervised machine learning analyses to identify which types of dissociation predicted suicide attempt. First, we examined the entire patient sample as one group (including PTSD, PTSD-DS, DID). The top predictors were all Schneiderian first-rank symptoms, including ‘hearing voices commenting in your head’, experiencing thought insertion in which thoughts are ‘imposed on your mind’ and may feel like they do not belong to you, and ‘made’ actions where you feel that your actions were conducted by someone/thing else (Schneider, Citation1959). These experiences are traditionally linked to schizophrenia, however, 8 of 11 Schneider's first-rank symptoms also occur in complex dissociative disorders (Somer & Dell, Citation2005) and some occur in PTSD as well (Frewen & Lanius, Citation2015; Shinn et al., Citation2019). Importantly, there are critical differences between how these symptoms manifest in PTSD and dissociative disorders compared to schizophrenia. In PTSD and dissociative disorders, reality testing remains intact, while in schizophrenia, reality testing is compromised, and the explanations given for these experiences are often bizarre (Somer & Dell, Citation2005). For example, someone with schizophrenia might think that ‘Oprah is inserting thoughts in my mind’ vs. someone with DID might feel that some of their own thoughts feel like they don't belong to them. Central to these experiences is the awareness of a loss of agency. Individuals with DID consciously experience the voices, thought insertion, and made actions as ‘ego-alien intrusions into executive functioning’ (Dell, Citation2010). This is not psychosis; however, this type of intrusion provokes increased distress (Dell, Citation2010), and may be one reason why these experiences predict suicidal self-injury.
Next, we looked within diagnostic categories to identify types of dissociation related to suicide attempt. For the PTSD analysis, we collapsed across conventional PTSD and PTSD-DS. We found that several forms of hearing voices and amnesia for actions (i.e. ‘coming to’ during the middle of something you don't recall initiating) predicted the incidence of a past suicide attempt. The voice hearing involved voices commenting and experiences of ‘auditory harassment and persecution’ in which voices or ‘loud thoughts’ comment punitively or command self-harm (Dell et al., Citation2017). Several studies have documented voice hearing in PTSD and characterised it as different than voice hearing experienced in primary psychotic disorders (Barlow & Chu, Citation2014; Shinn et al., Citation2019). As voice hearing remains a little-known phenomenon in PTSD, researchers and clinicians may not assess for these experiences – therefore, missing an opportunity to identify symptoms potentially predictive of suicidal self-injury.
Finally, predictors of suicide attempt in our DID sample involved amnesia for actions. Specifically, these amnestic actions included ‘coming to’ in the middle of an action you do not remember starting and discovering ‘objects, writings, or drawings’ in your possession that you do not remember acquiring/writing/drawing (Dell et al., Citation2017). These types of experiences are markers of more severe memory and identity disturbances in DID (Barlow & Chu, Citation2014). Our findings suggest someone with DID experiencing severe memory loss for actions may be at greater risk of suicidal self-injury.
Our analyses were limited by several factors. First, we completed a cross-sectional, retrospective analysis predicting the history of a past suicide attempt. While prior work has established that past suicide attempts are predictive of future attempts (Hawton et al., Citation2013), a longitudinal, prospective design is needed to test whether the features we identified as predictors of suicide attempt could be leveraged to predict the likelihood of a future suicide attempt. Second, our machine learning models and statistical analyses were restricted due to intrinsic factors of participant enrolment in the study. To improve the generalizability of the sample, patients were somewhat heterogeneous with regard to psychopharmacological treatment regimen and were seeking psychiatric care. The current sample size was not powered to examine these variables in the analysis. We also used a sample augmentation technique to address control-patient class imbalance in our sample. While steps were taken to minimise bias associated with sample augmentation, this technique is not equivalent to enrolling real study participants. Moreover, the DDNOS group contained only three patients, which prohibited us from including them in the supervised learning analysis. Additional work is needed to understand predictors of suicidal behaviours in this diagnostic group. Our sample was also limited to individuals who were assigned female sex at birth – a group historically excluded from research. These results may not be generalisable beyond this sex. Future research should focus on replicating the results in a larger more generalisable sample.
In summary, AI techniques use algorithms to identify patterns in data with minimal intervention – thus, hopefully reducing human bias in how patterns and predictors are identified. Here we used AI approaches to: (1) identify clusters of patients that mapped onto a spectrum of dissociation severity; and (2) to predict suicide attempt with levels of accuracy seen in much larger samples. These insights provide an important validation of clinical experience and prior foundational research with data-driven methodologies. Most importantly, these findings underscore the need to assess for particular types of dissociation to identify individuals at high-risk of suicidal self-injury.
Supplemental Material
Download MS Word (1.4 MB)Acknowledgements
Suhas Srinivasan: Data Curation, Methodology, Software, Investigation, Validation, Formal analysis, Visualisation, Writing – Original Draft; Nathaniel Harnett: Methodology, Writing – Review & Editing; Liang Zhang: Data Curation, Methodology, Software, Investigation, Validation, Resources; Junbong Jang: Data Curation, Methodology, Software; Senbao Lu: Data Curation, Methodology; Mohamed Eltabakh: Conceptualisation, Supervision, Writing – Review & Editing, Funding acquisition; Blaise Frederick: Data curation, Methodology, Software, Validation, Writing – Review & Editing, Funding acquisition; Jean King: Conceptualisation, Supervision, Funding acquisition; Benjamin Nephew: Conceptualisation, Supervision, Project administration, Writing – Review & Editing, Funding acquisition; M. Kathryn Dahlgren: Methodology, Data Curation, Writing – Review & Editing; Staci Gruber: Conceptualisation, Investigation, Supervision, Writing – Review & Editing; Cori Palermo: Investigation, Resources, Data Curation, Visualisation; Xi Pan: Validation, Writing – Review & Editing; Milissa Kaufman: Conceptualisation, Investigation, Resources, Writing – Review and Editing, Supervision, Project Administration, Funding acquisition; Kerry Ressler: Conceptualisation, Writing – Review & Editing, Supervision, Funding acquisition; Sherry Winternitz: Writing – Review & Editing; Dmitry Korkin: Conceptualisation, Investigation, Supervision, Writing – Review & Editing, Funding acquisition; Lauren Lebois: Conceptualisation, Investigation, Resources, Data Curation, Writing – Review & Editing.
Disclosure statement
Dr. Lebois reports unpaid membership on the Scientific Committee for the International Society for the Study of Trauma and Dissociation (ISSTD), grant support from the National Institute of Mental Health (NIMH), K01 MH118467, and the Julia Kasparian Fund for Neuroscience Research. Dr. Lebois also reports spousal IP payments from Vanderbilt University for technology licensed to Acadia Pharmaceuticals unrelated to the present work. Dr. Kaufman reports unpaid membership on the Scientific Committee for the ISSTD and grant support from the NIMH, R21 MH112956, R01 MH119227. ISSTD and NIMH were not involved in the analysis or preparation of the manuscript. Dr. Ressler reports having performed scientific consultation for Bioxcel, Bionomics, Acer, Takeda, and Jazz Pharmaceuticals. Dr. Ressler also serves on Scientific Advisory Boards for Sage and the Brain Research Foundation. Dr. Ressler has received sponsored research support from Takeda, Brainsway and Alto Neuroscience. Dr. Korkin reports having performed scientific consultation for Syndax. Dr. Frederick reports having performed scientific consultation for Axial Biotherapeutics and Charles River Analytics and grant support from NIDA under R01DA048150 and R01DA039135.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Additional information
Funding
Related Research Data
References
- Afifi, T. O., Enns, M. W., Cox, B. J., Asmundson, G. J. G., Stein, M. B., & Sareen, J. (2008). Population attributable fractions of psychiatric disorders and suicide ideation and attempts associated with adverse childhood experiences. American Journal of Public Health, 98(5), 946–952. https://doi.org/10.2105/AJPH.2007.120253
- Allen, M., Poggiali, D., Whitaker, K., Marshall, T. R., & Kievit, R. A. (2019). Raincloud plots: A multi-platform tool for robust data visualization. Wellcome Open Res, 4(63), 1–46. https://doi.org/10.12688/wellcomeopenres.15191.1
- American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Pub.
- Barlow, M. R., & Chu, J. A. (2014). Measuring fragmentation in dissociative identity disorder: The integration measure and relationship to switching and time in therapy. European Journal of Psychotraumatology, 5(1), 1–8. https://doi.org/10.3402/ejpt.v5.22250
- Beck, A. T., Steer, R. A., & Brown, G. (1996). Beck depression inventory–II. Psychological assessment.
- Bernstein, D.P., Fink, L., Handelsman, L., Foote, J., Lovejoy, M., Wenzel, K., Sapareto, E., & Ruggiero J. (1994). Initial reliability and validity of a new retrospective measure of child abuse and neglect. American Journal of Psychiatry, 151(1), 1132–1136. https://doi.org/10.1176/ajp.151.1.18
- Bruffaerts, R., Demyttenaere, K., Borges, G., Haro, J. M., Chiu, W. T., Hwang, I., Karam, E. G., Kessler, R. C., Sampson, N., Alonso, J., Andrade, L. H., Angermeyer, M., Benjet, C., Bromet, E., de Girolamo, G., de Graaf, R., Florescu, S., Gureje, O., Horiguchi, I., … Nock, M. K. (2010). Childhood adversities as risk factors for onset and persistence of suicidal behaviour. British Journal of Psychiatry, 197(1), 20–27. https://doi.org/10.1192/bjp.bp.109.074716
- Burke, T. A., Ammerman, B. A., & Jacobucci, R. (2019). The use of machine learning in the study of suicidal and non-suicidal self-injurious thoughts and behaviors: A systematic review. Journal of Affective Disorders, 245, 869–884. https://doi.org/10.1016/j.jad.2018.11.073
- Buse, A. The likelihood ratio, Wald. (1982). And Lagrange multiplier tests: An expository note. American Statistical Association, 36(3), 153–157.
- Calati, R., Bensassi, I., & Courtet, P. (2017). The link between dissociation and both suicide attempts and non-suicidal self-injury: Meta-analyses. Psychiatry Research, 251, 103–114. https://doi.org/10.1016/j.psychres.2017.01.035
- Carlson, E. B., & Putnam, F. W. (1993). An update on the dissociative experiences scale. Dissociation: Progress in the Dissociative Disorders, 6, 16–27.
- Chawla, N. V., Bowyer, K. W., Hall, L. O., & Kegelmeyer, W. P. (2002). SMOTE: Synthetic minority over-sampling technique. Journal of Artificial Intelligence Research, 16, 321–357. https://doi.org/10.1613/jair.953
- Copeland, W.E., Shanahan, L., Hinesley, J., Chan, R.F., Aberg, K.A., Fairbank, J.A., van den Oord, E.J. and Costello, E.J. (2018). Association of childhood trauma exposure with adult psychiatric disorders and functional outcomes. JAMA Network Open, 1(7), e184493–e184493. https://doi.org/10.1001/jamanetworkopen.2018.4493
- Dalenberg, C. J., Brand, B. L., Gleaves, D. H., Dorahy, M. J., Loewenstein, R. J., Cardeña, E., Frewen, P. A., Carlson, E. B., & Spiegel, D. (2012). Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychological Bulletin, 138(3), 550–588. https://doi.org/10.1037/a0027447
- Delgado-Gomez, D., Baca-Garcia, E., Aguado, D., Courtet, P., & Lopez-Castroman, J. (2016). Computerized Adaptive Test vs. decision trees: Development of a support decision system to identify suicidal behavior. Journal of Affective Disorders, 206, 204–209. https://doi.org/10.1016/j.jad.2016.07.032
- Dell, P. F. (2006). The multidimensional inventory of dissociation (MID): A comprehensive measure of pathological dissociation. Journal of Trauma & Dissociation, 7(2), 77–106. https://doi.org/10.1300/J229v07n02_06
- Dell, P. F. (2010). 15 The Phenomena of Pathological Dissociation. Dissociation and the dissociative disorders: DSM-V and beyond 225.
- Dell, P. F., Coy, D. M., & Madere, J. (2017). An interpretive manual for the multidimensional inventory of dissociation (MID). Preprint at https://www.mid-assessment.com/wp-content/uploads/2020/05/An-Interpretive-Manual-for-the-Multidimensional-Inventory-of-Dissociation-MID-3rd-Edition.pdf.
- Dube, S. R., Anda, R. F., Felitti, V. J., Chapman, D. P., Williamson, D. F., & Giles, W. H. (2001). Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: Findings from the Adverse Childhood Experiences Study. JAMA, 286(24), 3089–3096. https://doi.org/10.1001/jama.286.24.3089
- Dwyer, D. B., Falkai, P., & Koutsouleris, N. (2018). Machine learning approaches for clinical psychology and psychiatry. Annual Review of Clinical Psychology, 14(1), 91–118. https://doi.org/10.1146/annurev-clinpsy-032816-045037
- Edgcomb, J. B., Thiruvalluru, R., Pathak, J., & Brooks, J. O. 3rd (2021). Machine learning to differentiate risk of suicide attempt and self-harm after general medical hospitalization of women With mental illness. Medical Care, 59, S58–S64. https://doi.org/10.1097/MLR.0000000000001467
- Eidhof, M. B., Djelantik, A. A. A. M. J., Klaassens, E. R., Kantor, V., Rittmansberger, D., Sleijpen, M., Steenbakkers, A., Weindl, D., & ter Heide, F. J. J. (2019). Complex posttraumatic stress disorder in patients exposed to emotional neglect and traumatic events: Latent class analysis. Journal of Traumatic Stress, 32(1), 23–31. https://doi.org/10.1002/jts.22363
- Foote, B., Smolin, Y., Neft, D. I., & Lipschitz, D. (2008). Dissociative disorders and suicidality in psychiatric outpatients. Journal of Nervous & Mental Disease, 196(1), 29–36. https://doi.org/10.1097/NMD.0b013e31815fa4e7
- Ford, J. D., & Gómez, J. M. (2015). Self-injury and suicidality: The impact of trauma and dissociation. Journal of Trauma & Dissociation, 16(3), 225–231. https://doi.org/10.1080/15299732.2015.989648
- Fortgang, R. G., Wang, S. B., Millner, A. J., Reid-Russell, A., Beukenhorst, A. L., Kleiman, E. M., Bentley, K. H., Zuromski, K. L., Al-Suwaidi, M., Bird, S. A., Buonopane, R., DeMarco, D., Haim, A., Joyce, V. W., Kastman, E. K., Kilbury, E., Lee, H.-I. S., Mair, P., Nash, C. C., … Nock, M. K. (2021). Increase in suicidal thinking during COVID-19. Clinical Psychological Science, 9(3), 482–488. https://doi.org/10.1177/2167702621993857
- Frewen, P., & Lanius, R. (2015). Healing the Traumatized Self: Consciousness, Neuroscience, Treatment (Norton Series on Interpersonal Neurobiology). W. W. Norton & Company.
- Fukunaga, K., & Narendra, P. M. (1975). A branch and bound algorithm for computing k-nearest neighbors. IEEE Transactions on Computers, 24(7), 750–753. https://doi.org/10.1109/T-C.1975.224297
- Hawton, K., Saunders, K., Topiwala, A., & Haw, C. (2013). Psychiatric disorders in patients presenting to hospital following self-harm: A systematic review. Journal of Affective Disorders, 151(3), 821–830. https://doi.org/10.1016/j.jad.2013.08.020
- Hill, S. B., Wolff, J. D., Bigony, C. E., Winternitz, S. R., Ressler, K. J., Kaufman, M. L., & Lebois, L. A. M. (2020). Dissociative subtype of posttraumatic stress disorder in women in partial and residential levels of psychiatric care. Journal of Trauma & Dissociation, 21(3), 305–318. https://doi.org/10.1080/15299732.2019.1678214
- Holland, K. M., Jones, C., Vivolo-Kantor, A. M., Idaikkadar, N., Zwald, M., Hoots, B., Yard, E., D’Inverno, A., Swedo, E., Chen, M. S., Petrosky, E., Board, A., Martinez, P., Stone, D. M., Law, R., Coletta, M. A., Adjemian, J., Thomas, C., Puddy, R. W., … Houry, D. (2021). Trends in US emergency department visits for mental health, overdose, and violence outcomes before and during the COVID-19 pandemic. JAMA Psychiatry, 78(4), 372–379. https://doi.org/10.1001/jamapsychiatry.2020.4402
- Kotsiantis, S. B. (2007). Supervised machine learning: A review of classification techniques. Informatica, 31(1), 249–268.
- Liaw, A., & Wiener, M. (2002). Classification and Regression by randomForest. R News 2, 18–22.
- Sar, V., & Ross, C. (2006). Dissociative disorders as a confounding factor in psychiatric research. Psychiatric Clinics of North America, 29(1), 129–144. https://doi.org/10.1016/j.psc.2005.10.008
- Schneider, K. (1959). Clinical Psychopathology. Grune & Stratton.
- Shepard, D. S., Gurewich, D., Lwin, A. K., Reed, G. A., Jr, & Silverman, M. M. (2016). Suicide and suicidal attempts in the United States: Costs and policy implications. Suicide and Life-Threatening Behavior, 46(3), 352–362. https://doi.org/10.1111/sltb.12225
- Shinn, A. K., Wolff, J. D., Hwang, M., Lebois, L. A. M., Robinson, M. A., Winternitz, S. R., Öngür, D., Ressler, K. J., & Kaufman, M. L. (2019). Assessing voice hearing in trauma spectrum disorders: A comparison of two measures and a review of the literature. Frontiers in Psychiatry, 10, 1011. https://doi.org/10.3389/fpsyt.2019.01011
- Somer, E., & Dell, P. F. (2005). Development of the Hebrew-Multidimensional Inventory of Dissociation (H-MID): a valid and reliable measure of pathological dissociation. Journal of Trauma & Dissociation, 6(1), 31–53. https://doi.org/10.1300/J229v06n01_03
- Srinivasan, S., Leshchyk, A., Johnson, N. T., & Korkin, D. (2020). A hybrid deep clustering approach for robust cell type profiling using single-cell RNA-seq data. RNA, 26(10), 1303–1319. https://doi.org/10.1261/rna.074427.119
- Steinberg, M. (1994). Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D). American Psychiatric Press.
- Szumilas, M. (2010). Explaining odds ratios. European Child & Adolescent Psychiatry, 19(3), 227–229. https://doi.org/10.1007/s00787-010-0087-7
- Theodoridis, S., & Koutroumbas, K. (2008). Pattern Recognition, 4th edition. vol. 19. Academic Press, 376.
- Torous, J., Larsen, M.E., Depp, C., Cosco, T.D., Barnett, I., Nock, M.K. and Firth, J. (2018). Smartphones, sensors, and machine learning to advance real-time prediction and interventions for suicide prevention: a review of current progress and next steps. Current psychiatry reports, 20(7), 1–6.
- Van der Maaten, L., & Hinton, G. (2008). Visualizing data using t-SNE. Journal of Machine Learning Research, 9(11), 2579–2605.
- Vine, V., Victor, S. E., Mohr, H., Byrd, A. L., & Stepp, S. D. (2020). Adolescent suicide risk and experiences of dissociation in daily life. Psychiatry Research, 287, 112870. https://doi.org/10.1016/j.psychres.2020.112870
- Weathers, F. W., Bovin, M. J., Lee, D. J., Sloan, D. M., Schnurr, P. P., Kaloupek, D. G., Keane, T. M., & Marx, B. P. (2018). The clinician-administered PTSD scale for DSM-5 (CAPS-5): development and initial psychometric evaluation in military veterans. Psychological Assessment, 30(3), 383–395. https://doi.org/10.1037/pas0000486
- Weathers, F. W., Litz, B. T., Keane, T. M., Palmieri, P. A., Marx, B. P., & Schnurr, P. P. (2013). The PTSD checklist for DSM-5 (PCL-5). Scale available from the National Center for PTSD at www.ptsd.va.gov.
- Wilcoxon, F. (1992). Individual comparisons by ranking methods. In K. Samuel & L.J. Norman (Eds.), Springer Series in Statistics (pp. 196–202). Springer New York. https://doi.org/10.1007/978-1-4612-4380-9_16.
- Wolf, E. J., Lunney, C. A., Miller, M. W., Resick, P. A., Friedman, M. J., & Schnurr, P. P. (2012). The dissociative subtype of PTSD: A replication and extension. Depression and Anxiety, 29(8), 679–688. https://doi.org/10.1002/da.21946
- World Health Organization. (2014). Preventing Suicide: A Global Imperative.
- Yard, E., Radhakrishnan, L., Ballesteros, M. F., Sheppard, M., Gates, A., Stein, Z., Hartnett, K., Kite-Powell, A., Rodgers, L., Adjemian, J., Ehlman, D. C., Holland, K., Idaikkadar, N., Ivey-Stephenson, A., Martinez, P., Law, R., & Stone, D. M. (2021). Emergency department visits for suspected suicide attempts Among persons aged 12-25 years before and during the COVID-19 pandemic - United States, January 2019–May 2021. MMWR Morbidity and Mortality Weekly Report, 70(24), 888–894. https://doi.org/10.15585/mmwr.mm7024e1