
ABSTRACT
Background: Intrusive memories form a core symptom of Posttraumatic Stress Disorder (PTSD). Based on concepts of visuospatial interference and memory-updating accounts, technological innovations aim to attenuate such intrusions using visuospatial interventions.
Objective: This study aims to test the effect of a visuospatial Tetris-based intervention versus a verbal condition (Wiki) and a never-targeted control (no intervention) on intrusion frequency.
Method: A randomized crossover trial was conducted including N = 38 PTSD patients who had at least 3 distinct intrusive memories of trauma. After both 2 weeks (intervention 1) and 4 weeks (intervention 2), one of the three memories was randomly selected and either the visuospatial intervention (memory reminder of a traumatic memory + Tetris) or verbal condition (reading a Wikipedia article + answering questions) was performed on their first memory in randomized order. In the week 4 session, the patient conducted the other intervention condition on their second memory (crossover). The third memory was never targeted (no intervention). Daily occurrence of intrusions over 8 weeks was collected using a diary and analysed using mixed Poisson regression models.
Results: Overall, there was no significant reduction in intrusion frequency from either intervention compared to each other, and to no intervention control (relative risk Tetris/Wiki: 0.947; p = .31; relative risk no intervention/Tetris: 1.060; p = .15; relative risk no intervention/Wiki: 1.004; p = .92).
Conclusions: There was no effect of either intervention on intrusions when administered in a crossover design where participants received both interventions. Design shortcomings and consequences for future studies are discussed.
HIGHLIGHTS
Visuospatial interventions, including the computer game Tetris, have been studied as a potential means to decrease intrusive memories, a core feature of Posttraumatic Stress Disorder.
In this study, two interventions are tested in a crossover design with patients with intrusive memories after traumatic experiences.
There was no effect of either the visuospatial intervention or the verbal condition in this design.
Antecedentes: Los recuerdos intrusivos constituyen un síntoma central del Trastorno de Estrés Postraumático (TEPT). Basándose en conceptos de interferencia visoespacial y capacidad de actualización de la memoria, las innovaciones tecnológicas buscan como objetivo atenuar tales intrusiones, utilizando intervenciones visoespaciales.
Objetivo: Este estudio tiene como objetivo evaluar el efecto de una intervención visoespacial basada en el Tetris, en comparación con una condición verbal (Wiki) y un grupo control sin intervención (ninguna intervención), sobre la frecuencia de las intrusiones.
Método: Se llevó a cabo un ensayo aleatorizado cruzado, que incluyó N = 38 pacientes con TEPT, que tenían al menos 3 recuerdos intrusivos distintivos de trauma. Después de 2 semanas (intervención 1) y 4 semanas (intervención 2), se seleccionó al azar uno de los tres recuerdos y se realizó la intervención visoespacial (recordatorio de un recuerdo traumático + Tetris) o la condición verbal (lectura de un artículo de Wikipedia + responder preguntas) realizado sobre su primer recuerdo en orden aleatorio. En la sesión de la semana 4, el paciente realizó la otra condición de intervención (cruzado), sobre su segundo recuerdo. El tercer recuerdo nunca fue intervenido (sin intervención). La ocurrencia diaria de intrusiones durante 8 semanas se recopiló mediante un diario y se analizó utilizando modelos de regresión mixtos de Poisson.
Resultados: En general, no hubo una reducción significativa en la frecuencia de las intrusiones a partir de ninguna de las intervenciones comparadas entre sí, y tampoco con el control sin intervención (riesgo relativo Tetris/Wiki: 0.947; p = .31; riesgo relativo sin intervención/Tetris: 1.060; p = .15; riesgo relativo sin intervención/Wiki: 1.004; p = .92).
Conclusiones: No hubo un efecto en ninguna de las intervenciones sobre las intrusiones, cuando se administraron en un diseño cruzado donde los participantes recibieron ambas intervenciones. Se discuten las deficiencias del diseño y las consecuencias para estudios futuros.
1. Introduction
Posttraumatic stress disorder (PTSD) has a high world-wide prevalence (Atwoli et al., Citation2015; Kessler et al., Citation2005), with recurrent intrusive memories of trauma, which are involuntary and distressing, as the core clinical symptom (American Psychiatric Association, Citation2013; Kupfer & Regier, Citation2011). Existing treatments are effective (Schäfer et al., Citation2019), but many of them are limited in accessibility. For example, even when a gold standard treatment such as trauma-focused cognitive therapy is delivered in a digital format rather than in person, the therapist time was only halved (Ehlers et al., Citation2023). Further, treatments such as prolonged exposure or other trauma-focused cognitive therapies can require highly qualified therapists to be delivered, are time-consuming, costly and typically imply significant emotional distress whereby patients narrate their trauma in detail as part of the therapy (Schäfer et al., Citation2019). In contrast, treatments like Narrative Exposure Therapy (Ellis & Jones, Citation2022; Neuner et al., Citation2008) can also achieve good results with lay or semi-professional therapists, and have been associated with fewer concerns about emotional distress. There is evidence that trauma-focused treatments can come with particularly high drop-out rates, although this is still a topic of debate (see, e.g. Imel et al., Citation2013). Hence, on a global scale, the majority of patients do not receive any form of treatment for PTSD (Schreiber et al., Citation2009), causing enormous suffering and societal costs (Kessler , Citation2000).
Consequently, there is a need for new therapeutic approaches that (1) are widely available and free/inexpensive for patients, (2) can be easily administered (even by lay people rather than mental health professionals), (3) are cost-efficient, (4) less distressing and (5) effective. The approach presented here meets these demands, as just one key symptom of PTSD (intrusive memories) is targeted in a mechanistically-driven intervention (Holmes et al., Citation2009; Singh et al., Citation2020). Further, the intervention is relatively simple and could be provided by non-specialists.
Since intrusions are mostly visual representations of traumatic memories, visuospatial tasks have repeatedly been examined in tests of this emerging intervention approach, guided by two concepts: dual-task interference and memory-updating accounts. Tasks conducted simultaneously compete for the same limited working memory resources (Baddeley, Citation2012), leading to an interference effect. Performing a visuospatial task while simultaneously activating inner mental images is thought to yield a weakening of the vividness and emotionality of the latter (Baddeley & Andrade, Citation2000; Engelhard et al., Citation2010). Memory-updating (or reconsolidation) accounts posit that already consolidated memories can be labilised by reactivating them, and can then be modified within a certain time window (Alberini, Citation2005; Nader & Einarsson, Citation2010). Theoretically grounded in both interference and memory-updating approaches, the aim is to provide a memory reminder cue for a traumatic visual memory, render it labile and let a concurrent visuospatial task interfere with its so-called reconsolidation to affect that specific memory fragment and render it less intrusive. We have also developed bespoke procedures to deliver this intervention approach, informed by the type of patient preference and context (e.g. Kessler et al., Citation2018).
Much experimental research on this approach has used the computer game Tetris as a visuospatial task within the framework of the ‘trauma film’ paradigm (Holmes & Bourne, Citation2008; James et al., Citation2016). After viewing a trauma film, healthy participants that played Tetris after a reminder cue, had less intrusions compared to e.g. verbal control conditions (e.g. Holmes et al., Citation2009, Citation2010), with moderate to large effect sizes. This effect is also apparent when the reminder cue procedure plus Tetris was done at 24 h (James et al., Citation2015) or even 72 h (Hagenaars et al., Citation2017; Kessler et al., Citation2020) afterwards, with large effect sizes in James et al. (Citation2015), and moderate to large effect sizes in Kessler et al. (Citation2020). Since there was a reminder of the intrusive memories shortly before playing Tetris, those studies draw on the method steps suggested by a memory-updating account (Visser et al., Citation2018).
Furthermore, a small number of clinical studies have now applied these novel behavioural interventions to patients. Intrusion frequency could be reduced for patients in an emergency room after road traffic accidents in the UK (Iyadurai et al., Citation2018) and Sweden (Kanstrup, Singh, et al., Citation2021) or after traumatic childbirth (Horsch et al., Citation2017). In a single case series with 4 refugees with PTSD, a novel intervention containing Tetris led to a reduction of intrusion frequency (Kanstrup, Kontio, et al., Citation2021). Since designing the current study, further studies are emerging, including after traumatic childbirth (Deforges et al., Citation2023), with an impact on PTSD at 6 months, and in intensive care healthcare staff exposed to trauma in their work (Iyadurai et al., Citation2023; Ramineni et al., Citation2023).
A critical question is whether experimental and early clinical studies typically applied very soon after a traumatic event occurred, could also extend to older long-standing memories of trauma that occurred many years ago. In the first study of long standing trauma many years old, 20 inpatients with complex PTSD received weekly sessions including writing down the content of a specific traumatic memory and playing Tetris afterwards (Kessler et al., Citation2018). The memory reactivation procedure was developed together with the inpatients to ensure it was acceptable to them, and involved their writing down the trauma in a way they did not need to share with the experimenter, and then shredding it. The intrusion frequency of the memories that were targeted by this intervention was reduced by on average 64% compared to a reduction of only 11% for the memories that were never targeted. This study from our group, and the first on longstanding trauma, was promising but had a major limitation: there was no control condition to compare the experimental intervention with.
Hence, the current study is the first application of this bespoke adaption of the novel behavioural visuospatial intervention from Kessler et al. (Citation2018) with inpatients, here in a within-patient randomized controlled trial with outpatients suffering from trauma-related disorders. Critical to our design is that one person typically has more than one different intrusive memory (Grey & Holmes, Citation2008). Distributed over 8 weeks, within one patient, three different intrusive memories randomly received either the visuospatial Tetris-based intervention, or a verbal condition (Wiki), or no intervention at all.
The main hypothesis is that the visuospatial Tetris-based intervention will lead to a significant reduction in the frequency of intrusions of the targeted memory compared to both the verbal condition (Wiki), and the no intervention control.
2. Materials and methods
2.1. Participants
Study participants were recruited from the outpatient unit of the Department of Psychosomatic Medicine and Psychotherapy, LWL-University Hospital, Ruhr-Universität Bochum. Inclusion criteria were: more than 18 years of age, fulfil Criterion A of the DSM-5 diagnosis of PTSD, experience at least three distinguishable intrusive memories in the form of recurrent intrusions, sufficient knowledge of the German language. Exclusion criteria were: acute suicidal tendencies, severe self-harming behaviour, substance abuse, or psychotic symptoms within the last six months.
The study received approval from the Ethics Committee of the Medical Faculty of Ruhr-University Bochum, Germany (Ref.-No. 20-6841). The study was pre-registered with the ISRCTN registry (ISRCTN17247193) on 13/11/2020, prior to start of patient recruitment. We report how we determined our sample size, all data exclusions (if any), all manipulations, and all measures in the study. Data, study materials, and the intervention manual are available from the corresponding author upon request.
2.2. Procedure
The study was conducted as a within-patient randomized controlled trial (see below) with 4 study appointments (T0 – T3) over the course of 8 weeks (see ). At T0, patients were asked to identify three memories from (one or several) traumatic events that occur regularly as intrusions (i.e. three intrusive memories with different content). The three most distressing/frequent intrusive memories were chosen to be monitored. These memories were numbered (1–3), labelled with a keyword, and self-recorded from then on. To continue the study and be included in analyses, patients had to experience each of the 3 intrusive memories at least once per week in the 2-week baseline interval before T1.
Figure 1. Study design.
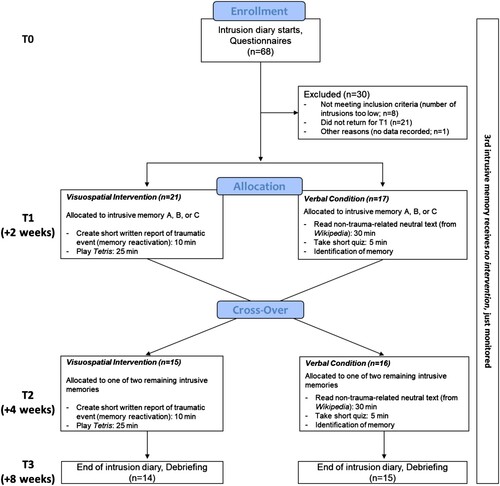
At T1, patients received the first of two interventions, specifically targeted on one of the three intrusive memories defined (both, intervention and memory, selected randomly, using REDCap software; Harris et al., Citation2009; Harris et al., Citation2019): either the visuospatial intervention (Tetris), or the verbal condition (Wiki). Two weeks later (T2), patients received the other intervention randomly targeted on one of the two remaining intrusive memories. Four weeks later (T3), patients returned to the lab for a short debriefing questionnaire and collection of the intrusion diary. The third (remaining) memory has thus never been targeted (no intervention). Although we did not expect any specific effects on intrusion frequency from the verbal condition (Wiki), it would be possible to have non-specific effects of receiving attention, being taken care of, or other factors contributing to a Placebo effect. The memory that was never targeted was therefore included in the diary to have a measure of a ‘naturalistic’ course of intrusion frequency and to have the possibility to compare it to both the verbal Wiki-condition (as a measure of potential non-specific effects) and the visuospatial Tetris-based intervention.
Note that in a standard cross-over design, the different interventions are aimed at the same medical condition, whereas in our within-patient design we randomly target different trauma memories within each patient (Nair, Citation2019), see also Kessler et al. (Citation2018).
2.3. Intrusion diary
A daily intrusion diary was used to record intrusion frequency over the 8-week-course of the study. It was adapted from versions used in previous studies (e.g. Holmes et al., Citation2010; Iyadurai et al., Citation2018; Kessler et al., Citation2018, Citation2020). The three defined intrusive memories at T0 were recorded separately to detect potential specific effects of an intervention on that memory.
The diary was available both in paper (as in Kessler et al., Citation2018) and optionally in digital form. The digital version was implemented using the electronic data capture system REDCap (Research Electronic Data Capture; Harris et al., Citation2019; Citation2009). In the digital version, patients received daily emails containing a hyperlink to the digital intrusion diary, in which the number of intrusions for each of the three memories (and total number of intrusions of other memories) were entered once every 24 h. If participants preferred to use the paper version of the intrusion diary, they were instructed to fill it in at least every 24 h (preferably at the same time of the day each time), but were free to carry it with them and update it more often (e.g. each time an intrusion occurred).
2.4. Visuospatial Tetris-based intervention
This intervention consisted of two phases, a memory reminder procedure targeting one of the three traumatic memories (hypothesized to reactivate the memory and render it labile), followed by 25 min of Tetris gameplay. First, patients were asked to create a written report of the memory chosen randomly at the beginning of the appointment (total duration ∼10 min). The instruction was to describe the memory as visually and vividly as possible with details to facilitate activation of the traumatic memory. Based on our previous research, and to help patients report on their memories yet keep their writing private, participants were told that the report would be directly destroyed afterwards without anyone reading it. Afterwards, they played the computer game Tetris (by N3TWORK, Citation2020) on a 10.1-inch Samsung Galaxy A6 Tablet Computer for 25 min. (for details see Kessler et al., Citation2018). Patients were instructed to focus on the ‘mental rotation’ aspect, and to play continuously for the whole 25 min. The focus on ‘mental rotation’ was emphasized in order to maximize visuospatial processing, which according to the theoretical foundations of this experimental paradigm should create a stronger interference effect due to competition for limited working memory resources (see Introduction).
2.5. Verbal condition (Wiki)
In the verbal condition, patients were asked to read a shortened Wikipedia article about Postage Stamps (in German; Wikipedia, Citation2021) on a tablet computer and were informed that they would have to answer multiple-choice questions afterwards. Estimated reading time of the article was ∼30 min, and reading of the article was interrupted after 30 min if participants were not finished. Afterwards, participants were given 8 multiple-choice questions with 4 choice options (A-D), which took about 5 min to answer. Hence, both conditions were similar in mode of delivery (via tablet computer) and duration (∼35 min). Finally, one of the (remaining) intrusive memories was randomly selected and patients were informed that the task had been delivered to target that specific memory.
2.6. Power analysis
To calculate the sample size, an analogue Poisson model has been fitted to data from a previous uncontrolled before-after study with the visuospatial Tetris-based intervention in our clinic (Kessler et al., Citation2018). In this study, frequency of intrusions could be reduced by the intervention with a relative risk of .63 compared to no intervention. Additionally, a variance-covariance matrix for random effects has been derived from this model. Furthermore, for sample size determination we assume that the effect of the verbal condition (Wiki) is only half as strong as the observed effect of the visuospatial Tetris-based intervention (on the additive scale of the linear predictor in the Poisson regression) resulting in the assumption of a relative reduction of 0.8 compared to no intervention. Running a simulation with 1000 iterations (R package simr) revealed a power of approximately 81% to detect differences between the visuospatial intervention and the verbal condition (RR = 0.63/0.8; two-tailed testing with type I error of 5%) with 40 study patients. Simulations have been run at the department of Medical Informatics, Biometry and Epidemiology of the Ruhr-University Bochum.
2.7. Statistical analysis
The main outcome variable was the number of intrusions per day, counted separately for each of the three intrusive memories. Analyses were performed as Intention-to-Treat-analyses (ITT), including all patients who had submitted data into the intrusion diary and were randomized at T1. To test our hypothesis whether the visuospatial Tetris-based intervention reduced intrusion frequency more than the verbal condition (Wiki), a mixed Poisson regression was modelled, with intervention type as a fixed effect and random effects for patient (individual intrusion frequency), intrusive memory (individual intrusion frequency per memory), and day (variation in individual intrusion frequency per day). Outcomes are reported as risk ratios.
Analyses were performed with R statistics, version 3.6.2 (R Core Team, Citation2013; Function glmer; CRAN, Comprehensive R Archive Network, open-source) with package Ime4 (Bates et al., Citation2015) and for the calculation of contrasts package emmeans (Lenth, Citation2022).
3. Results
A total of N = 38 participants (of N = 68 recruited, see ) were included in the Intention-To-Treat analyses. The mean age of participants was 42.2 years (SD 13.3 years), N = 31 participants (81.6%) were female. Mean time interval between the traumatic event(s) (in case of complex trauma calculated using the last given time point) and study participation was 13.8 years (SD = 15.0 years). Demographic characteristics, main diagnosis and comorbid diagnoses, as well as previous treatments are reported in .
Table 1. Demographic data and clinical background.
Intrusion frequencies at baseline were comparable across experimental conditions (see ). Please see for descriptive data of intrusion frequency pre- and post-intervention over both interventions for the whole group, as well as descriptive data with the sample split in two subgroups, depending on which intervention was delivered first (Tetris vs Wiki), in order to identify possible order effects.
Table 2. Number of Intrusions / day.
In the Poisson regression, it was observed that the memory that received the visuospatial Tetris-based intervention showed a non-significant relative risk reduction regarding intrusion frequency of only 5.3%, compared to the memory that received the verbal Wiki-condition (risk ratio: 0.947; 95%-CI: 0.85–1.05; p = .31). There also were no significant differences between the no intervention control and the visuospatial Tetris-based intervention (risk ratio: 1.060; 95%-CI: 0.98–1.15; p = .15), or between no intervention control and the verbal Wiki-condition (risk ratio: 1.004; 95%-CI: 0.93-1.09; p = .92).
4. Discussion
In this study, we applied the same behavioural imagery-competing task intervention (here using a bespoke reminder procedure previously developed with inpatients, alongside Tetris gameplay) as in Kessler et al. (Citation2018), a case series study of inpatients with complex PTSD. We have advanced the previous initial findings by here using a within-patients RCT with a larger patient sample (N = 38 vs. 20), and by including both a verbal and a no intervention control comparison. There was no significant difference between the three conditions in this cross over design.
It is possible that the lack of a significant result may at least in part be due to methodological reasons. The main advantage of our specific design within the framework of RCTs is that it allows for relatively smaller numbers of participants, as each participant receives both conditions (within-patient design). At this early stage of clinical research into our novel intervention, we attempted to keep participant numbers small for ethical and pragmatic reasons. As a major drawback, this design may produce carry-over effects: Since each participant received both interventions just in a different order (and with only 2 weeks in between), the intrusion frequency at T2 might have been influenced by any of the two conditions without being able to disentangle the effects. This assumption is descriptively supported by the descriptive statistics () that the group playing Tetris when given first in order had a reduction for both memories, whereas the group reading Wikipedia at first had an increase for the Wiki-targeted memory and virtually no reduction for the memory targeted by Tetris (see ). Results show a different pattern for the second type of intervention delivered raising the possibility of carry-over effects. Hence, statistically, this could have confounded results by introducing order effects.
In order to further investigate the clinical potential of our novel intervention approach, future studies should apply a classical RCT design (two arms, each one receiving just a visuospatial intervention or a control condition) to rule out carry-over effects, and also because such an approach might be less demanding or even less confusing than presenting multiple intervention types to patients with complex PTSD. Future studies also need to assess intrusive memories and other symptoms of PTSD some time later, in order to assess the development or improvement of the symptomatology over longer periods of time.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Alberini, C. M. (2005). Mechanisms of memory stabilization: Are consolidation and reconsolidation similar or distinct processes? Trends in Neurosciences, 28(1), 51–56. https://doi.org/10.1016/j.tins.2004.11.001
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders: Dsm-5 (5th ed). American Psychiatric Publishing. http://swb.eblib.com/patron/FullRecord.aspx?p = 1811753.
- Atwoli, L., Stein, D. J., Koenen, K. C., & McLaughlin, K. A. (2015). Epidemiology of posttraumatic stress disorder: Prevalence, correlates and consequences. Current Opinion in Psychiatry, 28(4), 307–311. https://doi.org/10.1097/YCO.0000000000000167
- Baddeley, A. (2012). Working memory: Theories, models, and controversies. Annual Review of Psychology, 63(1), 1–29. https://doi.org/10.1146/annurev-psych-120710-100422
- Baddeley, A. D., & Andrade, J. (2000). Working memory and the vividness of imagery. Journal of Experimental Psychology: General, 129(1), 126–145. https://doi.org/10.1037/0096-3445.129.1.126
- Bates, D., Mächler, M., Bolker, B., & Walker, S. (2015). Fitting linear mixed-effects models using lme4. Journal of Statistical Software, 67(1), 1–48. https://doi.org/10.18637/jss.v067.i01
- Deforges, C., Sandoz, V., Noël, Y., Avignon, V., Desseauve, D., Bourdin, J., Vial, Y., Ayers, S., Holmes, E. A., Epiney, M. [Emily A.], & Horsch, A. (2023). Single-session visuospatial task procedure to prevent childbirth-related posttraumatic stress disorder: A multicentre double-blind randomised controlled trial. Molecular Psychiatry, 28(9), 3842–3850. https://doi.org/10.1038/s41380-023-02275-w
- Ehlers, A., Wild, J., Warnock-Parkes, E., Grey, N., Murray, H., Kerr, A., Rozental, A., Thew, G., Janecka, M., Beierl, E. T., Tsiachristas, A., Perera-Salazar, R., Andersson, G., & Clark, D. M. (2023). Therapist-assisted online psychological therapies differing in trauma focus for post-traumatic stress disorder (STOP-PTSD): A UK-based, single-blind, randomised controlled trial. The Lancet Psychiatry, 10(8), 608–622. https://doi.org/10.1016/S2215-0366(23)00181-5
- Ellis, K., & Jones, F. (2022). An initial evaluation of narrative exposure therapy as a treatment of posttraumatic stress disorder among Sudanese refugees in Cairo, delivered by lay counselors. Middle East Current Psychiatry, 29(1). https://doi.org/10.1186/s43045-022-00194-0
- Engelhard, I. M., van Uijen, S. L., & van den Hout, M. A. (2010). The impact of taxing working memory on negative and positive memories. European Journal of Psychotraumatology, 1(1). https://doi.org/10.3402/ejpt.v1i0.5623
- Grey, N., & Holmes, E. A. [Emily A.] (2008). “Hotspots” in trauma memories in the treatment of post-traumatic stress disorder: A replication. Memory (Hove, England), 16(7), 788–796. https://doi.org/10.1080/09658210802266446
- Hagenaars, M. A., Holmes, E. A [Emily A.], Klaassen, F., & Elzinga, B. (2017). Tetris and Word games lead to fewer intrusive memories when applied several days after analogue trauma. European Journal of Psychotraumatology, 8(sup1), 1386959. https://doi.org/10.1080/20008198.2017.1386959
- Harris, P. A., Taylor, R., Minor, B. L., Elliott, V., Fernandez, M., O'Neal, L., McLeod, L., Delacqua, G., Delacqua, F., Kirby, J., & Duda, S. N. (2019). The REDCap consortium: Building an international community of software platform partners. Journal of Biomedical Informatics, 95, 103208. https://doi.org/10.1016/j.jbi.2019.103208
- Harris, P. A., Taylor, R., Thielke, R., Payne, J., Gonzalez, N., & Conde, J. G. (2009). Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2), 377–381. https://doi.org/10.1016/j.jbi.2008.08.010
- Holmes, E. A. [Emily A.], & Bourne, C. (2008). Inducing and modulating intrusive emotional memories: A review of the trauma film paradigm. Acta Psychologica, 127(3), 553–566. https://doi.org/10.1016/j.actpsy.2007.11.002
- Holmes, E. A. [Emily A.], James, E. L., Coode-Bate, T., & Deeprose, C. (2009). Can playing the computer game “Tetris” reduce the build-up of flashbacks for trauma? A proposal from cognitive science. PLoS One, 4(1), e4153. https://doi.org/10.1371/journal.pone.0004153
- Holmes, E. A. [Emily A.], James, E. L., Kilford, E. J., & Deeprose, C. (2010). Key steps in developing a cognitive vaccine against traumatic flashbacks: Visuospatial Tetris versus verbal Pub Quiz. PLoS One, 5(11), e13706. https://doi.org/10.1371/journal.pone.0013706
- Horsch, A., Vial, Y., Favrod, C., Harari, M. M., Blackwell, S. E. [Simon E.], Watson, P., Iyadurai, L. [Lalitha], Bonsall, M. B. [Michael B.], & Holmes, E. A. [Emily A.] (2017). Reducing intrusive traumatic memories after emergency caesarean section: A proof-of-principle randomized controlled study. Behaviour Research and Therapy, 94, 36–47. https://doi.org/10.1016/j.brat.2017.03.018
- Imel, Z. E., Laska, K., Jakupcak, M., & Simpson, T. L. (2013). Meta-analysis of dropout in treatments for posttraumatic stress disorder. Journal of Consulting and Clinical Psychology, 81(3), 394–404. https://doi.org/10.1037/a0031474
- Iyadurai, L [L.], Blackwell, S. E [S. E.], Meiser-Stedman, R., Watson, P. C., Bonsall, M. B [M. B.], Geddes, J. R [J. R.], Nobre, A. C., & Holmes, E. A [E. A.] (2018). Preventing intrusive memories after trauma via a brief intervention involving Tetris computer game play in the emergency department: A proof-of-concept randomized controlled trial. Molecular Psychiatry, 23(3), 674–682. https://doi.org/10.1038/mp.2017.23
- Iyadurai, L [Lalitha], Highfield, J., Kanstrup, M., Markham, A., Ramineni, V., Guo, B., Jaki, T., Kingslake, J., Goodwin, G. M., Summers, C., Bonsall, M. B [Michael B.], & Holmes, E. A [Emily A.] (2023). Reducing intrusive memories after trauma via an imagery-competing task intervention in COVID-19 intensive care staff: A randomised controlled trial. Translational Psychiatry, 13(1), 290. https://doi.org/10.1038/s41398-023-02578-0
- James, E. L., Bonsall, M. B [Michael B.], Hoppitt, L., Tunbridge, E. M., Geddes, J. R [John R.], Milton, A. L., & Holmes, E. A [Emily A.] (2015). Computer game play reduces intrusive memories of experimental trauma via reconsolidation-update mechanisms. Psychological Science, 26(8), 1201–1215. https://doi.org/10.1177/0956797615583071
- James, E. L., Lau-Zhu, A., Clark, I. A., Visser, R. M., Hagenaars, M. A., & Holmes, E. A [Emily A.] (2016). The trauma film paradigm as an experimental psychopathology model of psychological trauma: Intrusive memories and beyond. Clinical Psychology Review, 47, 106–142. https://doi.org/10.1016/j.cpr.2016.04.010
- Kanstrup, M., Kontio, E., Geranmayeh, A., Olofsdotter Lauri, K., Moulds, M. L., & Holmes, E. A [Emily A.] (2021a). A single case series using visuospatial task interference to reduce the number of visual intrusive memories of trauma with refugees. Clinical Psychology & Psychotherapy, 28(1), 109–123. https://doi.org/10.1002/cpp.2489
- Kanstrup, M., Singh, L., Göransson, K. E., Widoff, J., Taylor, R. S., Gamble, B., Iyadurai, L [Lalitha], Moulds, M. L., & Holmes, E. A [Emily A.] (2021b). Reducing intrusive memories after trauma via a brief cognitive task intervention in the hospital emergency department: An exploratory pilot randomised controlled trial. Translational Psychiatry, 11(1), 30. https://doi.org/10.1038/s41398-020-01124-6
- Kessler, H., Holmes, E. A [Emily A.], Blackwell, S. E [Simon E.], Schmidt, A.-C., Schweer, J. M., Bücker, A., Herpertz, S., Axmacher, N., & Kehyayan, A. (2018). Reducing intrusive memories of trauma using a visuospatial interference intervention with inpatients with posttraumatic stress disorder (PTSD). Journal of Consulting and Clinical Psychology, 86(12), 1076–1090. https://doi.org/10.1037/ccp0000340
- Kessler, H., Schmidt, A.-C., James, E. L., Blackwell, S. E [Simon E.], Rauchhaupt, M. von, Harren, K., Kehyayan, A., Clark, I. A., Sauvage, M., Herpertz, S., Axmacher, N., & Holmes, E. A [Emily A.] (2020). Visuospatial computer game play after memory reminder delivered three days after a traumatic film reduces the number of intrusive memories of the experimental trauma. Journal of Behavior Therapy and Experimental Psychiatry, 67, 101454. https://doi.org/10.1016/j.jbtep.2019.01.006
- Kessler, R. C [R. C.] (2000). Posttraumatic stress disorder: The burden to the individual and to society. The Journal of Clinical Psychiatry, 61(Suppl 5) Suppl 5, 4-12; discussion 13-4.
- Kessler, R. C [Ronald C.], Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. https://doi.org/10.1001/archpsyc.62.6.593
- Kupfer, D. J., & Regier, D. A. (2011). Neuroscience, clinical evidence, and the future of psychiatric classification in DSM-5. American Journal of Psychiatry, 168(7), 672–674. https://doi.org/10.1176/appi.ajp.2011.11020219
- Lenth, R. V. (2022). emmeans: Estimated MARGINAL MEANS, AKA LEAST-SQUARES MEANS (Version 1.7.2) [Computer software]. https://CRAN.R-project.org/package = emmeans.
- N3TWORK. (2020). Tetris (Android) [Computer software]. https://tetris.com/product/123/tetris-android-mobile.
- Nader, K., & Einarsson, E. O. (2010). Memory reconsolidation: An update. Annals of the New York Academy of Sciences, 1191(1), 27–41. https://doi.org/10.1111/j.1749-6632.2010.05443.x
- Nair, B. (2019). Clinical trial designs. Indian Dermatology Online Journal, 10(2), 193–201. https://doi.org/10.4103/idoj.IDOJ_475_18
- Neuner, F., Onyut, P. L., Ertl, V., Odenwald, M., Schauer, E., & Elbert, T. (2008). Treatment of posttraumatic stress disorder by trained lay counselors in an African refugee settlement: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 76(4), 686–694. https://doi.org/10.1037/0022-006X.76.4.686
- R Core Team. (2013). R: A language and environment for statistical computing [Computer software]. R Foundation for Statistical Computing. Vienna, Austria.
- Ramineni, V., Millroth, P., Iyadurai, L., Jaki, T., Kingslake, J., Highfield, J., Summers, C., Bonsall, M. B., & Holmes, E. A. (2023). Treating intrusive memories after trauma in healthcare workers: A Bayesian adaptive randomised trial developing an imagery-competing task intervention. Molecular Psychiatry, 28(7), 2985–2994. https://doi.org/10.1038/s41380-023-02062-7
- Schäfer, I., Gast, U., Hofmann, A., Knaevelsrud, C., Lampe, A., Liebermann, P., Lotzin, A., Maercker, A., Rosner, R., & Wöller, W. (2019). S3-Leitlinie Posttraumatische Belastungsstörung. Springer.
- Schreiber, V., Renneberg, B., & Maercker, A. (2009). Seeking psychosocial care after interpersonal violence: An integrative model. Violence and Victims, 24(3), 322–336. https://doi.org/10.1891/0886-6708.24.3.322
- Singh, L., Espinosa, L., Ji, J. L., Moulds, M. L., & Holmes, E. A [Emily A.] (2020). Developing thinking around mental health science: The example of intrusive, emotional mental imagery after psychological trauma. Cognitive Neuropsychiatry, 25(5), 348–363. https://doi.org/10.1080/13546805.2020.1804845
- Visser, R. M., Lau-Zhu, A., Henson, R. N., & Holmes, E. A. (2018). Multiple memory systems, multiple time points: How science can inform treatment to control the expression of unwanted emotional memories. Philosophical Transactions of the Royal Society B: Biological Sciences, 373(1742), 20170209. https://doi.org/10.1098/rstb.2017.0209
- Wikipedia. (2021). Briefmarke. https://de.wikipedia.org/wiki/Briefmarke.