
ABSTRACT
Objective: To review the safety and efficacy of early interventions after sexual assault in reducing or preventing posttraumatic stress disorder (PTSD).
Method: Systematic searches were performed on studies (1980–2018) that examined the efficacy of interventions for PTSD within 3 months after sexual assault.
Results: The review identified 7 studies (n = 350) with high risk of bias that investigated 5 interventions. Only two studies reported on safety. Contact with the authors of six studies provided no indications for the occurrence of adverse events. Two studies reported the efficacy using PTSD diagnosis as dependent variable but found no difference between groups. All studies reported on efficacy using PTSD severity as dependent variable. For the meta-analysis, 4 studies (n = 293) were included yielding significantly greater reductions of PTSD severity than standard care at 2 to 12 months follow-up (g = −0.23, 95% CI [−0.46, 0.00]), but not at 1 to 6 weeks post-intervention (g = −0.28, 95% CI [−0.57, 0.02]). The heterogeneity of the interventions precluded further analyses.
Discussion: Findings suggest that early interventions can lead to durable effects on PTSD severity after sexual assault. However, due to limited availability of data, it is impossible to draw definite conclusions about safety and efficacy of early interventions, and their potential to prevent PTSD.
HIGHLIGHTS
• Seven studies have investigated early interventions post-rape.• The studies have a highly diverse design and a high risk of bias.• There is little data on safety and the prevention of posttraumatic stress disorder.• Early intervention can potentially reduce the severity of posttraumatic stress disorder.
Objetivo: revisar la seguridad y eficacia de intervenciones tempranas tras abuso sexual para reducir o prevenir trastorno de estrés postraumático (TEPT).
Método: se realizaron búsquedas sistemáticas sobre estudios (1980-2018) que examinaron la eficacia de intervenciones para TEPT dentro de 3 meses tras un abuso sexual.
Resultados: la revisión identificó 7 estudios (n=350) con alto riesgo de sesgos, que investigaron 5 intervenciones. Sólo 2 estudios reportaron sobre seguridad. El contacto con los autores de 6 estudios no proporcionó indicios de ocurrencia de eventos adversos. Dos estudios reportaron la eficacia de usar el diagnóstico de TEPT como una variable dependiente, pero no encontraron diferencias entre los grupos. Todos los estudios reportaron sobre eficacia usando la severidad de TEPT como variable dependiente. Para el meta-análisis, 4 estudios (n=293) fueron incluidos, brindando reducciones significativamente mayores de la severidad de TEPT que el cuidado estándar a los 2 y 12 meses de seguimiento (g=−0.23, 95% IC [−0.46, 0.00]), pero no respecto a 1 y 6 semanas post-intervención (g=−0.28, 95% IC [−0.57, 0.02]). La heterogeneidad de las intervenciones impidió mayores análisis.
Discusión: los hallazgos sugieren que las intervenciones tempranas pueden llevar a efectos duraderos sobre la severidad de TEPT tras abuso sexual. Sin embargo, debido a la disponibilidad limitada de los datos, es imposible sacar conclusiones definitivas sobre la seguridad y eficacia de las intervenciones tempranas, y su potencial para prevenir TEPT.
目的:探讨性侵害后早期干预在减少或预防创伤后应激障碍(PTSD)中的安全性和有效性。
方法:系统检索了1980-2018年间考查了针对性侵害后3个月内PTSD干预措施有效性的研究。
结果:本综述识别出考查了5种干预措施的7项研究(n = 350)具有高偏差风险。只有2项研究报告了安全性。与6项研究的作者进行的联系没有提供不良事件发生的指征。两项研究报告了使用PTSD诊断作为因变量的有效性,但未发现组间差异。所有研究都报告了使用PTSD严重程度作为因变量的有效性。对于元分析,入组了4项研究(n = 293),发现在2至12个月内的追踪调查中PTSD严重程度的降低明显强于标准护理(g = −0.23,95%CI [−0.46,0.00]),但在干预后1至6周内则无此效应(g = −0.28,95%CI [−0.57,0.02])。干预措施的异质性妨碍了进一步的分析。
讨论:研究结果表明,早期干预可以对性侵害后PTSD严重程度产生持久影响。但是,由于数据的可用性有限,不可能就早期干预措施的安全性和有效性以及它们预防PTSD的潜力得出明确的结论。
Sexual assault or rape is a highly common trauma with an estimated lifetime prevalence of up to 10% (Benjet et al., Citation2016; FRA (European Union Agency for Fundamental Rights), Citation2015; Kessler, Sonnega, Bromet, Hughes, & Nelson, Citation1995). In the aftermath of sexual assault 30–50% of rape victims develop posttraumatic stress disorder (PTSD; e.g. Elklit & Christiansen, Citation2010; Kessler et al., Citation1995; Möller, Bäckström, Söndergaard, & Helström, Citation2014; Rothbaum, Foa, Riggs, Murdock, & Walsh, Citation1992; Steenkamp, Dickstein, Salters-Pedneault, Hofmann, & Litz, Citation2012; Zinzow et al., Citation2012), with a mean duration of 9 years and 2 months (Kessler et al., Citation2017). PTSD has marked consequences on victims’ social, interpersonal, and occupational functioning (Perilloux, Duntley, & Buss, Citation2012). Given the high prevalence of sexual assault and its severe and long-lasting consequences, there is a great need for effective interventions after sexual assault.
An important issue that arises in developing and implementing such interventions is their timing. PTSD symptoms usually stabilize at 3-months post-trauma (American Psychiatric Association [APA], Citation2013). As such, late intervention can be defined as any treatment applied 3 months or more post-trauma. The effectiveness of late interventions is well documented by systematic reviews (Regehr, Alaggia, Dennis, Pitts, & Saini, Citation2013; Vickerman & Margolin, Citation2009) and these are integrated into international treatment guidelines (APA, Citation2017; International Society for Traumatic Stress Studies Guidelines Committee [ISTSS], Citation2018; National Health and Medical Research Council [NHMRC], Citation2013; National Institute for Health and Care Excellence [NICE], Citation2018; World Health Organization [WHO], Citation2013, Citation2017). Nonetheless, these interventions are not effective for all victims of sexual assault. In a systematic review of rape intervention research, Vickerman and Margolin (Citation2009) reported that in all these intervention studies at least one-third of victims remained symptomatic at post-treatment follow-up. As such, it seems important to develop early interventions, defined as interventions within 3 months after the sexual assault, aimed at preventing PTSD.
As a matter of fact, there are solid arguments in favour of early interventions. Foremost, availability of effective early interventions could reduce the significant portion of sexual assault victims that currently goes on to develop PTSD and is burdened for many years after. Prevention of PTSD could also reduce the risk of comorbid problems such as substance dependence, depression, anxiety, and suicidality (Galatzer-Levy, Nickerson, Litz, & Marmar, Citation2013). A second argument in favour of early intervention is economics. Sexual assault is a notable economic burden for society. For example, the cost of adult rape victims in the USA in 2014 was more than 3.1 trillion dollars, allocating more than 2 trillion dollars to the costs of victims’ mental health problems (Peterson, DeGue, Florence, & Lokey, Citation2017). Thus, early intervention might reduce these costs. A third argument concerns the access to victims. The early stages after sexual assault provide unique access to these victims when they contact rape crisis centres, present themselves at hospitals for forensic examinations, or receive medical care for physical injuries and/or preventative measures for sexually transmitted diseases and pregnancy (Miller, Cranston, Davis, Newman, & Resnick, Citation2015; Price, Davidson, Ruggiero, Acierno, & Resnick, Citation2014). Hence, early intervention in a multidisciplinary setting can reach the many victims who otherwise do not seek help for the psychological sequelae of sexual assault until years later (Ahrens, Campbell, Ternier-Thames, Wasco, & Sefl, Citation2007; Ullman, Citation2007; Walsh, Banyard, Moynihan, Ward, & Cohn, Citation2010).
In line with these arguments, international treatment guidelines on PTSD also recommend intervention for those with severe posttraumatic stress symptoms, as well as psychological monitoring for those with mild posttraumatic stress symptoms immediately post-trauma (APA, Citation2017; ISTSS, Citation2018; NHMRC, Citation2013; NICE, Citation2018; WHO, Citation2013, Citation2017). The most recent treatment guidelines further acknowledge that there is emerging evidence for the prevention of PTSD with single session EMDR therapy, debriefing supplemented with cohesion training exercises, brief dyadic therapy and self-guided internet-based interventions (ISTSS, Citation2018). Nevertheless, these guidelines acknowledge that the level of evidence for these recommendations is low. One meta-analysis that examined the efficacy of early intervention in victims of varied forms of trauma found that the effectiveness of early intervention is not superior to no intervention in reducing PTSD symptoms, nor in preventing the development of PTSD (Roberts, Kitchiner, Kenardy, & Bisson, Citation2009). However, these findings may not be applicable to sexual assault victims, as they comprise a subset of trauma victims who are at the highest risk of developing PTSD. In fact, the World Mental Health Surveys reported that 30% of rape victims developed PTSD compared to 4% of all trauma-exposed individuals (Kessler et al., Citation2017). Dworkin and Schumacher (Citation2016) conducted a systematic review of post-rape help-seeking behaviour and posttraumatic stress and reported that some studies suggest that early psychological intervention could reduce the risk of posttraumatic stress.
It is important to note that to date, no meta-analysis or (systematic) review has been conducted on the safety and efficacy of data specifically pertaining to early interventions after sexual trauma. The cause of this lack of research may lie in a number of arguments that have been raised against the application of early interventions. Firstly, posttraumatic stress symptoms are likely to regress naturally during the first 3 months after sexual assault. For example, up to 94% meets the criteria (aside from the criterion of symptom duration) for a PTSD diagnosis 1 week following sexual assault, while only 45–48% meets these criteria after 3 months (Elklit & Christiansen, Citation2010; Rothbaum et al., Citation1992; Steenkamp et al., Citation2012). Secondly, mental health treatments are time-intensive as well as expensive whereas mental health professionals are scarce. Therefore, some scholars regard it an unnecessary use of valuable resources to intervene at an earlier stage (McNally, Bryant, & Ehlers, Citation2003), and recommend that interventions should be postponed until PTSD has developed and can be determined. Thirdly, and probably most important, meta-analyses of controlled studies on the effectiveness of psychological debriefing immediately post-trauma have found the use of early intervention ineffective or even harmful (Rose, Bisson, Churchill, & Wessely, Citation2002; Van Emmerik, Kamphuis, Hulsbosch, & Emmelkamp, Citation2002), resulting in debate about the safety of early interventions (Litz, Gray, Bryant, & Adler, Citation2006).
Examining the impact of early interventions on PTSD is important for the development of treatment directives and clinical decision-making. To determine whether early interventions after sexual assault – other than psychological debriefing – should be implemented, we conducted a systematic literature review and meta-analyses to synthesize the existing evidence on early interventions after sexual assault and to determine their safety, efficacy in preventing PTSD. It was hypothesized that early intervention would be safe and efficacious in preventing PTSD and reducing PTSD symptom severity.
1. Methods
This systematic literature review is conducted according to the guidelines of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, Citation2011) and reported following the PRISMA Statement (Liberati et al., Citation2009).
1.1. Criteria for the selection of studies
1.1.1. Types of studies
For the current review, any type of intervention study was eligible. Both randomized and non-randomized trials were considered. Studies had to be reported in English or Dutch.
1.1.2. Types of participants
The studies should include participants that experienced a sexual trauma within 3 months prior to the intervention. Sexual trauma was defined as any type of nonconsensual sexual activity including oral, vaginal or anal penetration or any other type of sexual assault. Three months were chosen as a timeframe for an early intervention because PTSD symptoms usually begin within that timeframe (APA, Citation2013). Studies were also excluded if participants were younger than 16 years old because trauma responses including PTSD are expressed differently in children (APA, Citation2013).
1.1.3. Types of intervention
Any type of intervention aimed at treating or preventing posttraumatic stress was eligible with the exception of psychological debriefing. Psychological debriefing was excluded because it has been found detrimental to the treatment of sexual assault victims as evidenced by Rose et al. (Citation2002) in a Cochrane review on psychological debriefing for preventing PTSD.
1.1.4. Types of outcome
Finally, studies were eligible for inclusion if they measured the outcome of the intervention in terms of PTSD symptom decrease or meeting the criteria of a PTSD diagnosis. This could be either a primary or secondary outcome measure of the study and could be reported as any statistical parameter.
1.2. Search methods for identification of studies
For this literature review, systematic searches were performed of the following databases: MEDLINE, Embase, CINAHL, PsycINFO, the Social Sciences Citation Index and the Cochrane database. The full search strategies for each database can be found in Appendix A. Boolean operators were used to create search strings searching for studies about sexual trauma, intervention or prevention, and PTSD. Each search string included a concept to exclude studies targeting children or childhood sexual abuse, using the search term ‘child*’. The search strings were limited to include records published from 1 January 1980 because PTSD did not exist as a diagnosis in the Diagnostic and Statistical Manual of Mental Disorders (DSM) before 1980 (APA, Citation1968). The search was executed on 30 April 2018.
Meta-analyses and systematic reviews were only excluded at the full-text assessment stage. Additionally, the references listed in all included studies were reviewed as well as the articles listed as citing the included studies in Google Scholar.
1.3. Data collection and analysis
1.3.1. Methods for the selection of studies
The search results from the different databases were merged in Rayyan, a website for systematic reviews (Ouzzani, Hammady, Fedorowicz, & Elmagarmid, Citation2016), and duplicate records were removed. The first two review authors independently screened titles and abstracts of the remaining records to identify those that needed to be examined in full-text. This resulted in 2.9% disagreement between authors, which was resolved by discussion. Both authors also independently assessed the full-text reports on the eligibility criteria. The 4% disagreement was solved by discussion and usually stemmed from inaccuracy from either one of the authors.
1.3.2. Data extraction and management
Both authors independently extracted the relevant data from the included studies which pertained to details of the studies’ setting, eligibility criteria, procedure of randomization and blinding, participant characteristics, outcome measures, follow-up, results, analysis, drop-out rates, reasons for drop-out, (serious) adverse events, and main conclusion and topics of discussion. Minor disagreements about randomization and drop-out rates were solved by discussion.
1.3.3. Data analysis
For each study, the first two review authors independently assessed the risk of bias using the Cochrane tool of Bias. A qualitative synthesis was conducted by comparing the included studies on the extracted data. Two meta-analyses were conducted to analyse the effect of early intervention compared to standard care on PTSD symptom severity at first post-treatment assessment and longest follow-up. Because the studies utilized different instruments to measure PTSD, the standardized mean differences (i.e., Hedges’ g) were calculated. Due to clinical heterogeneity in interventions, measures and timing of measurements, random effects models were chosen. Resnick et al. (Citation2007) and Miller et al. (Citation2015) reported means and standard deviations separately for victims with and without prior rape history. However, prior rape history was not of interest for the present study. Therefore, the means and standard deviations in the intervention and control groups of all rape victims were calculated by pooling the standard deviations and means of those with and without prior rape history. Review Manager (Citation2014) was used to conduct the meta-analyses and to produce the forest plots as well as the summary graph of the risk of bias.
2. Results
2.1. Results of the search
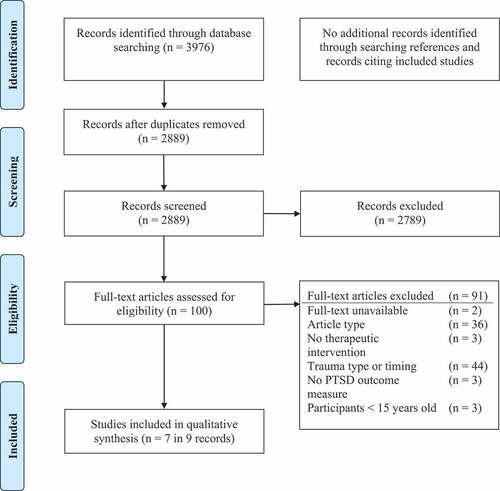
depicts a flowchart of the search process. Ultimately, seven studies reported in nine records met the eligibility criteria and were included in the qualitative synthesis presented in this review. The study reported by Resnick et al. (Citation2007) was preliminarily reported by Resnick, Acierno, Holmes, Kilpatrick, and Jager (Citation1999) and Resnick, Acierno, Kilpatrick, and Holmes (Citation2005). Because the longest follow-up of the largest population is reported in Resnick et al. (Citation2007), this record was used in the qualitative synthesis of this review.
Figure 1. Flow diagram of the study selection process. PTSD = Posttraumatic stress disorder. Adapted from ‘preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement’ (Moher, Liberati, Tetzlaff, Altman, & the PRISMA group, Citation2009).
2.2. Included studies
The seven included studies were all reported in English. shows an overview of the characteristics of these studies.
Table 1. Characteristics of included studies.
2.2.1. Setting
The studies were conducted in high-income countries, generally among individuals seeking medical, forensic or psychological care/examination.
2.2.2. Participants
The studies exclusively included sexual assault victims, except for Rothbaum et al. (Citation2012), who recruited all participants presenting at a hospital emergency department but reported results of rape victims separately. Sexual assault was generally not further defined, meaning it could include, but was not limited to, unwanted oral, anal, or vaginal penetration. The inclusion period ranged from 72 h through 3 months after the assault. The majority of the participants was female. The mean age of the participants in the various studies ranged from 22 years to 33.8 years.
2.2.3. Intervention
The seven studies investigated a multitude of different interventions (). On average, participants received three-and-a-half sessions in the active trial phase. Two studies of the same research group investigated the addition of a video intervention to a forensic examination. Immediately preceding the forensic examination, Resnick et al. (Citation2007) showed participants a video that was designed to reduce distress during the forensic examination and provide psychoeducation on coping strategies and substance abuse prevention. Using only the psychoeducational and coping strategies components of the video used in the study of Resnick et al. (Citation2007), Miller et al. (Citation2015) showed participants in their intervention group the adapted video immediately after forensic examination.
2.2.4. Control
Four of the seven studies contained a control group in which the participants received standard care. The standard care in the two video intervention studies (Miller et al., Citation2015; Resnick et al., Citation2007) consisted of the forensic rape examination accompanied by a rape crisis counsellor, who provided information about the examination and services available in the community. The standard care in the study of Nixon et al. (Citation2016) combined methods ranging from psychoeducation, supportive counselling, problem-solving, interpersonal therapy elements of mindfulness, acceptance and value-based techniques to discussion of thoughts and feelings. Notably, over the course of the study, participants in the standard care group received more sessions than those receiving cognitive processing therapy. Rothbaum et al. (Citation2012) provided few details about the standard care. However, their control group seemed to receive only medical emergency care, which might be comparable to the standard care of Resnick et al. (Citation2007) and Miller et al. (Citation2015). The two pilot EMDR studies (Tarquinio, Brennstuhl, Reichenbach, Rydberg, & Tarquinio, Citation2012a; Tarquinio, Schmitt, Tarquinio, Rydberg, & Spitz, Citation2012b) did not contain a control group and Echeburúa, de Corral, Sarasua, and Zubizarreta (Citation1996) compared two interventions.
2.2.5. Outcome measure
Two studies (Echeburúa et al., Citation1996; Nixon et al., Citation2016) reported on the categorical outcome measure of a PTSD diagnosis. PTSD symptom severity was a primary outcome measure of all studies. Miller et al. (Citation2015), Resnick et al. (Citation2007) and Rothbaum et al. (Citation2012) used the PTSD Symptom Scale (PSS) for the DSM-IV and Echeburúa et al. (Citation1996) used the PSS for the DSM-III-Revised (DSM-III-R). Two studies (Tarquinio et al., Citation2012a, Citation2012b) used the Impact of Events Scale (IES; Horowitz, Wilner, & Alvarez, Citation1979), which is a self-report measure of post-trauma intrusions and avoidance symptoms. The hyperarousal dimension of PTSD is not tested in the IES. Lastly, Nixon et al. (Citation2016) used the Clinician-Administered PTSD Scale (CAPS), which is a structured clinical interview assessing PTSD symptoms according to DSM-IV criteria.
2.3. Risk of bias of included studies
The risk of bias as assessed by the Cochrane Tool of Bias is summarized for each study in . Appendix B contains the judgement of the risk of bias of the individual studies. While all five studies comparing different treatment groups claimed to be randomized trials, true randomization only occurred in two of them (Miller et al., Citation2015; Rothbaum et al., Citation2012), meaning that the other studies risk selection bias due to quasi-randomization (Higgins & Green, Citation2011). Furthermore, although blinding participants and personnel in psychological interventions is impossible, it is possible to blind the outcome assessment. Of the five studies comparing two interventions, only Echeburúa et al. (Citation1996) failed to blind the outcome assessment by having one therapist performing both the therapy and the outcome assessment. Two studies might have been exposed to attrition bias as they reported an as-treated analysis while having significant drop-outs (50–64% in Miller et al. (Citation2015) and 38% in Resnick et al. (Citation2007)). The study of Miller et al. (Citation2015) was the only one that was selective in reporting outcome data. They carried out many analyses between different subgroups of their participants, but only reported exact data of significant differences. Other comparisons were only mentioned in passing: ‘No other statistically significant results were found’ (p.133).
Figure 2. Risk of bias summary of included studies. The minus sign represents a high risk of bias, the plus sign a low risk of bias, and the question mark an unclear risk of bias. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
![Figure 2. Risk of bias summary of included studies. The minus sign represents a high risk of bias, the plus sign a low risk of bias, and the question mark an unclear risk of bias. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.](/cms/asset/8f0a16b7-4413-48d0-bf38-7037f2b9a042/zept_a_1682932_f0002_oc.jpg)
2.4. Reporting of safety and harms
None of the studies reported a strategy for collecting or analysing harms-related information. Accordingly, five studies did not report any data on (serious) adverse events (i.e. fatal or life-threatening events, events that require hospitalization or cause invalidity or disability). Rothbaum et al. (Citation2012) and Nixon et al. (Citation2016) appeared to have adopted a passive strategy of the surveillance of harms, as their results sections stated that there were no (serious) adverse events reported. In addition, most studies did not report drop-outs or the reasons for attrition. Nixon et al. (Citation2016) reported that one participant stopped treatment due to life-threatening illness. Additionally, they reported that two participants who received the intervention showed an increase in clinician-reported PTSD symptom severity at some point during the trial, with one participant reporting higher PTSD symptom severity at the 12-month follow-up than at pretreatment. Due to this lack of safety data, we contacted the authors of the studies for further information and received additional information from Echeburúa et al. (Citation1996), Tarquinio et al. (Citation2012a), Tarquinio et al. (Citation2012b), and Resnick et al. (Citation2007). Echeburúa et al. (Citation1996), Tarquinio et al. (Citation2012a), and Tarquinio et al. (Citation2012b) stated not to have applied a predetermined strategy for the surveillance of harms. Resnick et al. (Citation2007) systematically asked victims about their opinion of the helpfulness of the procedures and no participants had found the trial problematic. Furthermore, Echeburúa et al. (Citation1996), Tarquinio et al. (Citation2012a), Tarquinio et al. (Citation2012b), and Resnick et al. (Citation2007) reported that no (serious) adverse events had occurred.
2.5. Prevention of PTSD diagnosis
As previously mentioned, two studies reported the efficacy of the interventions on the development of PTSD after sexual assault based upon the presence of a PTSD diagnosis (Echeburúa et al., Citation1996; Nixon et al., Citation2016). When focusing on the difference between groups, Echeburúa et al. (Citation1996) found no difference at any time point in PTSD diagnoses between the group that received cognitive restructuring training and the group that received progressive muscular relaxation training. Similarly, Nixon et al. (Citation2016) found no difference between cognitive processing therapy and standard care in PTSD diagnoses at posttreatment and follow-up.
2.6. Reduction of PTSD symptom severity
The results of the within-group and between-group analyses of all studies on PTSD symptom severity are summarized in .
Table 2. Effects of interventions of included studies.
2.6.1. Within-group analyses of intervention
All four studies (Echeburúa et al., Citation1996; Nixon et al., Citation2016; Tarquinio et al., Citation2012a, Citation2012b) that conducted a within-group analysis reported a significant decrease in PTSD symptom severity across the treatment up until the latest follow-up, the longest of which was 12 months. However, without comparing these results to a control group, this decrease in symptoms cannot be differentiated from natural recovery. The remaining three studies did not report a within-group analysis. For Miller et al. (Citation2015) a within-group hedge’s g was calculated using the reported means and standard deviations of the PSS total symptom scores. This revealed a significant increase in PTSD symptom severity from pretreatment to posttreatment (g = 0.90, 95% CI = 0.38, 1.41) that was no longer significant from pretreatment to the 2-month follow-up (g = 0.47, 95% CI = −0.03, 0.97). Rothbaum et al. (Citation2012) and Resnick et al. (Citation2007) did not collect baseline data, therefore calculating within-group analyses was not possible.
2.6.2. Between-group analyses comparing intervention to standard care
Four studies (Miller et al., Citation2015; Nixon et al., Citation2016; Resnick et al., Citation2007; Rothbaum et al., Citation2012) provided a between-group analysis comparing an intervention to standard care. A meta-analysis of the aggregated data of these four studies did not show a significant effect of early intervention on PTSD symptom severity at the first post-intervention follow-up, as shown in . However, at the latest follow-up, early intervention corresponded to significantly lower PTSD severity scores,Footnote1 see . No evidence was found for an effect at the first follow-up, ranging from one to 6-weeks post-intervention (random effects) (k = 4, n = 292, g = −0.28, 95% CI = −0.57, 0.02). However, a trend in favour of early intervention can be found in all four studies. There was a moderate level of statistical heterogeneity (I2 = 33%). At the last follow-up, ranging from two to 12-months post-intervention, a modest effect of the early intervention on PTSD symptom severity just reached significance (random effects) (k = 4, n = 293, g = −0.23, 95% CI = −0.46, 0.00). There was no statistical heterogeneity (I2 = 0%).
Figure 3. Forest plot of comparison: intervention versus standard care. Outcome: severity of PTSD symptoms at first follow-up. The first follow-up post-intervention was: for Resnick et al. (Citation2007) six weeks, for Rothbaum et al. (Citation2012) 4 weeks, for Miller et al. (Citation2015) 2 weeks and for Nixon et al. (Citation2016) 1 week. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
![Figure 3. Forest plot of comparison: intervention versus standard care. Outcome: severity of PTSD symptoms at first follow-up. The first follow-up post-intervention was: for Resnick et al. (Citation2007) six weeks, for Rothbaum et al. (Citation2012) 4 weeks, for Miller et al. (Citation2015) 2 weeks and for Nixon et al. (Citation2016) 1 week. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.](/cms/asset/ebfade93-56b4-4e53-b17f-5d3c26072f49/zept_a_1682932_f0003_oc.jpg)
Figure 4. Forest plot of comparison: intervention versus standard care. Outcome: severity of PTSD symptoms at latest follow-up. The latest follow-up was: for Resnick et al. (Citation2007) 6-months post-intervention, for Rothbaum et al. (Citation2012) 12 weeks, for Miller et al. (Citation2015) 2 months and for Nixon et al. (Citation2016) 1 year. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
![Figure 4. Forest plot of comparison: intervention versus standard care. Outcome: severity of PTSD symptoms at latest follow-up. The latest follow-up was: for Resnick et al. (Citation2007) 6-months post-intervention, for Rothbaum et al. (Citation2012) 12 weeks, for Miller et al. (Citation2015) 2 months and for Nixon et al. (Citation2016) 1 year. Produced using Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.](/cms/asset/629be318-1850-4040-b986-8609792e4e36/zept_a_1682932_f0004_oc.jpg)
3. Discussion
The goal of this study was to review the safety and efficacy of early interventions in reducing or preventing PTSD after sexual assault. The systematic review identified seven studies that met the eligibility criteria. The included studies investigated a range of different interventions, including EMDR, prolonged exposure, cognitive restructuring, cognitive processing, and a mainly psycho-educational video intervention. Due to this heterogeneity and the small number of studies, the types of interventions could not be examined separately nor compared. The studies were also diverse in research design and timing. The methodological quality of the included studies was mostly low, resulting in a high risk of selection bias.
The results firstly show that there is limited documentation on the safety of early intervention after sexual assault. Most studies did not mention safety at all. The passive surveillance of two studies reported no (serious) adverse events. Nixon et al. (Citation2016) found a significant worsening of PTSD symptoms who received the intervention (i.e., cognitive processing therapy) as indexed by the clinical interview. However, these participants did not self-report a worsening in symptoms. In addition, an increase in PTSD symptom severity was also found in two participants in the control condition which suggests that the most likely explanation for the purported symptom increase is a natural course of symptoms. No serious adverse events were found in any of the trials (excluding Miller et al. (Citation2015) due to lack of information). Thus, we have found no evidence to suggest early interventions after sexual assault are unsafe. However, given the debate about potential harm that can be induced by the application of early interventions for PTSD (e.g. Litz et al., Citation2006), it is quite noteworthy that none of the studies implemented an active strategy to identify potential harm or the occurrence of adverse events during the trial, even though such an active strategy is likely to uncover adverse events (Stephens, Talbot, & Routledge, Citation1998). In light of the negative effects of psychological debriefing (Rose et al., Citation2002), a focus on safety should be prioritized in early intervention research.
In terms of the prevention of PTSD, early interventions resulted in no fewer PTSD diagnoses than control settings. However, only two studies reported on the differences in post-intervention PTSD diagnosis between groups. The small samples and the heterogeneity of the studies preclude generalization of these findings. With regard to the efficacy of early interventions to reduce PSTD symptom severity, a significant decrease in symptom severity across post-intervention and follow-up was detected in the intervention group of all studies that reported baseline data. Meta-analyses using the data of four studies found no difference at one to 6-weeks post-intervention but revealed that early intervention generated a significantly greater reduction in PTSD symptom severity than standard care at 2–12-months follow-up. In other words, the meta-analyses were unable to find evidence for the efficacy of early intervention on a short term, but did find a trend in favour of early intervention. Additionally, the meta-analysis found evidence for long-term efficacy of the early intervention in reducing the severity of PTSD symptoms.
Although this narrow-scoped review of early intervention after sexual assault has not been conducted previously, similar reviews on the broader scope of early post-trauma intervention should be considered. For example, in their review on help-seeking behaviour in sexual assault victims, Dworkin and Schumacher (Citation2016) concluded that early psychological treatment may reduce the risk of posttraumatic stress for the first few months. These findings are in line with the results of the current review. In contrast, a Cochrane review by Roberts et al. (Citation2009) found cognitive behavioural therapy and cognitive restructuring to be the most efficacious in preventing PTSD in trauma patients. Our results do not seem to support this finding in a sample of sexual assault victims, because the two included articles that studied interventions with a cognitive element showed mixed results: More specifically, Echeburúa et al. (Citation1996) reported cognitive restructuring to be more effective than relaxation training at 12 months, whereas Nixon et al. (Citation2016) measured no increased efficacy of cognitive reprocessing over standard care. It should be noted that these studies used different control groups, and the findings of two studies are insufficient to reject the finding of Roberts et al. (Citation2009). Still, the inconsistency in findings underlines the importance of examining interventions after sexual assault in homogenous samples.
The studies that were included in this systematic review show noteworthy limitations. Foremost, only seven studies were included in this review, making it difficult to draw reliable conclusions. Additionally, these studies presented methodological and statistical heterogeneity. Particularly, they included a range of interventions, making generalizations on intervention-type unreliable, and had a high risk of bias, which increases the likelihood of a Type I error (Moher et al., Citation1998). It should also be noted that the included studies presented PTSD symptoms as described by the DSM-III-R or DSM-IV. However, because the current DSM-5 defines PTSD differently by adding the domain of negative cognitions, no generalizations to this definition of PTSD can be made.
In light of these limitations, several implications for future research can be drawn. Foremost, as stated before, the safety of early interventions should be taken into consideration in future trials: Future research should report any adverse events, drop-outs or negative effects within the trial sample and should adopt active strategies to detect them. In addition, to determine the efficacy of early intervention in preventing PTSD diagnosis, future efficacy trials should report the prevalence of PTSD diagnosis as well as PTSD symptoms. Furthermore, future research needs to resolve differences in the wide variety of study designs in order to determine the most efficacious type, timing and length of intervention. In doing so, a focus on high quality of design is crucial to reduce the risk of bias. Lastly, future research should compare the effect of early interventions to the effect of standard treatment at a later point in time. Considering the previously stated arguments in favour of early intervention, this type of research should extend beyond the effect on PTSD, and include comorbid psychopathology, cost-effectiveness, and the accessibility for victims of sexual assault.
In conclusion, the findings of this review and meta-analyses suggest that early interventions can lead to durable effects on PTSD symptom severity reduction after sexual assault. Therefore, the present study provides support for the development of early interventions. However, due to a limited availability of data, it is not yet possible to draw any definite conclusions about the safety of early interventions after sexual assault, their efficacy and their potential as a preventive treatment for PTSD. Nevertheless, the present review and meta-analysis show that, although psychological debriefing has been found to be ineffective, other interventions can be effective as early intervention after sexual assault. Therefore, we urge researchers not to shy away from this field but instead invest in the exploration and further development of effective interventions to prevent PTSD in victims of sexual assault.
Disclosure statement
All authors are involved in the Early EMDR Study (Early Intervention with Eye Movement Desensitization and Reprocessing to reduce PTSD symptom severity: A randomized controlled trial in recent rape victims). The trial is registered in the Dutch trial register (www.trialregister.nl) under NTR6760. All authors declare no further conflict of interests.
Additional information
Funding
Notes
1. The Hedges’ g and confidence interval that we calculated for Rothbaum et al. (Citation2012) differs from their reported values. From personal communications with the authors, these differences are allocated to their use of covariates in their analysis.
References
- Ahrens, C. E., Campbell, R., Ternier-Thames, N. K., Wasco, S. M., & Sefl, T. (2007). Deciding whom to tell: Expectations and outcomes of rape survivors’ first disclosures. Psychology of Women Quarterly, 31(1), 38–15.
- American Psychiatric Association. (1968). Diagnostic and statistical manual of mental disorders (2nd ed., text rev.). Washington, DC: Author.
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author.
- American Psychiatric Association. (2017). Clinical practice guideline for the treatment of posttraumatic stress disorder in adults. Retrieved from http://www.apa.org/ptsd guideline/
- Benjet, C., Bromet, E., Karam, E. G., Kessler, R. C., McLaughlin, K. A., Ruscio, A. M., … Alonso, J. (2016). The epidemiology of traumatic event exposure worldwide: Results from the world mental health survey consortium. Psychological Medicine, 46(2), 327–343.
- Dworkin, E. R., & Schumacher, J. A. (2016). Preventing posttraumatic stress related to sexual assault through early intervention: A systematic review. Trauma, Violence, & Abuse, 19(4), 459–472.
- Echeburúa, E., de Corral, P., Sarasua, B., & Zubizarreta, I. (1996). Treatment of acute posttraumatic stress disorder in rape victims: An experimental study. Journal of Anxiety Disorders, 10(3), 185–199.
- Elklit, A., & Christiansen, D. M. (2010). ASD and PTSD in rape victims. Journal of Interpersonal Violence, 25(8), 1470–1488.
- FRA (European Union Agency for Fundamental Rights). (2015). Violence against women: An EU-wide survey. Luxembourg: Publications Office of the European Union.
- Galatzer-Levy, I. R., Nickerson, A., Litz, B. T., & Marmar, C. R. (2013). Patterns of lifetime PTSD comorbidity: A latent class analysis. Depression and Anxiety, 30, 489–496.
- Higgins, J., & Green, S. (Eds.) (2011). Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. The Cochrane Collaboration. Retrieved from www.handbook.cochrane.org
- Horowitz, M., Wilner, N., & Alvarez, W. (1979). Impact of event scale: A measure of subjective stress. Psychosomatic Medicine, 41(3), 209–218.
- International Society for Traumatic Stress Studies Guidelines Committee (2018). Posttraumatic stress disorder prevention and treatment guidelines methodology and recommendations. Oakbrook Terrace, IL: Author. Retrieved from http://www.istss.org/treating-trauma/new-istss-prevention-and-treatment-guidelines.aspx.
- Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., … Florescu, S. (2017). Trauma and PTSD in the WHO world mental health surveys. European Journal of Psychotraumatology, 8(sup5), 1353383.
- Kessler, R. C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the national comorbidity survey. Archives of General Psychiatry, 52(12), 1048–1060.
- Liberati, A., Altman, D. G., Tetzlaff, J., Mulrow, C., Gøtzsche, P. C., Ioannidis, J. P., … Moher, D. (2009). The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Medicine, 6(7), e1000100.
- Litz, B. T., Gray, M. J., Bryant, R. A., & Adler, A. B. (2006). Early intervention for trauma: Current status and future directions. Clinical Psychology Science and Practice, 9(2), 112–134.
- McNally, R. J., Bryant, R. A., & Ehlers, A. (2003). Does early psychological intervention promote recovery from posttraumatic stress? Psychological Science in the Public Interest, 4(2), 45–79.
- Miller, K. E., Cranston, C. C., Davis, J. L., Newman, E., & Resnick, H. (2015). Psychological outcomes after a sexual assault video intervention: A randomized trial. Journal of Forensic Nursing, 11(3), 129–136.
- Moher, D., Pham, B., Jones, A., Cook, D. J., Jadad, A. R., Moher, M., … Klassen, T. P. (1998). Does quality of reports of randomized trials affect estimates of intervention efficacy reported in meta-analyses? Lancet, 352, 609–613.
- Moher, S., Liberati, A., Tetzlaff, J., & Altmann, D. G.; The PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Medicine, 6(7), e1000097.
- Möller, A. T., Bäckström, T., Söndergaard, H. P., & Helström, L. (2014). Identifying risk factors for PTSD in women seeking medical help after rape. PLoS One, 9(10), e111136.
- National Health and Medical Research Council. (2013). Australian guidelines for the treatment of acute stress disorder and posttraumatic stress disorder. Retrieved from https://www.clinicalguidelines.gov.au/node/3268
- National Institute for Health and Care Excellence. (2018). Post-traumatic stress disorder: Evidence reviews on care pathways for adults, children and young people with PTSD (NICE Guideline Standard No. NG116). Retrieved from https://www.nice.org.uk/guidance/ng116.
- Nixon, R. D., Best, T., Wilksch, S. R., Angelakis, S., Beatty, L. J., & Weber, N. (2016). Cognitive processing therapy for the treatment of acute stress disorder following sexual assault: A randomised effectiveness study. Behaviour Change, 33(4), 232–250.
- Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan – A web and mobile app for systematic reviews. Systematic Reviews, 5(1), 210.
- Perilloux, C., Duntley, J. D., & Buss, D. M. (2012). The costs of rape. Archives of Sexual Behavior, 41(5), 1099–1106.
- Peterson, C., DeGue, S., Florence, C., & Lokey, C. N. (2017). Lifetime economic burden of rape among U.S. adults. American Journal of Preventive Medicine, 52, 691–701.
- Price, M., Davidson, T. M., Ruggiero, K. J., Acierno, R., & Resnick, H. S. (2014). Predictors of using mental health services after sexual assault. Journal of Traumatic Stress, 27(3), 331–337.
- Regehr, C., Alaggia, R., Dennis, J., Pitts, A., & Saini, M. (2013). Interventions to reduce distress in adult victims of rape and sexual violence: A systematic review. Research on Social Work Practice, 23(3), 257–265.
- Resnick, H., Acierno, R., Holmes, M., Kilpatrick, D. G., & Jager, N. (1999). Prevention of post-rape psychopathology: Preliminary findings of a controlled acute rape treatment study. Journal of Anxiety Disorders, 13(4), 359–370.
- Resnick, H., Acierno, R., Kilpatrick, D. G., & Holmes, M. (2005). Description of an early intervention to prevent substance abuse and psychopathology in recent rape victims. Behavior Modification, 29(1), 156–188.
- Resnick, H., Acierno, R., Waldrop, A. E., King, L., King, D., Danielson, C., … Kilpatrick, D. (2007). Randomized controlled evaluation of an early intervention to prevent post rape psychopathology. Behaviour Research and Therapy, 45(10), 2432–2447.
- Review Manager(RevMan)[Computer program]. (2014). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration.
- Roberts, N. P., Kitchiner, N. J., Kenardy, J., & Bisson, J. I. (2009). Systematic review and meta-analysis of multiple-session early interventions following traumatic events. American Journal of Psychiatry, 166(3), 293–301.
- Rose, S., Bisson, J., Churchill, R., & Wessely, S. (2002). Psychological debriefing for preventing post traumatic stress disorder (PTSD). Cochrane Database Syst Rev, 2(2), 1465–1858.
- Rothbaum, B. O., Foa, E. B., Riggs, D. S., Murdock, T., & Walsh, W. (1992). A prospective examination of posttraumatic stress disorder in rape victims. Journal of Traumatic Stress, 5(3), 455–475.
- Rothbaum, B. O., Kearns, M. C., Price, M., Malcoun, E., Davis, M., Ressler, K. J., … Houry, D. (2012). Early intervention may prevent the development of posttraumatic stress disorder: A randomized pilot civilian study with modified prolonged exposure. Biological Psychiatry, 72(11), 957–963.
- Shapiro, F. (2001). Eye movement desensitization and reprocessing (EMDR): Basic principles, protocols, and procedures. New York: Guilford Press.
- Steenkamp, M. M., Dickstein, B. D., Salters‐Pedneault, K., Hofmann, S. G., & Litz, B. T. (2012). Trajectories of PTSD symptoms following sexual assault: Is resilience the modal outcome? Journal of Traumatic Stress, 25(4), 469–474.
- Stephens, M. D., Talbot, J. C., & Routledge, P. A. (1998). The detection of new adverse reactions (4th ed.). London: Macmillan Reference.
- Tarquinio, C., Brennstuhl, M. J., Reichenbach, S., Rydberg, J. A., & Tarquinio, P. (2012a). Early treatment of rape victims: Presentation of an emergency EMDR protocol. Sexologies, 21(3), 113–121.
- Tarquinio, C., Schmitt, A., Tarquinio, P., Rydberg, J. A., & Spitz, E. (2012b). Benefits of “eye movement desensitization and reprocessing” psychotherapy in the treatment of female victims of intimate partner rape. Sexologies, 21(2), 60–67.
- Ullman, S. E. (2007). Mental health services seeking in sexual assault victims. Women & Therapy, 30(1–2), 61–84.
- Van Emmerik, A. A., Kamphuis, J. H., Hulsbosch, A. M., & Emmelkamp, P. M. (2002). Single session debriefing after psychological trauma: A meta-analysis. The Lancet, 360, 766–771.
- Vickerman, K. A., & Margolin, G. (2009). Rape treatment outcome research: Empirical findings and state of the literature. Clinical Psychology Review, 29(5), 431–448.
- Walsh, W. A., Banyard, V. L., Moynihan, M. M., Ward, S., & Cohn, E. S. (2010). Disclosure and service use on a college campus after an unwanted sexual experience. Journal of Trauma & Dissociation, 11(2), 134–151.
- World Health Organization. (2013). Guidelines for the management of conditions specifically related to stress. Retrieved from http://www.who.int/mental_health/emergencies/stress_guidelines/en/
- World Health Organization. (2017). Responding to children and adolescents who have been sexually abused. WHO clinical guidelines. Geneva: World Health Organization. Retrieved from http://www.who.int/reproductivehealth/publications/violence/clinical-response-csa/en/.
- Zinzow, H. M., Resnick, H. S., McCauley, J. L., Amstadter, A. B., Ruggiero, K. J., & Kilpatrick, D. G. (2012). Prevalence and risk of psychiatric disorders as a function of variant rape histories: Results from a national survey of women. Social Psychiatry and Psychiatric Epidemiology, 47(6), 893–902.
Appendix A.
Search strings
MEDLINE (via Pubmed)
Using the PubMed advanced search builder:
#1 = (((((((((((((((sex offences[MeSH Terms]) OR rape*[Title/Abstract]) OR sexu* traum*[Title/Abstract]) OR sex traum*[Title/Abstract]) OR sexu* abus*[Title/Abstract]) OR sex abus*[Title/Abstract]) OR sexu* assault*[Title/Abstract]) OR sex assault*[Title/Abstract]) OR sexu* viol*[Title/Abstract]) OR sex viol*[Title/Abstract])
#2 = 6,151,349 = (((((((((((psychotherapies[MeSH Terms]) OR psychotherap*[Title/Abstract]) OR emdr[Title/Abstract]) OR eye movement desensiti*[Title/Abstract]) OR emdr[MeSH Terms]) OR prevention[Title/Abstract]) OR intervention[Title/Abstract]) OR therap*[Title/Abstract]) OR psychoeducation[Title/Abstract]) OR education[Title/Abstract]) OR treatment[Title/Abstract])
#3 = ((((ptsd[MeSH Terms]) OR ptsd[Title/Abstract]) OR posttraumatic [Title/Abstract]) OR post traumatic [Title/Abstract])
#4 = #1 AND #2 AND #3 NOT child*[Title/Abstract]
Filter: publication date from 1980/01/01 to 2018/05/01 = 179 items
Results = 179 items
Embase
Using the advanced search:
#1 = (‘rape*’:ab,ti OR ‘sexu* assault*’:ab,ti OR ‘sex assault*’:ab,ti OR ‘sexu* abus*’:ab,ti OR ‘sex abus*’:ab,ti OR ‘sexu* traum*’:ab,ti OR ‘sex traum*’:ab,ti OR ‘sexu* viol*’:ab,ti OR ‘sex viol*’:ab,ti OR ‘sexual assault’/exp) AND [embase]/lim
#2 = (‘emdr’:ab,ti OR ‘eye movement desensiti*’:ab,ti OR ‘eye movement desensitization and reprocessing’/exp OR ‘psychotherap*’:ab,ti OR ‘prevention’:ab,ti OR ‘intervention’:ab,ti OR ‘therap*’:ab,ti OR ‘psychoeducation’:ab,ti OR ‘education’:ab,ti OR ‘treatment’:ab,ti) AND [embase]/lim
#3 = (‘ptsd’:ab,ti OR ‘posttraumatic stress’:ab,ti OR ‘post traumatic stress’:ab,ti OR ‘posttraumatic stress disorder’/exp) AND [embase]/lim
#4 = #1 AND #2 AND #3 NOT ‘child*’:ab,ti
From 1980
Results = 819 items
CINAHL (via EBSCOhost)
Using the advanced search wizard:
#1 = rape* or sexu* assault* or sex assault* or sexu* abus* or sex abus* or sexu* traum* or sex traum* or sexu* viol* or sex viol*
#2 = emdr or eye movement desensiti* or psychotherap* or prevention or intervention or therap* or psychoeducation or education or treatment
#3 = ptsd or posttraumatic stress or post traumatic stress
#4 = #1 AND #2 AND #3 NOT child*
From 1991–2018
Results = 284 items
PsycINFO (via OVID)
Using the advanced search:
#1 = (rape* or sexu* traum* or sex traum* or sexu* abus* or sex abus* or sexu* assault* or sex assault* or sexu* viol* or sex viol*).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures]
#2 = (psychotherap* or eye movement desensiti* or emdr or prevention or intervention or therap* or psychoeducation or education or treatment).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures], limit to yr = ‘1980-current’
#3 = (ptsd or posttraumatic or post traumatic).mp. [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures], limit to yr = ‘1980-current’
#4 = child*.mp [mp = title, abstract, heading word, table of contents, key concepts, original title, tests & measures]
#5 = #1 AND #2 AND #3 NOT #4
Limit to yr = ‘1980-current’
Results = 941 items
Social Sciences Citation Index (via Web of Science)
Using the advanced search:
#1: TS = (rape* OR sexu* traum* OR sex traum* OR sexu* abus* OR sex abus* OR sexu* assault* OR sex assault* OR sexu* viol* OR sex viol*)
#2: TS = (psychotherap* OR emdr OR eye movement desensiti* OR prevention OR intervention OR therap* OR psychoeducation OR education OR treatment)
#3: TS = (ptsd OR posttraumatic OR post traumatic)
#4: TS = child*
#5 = #1 AND #2 AND #3 AND #4 NOT #5
Timespan 1980–2018, Social Sciences Citation index only
Results = 1671 items
Cochrane Database
Using the advanced search:
#1 = ‘rape*’:ti,ab,kw or ‘sexu* assault*’:ti,ab,kw or ‘sex assault*’:ti,ab,kw or ‘sexu* abus*’:ti,ab,kw or ‘sex abus*’:ti,ab,kw or ‘sexu* traum*’:ti,ab,kw or ‘sex traum*’:ti,ab,kw or ‘sexu* viol*’:ti,ab,kw or ‘sex viol*’:ti,ab,kw
#2 = ‘EMDR’:ti,ab,kw OR ‘eye movement desensiti*’:ti,ab,kw OR ‘psychotherap*’:ti,ab,kw OR ‘prevention’:ti,ab,kw OR ‘intervention’:ab,ti,kw OR ‘therap*’:ab,ti,kw OR ‘psychoeducation’:ab,ti,kw OR ‘education’:ab,ti,kw OR ‘treatment’:ab,ti,kw
#3 = ‘PTSD’:ti,ab,kw OR ‘posttraumatic stress’:ti,ab,kw OR ‘post traumatic stress’:ti,ab,kw
#4 = #1 AND #2 AND #3 NOT ‘child*’:ti,ab,kw
Filter: 1980–2018
Results = 82 items
Appendix B.
Risk of Bias of Individual Studies
Table B1. Risk of bias of Echeburúa et al. (Citation1996).
Table B2. Risk of bias of Resnick et al. (Citation2007).
Table B3. Risk of bias of Rothbaum et al. (Citation2012).
Table B4. Risk of bias of Tarquinio et al. (Citation2012a).
Table B5. Risk of bias of Tarquinio et al. (Citation2012b).
Table B6. Risk of bias of Miller et al. (Citation2015).
Table B7. Risk of bias of Nixon et al. (Citation2016).