
ABSTRACT
Background
Individuals with posttraumatic stress disorder (PTSD) often report intrusive memories that appear to lack the appropriate spatio-temporal context.
Objective
We examined whether focusing on the spatio-temporal context of aversive autobiographical memories reduces negative emotions, appraisals, and re-experiencing symptoms.
Methods
We recruited 109 healthy adults and had them rate emotionality, vividness, and re-experiencing of an aversive autobiographical memory. Furthermore, we assessed automatic associations of idiosyncratic memory triggers with the concepts ‘past’ vs. ‘now’, and self-reported sense of memory closure and distancing. To manipulate spatio-temporal memory (re-)organization, the experimental group (n = 53) performed a lifeline exercise in virtual reality (VR), where participants symbolically placed memory triggers along a path representing their own personal life story. The control group (n = 56) completed a non-personalized VR task.
Results
We found a marked decrease in negative emotions, negative appraisals, and re-experiencing in the following week, but on average, the lifeline exercise was not superior to the control condition. However, those in the lifeline group with stronger trigger-past associations subsequently exhibited a more pronounced reduction in re-experiencing. Also, participants with a higher subjective sense of memory distancing reported less re-experiencing.
Conclusions
The findings lend tentative support for theoretical assumptions about PTSD, but the potential causal role of automatic associations with spatio-temporal information remains to be clarified.
HIGHLIGHTS
We tested a VR lifeline exercise to alter spatio-temporal associations and intrusions of aversive autobiographical memories.
This was not superior to a non-personalized control group, but temporal associations and memory distancing predicted reduced re-experiencing.
Antecedentes: Las personas con trastorno de estrés postraumático (TEPT) con frecuencia informan recuerdos intrusivos que parecen carecer del contexto espacio-temporal adecuado.
Objetivo: Examinamos si centrarse en el contexto espacio-temporal de los recuerdos autobiográficos aversivos reduce las emociones negativas, las valoraciones, y los síntomas de re-experimentación.
Métodos: Reclutamos 109 adultos sanos y les pedimos que calificaran la emocionalidad, vivacidad y re-experimentación de un recuerdo autobiográfico aversivo. Además, evaluamos las asociaciones automáticas de los desencadenantes de la memoria idiosincrática con los conceptos de ‘pasado’ vs ‘ahora’ y la sensación auto-reportada de la cercanía o lejanía del recuerdo. Para manipular la (re-)organización de la memoria espacio-temporal, el grupo experimental (n = 53) realizo un ejercicio de Línea de Vida en realidad virtual (RV), donde los participantes simbólicamente pusieron los gatilladores del recuerdo a lo largo de un sendero que representaba sus propias historias de vida personales. El grupo control (n = 56) completo una tarea de RV no personalizada.
Resultados: Encontramos una disminución marcada de las emociones negativas, valoraciones negativas y re-experimentación en la semana siguiente, pero en promedio, el ejercicio de la Línea de Vida no fue superior a la condición de control. Sin embargo, aquellos del grupo de la Línea de Vida con asociaciones más fuertes de los gatilladores del pasado exhibieron subsecuentemente una disminución más pronunciada en la re-experimentación. Tambien, los participantes con un sentido de la memoria de distanciamiento subjetivamente más alta informaron menor re-experimentación.
Conclusiones: Los hallazgos brindan un apoyo tentativo a las suposiciones teóricas acerca del TEPT, pero el posible papel causal de las asociaciones automáticas con la información espacio-temporal aún no se ha aclarado.
背景: 患有创伤后应激障碍 (PTSD) 的个体经常报告似乎缺乏适当时空背景的闯入性记忆。
目的: 我们考查了关注厌恶自传记忆的时空背景是否会减少负性情绪, 评价和再体验症状。
方法: 我们招募了 109 名健康成年人, 让他们对厌恶自传记忆的情绪性, 生动性和再体验进行评分。此外, 我们评估了特殊记忆触发与‘过去’与‘现在’概念的自动关联, 以及自我报告的记忆闭合和疏离。为了操纵时空记忆 (再) 组织, 实验组 (n = 53) 在虚拟现实 (VR) 中进行了生命线练习, 参与者象征性地将记忆触发器放置在代表他们自己个人生活故事的路径上。对照组 (n = 56) 完成了非个性化的 VR 任务。
结果: 我们发现在接下来的一周内, 负性情绪, 负性评价和再体验明显减少, 但平均而言, 生命线练习并不优于对照条件。然而, 生命线组中具有更强触发-过去关联的人随后表现出更明显的再体验减少。此外, 具有更高主观记忆距离疏离感的参与者报告的再体验更少。
结论:研究结果为关于 PTSD 的理论假设提供了初步支持, 但与时空信息自动关联的潜在因果作用仍有待澄清。
Trauma survivors often develop distressing intrusive memories that persist long after the event is over. In individuals with post-traumatic stress disorder (PTSD), trauma memories are rich in perceptual details and entail a strong sense of reliving (Birrer, Michael, & Munsch, Citation2007; Crespo & Fernández-Lansac, Citation2016; Michael, Ehlers, Halligan, & Clark, Citation2005), making them feel as if the traumatic experience were happening again in the present moment. However, it remains poorly understood what pathways lead to the immersive and intrusive phenomenology of traumatic memory in PTSD, and how it can be ameliorated or prevented. Clinical and information processing accounts of PTSD characterize intrusive memories as overly accessible, insufficiently processed, and strongly associated with negative appraisals (Brewin, Gregory, Lipton, & Burgess, Citation2010; Ehlers & Clark, Citation2000; Foa, Huppert, & Cahill, Citation2006: for an alternative account, see, e.g. Rubin, Berntsen, & Bohni, Citation2008). Accordingly, PTSD patients excessively encode aversive perceptual elements along with fear-related responses and interpretation patterns (Foa et al., Citation2006), while failing to encode contextualized representations that are integrated with other autobiographical memories (Bisby, Burgess, & Brewin, Citation2020). Consequently, perceptual cues can easily trigger the recall of trauma elements and co-activate threat-related appraisals and behavioural response schemata. Critically, at the time of remembering, poor contextual memory integration may inhibit the realization that the event happened in the past and elsewhere, leading to trauma re-experiencing and an activation of affective and behavioural responses.
In line with these assumptions, research indicates that aversive memories lack associative binding among their episodic elements (Bisby et al., Citation2020), and virtually all empirically supported trauma-focused therapies converge in their goal to reorganize memory and to create coherent trauma narratives (Schnyder et al., Citation2015). Additionally, studies in clinical and healthy populations suggest that a poorer ability to memorize contextual, spatial, and/or temporal sequence information makes people more vulnerable to develop PTSD symptoms (e.g. Meyer, Krans, van Ast, & Smeets, Citation2017; Meyer et al., Citation2013; Sierk et al., Citation2019; Smith, Burgess, Brewin, & King, Citation2015). Furthermore, automatic attentional biases that prioritize trauma-related information have been linked to the development and maintenance of PTSD symptoms (for review, see Woud, Verwoerd, & Krans, Citation2017). Accordingly, PTSD may be critically linked to an automatic reactivity to trauma-related stimuli along with impaired access to contextual information about the traumatic events.
Further support comes from a recent experimental study that assessed automatic associations between memory cues and spatio-temporal context information in healthy volunteers who had seen traumatic film fragments (Meyer, Ikani, & Morina, Citation2019). Here, a computerized training programme was used to link reminder cues pertaining to one traumatic film with the verbal response ‘now’, while reminder cues of another film were paired with the verbal response ‘past’. This manipulation altered implicit associations between the film cues and the categories ‘now’ and ‘past’ on a subsequent implicit association test (IAT; Greenwald, McGhee, & Schwartz, Citation1998). Yet, there were no direct effects on the development of intrusive memories or other outcomes at one-week follow-up. Also, interpretation of the results was complicated by the fact that one of the films was more easily associated with the ‘now’ response than the other. However, when these differences were statistically accounted for, participants who preferentially associated one set of film cues with the concept ‘now’ developed higher levels of intrusions about the respective film fragments, as compared with the film fragments that they preferentially associated with the concept ‘past’. Thus, spatio-temporal associations may be associated with intrusive memories, although a potentially causal link remains to be established.
To further investigate this, we devised an intervention fostering spatio-temporal integration of idiosyncratic aversive memories in a non-clinical sample, based on a Lifeline exercise (e.g. Adler & Rungta, Citation2002), and using real-time 3D Virtual Reality (VR). The exercise applied principles of narrative exposure therapy for PTSD (NET; Elbert, Schauer, & Neuner, Citation2015), in which patients are instructed to symbolically place representations of relevant life events along a line representing their life story. Similarly, we had participants virtually walk along a path representing their personal life story and symbolically place triggers and emotions associated with an aversive memory. As an experimental control group, we devised a similar VR task that involved walking along a path without using the symbolism of a lifeline.
Relative to control, we expected the lifeline intervention to increase automatic associations between trigger words and the past, as opposed to the present, which we assessed with a Single-Category Implicit Association Test (SC-IAT; Karpinski & Steinman, Citation2006). Phenomenologically, we expected the lifeline intervention to increase a sense of distancing, defined as a feeling of closure and psychological distance between the past and the present situation and self (cf. ‘sense of closure’; Beike & Wirth-Beaumont, Citation2005; ‘self-concept change’; Libby & Eibach, Citation2002; ‘distancing’; Sutin & Robins, Citation2007). Next, like other experimental manipulations of autobiographical memories (e.g. using guided eye-movements; Houben, Otgaar, Roelofs, Merckelbach, & Muris, Citation2020), we expected short-term reductions in memory vividness and emotionality. In the week following the intervention, we expected the Lifeline condition to reduce distress and re-experiencing, whereby symptom changes would be linearly associated with prior (changes in) automatic associations with the past and of the sense of distancing (Meyer et al., Citation2019; Schuettler & Boals, Citation2011). Finally, we explored whether potential effects extend to negative appraisals or specific negative emotions that participants associate with their aversive memories.
1. Method
1.1. Participants
One-hundred and nine participants (84.4% women) with a mean age of 22.6 years (SD = 2.8) completed this study and were allocated to the Lifeline (n = 53) or to the control (n = 56) condition (for details, see below). Six additional participants enrolled but did not complete the study and were excluded from all analyses. Participants were recruited via news bulletins, social media, and university newsletters. Inclusion criteria were age between 18 and 65 years, fluency in German, and current enrolment as a student of University of Münster. Due to ethical considerations regarding the potentially confronting nature of our procedure, we excluded candidates (a) with a history of sexual violence and (b) exceeded screening thresholds for PTSD. Further exclusion criteria were (c) current mental disorder and/or recent psychological or psychiatric treatment, (d) current psychoactive medication, (e) high alcohol (>15 units per week) or drug (>1 unit per week) consumption. All criteria were established with an online screening. Participants provided written informed consent and received a small financial compensation or partial course credits in return for completion of the study. This study was approved by the research ethics committee of University of Münster.
1.2. Screening
The screening battery was administered prior to including participants in this study and comprised general screening questions, items from the Life Event Checklist (LEC-5; Weathers et al., Citation2013), and the International Trauma Questionnaire (ITQ; Cloitre et al., Citation2018). The LEC-5 consists of a list of 17 potentially traumatic experiences, requiring participants to indicate their level of exposure. Affirmative responses on items addressing sexual violence led to exclusion from this study. In addition, we used nine items from the ITQ that assess the core PTSD symptoms re-experiencing, avoidance, sense of threat, and functional impairments on nine Likert-type items (1 = not at all; 5 = very much). Candidates were excluded if they fulfilled criteria for PTSD according to the instrument’s algorithm.
1.3. Aversive autobiographical memories
As part of a semi-structured interview administered at the beginning of the study, participants were asked to think of three situations in which they felt anxious, uneasy or shocked and which still had some emotional relevance for them today. Losing a loved person, witnessing an accident, or going unprepared into an important exam were given as possible examples. Events within the past months were not selected. For each event, participants rated on an 11-point Likert scale (0 = not at all to 10 = very much) to what extend the associated memory still elicits distress today. If participants rated all events below 6, they were asked if they could think of another more distressing event – but were not required to find one. After identifying a suitable distressing memory (i.e. preferably the most distressing event that is clearly defined in space and time), participants were asked to give it a short label, provide seven unique trigger words that reminded them of the event within their daily lives, and indicate the predominant feeling(s) associated with the memory. In preparation for the Lifeline exercise, we also recorded the participant’s age at the memory and other important life events (i.e. first day of school, first day of university, and current age). Sample and event characteristics are summarized in .
Table 1. Sample and event characteristicsfor the control and experimental group
1.4. Lifeline exercise
The VR Lifeline exercise was designed to visualize and emphasize the distance of the aversive experience in time and space. Therefore, the virtual environment depicted locations symbolizing the present moment, the aversive autobiographical memory, and other salient life events along a path representing the participant’s individual lifeline. To increase the sense of temporal distance between the aversive event and the present moment, participants were required to move (virtually) between the two points in time.
The path was constructed as a walking trail weaving through a grassy, undulating landscape, with signposts representing idiosyncratic life events (birth, first day of school, first day of university, aversive event as labelled by participants). The distance between the aversive event and the current moment was fixed at 70 m within the virtual environment (i.e. typically corresponding to about 100 walking steps). The location of all other events along the trail was adjusted accordingly, to approximate their actual chronology. The ‘current moment’ was set as the starting point of the scenario, at which sign posts pointed towards the various events and indicated the temporal distance in years or months (e.g. ‘first day of school: 20 years’). Also at the starting point, there was a table with two stone tablets laying on it. These tablets had the personal trigger words and the most relevant associated feeling(s) engraved on them, respectively.
Recorded audio instructions informed the participants about the meaning of the lifeline, signposts, and stone tablets. Then, participants were instructed to pick up the first stone tablet and carry it to the signpost representing the aversive event. Upon arrival, they had to reread the trigger words before placing the tablet onto a stone boulder. Next, participants returned to the starting point and then repeated the actions with the second stone tablet. The interactive VR scenario (including audio instructions) was programmed using CyberSession by VTplus GmbH, and was presented via an HTC Vive Pro headset. Participants carried the stone tablets and navigated by pressing and holding the trigger while continuously steering with the trackpad of the HTC Vive controller.
1.5. Control exercise: walking only
For the control condition, we designed a VR task that closely resembled the activities of the lifeline task while eliminating references to life events and their chronology. In particular, participants were not informed that the walking trail symbolizes their lifeline. Only one signpost was placed along the trail, bearing a red ‘X’. At the starting point, the signposts indicated the cardinal directions, and both stone tablets were blank. Participants of the control group were asked to carry both stone tablets separately to the signpost with the ‘X’, to look at the tablets carefully and place them on the stone boulder. The length of the path was set at 70 m, matching the Lifeline condition. Hence, in total, participants in the control condition navigated the same distance as participants in the intervention group.
1.6. Assessment of past/nowness associations
The SC-IAT (Karpinski & Steinman, Citation2006) assessed implicit associations between the idiosyncratic trigger words and the semantic concepts of now versus past and was administered after completion of the VR task. The SC-IAT is a modification of the Implicit Association Test (Greenwald et al., Citation1998; Meyer et al., Citation2019) that measures the strength of associations with one single category instead of two. Following the procedure of Karpinski and Steinman (Citation2006) implemented in Inquisit (v4; Millisecond Software), single word stimuli were presented in the middle of the screen and had to be categorized as quickly and accurately as possible by the participant, using the left (‘e’) or right (‘i’) response button on the keyboard. To indicate which of the two buttons corresponded to which category, the attributes now and past were written in the top left and right corners of the screen. In addition, the label of the participant’s aversive event (e.g. ‘car accident’) was also written either in the top left or the top right corner of the screen. Participants were instructed: ‘Words belonging to the categories above will appear in the middle of the screen. If the word belongs to the left category, press “e”. If the word belongs to the right category, press “i”. Each word belongs to only one category. When you make a mistake, an X will appear in the middle of the screen’. Word stimuli were presented until the correct response was given (i.e. requiring participants to correct error responses). The task began with a practice block (24 trials), which was followed by a test block (72 trials). Then, a second practice block and a second test block followed, in which the pairing of the event label with the attributes now and past was swapped (order of pairings was counterbalanced). The seven idiosyncratic trigger words served as word stimuli, as well as 21 synonyms for each attribute dimension (e.g. now: current, here; past: over, then).
We calculated the D-600 score in line with Greenwald, Nosek, and Banaji (Citation2003), omitting practice blocks and replacing error responses with the block average plus 600 ms error penalty. The resulting D-score represents the standardized mean difference in reaction time between the two opposite pairings, such that higher scores indicate a relatively stronger association of the aversive autobiographical event and the attribute past. On average, accuracy during the SC-IAT was 93.5% (SD = 4.0; range: 72.9–100.0).
1.7. Sense of distancing
To assess the subjective sense of distancing associated with the aversive memory at baseline and post-intervention, we devised a set of four 100 mm visual analogue scales (VAS), in part adapted from the distancing subscale of the Memory Experiences Questionnaire (MEQ; Sutin & Robins, Citation2007), as well as the Closure Scale (Beike & Wirth-Beaumont, Citation2005). These items were ‘I feel that the event is a closed matter for me’, ‘I am a very different person today compared to the time of the event’, ‘My situation today is very different from my situation at the time of the event’, ‘Memories of the event still have a large impact on my life today’ (reverse-scored). Anchors were 0 = not at all and 100 = completely. The items were selected because they capture slightly different aspects of the memory phenomenology that our experimental manipulation was aiming to alter. Since there were no separate hypotheses and in order to reduce the number of statistical analyses and the probability of Type 1 error, scores were averaged into a single distancing score (αs >.54). For exploration, we re-ran the analyses addressing experimental effects reported below separately for the four individual items, which yielded no additional Time × Condition effects.
1.8. Memory characteristics
1.8.1. Imagery task
Before and after the VR intervention, we asked participants to close their eyes and imagine the most distressing aversive event in as much detail as possible. To facilitate vivid imagery, the experimenter prompted the participant to think for a period of approximately 60 s about what they see, hear, smell, taste, or sense, while recalling as many details as possible. With eyes closed, participants then verbally indicated on 0–100 scales how vivid their memory was (0 = no imagery at all, 100 = as vivid and clear as seeing it in real life) and how distressing it was (0 = not distressing at all, 100 = very distressing). This was followed by more specific questions about the specific negative emotions fear, sadness, shame, guilt, and anger. As with the distancing scale, we had no separate hypotheses for the different negative emotions, and therefore relied on an averaged negative emotionality score across items (αs >.54) to reduce the number of statistical analyses. For exploration, we re-ran the analyses addressing experimental effects reported below separately for the five negative emotions. Findings diverging from the analyses with the single negative emotionality score are summarized in a footnote.
1.8.2. Negative appraisal
We devised ten items to measure negative personal interpretations of the aversive event based on the Posttraumatic Cognitions Inventory (PTCI; Foa, Ehlers, Clark, Tolin, & Orsillo, Citation1999) and the Trauma Relevant Assumption Scale (TRAS; Buck, Kindt, Arntz, van den Hout, & Schouten, Citation2008). The items (example: ‘For me personally, the aversive event means that I am a weak person’) were rated on 100 mm VAS (0: do not agree at all; 100: fully agree) and averaged into a single negative appraisal score (αs >.81).
1.9. Psychological distress
We used the revised Impact of Events Scale (IES-r; Weiss & Marmar, Citation1997) to assess the frequency and intensity of psychological distress associated with the most aversive memory within the past week. Respondents indicate the frequency of stress-related symptoms on 22 items with four-point Likert scales (0 = not at all, to 5 = often). The intrusions subscale (7 items; αs >.81) was of specific interest, next to the total psychological distress score (αs >.88) that also comprised subscales for avoidance (8 items; αs >.73) and hyperarousal symptoms (7 items; αs >.76). The scale was administered once at baseline and again one week after the intervention.
1.10. Procedure
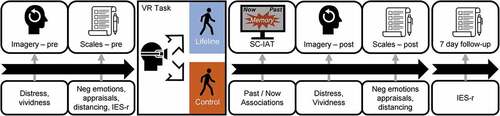
Following screening, eligible candidates were invited to an individual laboratory session. Participants first selected the aversive memory and then underwent the imagery task, providing baseline ratings for distress, vividness, and specific negative emotions. All self-report scales were administered electronically via a desktop computer, except during the imagery task where verbal responses were recorded by the experimenters. Then, they selected the trigger words and filled out baseline scales for sense of distancing, negative appraisal, and the IES-r. For blinding purposes, a separate experimenter guided the participants to an adjacent laboratory room, where the participants entered a VR training scenario to familiarize them with virtual environments and with the controller. Then, they performed the Lifeline or the control task based on a pre-determined randomization list handled by an independent researcher. After the VR task, the first experimenter (still blind to condition) administered the SC-IAT, the post-intervention imagery task, and scales on sense of distancing and negative appraisal. Finally, after one week, participants filled out the follow-up IES-r online. provides an overview of the procedure.Footnote1
Figure 1. Overview of the experimental procedure. IES-r = Impact of Event Scale, revised. Icons from thenounproject.com: change mind by Andrew Doane, exam sheet by Vectors Point, oculus rift by James Mayle, walk by Chris Thoburn; CCBY Licences
1.11. Statistical analyses
Memory distress and vividness, negative emotionality, negative appraisal, and intrusion-related symptomatology constituted the main outcome variables. Condition (Lifeline, Control) was the main independent variable. Implicit past/now associations and (an increased) sense of distancing were tested as additional predictors, potentially interacting with the condition effect. Individual extreme values on all variables were replaced such that their deviation from the entire sample mean equalled 2.5 times the sample SD (i.e. Winsorizing; Rivest, Citation1994). Mean differences were tested with mixed analyses of variance (ANOVA) and independent samples t-tests. Linear associations were tested by means of multiple linear regression and (partial) correlation analyses. Alpha was set at .05 (two-tailed) for all analyses. Based on previously reported medium-sized training effects on implicit spatio-temporal associations (average d = 0.55; Meyer et al., Citation2019), we conservatively determined a sample size of n = 53 participants per experimental condition to be sufficient to retain a power (1–β error probability) of >.80 for the two-sided detection of a between-sample difference (actual power = .81).
2. Results
2.1. Past/nowness associations and sense of distancing
We assessed effects of the experimental intervention on implicit past/nowness associations (i.e. SC-IAT D scores) with an independent samples t-test, yielding no difference between lifeline and control group, t(107) = 1.42, p = .156, d = 0.25. On average, D-scores did not indicate preferences for combining trigger words with either present or past (lifeline: M = −0.02, SD = 0.28; control: M = 0.05, SD = 0.27). Next, we addressed experimental effects on sense of distancing scores in a 2 (Time: Baseline, Post-intervention) × 2 (Condition: Lifeline, Control) repeated measures ANOVA, again not yielding any effects: critically, there was no Time × Condition interaction, F(1,107) = 0.53, p = .468, η2p = .005, and also no main effects for Time or Condition, ps = .096, η2ps < .026. Across conditions, sense of distancing scores were 54.2 (95% CI: 50.6–57.7) before, and 55.8 (95% CI: 52.0–59.5) after the VR tasks.
2.2. Distress, vividness, and negative appraisal
summarizes mean distress and vividness during memory imagery, as well as emotionality and negative appraisal scores. For imagery distress, a 2 (Time: Baseline, Post-intervention) × 2 (Condition: Lifeline, Control) ANOVA revealed a Time × Condition interaction, F(1,107) = 7.24, p = .008, η2p = .063. This was due to a larger decrease of distress for the control group (Mchange = −10.0, SD = 16.8) than in the Lifeline group (Mchange = −1.9, SD = 15.4), t (107) = 2.62, p = .010, d = 0.50. A similar interaction emerged for imagery vividness, F (1,107) = 5.16, p = .025, η2p = .046, again due to a larger decrease in the control group (Mchange = −7.9, SD = 15.6) than in the Lifeline group (Mchange = −1.8, SD = 12.3), t (107) = 2.27, p = .025, d = 0.43. However, note that excluding 4 participants with technical problems, this effect was smaller and not significant (p = .050; η2p = .037).
Table 2. Mean scores (SDs) of imagery vividness and distress, emotionality, and negative appraisal at baseline and post-intervention
For the negative emotions scale, there was no Time × Condition interaction, F(1,107) = 0.40, p = .529, η2p = .004,Footnote2 but a main effect of Time emerged, F(1,107) = 55.34, p < .001, η2p = .341, indicating an average decrease over time by 7.23 points (SD = 10.1) across conditions. Similarly, negative appraisal scores decreased over time by 3.9 points (SD = 5.8), F(1,107) = 49.78, p < .001, η2p = .318, which was unaffected by Condition, F (1,107) = 0.23, p = .633, η2p = .002.
2.3. Psychological distress
Mean IES-r scores are summarized in . A 2 (Time: baseline, one-week follow-up) × 2 (Condition Lifeline, Control) ANOVA on IES-r Intrusion scores revealed a main effect of Time, F (1,107) = 5.37, p = .022, η2p = .048, that did not interact with Condition, F(1,107) = 0.10, p = .755, η2p = .001. Scores decreased on average by 1.1 points (SD = 5.0). Similar main effects of Time were present for IES-r total scores, F(1,107) = 10.33, p = .002, η2p = .088 (Mchange = 3.3, SD = 11.1), and the Avoidance and Hyperarousal subscales (ps <.013), all in the absence of interactions with condition (all ps > .53).
Table 3. Mean impact of event scale – revised (IES-r) scores at baseline and follow-up
2.4. Predictors of change
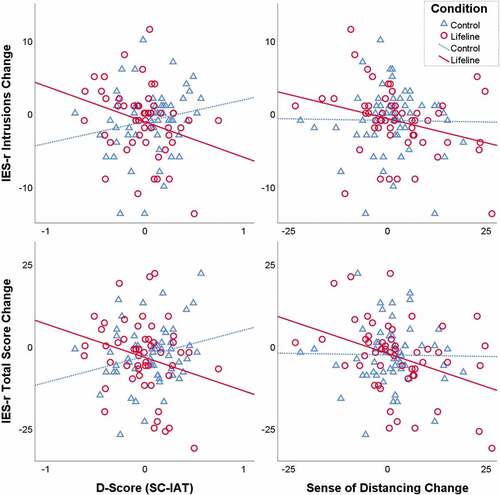
We tested for linear associations between implicit past/nowness associations and the outcomes, as well as potential interactions with Condition in hierarchical regression models. In step 1, we entered the respective Baseline scores, Condition (Control group serving as reference), as well as the SC-IAT D-scores as predictors. In a second step, we entered the interaction term Condition × D-Score (i.e. Lifeline dummy × z-transformed D-Scores). For details for all models, see Supplemental Table S1. A Condition × D-Score interactions emerged for IES-r Intrusions and IES-r Total scores (βs < −.22), indicating a stronger negative correlation between D-Scores (i.e. associations with the concept ‘past’) and intrusion-related symptoms in the Lifeline as compared with the control condition. Follow-up partial correlation analyses (controlling for baseline) in the Lifeline condition revealed negative partial correlations between D-scores and IES-r intrusions, r (df = 50) = −.309, p = .026, and IES-r total scores, r = −.276, p = .048 – though note that some of these effects are no longer significant when four participants with technical problems were excluded from the sample.Footnote3 In the control condition, these associations were positive and non-significant, ps >.18. These interactions are further illustrated in . For imagery distress, vividness, emotionality and negative appraisal, no significant partial correlations with D-scores emerged across the entire sample (df = 106), all ps > .20.
Next, we tested for potential interactions of the subjective sense of distancing with Condition. We entered sense of distancing change scores (post-intervention minus baseline) in step 1, followed by the respective interaction term in step two. Details of these regressions can be inspected in Supplemental Table S2. Critically, none of the models indicated a significant interaction term. Accordingly, we ran partial correlations between post-intervention sense of distancing and IES-r scores across the entire sample, correcting for the baseline scores of both variables. Negative partial correlations emerged for IES-r Intrusion scores, r(df = 105) = −.221, p = .022, as well as for IES-r total scores, r = −.273, p = .004, but not for imagery distress, emotionality, or negative appraisal, all ps > .37. To illustrate, depicts the correlations between sense of distancing and IES-r change scores, which were (non-significantly) larger in the Lifeline as compared to the Control condition.
Figure 2. Illustration of linear associations between D-Scores and sense of distancing with changes in IES-r scores per condition. Higher D-scores indicate a stronger association of the event triggers with ‘past’ relative to ‘present’. Regression analyses indicated significant interactions of Condition with D-Scores but not with sense of distancing
3. Discussion
We investigated whether strengthening automatic associations of aversive memories with the past and a sense of distancing through a VR-based lifeline exercise can reduce memory-related distress. Both the lifeline exercise and the walking-only control manipulation were followed by decreased re-experiencing, negative emotions, and negative appraisals, without statistical differences between the two groups. Also, participants in both conditions displayed similar past/nowness associations on the SC-IAT and comparable levels of sense of distancing. Against expectations, the control group had even lower distress and vividness scores immediately post-intervention than the lifeline condition. Meanwhile, in the lifeline condition, participants with higher SC-IAT D-scores (i.e. associations with the past), and those reporting a higher sense of distancing post-intervention, also had more pronounced reductions in intrusion-related symptomatology.
While the lifeline exercise was unsuccessful in reducing memory-related distress (relative to control), a striking pattern of findings was that in this condition, participants who preferentially associated their memory triggers with the past had the most pronounced reduction in re-experiencing symptoms in the following week. Moreover, this was paralleled by negative associations between IES-r scores and participants’ subjective sense of distancing – i.e. the degree to which they felt that their current situation and self is psychologically distant from the memory, perhaps by giving them a sense of closure (Beike & Wirth-Beaumont, Citation2005; Libby & Eibach, Citation2002; Sutin & Robins, Citation2007). As such, the pattern we found among healthy individuals aligns with prior findings linking a sense of closure with fewer PTSD symptoms (Schuettler & Boals, Citation2011). Moreover, Meyer et al. (Citation2019) experimentally induced intrusive memories using traumatic films and found tentative evidence that participants developed more re-experiencing symptoms for films that were preferentially associated with ‘present’ rather than with ‘past’ on an IAT. Our current results could suggest that automatic spatio-temporal associations may not only be linked with the initial development of intrusive memories, but also with intrusions of well-consolidated autobiographic memories. This interpretation would be in line with the key theoretical assumption that intrusive memories result from trauma representations that are poorly embedded and contextualized (Brewin et al., Citation2010; Ehlers & Clark, Citation2000). Note, however, that our experimental manipulation did not succeed in altering intrusive memories or the key predictors of change, meaning that no causal conclusions can be drawn based on our data.
The interaction of experimental condition with SCIAT D-scores may also indicate that our short lifeline exercise was effective only among participants who had less pronounced automatic spatio-temporal associations with the present to begin with. Although tentatively, these interpretations lend initial support to the rationale of the lifeline exercise in NET (Elbert et al., Citation2015), where the chronological visualization of critical life events serves as a short-term intervention to reorganize memory and alleviate PTSD. Of note, our lifeline exercise differs from the one used in NET in two crucial aspects: first, it was designed for negative memories in healthy participants rather than for traumatic memories, and second, we added a walking trail that was theorized to increase the subjective perception of spatio-temporal distance.
The above-mentioned theoretical considerations are limited by the fact that our Lifeline exercise did not differ on average from the walking-only task with respect to spatio-temporal associations or distancing. Consequently, it does not appear surprising that on the group level, there also were no effects on memory-related distress and symptomatology. A straightforward interpretation of this pattern of findings is that our Lifeline exercise was too weak to produce noticeable and clinically relevant effects. This calls for replications with an extended and more powerful Lifeline exercise (e.g. as a multisession intervention). In light of the tentative support for enhanced adaptive memory reorganization, this approach may be a promising avenue for future research.
An alternative view on our findings is that our walking-only control condition may have actively produced beneficial effects – through a different and yet unknown mechanism – thereby suppressing experimental group differences. Indeed, the walking-only exercise was followed by more pronounced reductions in vividness and emotionality than the lifeline exercise (a pattern that also emerged for the feeling sadness in our exploratory analyses). This finding runs counter to the idea that the symbolic visualization of chronological life events was the single ‘active ingredient’ varying between conditions. Speculatively, the walking-only exercise may have attenuated memory distress through distraction and/or active visuospatial engagement with the virtual environment (James et al., Citation2016; but see Meyer et al., Citation2020), possibly by disrupting reconsolidation/re-encoding of the aversive memories (e.g. James et al., Citation2015). Meanwhile, the Lifeline condition entailed more active engagement with aversive memory triggers, whereas the walking-only exercise was entirely unrelated to the memory. Accordingly, the short-term group differences may result from the longer exposure to the aversive memory in the Lifeline condition. Interestingly, this did not translate into group differences in IES-r scores in the following week, which leaves it to speculation whether the Lifeline intervention would have been superior to a memory-engaging control condition. Note that prior studies reporting successful manipulations of emotionality and vividness often relied on control conditions in which the aversive memories were activated (for review, see Houben et al., Citation2020).
3.1. Limitations
A number of limitations are noteworthy. First, healthy and non-traumatized participants reported mild to moderate distress when thinking about the events. Consequently, the results may not directly translate to trauma-exposed individuals. Note that we specifically excluded traumatized individuals due to ethical considerations, because the confronting Lifeline exercise was newly devised for this study and hence, no empirical data was available to justify its application among clinical samples. Should the Lifeline exercise turn out to be effective in reducing distress, we thus recommend extending this line of research to clinical samples in the next step. Second, our ability to detect effects involving automatic associations and memory characteristics is naturally bound to the reliability of our instruments. For instance, our SC-IAT relied on idiosyncratically chosen trigger words as stimuli. While strengthening the external validity of our study and findings, this may have introduced uncontrolled variance and reduced statistical power. However, note that a number of studies have demonstrated the validity of SC-IAT measures (e.g. Bluemke & Friese, Citation2008), and idiosyncratic stimulus selection may not negatively impact the reliability or correlations with convergent measures (Stieger, Göritz, & Burger, Citation2010). In a similar vein, our internal consistency analyses indicated that the sense of distancing scale may have suboptimal reliability. This limitation is possibly due to the small number of items, and partly offset by the fact that we could administer this scale repeatedly – with adequate stability of pre- to post-intervention scores across the sample (r = .868). Still, a replication with refined and additional phenomenology measures is desirable.
3.2. Conclusions
This study adds further evidence to the idea that re-experiencing symptoms are a consequence of inaccessible spatio-temporal context information surrounding a traumatic experience. Our results tentatively suggest that linking aversive memory with the past and perceiving it as a distant, closed event may help reducing trauma-related symptomatology. Since our intervention may have fostered this process and since additional effects may emerge against different control conditions, we view our VR based Lifeline exercise as a research tool that merits further development and testing. Critically, careful comparisons with conditions controlling for exposure and memory activation are warranted. In addition, automated computerized trainings may prove to be a fruitful avenue for future research. Eventually, this line of research may inform memory-focused therapies for PTSD and lead to the improvement of targeted interventions.
Supplemental Material
Download MS Word (18 KB)Supplemental Material
Download MS Word (17.6 KB)Acknowledgments
We are especially thankful to Katharina Wanninger, Gesa Beele, and Maika Reißel for their help in collecting the data and in the implementation of this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The data supporting the findings reported in this paper are openly available in the Open Science Framework repository at: https://osf.io/2n5ve
Supplementary material
Supplemental data for this article can be accessed here.
Additional information
Funding
Notes
1. Due to technical and/or experimenter error, 4 participants experienced technical difficulties during the VR tasks or were inadvertently given information that may have unblinded the manipulation. Excluding them from the analyses leaves the interpretation of results unaltered, except for two effects highlighted with footnotes. Four different participants failed to fill out the follow-up IES-r on time but completed it with some delay. Excluding these participants from the IES-r analyses leaves the interpretation of results virtually unchanged.
2. For exploration, we repeated this analysis separately for the negative emotions anxiety, sadness, shame, guilt, and anger. Only for sadness, the Time × Condition interaction was significant at trend level, F = 4.03, p = .047, η²p = .036, with stronger decreases in the Control (d = −0.64) than in the Lifeline condition (d = −0.37).
3. When removing 4 participants with technical problems, the interaction remained significant for IES-Intrusions but not total scores (see Supplementary Table 1). In line with this, the partial correlation for IES-Total in the Lifeline condition was slightly reduced and no longer significant (r = −.256, p = .072).
References
- Adler, M., & Rungta, S. (2002). Integrating new members into an ongoing therapy group: The life-line technique. Group, 26(4), 283–11. doi:10.1023/A:1021069312768
- Beike, D., & Wirth-Beaumont, E. (2005). Psychological closure as a memory phenomenon. Memory, 13(6), 574–593. doi:10.1080/09658210444000241
- Birrer, E., Michael, T., & Munsch, S. (2007). Intrusive images in PTSD and in traumatised and non-traumatised depressed patients: A cross-sectional clinical study. Behaviour Research and Therapy, 45(9), 2053–2065. doi:10.1016/j.brat.2007.03.005
- Bisby, J. A., Burgess, N., & Brewin, C. R. (2020). Reduced memory coherence for negative events and its relationship to posttraumatic stress disorder. Current Directions in Psychological Science, 29(3), 267–272. doi:10.1177/0963721420917691
- Bluemke, M., & Friese, M. (2008). Reliability and validity of the Single-Target IAT (ST-IAT): Assessing automatic affect towards multiple attitude objects. European Journal of Social Psychology, 38(6), 977–997. doi:10.1002/ejsp.487
- Brewin, C. R., Gregory, J. D., Lipton, M., & Burgess, N. (2010). Intrusive images in psychological disorders: Characteristics, neural mechanisms, and treatment implications. Psychological Review, 117(1), 210–232. doi:10.1037/a0018113
- Buck, N., Kindt, M., Arntz, A., van den Hout, M., & Schouten, E. (2008). Psychometric properties of the trauma relevant assumptions scale. Journal of Anxiety Disorders, 22(8), 1496–1509. doi:10.1016/j.janxdis.2008.03.010
- Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., … Hyland, P. (2018). The international trauma questionnaire: Development of a self-report measure of ICD-11 PTSD and complex PTSD. Acta Psychiatrica Scandinavica, 138(6), 536–546. doi:10.1111/acps.12956
- Crespo, M., & Fernández-Lansac, V. (2016). Memory and narrative of traumatic events: A literature review. Psychological Trauma: Theory, Research, Practice, and Policy, 8(2), 149. doi:10.1037/tra0000041
- Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345. doi:10.1016/S0005-7967(99)00123-0
- Elbert, T., Schauer, M., & Neuner, F. (2015). Narrative exposure therapy (NET): Reorganizing memories of traumatic stress, fear, and violence. In U. Schnyder & M. Cloitre (Eds.),Evidence based treatments for trauma-related psychological disorders (pp. 229–253). Springer.
- Foa, E. B., Ehlers, A., Clark, D. M., Tolin, D. F., & Orsillo, S. M. (1999). The Posttraumatic Cognitions Inventory (PTCI): Development and validation. Psychological Assessment, 11(3), 303–314. doi:10.1037/1040-3590.11.3.303
- Foa, E. B., Huppert, J. D., & Cahill, S. P. (2006). Emotional processing theory: An update. In B. O. Rothbaum (Eds.),Pathological anxiety: Emotional processing in etiology and treatment (pp. 3–24). New York: The Guilford Press.
- Greenwald, A. G., McGhee, D. E., & Schwartz, J. L. (1998). Measuring individual differences in implicit cognition: The Implicit Association Test. Journal of Personality and Social Psychology, 74(6), 1464. doi:10.1037/0022-3514.74.6.1464
- Greenwald, A. G., Nosek, B. A., & Banaji, M. R. (2003). Understanding and using the implicit association test: I. An improved scoring algorithm. Journal of Personality and Social Psychology, 85(2), 197. doi:10.1037/0022-3514.85.2.197
- Houben, S. T. L., Otgaar, H., Roelofs, J., Merckelbach, H., & Muris, P. (2020). The effects of eye movements and alternative dual tasks on the vividness and emotionality of negative autobiographical memories: A meta-analysis of laboratory studies. Journal of Experimental Psychopathology, 11(1), 2043808720907744. doi:10.1177/2043808720907744
- James, E. L., Bonsall, M. B., Hoppitt, L., Tunbridge, E. M., Geddes, J. R., Milton, A. L., & Holmes, E. A. (2015). Computer game play reduces intrusive memories of experimental trauma via reconsolidation-update mechanisms. Psychological Science, 26(8), 1201–1215. doi:10.1177/0956797615583071
- James, E. L., Lau-Zhu, A., Clark, I. A., Visser, R. M., Hagenaars, M. A., & Holmes, E. A. (2016). The trauma film paradigm as an experimental psychopathology model of psychological trauma: Intrusive memories and beyond. Clinical Psychology Review, 47, 106–142. doi:10.1016/j.cpr.2016.04.010
- Karpinski, A., & Steinman, R. B. (2006). The single category implicit association test as a measure of implicit social cognition. Journal of Personality and Social Psychology, 91(1), 16. doi:10.1037/0022-3514.91.1.16
- Libby, L. K., & Eibach, R. P. (2002). Looking back in time: Self-concept change affects visual perspective in autobiographical memory. Journal of Personality and Social Psychology, 82(2), 167. doi:10.1037/0022-3514.82.2.167
- Meyer, T., Brewin, C. R., King, J. A., Nijmeijer, D., Woud, M. L., & Becker, E. S. (2020). Arresting visuospatial stimulation is insufficient to disrupt analogue traumatic intrusions. PLoS ONE, 15(2), e0228416. doi:10.1371/journal.pone.0228416
- Meyer, T., Ikani, N., & Morina, N. (2019). Spatio-temporal associations with memory cues are linked to analogue traumatic intrusions. Behaviour Research and Therapy, 123, 103481. doi:10.1016/j.brat.2019.103481
- Meyer, T., Krans, J., van Ast, V., & Smeets, T. (2017). Visuospatial context learning and configuration learning is associated with analogue traumatic intrusions. Journal of Behavior Therapy and Experimental Psychiatry, 54, 120–127. doi:10.1016/j.jbtep.2016.07.010
- Meyer, T., Smeets, T., Giesbrecht, T., Quaedflieg, C. W. E. M., Girardelli, M. M., Mackay, G. R. N., & Merckelbach, H. (2013). Individual differences in spatial configuration learning predict the occurrence of intrusive memories. Cognitive, Affective & Behavioral Neuroscience, 13(1), 186–196. doi:10.3758/s13415-012-0123-9
- Michael, T., Ehlers, A., Halligan, S. L., & Clark, D. M. (2005). Unwanted memories of assault: What intrusion characteristics are associated with PTSD? Behaviour Research and Therapy, 43(5), 613–628. doi:10.1016/j.brat.2004.04.006
- Rivest, L. P. (1994). Statistical properties of Winsorized means for skewed distributions. Biometrika, 81(2), 373–383. doi:10.1093/biomet/81.2.373
- Rubin, D. C., Berntsen, D., & Bohni, M. K. (2008). Memory-based model of posttraumatic stress disorder: Evaluating basic assumptions underlying the PTSD diagnosis. Psychological Review, 115(4), 985–1011. doi:10.1037/a0013397
- Schnyder, U., Ehlers, A., Elbert, T., Foa, E. B., Gersons, B. P. R., Resick, P. A., … Cloitre, M. (2015). Psychotherapies for PTSD: What do they have in common? European Journal of Psychotraumatology, 6(1), 28186. doi:10.3402/ejpt.v6.28186
- Schuettler, D., & Boals, A. (2011). The path to posttraumatic growth versus posttraumatic stress disorder: Contributions of event centrality and coping. Journal of Loss & Trauma, 16(2), 180–194. doi:10.1080/15325024.2010.519273
- Sierk, A., Manthey, A., King, J., Brewin, C. R., Bisby, J. A., Walter, H., … Daniels, J. K. (2019). Allocentric spatial memory performance predicts intrusive memory severity in posttraumatic stress disorder. Neurobiology of Learning and Memory, 166, 107093. doi:10.1016/j.nlm.2019.107093
- Smith, K. V., Burgess, N., Brewin, C. R., & King, J. A. (2015). Impaired allocentric spatial processing in posttraumatic stress disorder. Neurobiology of Learning and Memory, 119, 69–76. doi:10.1016/j.nlm.2015.01.007
- Stieger, S., Göritz, A. S., & Burger, C. (2010). Personalizing the IAT and the SC-IAT: Impact of idiographic stimulus selection in the measurement of implicit anxiety. Personality and Individual Differences, 48(8), 940–944. doi:10.1016/j.paid.2010.02.027
- Sutin, A. R., & Robins, R. W. (2007). Phenomenology of autobiographical memories: The memory experiences questionnaire. Memory, 15(4), 390–411. doi:10.1080/09658210701256654
- Weathers, F., Blake, D., Schnurr, P., Kaloupek, D., Marx, B., & Keane, T. (2013). The life events checklist for DSM-5 (LEC-5): Instrument available from the National Center for PTSD. www.ptsd.va.gov.
- Weiss, D. S., & Marmar, C. R. (1997). The impact of event scale-revised. In J. P. Wilson & T. M. Keane (Eds.), Assessing Psychological Trauma and PTSD (pp. 399–411). New York: Guilford.
- Woud, M. L., Verwoerd, J., & Krans, J. (2017). Modification of cognitive biases related to posttraumatic stress: A systematic review and research agenda. Clinical Psychological Review, 54, 81–95. doi:10.1016/j.cpr.2017.04.003