
ABSTRACT
Background
Does exposure to events that transgress accepted norms, such as killing innocent civilians, prompt the psychological and emotional consequences of moral injury among soldiers? Moral injury is associated with negative emotions such as guilt, shame and anger, and a sense of betrayal and is identified among veterans following exposure to potentially morally injurious events (PMIE).
Objective
We experimentally investigate how PMIE characteristics affect the intensity of MI and related negative moral emotions in participants with varied military experience.
Method
We conducted three controlled, randomized experiments. Each exposed male respondents with active combat experience (Study 1) and varied military experience (Study 2) to four textual vignettes describing PMIE (child/adult and innocent/non-innocent suspect) that transpire at an Israeli checkpoint in the West Bank. In study 3, we exposed participants to two scenarios, where descriptions of police officers enforcing COVID 19 restrictions confronted lockdown violators.
Results
Participants assigned to vignettes describing killing an innocent civilian exhibited more intense levels of shame and guilt than those assigned to vignettes describing killing a person carrying a bomb. Religiosity and political ideology were strong predictors of guilt and shame in response to descriptions of checkpoint shootings. These effects disappeared in Study 3, suggesting that political ideology drives MI in intergroup conflict.
Conclusions
Background and PMIE-related characteristics affect the development of moral injury. Additionally, lab experiments demonstrate the potential and limitations of controlled studies of moral injury and facilitate an understanding of the aetiology of moral injury in a way unavailable to clinicians. Finally, experimental findings and methodologies offer further insights into the genesis of moral injury and avenues for therapy and prophylaxis.
HIGHLIGHTS
In three controlled experiments among participants with varied combat experience, morally injurious events characterized by killing innocent suspects triggered a greater degree of moral injury and related moral emotions than events characterized by killing non-innocent suspects.
Antecedentes: ¿La exposición a eventos que transgreden las normas aceptadas, como matar a civiles inocentes, provocan las consecuencias psicológicas y emocionales del daño moral entre los soldados? El daño moral (DM) se asocia con emociones negativas como la culpa, la vergüenza y la ira, y un sentido de traición y es identificado entre los veteranos después de la exposición a eventos potencialmente dañinos moralmente (EPDM).
Objetivo: Investigamos experimentalmente cómo las características de EPDM afectan la intensidad del DM y emociones moralmente negativas relacionadas en participantes con vasta experiencia militar.
Método: Realizamos tres experimentos controlados y aleatorizados. Cada varón expuesto respondió con experiencia en combate activo (Estudio 1) y vasta experiencia militar (Estudio 2) a cuatro viñetas textuales que describen EPDM (niño/adulto y sospechoso inocente/no inocente) que suceden en un puesto de control israelí en Cisjordania. En el estudio 3, expusimos a los participantes a dos escenarios, donde las descripciones de los agentes de policía que aplicaban las restricciones de COVID-19 enfrentaron a los infractores del confinamiento.
Resultados: Los participantes asignados a viñetas que describen el asesinato de un civil inocente exhibieron niveles más intensos de vergüenza y culpa que los asignados a las viñetas que describen el asesinato de una persona llevando una bomba. La religiosidad y la ideología política fueron fuertes predictores de culpa y vergüenza en respuesta a descripciones de tiroteos en puestos de control. Estos efectos desaparecieron en el Estudio 3, lo que sugiere que la ideología política impulsa al DM en los conflictos intergrupales.
Conclusiones: Los antecedentes y las características relacionadas con el EPDM afectan el desarrollo del daño moral. Adicionalmente, los experimentos de laboratorio demuestran el potencial y las limitaciones de los estudios de daño moral y facilitan una comprensión de la etiología del daño moral de una manera no disponible para los clínicos. Por último, los hallazgos y las metodologías experimentales ofrecen perspectivas adicionales en la génesis del daño moral y las vías para la terapia y la profilaxis.
背景: 暴露于违反公认规范的事件, 例如杀害无辜平民, 是否会导致士兵道德伤害的心理和情感后果? 道德伤害与内疚, 羞耻和愤怒等负面情绪以及背叛感有关, 并且在暴露于潜在道德伤害事件 (PMIE) 的退伍军人中发现。
目的: 我们通过实验研究 PMIE 特征如何影响具有不同军事经验参与者的 MI 强度和相关负性道德情绪。
方法: 我们进行了三项随机对照实验。每个都将具有现役战斗经验 (研究1) 和不同军事经验 (研究2) 的男性受访者暴露于四个描述在一个约旦河西岸以色列检查站发生的 PMIE (儿童/成人和无辜/非无辜嫌疑人) 的文本片段。在研究 3 中, 我们将参与者暴露于两种情景, 描述了执行 COVID 19限制警察遭遇封锁违规者。
结果: 被分配到描述杀害无辜平民片段的参与者比被分配到描述杀死炸弹携带者片段的参与者表现出更强的羞耻和内疚。宗教信仰和政治意识形态是对检查站枪击事件描述的内疚和羞耻的强预测因子。这些效应在研究 3 中消失了, 这表明政治意识形态在群体内部冲突中推动了 MI。
结论: 背景和PMIE相关特征影响道德伤害的发展。此外, 实验室实验证明了道德伤害对照研究的潜力和局限性, 并以临床医生难以获得的方式促进对道德伤害病因的理解。最后, 实验结果和方法提供了对道德伤害的产生以及治疗和预防的进一步见解。
1. Introduction
Moral injury (MI) signifies the intense distress that comes with taking the life of another human being. The distress is moral because killing, however convincingly sanctioned, upends deeply held moral convictions unallayed by the principles of self-defence that permit killing in war. The distress is injurious when the impact of killing has psychological and emotional consequences and evokes guilt, shame, anger, feelings of worthlessness, anomie, self-condemnation, and low self-esteem that become debilitating (Frankfurt, Frazier, & Engdahl, Citation2017). Injurious behaviours associated with MI include withdrawal, self-handicapping and depreciation, aggression towards others, substance abuse, and self-harm (Griffin et al., Citation2019, for review). Moral injury describes this constellation of sequelae following potentially morally injurious events (PMIEs) (Litz & Kerig, Citation2019). Distinct from PTSD, moral injury is largely an act of commission. Morally injured soldiers kill others (or stand by and fail to intercede); they are not usually victims (Canetti et al., Citation2010). On the other hand, traumatized soldiers suffering from PTSD are usually victims of armed attacks against their person. As a result, PTSD is largely driven by fear and insecurity, while guilt and shame are the engines of moral injury (Maguen & Burkman, Citation2013).
PMIEs are events in which a person perpetrates, fails to prevent, or bears witness to acts that transgress deeply held moral beliefs and expectations. PMIEs embrace distinct incidents: perpetration-based events that include manifest moral and legal transgressions (e.g. mass murder) and ethically permissible acts of killing (e.g. self-defence) and betrayal-based events wherein trusted authorities pursue morally transgressive policies (Jordan, Eisen, Bolton, Nash, & Litz, Citation2017). Treatment for moral injury encourages self-forgiveness and compassion through cognitive-behavioural and other psychotherapies (Coleman, Citation2015; Litz et al., Citation2009; Shay, Citation2014; Sherman, Citation2015) and resilience training (Rizzo & Shilling, Citation2017).
Our clinical understanding of moral injury and its treatment comes almost entirely from wounded veterans from the recent wars in Iraq, Afghanistan, and Vietnam who request or require medical care. Clinical studies of morally injured veterans usefully identify the phenomenon of MI but offer limited insights into its underlying psychological mechanism or the independent variables affecting the development of MI. There are no data, for example, linking the incidence of moral injury to the identity of the victim (combatant or non-combatant) or to the circumstances of the PMIE (self-defence or collateral harm) because many soldiers who kill civilians often kill combatants too (Maguen et al., Citation2009). While some retrospective studies discern personality and demographic correlates of moral injury and associated distress, none is a controlled laboratory experiment. On the other hand, a hypothesis-driven experimental platform facilitates the study of MI in a controlled environment. It can provide the data necessary for a more precise and unified conception of MI and a better understanding of the mechanisms of moral injury. By moving this line of research to a lab setting, we can disentangle the constructs and scales to generate testable hypotheses unavailable to clinical researchers. By carefully controlling for specific aspects of PMIEs (e.g. the identity of the victim or the circumstances of the killing) and by examining different manifestations of MI and its related emotions (e.g. guilt and shame), it is possible to determine and evaluate the predictors of each emotional component of moral injury. Controlled experiments facilitate the study of large cohorts of participants with varied characteristics (e.g. combat experience, political ideology) and allow researchers to evaluate how individual differences affect the perception of events as morally injurious.
The current study develops a lab-based MI model using vignettes to elicit a mild MI effect in participants, identify the situational triggers that affect moral injury, investigate how socio-demographic variables interact with the MI effect, and assess the importance of conflict vs. civilian settings. Importantly, we examine how the MI measures used in clinical investigations are relevant to lab-based investigations, how these scales relate to traditional metrics of moral emotions such as anger, guilt, and shame, and how the severity of moral injury depends on the salience of various components of potentially morally injurious events. Through a series of controlled, randomized experiments, we exposed 740 male respondents, with and without military experience, to four shooting scenarios that transpire at an Israeli checkpoint. The vignettes portray a PMIE where experimental subjects shoot and kill a suspect who approaches the checkpoint but refuses to stop when ordered. The vignettes differ concerning the suspect’s identity (child or adult) and the post hoc moral justification of the shooting. In half the scenarios, the suspect carries a bomb and is non-innocent, and in half, the suspect does not and is innocent. The terms innocent/non-innocent follow the literal meaning of threatening/non-threatening to represent an objective state of affairs rather than a legal category or state of mind. In a follow-up experiment, we moved to the civilian arena where police officers (not soldiers) confronted compatriots (not enemy agents) violating COVID-19 restrictions. Following the experimental manipulation, participants completed a MI scale and instruments measuring the moral emotions of guilt, shame, and anger. This experimental framework further permits us to examine how extant MI instruments perform outside a clinical context and how they relate to standardized moral emotion scales. In addition, these experiments allow us to distinguish among discrete PMIEs and to gauge their effects on MI.
2. Literature review and hypotheses
The MI constructs and scales prevalent in the clinical literature are closely tied to PMIEs, moral emotions, and demographic variables. However, as we move to the lab setting, we can disentangle the constructs and scales to generate testable hypotheses unavailable to clinical researchers.
2.1. PMIE characteristics and the severity of MI
Intuitively, a person who kills a threatening agent in self-defence should suffer less distress or injury than one who kills an innocent person (Fontana & Rosenheck, Citation1999). But the intuition is not straightforward. The justice of killing in self-defence may depend on the competence of the killer. A child playing with a rifle may be as threatening as a knife-wielding burglar, but each killing is sure to evoke a different degree of distress, shame, anger, or guilt (Schorr et al., Citation2018). An innocent person killed in cold blood will evoke a very different reaction than one killed by accident. In each case, our response to killing turns on the liability of the target. In war, liability also varies (Coleman, Citation1976; Crawford, Citation2013). Armed enemy combatants are the most threatening and should excite the least compunction, while the deaths of innocent civilians, whether young or old, should elicit the greatest moral distress.
The clinical picture, however, tells a somewhat different story. Here, children’s deaths affect combat soldiers more strongly than the deaths of innocent adults. Children also figure prominently in morally injurious events and events associated with severe PTSD (Currier, McCormick, & Drescher, Citation2015; Held, Klassen, Brennan, & Zalta, Citation2018; Schorr et al., Citation2018). Among a sample of Vietnam veterans, 13% were directly involved in an event where women, children, or the elderly were injured or killed. These veterans suffered greater emotional and psychological distress and functional impairment (PTSD and disassociative experience) than those not involved in the deaths of women or children (Maguen et al., Citation2009). It may be that armed soldiers believe that children are more innocent than male adults who may passively or indirectly aid insurgents in ways children cannot or that armed soldiers have a special obligation to protect women, the elderly, and children during wartime. In contrast, Smith, Duax, and Rauch (Citation2013), report on four traumatic events that saw combat soldiers beat unarmed villagers or kill an innocent child, wounded combatants, or surrendering enemy soldiers. Their report does not distinguish among the victims, and, in each case, the perpetrators suffered severe and debilitating guilt.
Two hypotheses test the association between MI, and the age and liability (innocence/non-innocence) of the victim:
H1: Killing a minor precipitates more intense moral injury than killing an adult.
H2: Killing an innocent party precipitates more intense moral injury than killing a non-innocent party.
To test each hypothesis in a lab setting, we first deconstructed the moral injury scale into its guilt, shame, and anger components.
2.2. Moral injury and moral emotions: guilt, shame, anger
PMIEs elicit feelings of guilt, shame, anger, and self-blame (Neria & Pickover, Citation2019; Steinmetz, Gray, & Clapp, Citation2019). Cognizant of the dominant role these variables play, standard instruments utilize guilt, shame, moral identity, the propensity to forgive, loss of trust, religious struggles, and self-condemnation to measure moral injury among combat veterans (Currier, McCormick, et al., Citation2015; Koenig et al., Citation2018; Nash et al., Citation2013).
Guilt is an emotion that arises after a moral transgression (Baumeister, Stillwell, & Heatherton, Citation1994). While many events may precipitate guilt, the guilt related to moral injury arises when a person inflicts harm on another and then perceives him or herself as a bad person (De Hooge, Zeelenberg, & Breugelmans, Citation2007). In response, the guilty person often tries to remedy the wrongdoing by undertaking measures to minimize the damage caused (Tangney, Miller, Flicker, & Barlow, Citation1996). Shame is closely related to guilt. Shame arises after a moral transgression or demonstration of incompetence (Keltner & Buswell, Citation1996) whereby one is shown to be inadequate. In response, the shamed individual experiences feelings of worthlessness and inferiority (Ausubel, Citation1955; Tangney, Wagner, & Gramzow, Citation1992) accompanied by attempts to hide or withdraw (Tangney et al., Citation1996). Anger might arise following experiencing unfairness and injustice and triggers the motivation to attack, humiliate, and seek retribution against the agent of injustice (Schamborg, Tully, & Browne, Citation2016). Responses to guilt, shame, and anger may also lead individuals to acknowledge their in-group’s responsibility, apologize or ask forgiveness, or offer reparation or compensation (e.g. Gillespie, Dietz, & Lockey, Citation2014; Kramer & Lewicki, Citation2010). Failure to address anger, whether by retribution or redress, may disrupt moral information-processing and emotion regulation and undermine the capacity for rewarding social connections (Litz & Kerig, Citation2019). Anger and retribution seeking characterize the reactions of many soldiers when they face enemy threats (Currier, McCormick, et al., Citation2015, p. 114, also: Marx et al., Citation2010).
Guilt, shame, and anger play a distinct role in the aetiology of moral injury. Shame and guilt mediate between perpetration-based events such as killing combatants and/or civilians and the resulting distress (Bryan et al., Citation2016; Jordan et al., Citation2017). Perpetration-based events describe acts of commission and killing, or acts of omission, where one refrains from interfering with or preventing acts of killing by others. In each case, shame and guilt are directed inwards towards the self. In contrast, anger mediates the association between betrayal-based PMIEs and moral distress. Betrayal-based PMIE reflect the actions of political or military superiors who order or conduct transgressive acts that MI-affected personnel cannot prevent. Here, anger is directed at others.
As this study focuses on perpetration-based events, we hypothesize a central role for guilt and shame but a less critical role for anger. Nevertheless, Vargas, Hanson, Kraus, Drescher, and Foy (Citation2013, p. 247) note that some Vietnam-era combat veterans in their sample saw ‘their inability to prevent the pain and suffering of children as consistent with betrayal.’ In which case, anger may characterize the moral distress that comes with killing children regardless of their liability.
In addition to instruments measuring moral injury, we added scales to capture the emotional outcomes of MI. While some MI scales include items of moral emotion (e.g. the Moral Injury Symptom Scale (MISS), Koenig et al., Citation2018), these scales measure moral injury following exposure to PMIEs in an austere and violent environment. They were not intended for less traumatic emotional insults and are, therefore, insufficiently sensitive to measure moral injury among test subjects responding to written vignettes. Nor would we expect such severe reactions as social withdrawal or self-condemnation (Frankfurt & Frazier, Citation2016) among experimental subjects responding to vignettes. We, therefore, decided to use dedicated measures of moral emotions: shame, guilt, and anger. These scales measure the well-documented emotional consequences of MI and generate a methodological hypothesis:
H3: In a lab-initiated perpetration-based PMIE, scales of guilt, shame and anger will correlate with MI scale.
Following this hypothesis, we can expand our initial hypotheses to the moral emotion scales:
H1a: Killing a minor precipitates more intense shame, guilt, and anger than killing an adult.
H2a: Killing an innocent party precipitates more intense shame, guilt, and anger than killing a non-innocent party.
3. Methodology and experimental design
To test hypotheses H1-H3, we first conducted two controlled, randomized experiments. Each exposed male respondents with active combat experience (Study 1) and varied military experience (Study 2) to four scenarios (experimental conditions) that transpire at an Israeli checkpoint in a between-subjects design. Regardless of military experience, most Israelis are familiar with the military scenarios our manipulations depict. Participants in both studies completed a post-survey after answering a series of questionnaires about their emotions along with relevant socio-demographic information.
Participants in both studies were divided into four groups, exposed to a different PMIE scenario. In all PMIEs, participants serve as soldiers at a military checkpoint in the West Bank. All read a paragraph informing them of a possible attack by men, women, or children armed with explosive devices. In the written vignette, the soldiers also receive instructions (rules of engagement) to fire a warning shot and then shoot at anyone approaching the checkpoint who refuses to stop when ordered, regardless of age or gender.
After reading the vignette and rules of engagement, participants were randomly assigned to one of four groups with different PMIEs. To evaluate MI’s different facets, we used a two-by-two factorial experimental design that varied the suspected perpetrator’s identity (child or adult) and the threat outcome (carried a bomb [non-innocent] or did not carry a bomb [innocent]). An unidentified man (or child) carrying a suspicious bag approaches the checkpoint and does not respond to your (the experimental subject’s) order to stop. Despite additional warnings, the suspect continues to advance and approach the checkpoint. You (the experimental subject) fire a warning shot in the air. The subject does not stop, and you shoot and kill the suspect. Upon examination, the dead child/adult was or was not carrying a bomb. (See online supplementary materials to view the different manipulation groups scenarios). In short, participants experienced one of four potentially morally injurious events:
After reading the vignettes, participants completed a detailed questionnaire exploring their levels of guilt, shame, anger, and MI. The 2 × 2 design tested H1-H4 by gauging the strength of MI, guilt, shame, and anger in four disparate situations not readily discernable on the battlefield. The multiple DV scales further allowed for assessing and identifying the dimensions of MI responding to each PMIE.
Study 1: The online survey experiment was administered in Israel in February 2020 via the Midgam Survey Panel and randomly assigned 120 adult Jewish men (>18) with combat experience to the four conditions (child/adult, bomb/no bomb). All the participants completing the survey were included in the data analysis. Table B1 in the supplementary materials displays their socio-demographic characteristics and the summary statistics of the different manipulation groups. These data indicate no significant difference between the groups.
Study 2: The online survey experiment was administered in Israel during July 2020 via the Midgam Survey Panel and randomly assigned to 495 Jewish men (>18) with and without combat experience to the four conditions (child/adult; bomb/no bomb). All the participants completing the survey were included in the data analysis. Table B2 in the supplementary materials describes socioeconomic and demographic information, and the summary statistics of the different manipulation groups. These data indicate no differences between the groups. In this study, 134 participants (27.1%) did not serve in the military, 101 participants (20.3%) served up to 3 years, 185 of them (37.4%) completed three years, and 75 participants (15.2%) served more than three years.
Study 3: In Study 3 we used a civilian-context PMIE where police officers (rather than soldiers) confronted business owners violating COVID-19 restrictions that kept shops closed. This study included two experimental conditions where a police officer issues a steep fine to an adult shop owner (Condition 1- adult) or his young child then managing the store (Condition 2-child) despite pleas that it was necessary to stay open to pay their family’s medical bills. We conducted the survey in Israel on December 29–30, 2020, during the first week of the third and near-total lockdown, randomly assigning 206 Jewish men (>18) to the child or adult vignette groups. All the participants completing the survey were included in the data analysis. The socio-demographic information and summary statistics of the different manipulation groups appear in the supplementary materials Table B3.
The University of Haifa ethics committee approved all the experiments. All participants signed a consent form after receiving an information sheet. Each person received $1.20 for participating. Upon completing the task, all participants received a debriefing page with researchers’ contact information should they experience distress or have additional questions or concerns. No one contacted the researchers following the experiment.
3.1. Measurements
This experiment incorporated four primary dependent variables: guilt, shame, anger, and moral injury. Participants provided demographic data before reading the manipulation vignette and afterwards completed the following randomized scales.
3.2. Moral injury
We adopted the nine-item Moral Injury Events Scale (MIES) (Bryan et al., Citation2016; Nash et al., Citation2013). Used to evaluate the perception and experience of MI events among combat veterans, this scale contains six questions that comprise perpetration-based events that reflect moral injury from one’s own acts or from the acts of others that one observed and failed to prevent, and three additional questions that comprise betrayal-based events. In contrast to other MI instruments such as the Moral Injury Questionnaire (Currier, Holland, et al., Citation2015), the Moral Injury Symptom Scale (Koenig et al., Citation2018), and the Expressions of Moral Injury Scale (Currier, Isaak, & McDermott, Citation2020), the MIES is combat-experience neutral and better suited to evaluate MI among participants with no combat experience and those exposed to non-military, law enforcement PMIEs as in the COVID experiment (Study 3). Following factor analysis, the MI scale yielded two factors in Study 1. Factor 1 included questions 1–6, and factor 2 included questions 7–9. These results confirm the distinction between items in this scale and track Bryan et al.’s (Citation2016) distinction between transgression by self (perpetration-based events) and transgressions by others (betrayal-based events). Because our manipulations were designed to simulate perpetration-based PMIEs or transgressions-by-self MI, we did not use questions 7–9 in the following analyses. (α Study 1 = .8; α Study 2 = .80). Each item was measured on a scale from ‘not at all’ (1) to ‘totally’ (6).
3.3. Guilt
A five-item Personal Feelings Questionnaire–2 measured guilt (Harder and Zalma (Citation1990). Participants were also asked whether they felt ‘intense guilt’ and ‘remorse’ after reading the vignette (α Study 1 = .74; α Study 2 = .84). Each item was measured on a scale from ‘not at all’ (1) to ‘totally’ (6).
3.4. Shame
A ten-item Personal Feelings Questionnaire–2 measured shame (Harder & Zalma, Citation1990). Participants were also asked whether they felt ‘embarrassed’ or “felt helpless and paralysed about the situation they just read (α Study 1 = .92; α Study 2 = .92). Each item was measured on a scale from ‘not at all’ (1) to ‘totally’ (6).
3.5. Anger
We used the State – Feeling Angry (S-Ang/F) subscale from the State-Trait Anger Expression Inventory II (Schamborg et al., Citation2016) to measure feelings of anger elicited by the vignette. Participants were also asked whether they felt ‘angry’ or ‘furious’ regarding the situation they just read about (α Study 1 = .92; α Study 2 = .95). Each item was measured on a scale from ‘not at all’ (1) to ‘totally’ (6).
3.6. Control variables
To control for the effects of prior exposure to terrorism present in many Israeli studies (Canetti, Citation2017; Canetti et al., Citation2010; Canetti-Nisim, Halperin, Sharvit, & Hobfoll, Citation2009), participants were asked whether they or their friends/family experienced a terror attack (Prior Exposure to Terrorism). Answers were ranked no/yes, scored 0–1, respectively. Battlefield Experience (Grossman, Manekin, & Miodownik, Citation2015) asked: Were you involved in a military operation where (1) civilians; (2) soldiers; (3) terrorists were injured or killed? (Yes = 1; No = 0). Military Service included length of military service, military rank, and reserve duty service. Socio-demographic variables included age, marital status, education, number of children, income, and subjective political ideology. Ideology asked: ‘How would you describe your political stance?’ Answers ranged on a 5-point scale from ‘very right-wing’ to ‘very left-wing.’ Religiosity asked: ‘How would you describe your religious observance level?’ Answers ranged on a 5-point scale from ‘very observant’ to ‘not at all.’ After verifying the correlation of these variables with the measured scales, they were added as control variables and variables of interest in analyses where such correlations were observed.
3.7. Analysis
SPSS Statistics (IBM) software was used for calculating summary statistics and correlation matrices. R Statistics Computing software was used for linear model fitting, reporting, and visualization (packages: stats, apa Tables, ggplot2). We used linear regressions to assess the effects of independent variables on dependent variables. We then examined the output of the linear models using ANCOVA tables (anova) to gain statistics such as F values and partial eta square.
4. Results
4.1. Socio-demographic and MI measures
The means, standard deviations, and inter-correlations among the study variables are displayed in Supplementary Tables D1 (Study 1) and D2 (Study 2). Significant correlations among the demographic parameters were observed. Among these, we focused on religiosity and political ideology. In addition, our scales of moral injury were highly correlated with moral emotions. We unpack these correlations in the following analysis steps.
4.2. Moral injury, shame, guilt, and anger
Before examining H1-H2, we assessed the association between responses to the MI scale and shame, guilt, and anger scales (H3). The multiple linear regression model determines the degree to which each independent variable – anger, shame, and guilt – is related to MI scores. In Study 1/Study 2 the model confirmed a significant association between scores on the modified MI scale (questions 1–6, transgression-by-self) and between shame (p = 0.038/ p < 0.0001) and guilt (p < 0.0001/ p < 0.0001). Anger was not found to significantly relate to MI scores (p = 0.919/ p = 0.267) (Full results in Supplementary Tables E1 and E2). These results confirmed the close association between the MI measures and the moral emotion scales guilt and shame (H3) and permitted us to use the latter as proxies for moral injury when the MI assessment instrument was insufficiently sensitive to capture the subjects’ responses to the experimental vignettes.
4.3. Moral injury and control variables
In Study 2 (males with and without combat experience), political ideology and religiosity are significantly associated with MI (Supplementary Table D2). Right-wing and religious respondents displayed lower MI responses on all scales. This finding was not significant in Study 1, suggesting that expanding the target population to non-combatants introduced a new dependency between background demographic variables and MI. As we are interested in examining factors affecting MI in the general population that includes those with and without combat experience, it is essential to consider that factors such as political ideology may influence participants’ responses. Here we included religiosity and political ideology when examining the effects of event characteristics on moral injury scores (Supplementary Tables F1 and F2). We also included income level and age as control variables in Experiment 2, as they correlated with some of the MI and moral emotion measures.
4.4. PMIE characteristic and MI
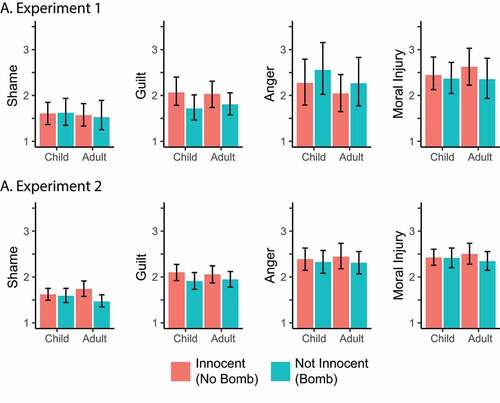
Linear regressions examined the association between the different PMIE manipulation (child/ adult, innocent/non-innocent) and MI (shame, guilt, and anger). describes the effects of the suspect’s ages and innocence on moral injury; Supplementary Tables F1 (Study 1) and F2 (Study 2) summarize the regression results. Among male combat veterans (Study 1), we observed significantly greater guilt when killing an innocent suspect (F117,1) = 4.19, p = 0.043). Among the general population male cohort (Study 2), we observed a significant interaction effect between the suspect’s age and innocence (F(1,491) = 4.86, p = 0.028) on feelings of shame, where the highest levels of shame were observed when killing innocent adults. These findings indicate that our manipulations affected some of the measures associated with moral injury. Contrary to H1 and H1a, killing a minor did not elicit any greater degree of shame and guilt than killing an adult. Consistent with H2 and H2a, however, killing an innocent suspect elicited a greater degree of guilt (Study 1) and shame (Study 2) than killing a non-innocent suspect carrying a bomb. The data do not support H3 and show no effects for anger when experimental subjects experience perpetration-based PMIEs.
Figure 1. The effect of suspect’s age and innocence on moral injury.
4.5. Study 3: MI in a non-military context
Notably, in Study 2, measures of shame, guilt, and anger increased with political ideology and religiosity (Table E2), in line with the correlations observed in the correlation matrices (Tables D1 and D2). Secular, liberal left-leaning participants suffered greater guilt and shame than the right-wing/religiously observant following the experimental manipulation. In Israel, the ‘left’ embraces a political ideology with a more favourable image of Palestinians than right-wing ideology. The Israeli left supports territorial concessions with Palestinians and a two-state solution and opposes the Israeli government’s settlement policy. The association between political ideology and moral injury in the context of the Palestinian-Israeli conflict suggests the following hypothesis:
H4: Political ideology strengthens resilience to moral injury in inter-group conflict while providing no benefit in intra-group contexts.
To explore this hypothesis, we conducted Study 3, a civilian-context PMIE where police officers (rather than soldiers) confronted business owners violating COVID-19 restrictions that kept shops closed. This study included two experimental conditions where a police officer issues a steep fine to an adult shop owner (Condition 1- adult) or his young child then managing the store (Condition 2-child) despite pleas that it was necessary to stay open to pay their family’s medical bills. After reading one of the vignettes, respondents completed the same questionnaires about guilt (α Study 3 = .80), shame (α Study 3 = .92), anger (α Study 3 = .96) and MI (α Study 3 = .84).
As in Study 1 and 2, MI scores in Study 3 were significantly associated with guilt (b = 0.43, p < 0.01) and shame (b = 0.18, p < 0.01) but not anger (Supplementary Tables D3, E3). The close relationship between MI and moral emotions is unaffected by the civilian/combat context. Simultaneously, the manipulations did not affect MI or moral emotions as they did in the earlier studies, while the effects of political ideology entirely disappeared despite similar inclusion criteria (Supplementary Table F3). While Study 2 suggests that political ideology is an important driver of MI in the general population, Study 3 lends preliminary weight to H4. Political ideology (right-wing in the Israel case) affects responses to PMIE and moral emotions in the context of inter-group conflict but does not affect MI in some intra-group settings. This finding may be related to increased resilience to MI in inter-group conflict, as suggested by our hypothesis H4, but other explanations cannot be excluded in the current experimental design. For example, right-wing Israelis may be affected by different PMIEs than those on the left.
5. Discussion
Studies of moral injury among affected combat veterans and in a clinical setting have paved the way for reliable instruments to measure the level of injury, and develop and evaluate appropriate therapies. A controlled experimental setting offers the opportunity to investigate the aetiology of moral injury in a way unavailable to clinicians. Examining the effects of vignettes among young males of combat age in Israel, many with combat experience, allowed us to test hypotheses about the genesis of MI and, with this, open the door not only to therapy but also to prophylaxis. Knowing more about the variables that predict MI makes it possible to think about those steps which might prevent it.
The first step was to develop an instrument sufficiently sensitive to vignette-induced moral distress. Standard MI scales did not register in the laboratory setting, nor are they suitable for the general population. Whether they might be more effective with a more powerful manipulation that employs audio-visual elements or VR is the subject of future research. One risk of stronger manipulations, however, might be greater stress among subjects. In this set of studies, confined to perpetration rather than betrayal-based MI, we could isolate shame and guilt measures that exhibited a strong association with clinical MI scales and responded to the experimental manipulations. These scales allowed us to investigate the association among demographic variables, moral injury, and central PMIE features that include the victim’s identity and innocence. They also provide tools to assess MI among populations without direct combat experience, which may, nonetheless, experience potentially morally injurious events.
Despite the observed effects of such situational factors (e.g. combat experience or length of deployment) or predeployment stressors (emotional trauma, abuse, mental illness, or drug abuse) (Bryan et al., Citation2016) in clinical studies, there are insufficient data to link predeployment personality traits or political ideology to the proclivity for moral injury (Frankfurt & Frazier). Doing so, write Vermetten and Jetly (Citation2018, p. 162), might make it possible ‘to identify those military members most likely to experience moral distress, to have resulting symptoms of guilt and shame, and to possibly be at a greater risk of developing combat-related PTSD and/or MDD [major depressive disorder].’ In the same vein, Nazarov et al. (Citation2015, p. 107) explains how ‘it may be possible to predict who is more likely to perceive [morally questionable] events as morally injurious by assessing predeployment styles of moral judgment using validated assessment tools.’ Moral judgement and political ideology are closely related (e.g. Emler, Citation2003; Fishkin, Keniston, & MacKinnon, Citation1973). Our data show how each may significantly affect moral injury when circumstances call for harming adults or children and for later confronting evidence that denies or confirms the suspect’s innocence.
In Israel, where the Palestinian conflict looms large, political ideology affects moral judgements about policy. In a sample of Israeli soldiers staffing a checkpoint in the Palestinian territories, for example, right-wing political attitudes strengthen justifications for Israeli policy, thereby enhancing post-deployment adjustment to civilian life (Kimhi & Sagy, Citation2008). Other studies note similar correlations between right-wing attitudes and the propensity to trivialize, dehumanize or resent enemy combatants and non-combatants (Ben-Nun Bloom, Kimhi, Fachter, Shamai, & Canetti, Citation2020; Maoz & McCauley, Citation2008). In terms of moral injury, right-wing attitudes, at least in Israel, offer some immunity to moral distress when serving in combat roles. Events that might otherwise be morally injurious no longer violate deeply held moral convictions.
To probe deeper, we divorced moral injury from the conflict/terror/military setting to look at police officers enforcing Covid-19 regulations. Here, among compatriots, political ideology did not affect feelings of guilt, shame, or anger. This finding suggests that political ideology is most salient in intergroup conflict. Of course, as the American experience has shown, Covid is easily politicized into group conflict. Here one might expect ideology to influence MI more substantially than in our Israeli sample. At the same time, the police did not inflict lethal harm on violators but only caused substantial financial loss. Less-than-lethal outcomes may, too, diminish the effects of moral injury.
Finally, these experiments allow us to disentangle some of the underlying causes of moral injury. Moral injury affects those who intentionally kill combatants and those who unintentionally or accidentally kill civilians. Liability varies with the identity of the killer and the victim. From a legal perspective, killing combatants is justifiable; collaterally killing civilians is excusable, while accidentally killing civilians is negligent, sometimes neither justifiable nor excusable (Gross, Citation2021, pp. 143–149). Each PMIE, then, is in a moral and legal class of its own and affects the intensity of moral injury that an experimental methodology can analyse. The studies in military settings also demonstrate how moral injury intensifies with the victim’s innocence, while shame increases when the victim is a minor. These findings are difficult to ascertain in a clinical setting. These preliminary results suggest that treatment for moral injury might be effectively tailored to its underlying conditions insofar as these can be determined. Compensation, for example, is a legal remedy for causing excusable harm. Therefore, restitution or ‘making amends’ might more readily expiate the moral injury suffered from collaterally killing civilians than justifiably killing a combatant where the grounds for compensation are less compelling.
A contentious role for religion also emerges from this study. Among Coalition service personnel, religious observance and ritual offered many the means to confront, make sense of, and mitigate the MI they suffered (Frame, Citation2015; Hodgson & Carey, Citation2017; Worthington & Langberg, Citation2012). Religious observance does not prevent moral injury but opens the way to moral repair following injury. In our sample, however, religion was a bulwark against moral injury in some conflict settings. Further studies will illuminate the relationship between political ideology, religious observance, and moral injury.
6. Limitations
This study is subject to several limitations that should inform future efforts to investigate moral injury experimentally. First, experimental subjects in a lab setting are not morally injured. Thus, one can only create mildly stressful MI conditions to conduct controlled studies. Future studies may go beyond textual vignettes, as used here, and employ audio/visual film clips or virtual reality to strengthen the effects of experimental manipulations. Second, civilian contexts (Study 3) that depict economic harm to shopkeepers do not provide PMIEs of the same intensity as do military contexts that depict the killing of terror suspects. This difference limits the conclusions drawn from the direct comparison between Studies 1,2 (military context) and 3 (civilian context). However, we suggest that these differences are a matter of degree and not of kind, a hypothesis that may be fully explored in future works. Third, we acknowledge biases in the sample of participants. In the studies presented here, political ideology, religiosity, and age correlated with MI scale measures in a manner that may be specific to the Israeli-Palestinian conflict. While we tried to control for such dependencies by including these variables in the analyses, future investigations will require diverse populations from different countries to validate our results. Finally, the measure of MI used in this work, the MIES, was selected based on clinical studies of veterans suffering from MI and by directly examining the features of PMIEs leading to MI. And while the MIES is the scale that depends least on specific military experiences, this instrument may have only limited relevance to the lab-based scenario, as was indicated by the smaller effect sizes of this measure. Future works may choose to modify existing scales, develop new ones suitable for non-military participants, including police officers, and/or adopt moral emotion measures similar to those utilized in this study.
7. Conclusions
Investigating moral injury in a laboratory setting facilitates two avenues of inquiry. First, by providing a platform to distinguish among the variables that contribute to moral injury, such as political ideology, there will be room to develop countervailing prophylactic measures such as moral education. Second, identifying the field conditions that precipitate moral injury increases the chances of more effective treatment for combat veterans, drone operators, and law enforcement agents.
Data availability
Due to considerations of participants’ privacy, the data that support the findings of this study are available from the corresponding author, UH, upon reasonable request.
Supplemental Material
Download MS Word (108.2 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Supplementary material
Supplemental data for this article can be accessed here
Additional information
Funding
References
- Ausubel, D. P. (1955). Relationships between shame and guilt in the socialization process. Psychological Review, 62(5), 378–11. doi:10.1037/h0042534
- Baumeister, R. F., Stillwell, A. M., & Heatherton, T. F. (1994). Guilt: An interpersonal approach. Psychological Bulletin, 115(2), 243–267. doi:10.1037/0033-2909.115.2.243
- Ben-Nun Bloom, P., Kimhi, S., Fachter, S., Shamai, M., & Canetti, D. (2020). Coping with moral threat: Moral judgment amid war on terror. Journal of Conflict Resolution, 64(2–3), 231–260. doi:10.1177/0022002719854209
- Bryan, C. J., Bryan, A. O., Anestis, M. D., Anestis, J. C., Green, B. A., Etienne, N., … Ray-Sannerud, B. (2016). Measuring moral injury: Psychometric properties of the moral injury events scale in two military samples. Assessment, 23(5), 557–570. doi:10.1177/1073191115590855
- Canetti-Nisim, D., Halperin, E., Sharvit, K., & Hobfoll, S. (2009). A new stress-based model for political extremism: Personal exposure to terrorism, psychological distress and exclusionist political attitudes. Journal of Conflict Resolution, 53(3), 363–389. doi:10.1177/0022002709333296
- Canetti, D., Galea, S., Hall, B. J., Johnson, R. J., Palmieri, P. A., & Hobfoll, S. E. (2010). Exposure to prolonged socio-political conflict and the risk of PTSD and depression among Palestinians. Psychiatry: Interpersonal and Biological Processes, 73(3), 219–231. doi:10.1521/psyc.2010.73.3.219
- Canetti, D. (2017). Emotional distress, conflict ideology, and radicalization. PS - Political Science and Politics, 50(4), 940–943. doi:10.1017/S1049096517001032
- Coleman, J. L. (1976). The morality of strict liability. William & Mary Law Review, 18(2), 259–286. https://digitalcommons.law.yale.edu/fss_papers/4206/
- Coleman, N. (2015). Moral status and reintegration. In T. Frame (Ed.), Moral injury: Unseen wounds in an age of Barbarism (pp. 116–122). Sydney NSW, Australia: UNSW Press.
- Crawford, N. C. (2013). Accountability for killing: Moral responsibility for collateral damage in America’s post-9/11 wars. Oxford: Oxford University Press.
- Currier, J. M., Holland, J. M., Drescher, K., & Foy, D. (2015). Initial psychometric evaluation of the moral injury questionnaire—military version. Clinical Psychology & Psychotherapy, 22(1), 54–63. doi:10.1002/cpp.1866
- Currier, J. M., Isaak, S. L., & McDermott, R. C. (2020). Validation of the Expressions of Moral Injury Scale‐Military version‐short form. Clinical Psychology and Psychotherapy, 27(1), 61–68. doi:10.1002/cpp.2407
- Currier, J. M., McCormick, W., & Drescher, K. D. (2015). How do morally injurious events occur? A qualitative analysis of perspectives of veterans with PTSD. Traumatology, 21(2), 106–116. doi:10.1037/trm0000027
- De Hooge, I. E., Zeelenberg, M., & Breugelmans, S. M. (2007). Moral sentiments and cooperation: Differential influences of shame and guilt. Cognition and Emotion, 21(5), 1025–1042. doi:10.1080/02699930600980874
- Emler, N. (2003). Morality and political orientations: An analysis of their relationship. European Review of Social Psychology, 13(1), 259–291. doi:10.1080/10463280240000082
- Fishkin, J., Keniston, K., & MacKinnon, C. (1973). Moral reasoning and political ideology. Journal of Personality and Social Psychology, 27(1), 109–119. doi:10.1037/h0034434
- Fontana, A., & Rosenheck, R. (1999). A model of war zone stressors and posttraumatic stress disorder. Journal of Traumatic Stress, 12(1), 111–126. doi:10.1023/A:1024750417154
- Frame, T. (2015). The influence of religious conviction. In T. Frame (Ed.), Moral injury: Unseen wounds in an age of Barbarism (pp. 132–138). Sydney: UNSW Press.
- Frankfurt, S., Frazier, P., & Engdahl, B. (2017). Indirect relations between transgressive acts and general combat exposure and moral injury. Military Medicine, 182(11–12), 1950–1956. doi:10.7205/MILMED-D-17-00062
- Frankfurt, S., & Frazier, P. (2016). A review of research on moral injury in combat veterans. Military Psychology, 28(5), 318–330. doi:10.1037/mil0000132
- Gillespie, N., Dietz, G., & Lockey, S. (2014). Organizational reintegration and trust repair after an integrity violation: A case study. Business Ethics Quarterly, 24(3), 371–410. doi:10.5840/beq2014437
- Griffin, B. J., Purcell, N., Burkman, K., Litz, B. T., Bryan, C. J., Schmitz, M., … Maguen, S. (2019). Moral injury: An integrative review. Journal of Traumatic Stress, 23(3), 350–362. doi:10.1002/jts.22362
- Gross, M. L. (2021). Military medical ethics in contemporary armed conflict: Mobilizing medicine in the pursuit of just war. Oxford: Oxford University Press.
- Grossman, G., Manekin, D., & Miodownik, D. (2015). The political legacies of combat: Attitudes toward war and peace among Israeli ex-combatants. International Organization, 69(4), 981–1009. doi:10.1017/S002081831500020X
- Harder, D. H., & Zalma, A. (1990). Two promising shame and guilt scales: A construct validity comparison. Journal of Personality Assessment, 55(3–4), 729–745. doi:10.1080/00223891.1990.9674108
- Held, P., Klassen, B. J., Brennan, M. B., & Zalta, A. K. (2018). Using prolonged exposure and cognitive processing therapy to treat veterans with moral injury-based PTSD: Two case examples. Cognitive and Behavioral Practice, 25(3), 377–390. doi:10.1016/j.cbpra.2017.09.003
- Hodgson, T. J., & Carey, L. B. (2017). Moral injury and definitional clarity: Betrayal, spirituality and the role of chaplains. Journal of Religion and Health, 56(4), 1212–1228. doi:10.1007/s10943-017-0407-z
- Jordan, A. H., Eisen, E., Bolton, E., Nash, W. P., & Litz, B. T. (2017). Distinguishing war-related PTSD resulting from perpetration- and betrayal-based morally injurious events. Psychological Trauma: Theory, Research, Practice, and Policy, 9(6), 627–634. doi:10.1037/tra0000249
- Keltner, D., & Buswell, B. N. (1996). Evidence for the distinctness of embarrassment, shame and guilt: A study of recalled antecedents and facial expressions of emotion. Cognition and Emotion, 10(2), 155–171. doi:10.1080/026999396380312
- Kimhi, S., & Sagy, S. (2008). Moral justification and feelings of adjustment to military law-enforcement situation: The case of Israeli soldiers serving at army roadblocks. Mind & Society, 7(2), 177. doi:10.1007/s11299-008-0051-0
- Koenig, H. G., Ames, D., Youssef, N. A., Oliver, J. P., Teng, E. J., Haynes, K., … Pearce, M. (2018). The Moral Injury Symptom Scale–Military version. Journal of Religion and Health, 57(1), 249–265. doi:10.1007/s10943-017-0531-9
- Kramer, R. M., & Lewicki, R. J. (2010). Repairing and enhancing trust: Approaches to reducing organizational trust deficits. Academy of Management Annals, 4(1), 245–277. doi:10.5465/19416520.2010.487403
- Litz, B. T., & Kerig, P. K. (2019). Introduction to the special issue on moral injury: Conceptual challenges, methodological issues, and clinical applications. Journal of Traumatic Stress, 32(3), 341–349. doi:10.1002/jts.22405
- Litz, B. T., Stein, N., Delaney, E., Lebowitz, L., Nash, W. P., Silva, C., & Maguen, S. (2009). Moral injury and moral repair in war veterans: A preliminary model and intervention strategy. Clinical Psychology Review, 29(8), 695–706. doi:10.1016/j.cpr.2009.07.003
- Maguen, S., & Burkman, K. (2013). Combat-related killing: Expanding evidence-based treatments for PTSD. Cognitive and Behavioral Practice, 20(4), 476–479. doi:10.1016/j.cbpra.2013.05.003
- Maguen, S., Metzler, T. J., Litz, B. T., Seal, K. H., Knight, S. J., & Marmar, C. R. (2009). The impact of killing in war on mental health symptoms and related functioning. Journal of Traumatic Stress, 22(5), 435–443. doi:10.1002/jts.20451
- Maoz, I., & McCauley, C. (2008). Threat, dehumanization, and support for retaliatory aggressive policies in asymmetric conflict. Journal of Conflict Resolution, 52(1), 93–116. doi:10.1177/0022002707308597
- Marx, B. P., Foley, K. M., Feinstein, B. A., Wolf, E. J., Kaloupek, D. G., & Keane, T. M. (2010). Combat-related guilt mediates the relations between exposure to combat-related abusive violence and psychiatric diagnoses. Depression and Anxiety, 27(3), 287–293. doi:10.1002/da.20659
- Nash, W. P., Marino Carper, T. L., Mills, M. A., Au, T., Goldsmith, A., & Litz, B. T. (2013). Psychometric evaluation of the Moral Injury Events Scale. Military Medicine, 178(6), 646–652. doi:10.7205/MILMED-D-13-00017
- Nazarov, A., Jetly, R., McNeely, H., Kiang, M., Lanius, R., & McKinnon, M. C. (2015). Role of morality in the experience of guilt and shame within the armed forces. Acta Psychiatrica Scandinavica, 132(1), 4–19. doi:10.1111/acps.12406
- Neria, Y., & Pickover, A. (2019). Commentary on the special issue on moral injury: Advances, gaps in literature, and future directions. Journal of Traumatic Stress, 32(3), 459–464. doi:10.1002/jts.22402
- Rizzo, A. S., & Shilling, R. (2017). Clinical virtual reality tools to advance the prevention, assessment, and treatment of PTSD. European Journal of Psychotraumatology, 8(Supp.5), Article 1414560. doi:10.1080/20008198.2017.1414560
- Schamborg, S., Tully, R. J., & Browne, K. D. (2016). The use of the State–Trait Anger Expression Inventory–II with forensic populations: A psychometric critique. International Journal of Offender Therapy and Comparative Criminology, 60(11), 1239–1256. doi:10.1177/0306624X15577932
- Schorr, Y., Stein, N. R., Maguen, S., Barnes, J. B., Bosch, J., & Litz, B. T. (2018). Sources of moral injury among war veterans: A qualitative evaluation. Journal of Clinical Psychology, 74(12), 2203–2218. doi:10.1002/jclp.22660
- Shay, J. (2014). Moral injury. Psychoanalytic Psychology, 31(2), 182. doi:10.1037/a0036090
- Sherman, N. (2015). Afterwar: Healing the moral wounds of our soldiers. Oxford: Oxford University Press.
- Smith, E. R., Duax, J. M., & Rauch, S. A. (2013). Perceived perpetration during traumatic events: Clinical suggestions from experts in prolonged exposure therapy. Cognitive and Behavioral Practice, 20(4), 461–470. doi:10.1016/j.cbpra.2012.12.002
- Steinmetz, S. E., Gray, M. J., & Clapp, J. D. (2019). Development and evaluation of the Perpetration‐Induced Distress Scale for measuring shame and guilt in civilian populations. Journal of Traumatic Stress, 32(3), 437–447. doi:10.1002/jts.22377
- Tangney, J. P., Miller, R. S., Flicker, L., & Barlow, D. H. (1996). Are shame, guilt and embarrassment distinct emotions? Journal of Personality and Social Psychology, 70(6), 1256–1269. doi:10.1037/0022-3514.70.6.1256
- Tangney, J. P., Wagner, P., & Gramzow, R. (1992). Proneness to shame, proneness to guilt, and psychopathology. Journal of Abnormal Psychology, 101(3), 469. doi:10.1037/0021-843X.101.3.469
- Vargas, F. A., Hanson, T., Kraus, D., Drescher, K., & Foy, D. (2013). Moral injury themes in combat veterans’ narrative responses from the National Vietnam Veterans’ Readjustment Study. Traumatology, 19(3), 243–250. doi:10.1177/1534765613476099
- Vermetten, E., & Jetly, R. (2018). A critical outlook on combat-related PTSD: Review and case reports of guilt and shame as drivers for moral injury. Military Behavioral Health, 6(2), 156–164. doi:10.1080/21635781.2018.1459973
- Worthington, E. L., Jr, & Langberg, D. (2012). Religious considerations and self-forgiveness in treating complex trauma and moral injury in present and former soldiers’. Journal of Psychology and Theology, 40(4), 274–288. doi:10.1177/009164711204000403