
ABSTRACT
Background:
The decade between the ages of 14 and 25 is a particularly vulnerable period for the development of mental health problems, especially of common mental disorders. Mental health and psychosocial prevention and support services for young people in the Republic of Georgia have been extremely limited, leaving a wide treatment and care gap. Club Synergy was designed as an innovative, pragmatic solution that is responsive to the needs of young people and incorporates all necessary levels of care required (prevention, early identification & intervention, and treatment) into a single, trauma-informed service that uses a transdiagnostic approach. This paper presents preliminary findings from the pilot phase of establishing and running the service.
Aim
To examine the characteristics of young people presenting to Club Synergy and the effectiveness of contact with the service.
Methods:
Quantitative evaluation of a consecutive series of young people seen by Club Synergy between November 2019 and July 2020. Demographic information was analysed using descriptive statistics. Pre–post outcomes for anxiety (GAD-7), depression (PHQ-9) and health-related quality of life (EQ-5D-5L) were analysed using the Wilcoxon signed-rank test.
Results:
Hundred and seventy-four young people were included. The majority (68.9%) self-referred, with referral from The Ministry of Justice due to conflict with law (23%) accounting for most of the other young people seen. Emotional disturbance (73.6%), anxiety (60.3%), problems in interpersonal relationships (57.5%) and low mood (49.4%) were the commonest presenting symptoms. Seventy-three per cent reported 4 or more adverse childhood experiences. After engaging in transdiagnostic modules, median baseline scores for depression and anxiety reduced by 40% and 45%, respectively, and self-rated health improved by 14%.
Conclusions:
Preliminary analysis indicates that Club Synergy’s trauma-informed model of care, based on a transdiagnostic approach, has the potential to provide an effective service to young people in Georgia at risk of developing and with mental health problems.
HIGHLIGHTS
This pragmatic study of a newly established mental health service for young people in Georgia suggests that a trauma-informed approach, using transdiagnostic modules, has the potential to effectively prevent and treat common mental health presentations.
Antecedentes:
La década comprendida entre los 14 y los 25 años es un período particularmente vulnerable para el desarrollo de problemas de salud mental, especialmente de trastornos mentales comunes. Los servicios de apoyo y prevención psicosocial y de salud mental para los jóvenes en la República de Georgia han sido extremadamente limitados, lo que ha dejado una gran brecha en el tratamiento y la atención. Club Synergy fue diseñado como una solución innovadora y pragmática que responde a las necesidades de los jóvenes e incorpora todos los niveles de atención necesarios (prevención, identificación e intervención tempranas, y tratamiento) en un solo servicio informado en trauma que utiliza una aproximación transdiagnóstica. Este estudio presenta los resultados preliminares de la fase piloto de establecimiento y funcionamiento del servicio.
Objetivo:
Examinar las características de los jóvenes que se presentan al Club Synergy y la efectividad del contacto con el servicio.
Métodos:
Evaluación cuantitativa de una serie consecutiva de observaciones en jóvenes atendidos por Club Synergy entre noviembre de 2019 y julio de 2020. La información demográfica se analizó mediante estadística descriptiva. Los resultados de ansiedad pre y post (GAD-7), depresión (PHQ-9) y calidad de vida relacionada con la salud (EQ-5D-5L) se analizaron mediante la prueba de rangos con signos de Wilcoxon.
Resultados:
Se incluyeron 174 jóvenes. La mayoría (68,9%) se autorrefirió, siendo la derivación por parte del Ministerio de Justicia por conflicto con la ley (23%) la que englobó a la mayoría de los otros jóvenes atendidos. Alteración emocional (73,6%), ansiedad (60,3%), problemas en las relaciones interpersonales (57,5%) y el estado de ánimo bajo (49,4%) fueron los síntomas más comúnmente presentados. El 73% informó 4 o más experiencias adversas en la infancia. Después de participar en módulos de transdiagnóstico, la media de las puntuaciones iniciales para la depresión y la ansiedad se redujo en un 40 y un 45%, respectivamente, y la salud autoevaluada mejoró en un 14%.
Conclusiones:
El análisis preliminar indica que el modelo de atención informado en trauma de Club Synergy, basado en una aproximación transdiagnóstica, tiene el potencial de brindar un servicio eficaz a los jóvenes en Georgia en riesgo de desarrollar y con problemas de salud mental.
背景:
14 岁至 25 岁之间的十年是心理健康问题,尤其是常见精神障碍发展的一个特别易感期。格鲁吉亚共和国为年轻人提供的心理健康和社会心理预防和支持服务极为有限,留下了巨大的治疗和护理缺口。 Club Synergy 旨在作为一种创新、务实的解决方案,响应年轻人需求,并将全部所需必要护理水平(预防、早期识别和干预以及治疗)整合到单一的使用跨诊断方法的创伤知情服务中。本文介绍了建立和运行该服务试点阶段的初步发现。
目的
考查 参与Club Synergy 年轻人的特征以及与服务联系的有效性。
方法
定量评估 Club Synergy 在 2019 年 11 月至 2020 年 7 月期间观察到的一系列年轻人。使用描述性统计分析人口信息。使用 Wilcoxon 符号秩检验分析焦虑 (GAD-7)、抑郁 (PHQ-9) 和健康相关生活质量 (EQ-5D-5L) 的事后结果。
结果
174 名年轻人被纳入研究。大多数 (68.9%) 自行转介,因触法而从司法部转介 (23%) 占所见其他年轻人的大部分。情绪障碍(73.6%)、焦虑(60.3%)、人际关系问题(57.5%)和情绪低落(49.4%)是最常见的症状。 73% 的人报告了 4 次或更多的不良童年经历。参与跨诊断模块后,抑郁和焦虑的中位基线分数分别降低了 40% 和 45%,自评健康状况提高了 14%。
结论
初步分析表明,基于跨诊断方法的Club Synergy 创伤知情护理模式,有可能为格鲁吉亚有发展风险和有心理健康问题的年轻人提供有效的服务。
1. Introduction
The decade between the ages of 14 and 25 is a particularly vulnerable period for the development of mental health (MH) problems. Most mental disorders have their origins in the teenage yearsFootnote1 and many have precursors in childhood. Half of all MH conditions start by 14 years of age, but most cases are undetected and untreated,Footnote2 and three-quarters of individuals with a mental disorder exhibit symptoms by the age of 24,Footnote3 The years 16–18 is a particularly critical period of vulnerability to mental illness, as well as a period of major physiological, emotional and social change for young people (YP).Footnote4 A systematic review of studies from low- and middle-income countries (LMICs) reported that experiencing MH problems during childhood or adolescence was linked to pre-mature death and serious dysfunction in adult lifeFootnote5; suicide is the second commonest cause of mortality in the 15–29 age group.Footnote6
Gustavson et al also concluded that common mental disorders are highly prevalent among young adults in their twenties, and somewhat less prevalent in their thirties/forties (see note 9). The 12-month prevalence of any mental disorder among people in their twenties was 19.8% (men) and 32.4% (women), with anxiety disorders the most prevalent followed by major depressive disorder in women and substance use disorder in men.Footnote7 A recent systematic review and meta-analyses found the global prevalence of common mental disorders (CMD) in adolescents (10–19 years old) to be 25.0% using a GHQ-12 cut-off of 4 and 31.0% using a GHQ-12 cut-off of 3.Footnote8
People of all ages with CMDs commonly do not receive mental health and psychosocial support (MHPSS) and the ‘treatment gap’ is especially wide in LMICs with estimates of only one in four receiving care,Footnote9 with particular concerns about children and young people.Footnote10 Morris et al. (Footnote2011) found that the median one-year treated prevalence for children and adolescents in LMICs was 159 per 100,000 population compared to 664 per 100,000 for adults. Children and adolescents made up 12% of the MH outpatient facility population and less than 6% in all other types of MH facility. Less than 1% of beds in inpatient facilities were reserved for children and adolescents. Training provided for MH professionals on child and adolescent mental health was minimal, with less than 1% receiving refresher training (Moris et al., Footnote2011).
1.1. Staging approach model
In LMICs, such as the Republic of Georgia, where general community-based services are scarce and primary care is ‘estranged’ from the MH field,Footnote11 pragmatic solutions that facilitate access to a wide age range of people with a wide range of difficulties are required. When considering possible approaches to addressing the large burden of mental ill-health in young people, a staging approach modelFootnote12 seems the most practical and applicable framework. The model calls for preventive interventions during non-specific mental distress and early identification and early interventions during subsyndromal and subthreshold conditions. When specific syndromes are manifested, the model suggests their management at primary healthcare, community and multisectoral levels; as for persistent and recurring syndromes and disorders, the response should be evidence-based treatment and rehabilitation interventions using collaborative approaches.
1.2. Trauma-informed care
Trauma-informed care represents the ‘new generation’ of transformed MH and allied services and programmes, that are informed about, and sensitive to, the potential for trauma-related issues to be present in clients, regardless of whether the issues are directly or obviously related to the presenting complaint or condition.Footnote13 Setbacks that a service could experience due to a lack of trauma-awareness include (1) failure to understand fully the presenting issues and their context; (2) failure to treat or have more appropriate (trauma-specific) referrals; (3) retraumatisation of clients with standard procedures or unintentional triggering events, which may slow progress, reduce openness to treatment or derail therapy altogether.Footnote14 A trauma-informed approach to MH care,Footnote15 perceives trauma not simply as a severe experience from the past, but as a formative one that may be causal to the client’s current condition.
Strong evidence supports significant and enduring associations between adverse childhood experiences (ACEs) and negative outcomes later in life.Footnote16 A trauma history is very common among people in contact with MH services. Fifty per cent of psychiatric outpatient case-notes documented a history of major trauma in one study,Footnote17 and 94% of poor inner-city youth using an urban outpatient MH clinic had experienced at least one lifetime trauma (most commonly physical attack, rape, or being threatened with a weapon). Forty-two per cent met the criteria for post-traumatic stress disorder (PTSD) in the last year.Footnote18
1.3. The transdiagnostic approach
The transdiagnostic (TD) approach to the prevention and management of MH problems is an emerging phenomenon. The TD approach is based on evidence that many different mental disorders share common vulnerabilities and symptoms,Footnote19 TD interventions aim to reduce and manage these common factors as opposed to treating specific disorders. A systematic review demonstrated that TD interventions were effective for anxiety and depression in adultsFootnote20 and other studies have provided evidence of efficacy with traumatised peopleFootnote21 and with people with addiction problems.Footnote22 Research has also shown that TD interventions can be effective for prevention of depression and anxiety.Footnote23 Implementation of TD interventions to youth populations is in its initial stages, though there is already evidence that TD therapies can be adaptedFootnote24 and work for children and adolescents with chronic pain comorbid with depression and anxiety.Footnote25 A recently published randomised clinical trialFootnote26 found a TD CBT programme to be superior to management as usual in youths with emotional and behavioural problems below the threshold for referral to MH care and TD approaches have been recommended for further evaluation with college-age students.Footnote27
1.4. The Georgian context
Georgia is struggling to reform its MH system.Footnote28 The underdevelopment of community care and lack of alternatives to hospital treatment leads to unnecessary psychiatric admissions,Footnote29 though there are only 10 in-patient beds for people up to 18 years old. In 2018, the number of officially registered persons with mental disorders was 76,508, of whom only 4% (3,217) were under 15Footnote30; young people represent a relatively larger proportion –14%.Footnote31 The main problems here are neurodevelopmental disorders (36,9%), while children and young people with behavioural and emotional problems represent 35,7%. ‘Registered patient’ figures are likely to grossly underestimate the true levels of MH disorder and needs in Georgia. Young people with behavioural and emotional problems do not receive adequate care at any level.
It is well recognised that substance misuse is widespread among young persons (YPs) in Georgia, causing severe mental and somatic consequences.Footnote32 Particularly high rates are also to be expected amongst the 6% of the Georgian population and their families who were internally displaced due to military conflicts in the 90s and 2008.Footnote33 Other groups identified as having significant MH needs in Georgia are the YP offending population (such as anger and impulse management, interpersonal communication, and social competences)Footnote34 and YP under state care. The Government managed to close 32 large children institutions between 2005 and 2013;under a robust de-institutionalisation programme, children were either reunited with their families, placed in a newly developed foster care system or at small group family-like homes, housing 8–10 children.Footnote35 Unpublished data indicated that around 80% of children and adolescents living in Small Family-like Houses, suffered from at least one mental disorder.Footnote36
Services in Georgia, including preventive programmes, for YP have been extremely limited, especially for dealing with common mental disorders and addiction problems. The government and policy makers in Georgia acknowledged the problems resulting from MH burden among YP and prepared a National Action Plan on MH Reform 2015–2020 that emphasised the needs of MH interventions development for YPs. This need is re-stated again in the National Strategic Plan for 2022–2030 that puts child and adolescent mental health as one of the country’s priorities.
1.5. Club Synergy
Club Synergy was designed as an innovative, pragmatic solution that is responsive to the needs of YP in Georgia and incorporates all necessary levels of care required (prevention, early identification & intervention, and treatment) into a single service. It is also the first service in Georgia to provide trauma-informed care using a TD approach. Plans were conceived locally, involving clinicians, child rights advocates, policy makers and YP who were engaged in MHPSS with initiators of the service, including co-authors of this paper, and then developed with the support of national and international colleagues, mostly clinical academics from Germany and UK. It was agreed that the Club Synergy model should be based on the evidence available with respect to trauma-informed care and the transdiagnostic approach. Regular meetings were held between stakeholders and iterations of the proposal were consulted on before it was finalised.
Effective communication was agreed to be very important with the choice of an appropriate name being a key early task in this regard. Club Synergy was chosen with consultations of potential service users as an attractive, non-stigmatising name that would attract YP to present to the service, removing a possible barrier to access and engagement. Club Synergy also emphasises the collaborative and integrative approach of the service with a culture of co-production with a range of stakeholders, including Synergy teams and YP service users, but also representatives of partner organisations, e.g. Crime Prevention Centre of Georgia.
Synergy opened in April 2019, with Clubs located in the two main cities of Georgia: Tbilisi (population 1,114,000) and Batumi (population 155,000), offering support for YP experiencing emotional and behavioural problems, including addiction problems (See Box 1). Both Clubs have capacity to serve around 600 YP per year. To facilitate access and engagement, the Clubs are open from 2pm to 7pm (after school hours) on weekdays and Saturdays. Club Synergy is an inclusive, free to access, preventive-intervention psychosocial service, that offers support to YP aged 14–25 with MH problems, however they manifest. The service caters for people with sub-diagnostic threshold MH problems, people in high risk-groups (e.g. with offending behaviour for secondary prevention) and people with manifest mental disorders. Club Synergy is available to all YP, but also supports specific target groups, including YP in conflict with the law; IDPs and war-affected YP; and their family members/carers. Club Synergy is managed by the NGO GIP-Tbilisi.
Box 1: Club Synergy Service: Indications for Referral.
The Club Synergy staff were selected to allow a multidisciplinary approach to service delivery. The specialists who work in the service are addictologists and psychologists trained in delivering MHPSS social workers, a doctor somatologist and psychiatrists. In preparation for the launch of Club Synergy, almost 18 months of training was provided to staff by local experts, addictologists from Hamburg University (Germany) and experts in CYP MH and traumatic stress from Cardiff University (UK).Footnote37 The external supervisors – experienced, trained and certified MH specialists from GIP-Tbilisi – were assigned to both Clubs and weekly case and team supervision was established.1.6. Operating procedure
A common operating procedure has been adopted across both Clubs, comprising a case management system and essential documentation, including a code of conduct, ethical procedures, and informed consent forms (for the first time in Georgia).
Awareness raising of Club Synergy and what it can offer was undertaken by preparing and publishing adverts, fliers and booklets and distributing them to relevant agencies and stakeholders. The majority of YP self-refer, whilst others are referred by various agencies, including the Crime Prevention Centre and the Probation Agency of Georgia (at the Ministry of Justice), the Social Agency of Georgia (at the Ministry of IDPs, Labor, Health and Social Care), and Psychological Centres (funded by the Ministry of Education) ().
Figure 1. Club Synergy Pathway for YP.
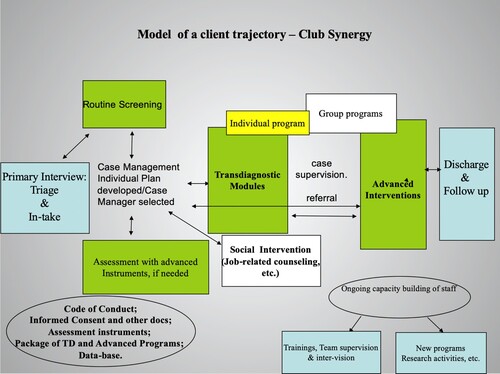
The Clubs offer a range of interventions developed specifically for Club Synergy, including individual counselling, family and parental/carers’ counselling, individual and group modules (See supplementary material). The model of care assumes that early detection of problems and timely intervention can prevent development of more severe conditions and/or alleviate, reduce or even stop symptoms from further evolving. Following assessment, intervention involves the delivery of basic TD modules and, if indicated, advanced, focused modules.
The interventions offered include existing evidence-based interventions that have been adapted for use in Georgia, e.g. cognitive behavioural therapy with a trauma focus for PTSD,Footnote38 and specifically developed transdiagnostic interventions based on the evidence available for these, e.g. emotional regulation.Footnote39 The local mental health professionals involved in the development of Club Synergy agreed and developed the modules that would be used, in consultation with international colleagues. More detailed information on the Club Synergy interventions and the evidence that supports their use can be found the supplementary material.
There are 7 TD modules that address skills building, resource activation and resilience building so that YP feel better able to deal with common specific problems. The modules have been personalised for two 2 age groups of 14–17 and 18–25 years.
The advanced, focused modules are based on cognitive–behavioural therapy (CBT) approaches and include interventions for PTSD, addiction, and gambling.
The client is usually offered one or more TD modules after an initial assessment interview and may then transition to the advanced module(s), if needed. There are cases when the TD and advanced modules are started in parallel. The decision is made by the transdiagnostic team, led by a case manager, who invites appropriate specialists to be part of the case management process that considers the relevance of the modules to the needs of the YP.
The modules were made up of multiple sessions and designed so that they could be delivered both individually and in a group format. Therapists were able to use their clinical judgement to combine modules rather than focusing on one at a time. The sessions were designed to last 45 min and included instruction in skills and between-session practice assignments.
2. Aim
To examine the characteristics of young people presenting to Club Synergy and the effectiveness of contact with the service.
3. Methods
Quantitative evaluation of a consecutive series of young people seen by Club Synergy between November 2019 and July 2020. Demographic information was analysed using descriptive statistics. Pre–post outcomes for anxiety (GAD-7), depression (PHQ-9) and health-related quality of life (EQ-5D-5L) were analysed using the Wilcoxon signed rank test.
This paper presents preliminary findings only; full evaluation of the service effectiveness (using both quantitative and qualitative analysis of gathered data) will be available in 2022/23.
3.1. Outcome/Screening Measures
Box 2 lists the core and optional measures adopted by Club Synergy. These have all been shown to be valid and reliable instruments in various contexts and, with the exception of the WHO ACEs, are completed as part of the intake assessment (pre-test), on completion of intervention(s) (post-test) and during a follow up session at 3 months. The WHO ACEs are completed at the third or fourth session of contact to reduce the risk of revictimisation and increased patient stigma.Footnote40
All data collected from 1 November 2019 have been analysed as part of a study looking at the clinical effectiveness of Club Synergy, whether YP benefit from the service provided and, if so, whether this is sustained. In addition, factors associated with outcome have also been studied.
Box 2: Club Synergy Outcome/Screening Measures
*Introduced February 2020.Since April 2020, due to the COVID-19 pandemic, the service has been working online, offering clients remote counselling via video platforms such as Zoom and Skype, with greater reliance on mobile phones, texts, and e-mails to provide support and deliver services. The development of a website to provide self-help tools to YP was also initiated.
4. Results
describes the demographic characteristics and data on source of referral of the 174 young persons, aged 14–25, who accessed the service between 1 November 2019 and 31 July 2020.
Table 1. Sample characteristics (N = 174).
The majority of clients self-referred (67.8%) with the Probation Agency making the most referrals (23%). There were almost twice as many females (61.5%) as males (38.5%). 36.2% were aged 18–21, 34.5% 14–17 and 29.3% 22–25.
provides data on the complaints and problems of YP presented with at initial assessment. The information was collected through standard clinical interviews and, in the case of YP in conflict with law, additional information was provided by a social worker. The symptoms/difficulties had to be felt to be significant and impacting the YP to be included.
Table 2. Symptoms/difficulties experienced on enrolment in the service (N = 174).
Some differences between females and males can be seen; more females reported symptoms of anxiety, low mood, sleep disturbances, loneliness, self-esteem problems, psychosomatic distress and suicidal ideation, while more male young people reported problems with aggression and addiction behaviours.
Ninety-six (55%) clients completed the ACE-IQ questionnaire. Other clients were not asked to complete the questionnaire as it was only introduced in February 2020, refused to complete it or did not complete it correctly.
shows the overall mean scores along with those for the 25th, 50th and 75th percentiles. It also shows the frequency of exposure during the childhood to different adverse experiences.
Table 3. Results of the ACE questionnaire (N = 96).
The binary data shows the number of childhood experiences across several domains: family dysfunction; physical, sexual and emotional abuse and neglect by parents or caregivers; peer violence; witnessing community violence, and exposure to collective violence. The frequency score refers to how frequent was the particular event happening to a person – ‘many times’, ‘a few times’, ‘once’ or ‘never’.
The number and frequency of adverse childhood experiences is shown the .
Table 4. Number of ACEs in the Synergy clients (N = 96).
The ACEs data demonstrates high exposure to childhood traumatic experiences –10.4% had experienced 3 ACEs (with frequency of 5.21%) and 72.92% were exposed to 4 and more (with frequency of 40.63%).
The most commonly used individual treatment modules were Emotional Regulation (61.5% of clients received this over a mean number of 6.1 sessions) and Effective Communication and Interpersonal Relationship Skills (30.5% of clients received this over a mean number of 4.2 sessions). The Raising Awareness of Committed Crime module was received by 10.3% of clients over a mean number of 2.6 sessions, and the Brief Addiction module by 5.2% of clients over a mean number of 2.9 sessions. The Short Multicomponent Programme was the least employed module and received by 2.9% of clients. The Positive Parenting module was received by nine parents over a mean of 1.8 visits. The most utilised group interventions were Art-Therapy (14 groups with a mean of 3.1 sessions) and Emotional Regulation (4 groups with a mean of 5.3 sessions). As for advanced individual modules, CBT-TF was used with 4% of clients with a mean of 8.6. sessions.
provides data comparing baseline and post-intervention scores on the main outcome measures for those YP who completed both assessments. 15.5% of clients remained in the service but did not complete post-intervention questionnaires and 13.8% dropped out from the service and did not complete post-intervention questionnaires. The missing data for clients who engaged with the service is likely associated with the fact that questionnaires were sent to clients after they were discharged, as opposed to being completed at the end of their final session with the service. It was also clear that some clients were not motivated to complete questionnaires, and it was agreed that after three reminders, it would be accepted that the data would not be returned. Younger and male clients were more likely not provide outcome data but the source of referral (self-referral or referral due to conflict with the law) was not associated with not providing outcome data.
Table 5. Comparison of Pre-Post testing of key outcome measures (Median of the difference between pre- and post-tests).
As can be seen, statistically significant improvements were found for all outcome measures with clear reductions in anxiety and depressive symptoms and improvements in health-related quality of life and functioning. Analysis of data from clients who received input from Club Synergy in person, on-line or a few a mixture of both showed no difference in outcomes on the PHQ9, EQ-5D-5L and GAD-7.
5. Discussion
Club Synergy was developed in Georgia to address major unmet mental health needs in YP. Preliminary findings suggest that the trauma-informed, TD psychosocial prevention-intervention service provided by Club Synergy improved the health and wellbeing of YP presenting with a range of MH difficulties who engaged with it. If these findings are confirmed by the full study evaluation, the Club Synergy model has the potential to be expanded and implemented elsewhere in Georgia and beyond, to help to address the major ‘treatment gap’ for people with MH problems, especially for YP in LMICs.
Flaherty et al.Footnote48 documented a graded relationship between adverse childhood exposures and MH problems. Exposure rates rise in risk-group YP due to several disadvantage factors, such as poverty, family and community violence, being orphaned and being in conflict with law.Footnote49 Consequently, we expected high rates of exposure in YP accessing Club Synergy and this was the case. Almost three quarters (73%) reported exposure to 4 or more ACES. Direct comparisons to general population in Georgia are not possible as such data do not exist among for the general population. However, it is significantly higher than general population studies of university students in Turkey,Footnote50 or young adultsFootnote51 and adults of all ages in China.Footnote52 Our data clearly suggests that YP presenting to Club Synergy had been exposed to significant trauma, were at very high risk of developing mental disorder and an appropriate group to attempt to reduce the impact of ACEs in through the provision of preventive interventions (Folk et al., 2020).
The prevalence of ACEs and overall Club Synergy experience underlines the importance of adopting a trauma-informed approach; the staff of Club Synergy tailored interventions to take into account the adverse experiences of the YP, recognising that the transition from adolescence to young adulthood is already a period of great change for individuals and families/carers. The range of relevant TD modules, including emotional regulation, psychoeducation and emotional disbalance management, were generally delivered over more sessions to YP with more ACEs.
Limited consensus exists on what constitute the optimal active ingredients for prevention, though, those aspects of an intervention that drive clinical effect, are conceptually well defined.Footnote53 The TD approach, combining common elements of cognitive–behavioural therapy-based treatment for multiple and comorbid mental health problems, was well received by YP and staff within Club Synergy. It appears well suited to the Club Synergy population and has been applied to numerous settings in low- and middle-income countriesFootnote54 and proved successful.Footnote55
We consider a particular strength of the Club Synergy model to be the development and personalisation of TD modules according to our experiences with YP, assessing their and their carers needs and problems, promoting the development of emotional and social skills and competences, while at the same time reducing disruptive behaviours and mental health symptoms and improving personal well-being.
The wide range of different MH presentations, and overlap in them, and the positive outcomes for YP who completed pre–post measures of depression, anxiety and health-related quality of life supports the decision to adopt a TD approach. Our results demonstrated a 40% reduction in median baseline scores for depression, a 45% reduction for anxiety and 100% and 50% improvements of reported functional impairment/impact for depression and anxiety respectively. A 14% improvement in YP self-rated health was also observed.
The findings are consistent with other studies of TD interventions, which have found positive effects for anxiety, depression, trauma, and addiction problems in adults (see notes 27–29,64), and the emerging evidence for TD interventions in YP with anxiety, depression, and behavioural difficulties (see notes 32–33).
It is difficult to determine the exact reasons why Club Synergy appears to have been successful, but several factors are likely to have contributed to this. It is well documented that help seeking is hindered by both personal and public stigmaFootnote56 and, therefore, the community-based set up of the Club Synergy service with a youth-friendly name, free-of-charge delivery, family friendly atmosphere is likely to have decreased key barriers to the access of care by YP not least by lessening the ‘psychological distance’ between the service and YP. Other key factors are likely to include the multidisciplinary nature of the service and personalised, transdiagnostic approach to the identification of needs and delivery of appropriate prevention and/or treatment interventions.
There are several strengths to this work, including the fact it represents an evaluation of a newly developed service (the first of its kind in Georgia), that was adapted during a global pandemic (e.g. through the use of remote delivery and blended approaches). The project is also an example of a collaborative approach between an international group of clinical researchers.
6. Limitations
A key limitation is that data was only available for a proportion of those presenting to Club Synergy and pre-post measures were available for a lesser proportion, not least because not all participants had completed their intervention(s) at the time the dataset was analysed. It should also be noted that our conclusions are based on a limited number of clinical outcomes without longer term follow-up. These issues should result in caution when interpreting the results, but it is important to remember that this is a preliminary analysis and quantitative and qualitative data collection is ongoing with further evaluation of the Club Synergy model and analyses planned for the future.
6.1. Clinical and Research implications
More than 40% of the world population is 24 years old or younger, the vast majority of whom live in low- and lower middle–income countries.Footnote57 Globally, a quarter of disability-adjusted life years (DALYs) for mental disorders and substance abuse is borne by this age group, and about 75% of mental disorders diagnosed in adulthood have their onset before the age of 24 years.Footnote58 There is growing evidence and awareness regarding the magnitude of mental health issues across the globe, these start in half of those affected before the age of 14 and have lifelong effects on individuals and society.Footnote59 Most children and young people in developing countries do not have access to mental health care. The disparities between need, demand and access to youth mental healthcare are very high in low and- middle-income countries (LMICs), where scarcity of available resources for youth mental healthcare represents a major obstacle to decreasing the impact of mental disorders across the lifespan.Footnote60 To address the mental health care services’ GAP in YP healthcare in LMICs, the balancing of comprehensive tertiary care (for a minority) with other forms of services to serve the majority is recommended.Footnote61
There is an urgent need to establish effective community-based services that offer a broad range of preventive and treatment modules to YP with emotional and behavioural problems and proof of concept has now been established for the Club Synergy service model. The pilot service was implemented through donor funding (European Comission), as is usual practice in LMICs,Footnote62 and is not yet part of the state system.
The main clinical implications are that the TD, trauma-informed model of care adopted by Club Synergy has the potential to: (1) provide an accessible service to YP in Georgia at risk of developing and with MH problems; and (2) provide interventions that have a positive impact on the health and wellbeing of YP who engage with them.
We have been collecting data using qualitative methods and this preliminary analysis of the effectiveness of the Club Synergy model will be followed by the publication of more detailed quantitative and qualitative evaluation, including consideration of health economic aspects of the service.
Supplemental Material
Download MS Word (37.6 KB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
Data can be made available upon request to the corresponding author.
Additional information
Funding
Notes
1 Jones, P. B. (2013). Adult mental health disorders and their age of onset. British Journal of Psychiatry, 202(Suppl 54), s5–s10.
2 Kessler, R. C., Angermeyer, M., Anthony, J. C., et al. (2007). Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry, 6, 168–176.
3 Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593–602. doi:10.1001/archpsyc.62.6.593. [Erratum in: Arch Gen Psychiatry. 2005 Jul;62(7):768. Merikangas, Kathleen R [added]. PMID: 15939837]. McGorry, P. (2007). The specialist youth mental health model: Strengthening the weakest link in the public mental health system. Medical Journal of Australia, 187(Suppl), S53–S56.
4 Jones, P. B. (2013). Adult mental health disorders and their age of onset. British Journal of Psychiatry, 202(Suppl 54), s5–s10.
5 Klasen, H., & Crombag, A. C. (2013). What works where? A systematic review of child and adolescent mental health interventions for low- and middle-income countries. Social Psychiatry and Psychiatric Epidemiology, 48(4), 595–611. doi:10.1007/s00127-012-0566-x. Epub 2012 Sep 9. PMID: 22961287.
7 Gustavson, K., Knudsen, A. K., Nesvåg, R., et al. (2018). Prevalence and stability of mental disorders among young adults: findings from a longitudinal study. BMC Psychiatry, 18(65). doi:10.1186/s12888-018-1647-5
8 Silva, S. A., Silva, S. U., Ronca, D. B., Gonçalves, V. S. S., Dutra, E. S., & Carvalho, K. M. B. (2020). Common mental disorders prevalence in adolescents: A systematic review and meta-analyses. PLoS ONE, 15(4), e0232007. doi:10.1371/journal.pone.0232007.
9 Alonso, J., Liu, Z., Evans-Lacko, S., Sadikova, E., Sampson, N., Chatterji, S., … WHO World Mental Health Survey Collaborators (2018). Treatment gap for anxiety disorders is global: Results of the World Mental Health Surveys in 21 countries. Depress Anxiety, 35(3), 195–208. doi:10.1002/da.22711. Epub 2018 Jan 22. PMID: 29356216; PMCID: PMC6008788. Araya, R., Zitko, P., Markkula, N., Rai, D., & Jones, K. (2018). Determinants of access to health care for depression in 49 countries: A multilevel analysis. Journal of Affective Disorders, 234, 80–88. doi:10.1016/j.jad.2018.02.092. Chisholm, D., Sweeny, K., Sheehan, P., Rasmussen, B., Smit, F., Cuijpers, P., & Saxena, S. (2016). Scaling-up treatment of depression and anxiety: A global return on investment analysis. Lancet Psychiatry, 3, 415–424. doi:10.1016/S2215-0366(16)30024-4. De Silva, M. J., Lee, L., Fuhr, D. C., Rathod, S., Chisholm, D., Schellenberg, J., & Patel, V. Estimating the coverage of mental health programmes: A systematic review. International Journal of Epidemiology, 43(2), 341–353. doi:10.1093/ije/dyt191.
10 Morris, J., et al. (2011). Treated prevalence of and mental health services received by children and adolescents in 42 low-and-middle-income countries. The Journal of Child Psychology and Psychiatry. doi:10.1111/j.1469-7610.2011.02409.x
11 Global Initiative on Psychiatry-Tbilisi. (2021). The policy recommendations on mental health reform. Tbilisi.
12 Patel, V., et al. (2018). The Lancet Commission on global mental health and sustainable development. The Lancet, 392, 10157. doi:10.1016/S0140-6736(18)31612-X
13 SAMHSA. (2014). Trauma-informed care in behavioral health services. Treatment Improvement Protocol (TIP) Series 57. HHS Publication No. (SMA) 13-4801. Rockville, MD: Substance Abuse and Mental Health Services Administration.
14 Butler, L., Filomena, D., Critell, M., & Rinfrette, E. S. (2011). Trauma-informed care and mental health. Directions in Psychiatry, 31, 197–210.
15 Harris, M., Fallot, R. D. (Eds.). (2001). Using trauma theory to design service (pp. 3–22). San Francisco, CA: Jossey-Bass. Jennings, A. (2008). Models for developing trauma informed behavioral health systems and trauma specific services: 2008 update. Abt Associates Inc. National Association of State Mental Health Program Directors and the National Center for Trauma Informed Care. Retrieved May 22, 2021, from https://www.theannainstitute.org/MDT2.pdf.
16 Felitti, V. J., Anda, R. F., Nordenberg, D., Williamson, D. F., Spitz, A. M., Edwards, V., & Marks, J. S. (1998). The relationship of adult health status to childhood abuse & household dysfunction. American Journal of Preventive Medicine, 14, 245–258. Meade, C. S., Kershaw, T. S., Hansen, N. B., & Sikkema, K. J. (2009). Long-term correlates of childhood abuse among adults with severe mental illness: Adult victimization, substance abuse, and HIV sexual risk behavior. AIDS and Behavior, 13(2), 207–216.
17 Posner, J., Eilenberg, J., Friedman, J. H., & Fullilove, M. J. (2008). Quality and use of trauma histories obtained from psychiatric outpatients: A ten-year follow-up. Psychiatric Services, 59(3), 318–321.
18 Switzer, G. E., Dew, M. A., Thompson, K., Goycoolea, J. M., Derricott, T., & Mullins, S. D. (1999). Posttraumatic stress disorder and service utilization among urban mental health center clients. Journal of Traumatic Stress, 12(1), 25–39.
19 Barlow, D. H., Sauer-Zavala, S., Carl, J. R., Bullis, J. R., & Ellard, K. K. (2014). The nature, diagnosis, and treatment of neuroticism: back to the future. Clinical Psychological Science, 2(3), 344–365. doi:10.1177/2167702613505532. Moses, E. B., & Barlow, D. H. (2006). A New unified treatment approach for emotional disorders based on emotion science. Current Directions in Psychological Science, 15(3), 146–150. doi:10.2307/20183098.
20 Newby, J. M., McKinnon, A., Kuyken, W., Gilbody, S., & Dalgleish, T. (2015). Systematic review and meta-analysis of transdiagnostic psychological treatments for anxiety and depressive disorders in adulthood. Clinical Psychology Review, 40, 91–110. doi:10.1016/j.cpr.2015.06.002.
21 Gutner, C. A., Galovski, T., Bovin, M. J., & Schnurr, P. P. (2016). Emergence of transdiagnostic treatments for PTSD and posttraumatic distress. Current Psychiatry Reports, 8(10), 95. doi:10.1007/s11920-016-0734-x.
22 Kim, H. S., & Hodgins, D. C. (2018). Component model of addiction treatment: A pragmatic transdiagnostic treatment model of behavioral and substance addictions. Frontiers in Psychiatry, 9, 406. doi:10.3389/fpsyt.2018.00406.
23 Dozois, D. J. A., Seeds, P. M., & Collins, K. A. (2009). Transdiagnostic approaches to the prevention of depression and anxiety. Journal of Cognitive Psychotherapy, 23(1), 44–59. doi:10.1891/0889-8391.23.1.44.
24 Chu, B. C. (2012). Translating transdiagnostic approaches to children and adolescents. Cognitive and Behavioral Practice, 19(1), 1–4. doi:10.1016/j.cbpra.2011.06.003.
25 Allen, L. B., Tsao, J. C. I., Seidman, L. C., Ehrenreich-May, J., & Zeltzer, L. K. (2012). A unified, transdiagnostic treatment for adolescents with chronic pain and comorbid anxiety and depression. Cognitive and Behavioral Practice, 19(1), 56–67. doi:10.1016/j.cbpra.2011.04.007.
26 Jeppesen, P., et al. (2020). Effectiveness of transdiagnostic cognitive-behavioral psychotherapy compared with management as usual for youth with common mental health problems - a randomized clinical trial. JAMA Psychiatry. doi:10.1001/jamapsychiatry.
27 Auerbach, R. P., et al. (2019). Mental disorder comorbidity and suicidal thoughts and behaviors in the World Health Organization World Mental Health Surveys International College Student initiative. International Journal of Methods in Psychiatric Research, 28(2), e1752.
28 Makhashvili, N., & van Voren, R. (2013). Balancing community and hospital care: A case study of reforming mental health services in Georgia. PLoS Med, 10(1), e1001366. doi:10.1371/journal.pmed.1001366. http://www.plosmedicine.org/article/info%3Adoi%2F10.1371%2Fjournal.pmed.1001366.
29 Winkler, P., et al. (2017). A blind spot on the global mental health map: a scoping review of 25 years’ development of mental health care for people with severe mental illnesses in central and eastern Europe. The Lancet Psychiatry. doi:10.1016/S2215-0366(17)30135-9. PMID: 28495549.
30 National Center for Disease Control and Public Health. (2019). Statistical yearbook.
31 National Statistics Office. (2020, January). Georgia.
32 Beselia, A., Gegenava, V., Kirtadze, I., Mgebrishvili, T., Otiashvili, D., Razmadze, M., … Javakhishvili, J. (2019). The drug situation in Georgia 2018. Tbilisi, Georgia. https://altgeorgia.ge/media/uploads/drug-situation-in-georgia-2018-summary.pdf. Otiashvili, D., Tabatadze, M., Balanchivadze, N., & Kirtadze, I. (2016). Policing, massive street drug testing and poly-substance use chaos in Georgia – a policy case study. Substance Abuse Treatment. Prevention, and Policy, 11(1), 1–12. doi:10.1186/s13011-016-0049-2.
33 Makhashvili, N., Chikovani, I., McKee, M., Bisson, J., Patel, V., & Roberts, B. (2014). Mental disorders and their association with disability among internally displaced persons and returnees in Georgia. Journal of Traumatic Stress, 27(5), 509–518. doi:10.1002/jts.21949. MCID: PMC4496794.
34 GCRT. (2020). Juvenile crime prevention (Research Report). GCRT. Tbilisi.
35 Greenberg, A. L., & Partskaladze, N. (2014). How the Republic of Georgia has nearly eliminated the use of institutional care for children. Infant Mental Health Journal, 35(2). doi:10.1002/imhj.21434.
36 GIP-Tbilisi. (2012). Mental health needs of children and adolescents residing at small family-like houses across Georgia.
37 The Club was established by Foundation Global Initiative on Psychiatry-Tbilisi and supported financially by EC and OSGF.
38 Bisson, J., Makhashvili, N., Javakhishvili, J., & Cloitre, M. (2017, November 8). Developing and delivering a train the trainer programme to implement evidence based practice in low- and middle-income countries. A workshop presented as a pre-meeting institutes at 33rd annual meeting of ISTSS. “Trauma and Complexity: From Self to Cells” in Chicago, Illinois, USA. https://istss.org/am20/daily-schedule#Nov%2012.
39 Larson, R. W., Moneta, G., Richards, M. H., & Wilson, S. (2002). Continuity, stability, and change in daily emotional experience across adolescence. Child Development, 73(4), 1151–1165. doi:10.1111/1467-8624.00464. PMID: 12146740.
40 Racine, N., Killam, T., & Madigan, S. (2020). Trauma-informed care as a universal precaution: Beyond the adverse childhood experiences questionnaire. JAMA Pediatrics, 174(1), 5–6. doi:10.1001/jamapediatrics.2019.3866
41 Kroenke, K., Spitzer, R. L., & Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613.
42 Spitzer, R. L., Kroenke, K., Williams, J. B., & Lowe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097.
43 Emrani, Z., Akbari Sari, A., Zeraati, H., et al. (2020). Health-related quality of life measured using the EQ-5D–5 L: population norms for the capital of Iran. Health Qual Life Outcomes, 18, 108. doi:10.1186/s12955-020-01365-5.
44 World Health Organization. (2018). Adverse Childhood Experiences International Questionnaire (ACE-IQ). Geneva: WHO.
45 Cloitre, M., Shevlin, M., Brewin, C. R., Bisson, J. I., Roberts, N. P., Maercker, A., … Hyland, P. (in press). The International Trauma Questionnaire: Development of a self-report measure of ICD-11 PTSD and Complex PTSD. Acta Psychiatrica Scandinavica. doi: 10.1111/acps.12956.
46 WHO. (2010). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): manual for use in primary care. Prepared by R. Humeniuk, et al. Geneva: Author.
47 Johnson, E. E., Hamer, R. M., & Nora, R. M. (1998). The Lie/Bet Questionnaire for screening pathological gamblers: A follow-up study. Psychological Reports, 83(3_suppl), 1219–1224. doi:10.2466/pr0.1998.83.3f.1219.
48 Flaherty, E. G., Thompson, R., Dubowitz, H., Harvey, E. M., English, D. J., Proctor, L. J., & Runyan, D. K. (2013). Adverse childhood experiences and child health in early adolescence. JAMA Pediatrics, 167(7), 622–629. doi:10.1001/jamapediatrics.2013.22.
49 Ali, S., Yildirim, M., Hussain, S., & Vostanis, P. (2020). Self-reported mental health problems and post traumatic stress growth among children in Pakistan care homes. Asia Pacific Journal of Social Work and Development, 30, 62–76. Folk, J. B., Kemp, K., et al. (2020). Adverse childhood experiences among justice-involved youth: data-driven recommendations for action using the sequential intercept model. https://escholarship.org/content/qt98g4m26v/qt98g4m26v_noSplash_09e1434b5fdb165d64f5c541dd3bd370.pdf.
50 WHO Europe. (2013). Adverse chidlhood experiences survey among university students in Turkey (Study Report 2013). WHO. Regional office for Europe. Retrieved May 22 2021 from https://www.euro.who.int/__data/assets/pdf_file/0010/267472/Adverse-childhood-experiences-survey-among-university-students-in-Turkey-Eng.pdf.
51 Ho, G. W. K., Chan, A. C. Y., Chien, W.-T., Bressington, D. T., & Karatzias, T. (2019). Examining patterns of adversity in Chinese young adults using the Adverse Childhood Experiences—International Questionnaire (ACE-IQ). Child Abuse & Neglect, 88, 179–188. doi:10.1016/j.chiabu.2018.11.009. ISSN 0145-2134.
52 Chang, X., Jiang, X., Mkandarwire, T., & Shen, M. (2019). Associations between adverse childhood experiences and health outcomes in adults aged 18–59 years. PLoS ONE, 14(2), e0211850. doi:10.1371/journal.pone.0211850.
53 Wolpert, M., Pote, I., & Sebastian, C. L. (2021). Identifying and integrating active ingredients for mental health. The Lancet Psychiatry. doi:10.1016/S2215-0366(21)00283-2.
54 Murray, L. K., Dorsey, S., Haroz, E., Lee, C., Alsiary, M. M., Haydary, A., … Bolton, P. (2014a). A common elements treatment approach for adult mental health problems in low- and middle-income countries. Cognitive and Behavioral Practice, 21, 111–123.
55 Bogdanov, S., et al. (2021). A randomized-controlled trial of community- based transdiagnostic psychotherapy for veterans and internally displaced persons in Ukraine. Global Mental Health, 8, e32. doi:10.1017/gmh.2021.27.
56 Schnyder, N., Panczak, R., Groth, N., & Schultze-Lutter, F. (2017). Association between mental health-related stigma and active help-seeking: Systematic review and meta-analysis. The British Journal of Psychiatry, 210(4), 261–268.
57 Global Burden of Disease Collaborative Network. (2016). Global Burden of Disease Study 2016 (GBD 2016) Results. Seattle, WA: Institute for Health Metrics and Evaluation (IHME) 2017. http://ghdx.healthdata.org/gbd-results-tool
58 Kessler, R. C., Angermeyer, M., Anthony, J. C., et al. (2007). Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry, 6, 168–176.
59 Polanczyk, G. V., Salum, G. A., Sugaya, L. S., Caye, A., & Rohde, L. A. (2015). Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. Journal of Child Psychology and Psychiatry, 56(3), 345–365. Rocío, G.-C., Beatriz, V.-C., & Lourdes, V.-G. (2019). Children and adolescents mental health: A systematic review of interaction-based interventions in schools and communities. Frontiers in Psychology, 10, 918. doi:10.3389/fpsyg.2019.00918. https://www.frontiersin.org/article/10.3389/fpsyg.2019.00918.
60 Rocha, T. B., Graeff-Martins, A. S., Kieling, C., & Rohde, L. A. (2015). Provision of mental healthcare for children and adolescents: a worldwide view. Current Opinion in Psychiatry, 28(4), 330–335. doi:10.1097/YCO.0000000000000169. PMID: 26001925
61 Dutsadee Juengsiragulwit. (2015). Opportunities and obstacles in child and adolescent mental health services in low- and middle-income countries: A review of the literature. WHO South-East Asia Journal of Public Health, 4(2), 110–122. World Health Organization. Regional Office for South-East Asia. https://apps.who.int/iris/handle/10665/329695.
62 Lu, C., Li, Z., & Patel, V. (2018). Global child and adolescent mental health: The orphan of development assistance for health. PLoS Medicine, 15(3), e1002524. doi:10.1371/journal.pmed.1002524. PMID: 29522518; PMCID: PMC5844520.