
ABSTRACT
Aspirin remains one of the most common agents involved in both accidental and intentional overdose. The availability of enhanced elimination and early hemodialysis has been known to reduce the number of deaths from salicylate poisoning. We present the case of an intentional aspirin overdose with enteric-coated preparation that had continuously rising salicylate levels despite treatment with bicarbonate drip, continuous dialysis and activated charcoal.
1. Case description
A 22-year-old female with a past medical history significant for depression and suicide presented with intentional salicylate overdose. She reported ingesting 500 enteric-coated tablets of 325mg aspirin approximately 5 hours prior to presentation. She complained of epigastric discomfort and nausea. At presentation, she was afebrile, heart rate of 113 beats per minute, blood pressure 130/81 mmHg, respiratory rate 20 breaths per minute and with oxygen saturation of 100% on room air. Glasgow Coma Scale score was 12; rest of the physical examination was normal. Initial blood tests revealed a salicylate level of 97.5 mg/dL (reference range <30 mg/dl), compensated metabolic acidosis and normal renal function. Electrocardiogram revealed sinus tachycardia with normal QRS and QT intervals. Chest radiogram showed no acute cardiopulmonary process.
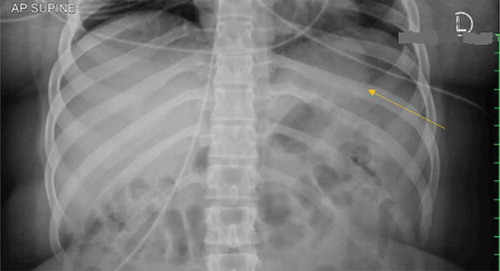
Urine alkalinization was started with a bolus of 100ml of 8.4% sodium bicarbonate solution intravenously followed by an infusion of sodium bicarbonate in D5W. Emergent hemodialysis was also initiated and continued for close to 30 hours because of persistently elevated salicylate levels. She also received 50g of activated charcoal. Despite the mentioned regimen, salicylate levels remained elevated at 52.4mg/dL. An abdominal radiogram was performed 12 hours after admission due to persistently elevated salicylate levels (). This revealed a radiopaque density in the stomach fundus, which raised concerns for an aspirin pharmacobezoar.
Figure 1. Density in the stomach fundus, suspicious for an aspirin bezoar (pointed by arrow).
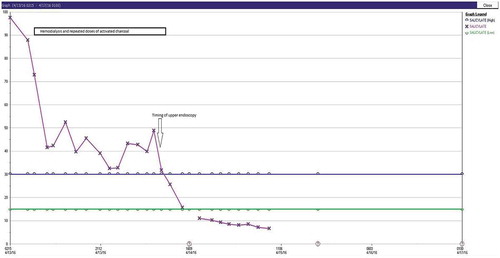
Gastroenterology was consulted, however an endoscopy was not performed till the next morning. Due to the delay in endoscopy, repeated doses of activated charcoal were administered. On endoscopy the following day, gastritis was noted, however there was no evidence of a bezoar. With continued hemodialysis for close to 30 hours, alkalinization of urine and activated charcoal, salicylate level finally began to decline (). The patient was discharged to inpatient psychiatry in a stable condition.
2. Discussion
Salicylate overdose is a common problem in the USA due to the ease of its availability and its presence in various over the counter preparations [Citation1]. It is known to have an increased morbidity and mortality especially if symptoms are not recognized and treated early.
Overdoses with aspirin have varying clinical presentations depending on dosage and acuity. Typically patients will present with tinnitus along with respiratory and gastrointestinal abnormalities [Citation2]. Effects in terms of metabolic and electrolyte disturbances may occur as well. These metabolic disturbances can include a mixed acid-base picture as well as either hypo- or hyperglycemia.
Usually the symptoms patients experience can be divided into acute and chronic presentations [Citation2,Citation3]. The longer the patient goes without treatment, the more severe the symptoms get and the greater the risk for mortality. Neurological symptoms such as altered mental status, seizures and coma are later manifestations of toxicity. Whereas stimulation of the respiratory center leading to alterations of the respiratory rate occurs early on. These patients will typically present with tachypnea with respiratory alkalosis [Citation2,Citation3]. Gastrointestinal issues of nausea, vomiting, abdominal pain, and diarrhea can also be seen in an acute presentation. The GI disturbances that patients experience are largely due to the fact that aspirin causes corrosive injury to the GI tract.
Aspirin, particularly the enteric-coated formulations, have also been known to have a propensity for bezoar development in the stomach [Citation3]. A pharmacobezoar most often occurs when there is an altered motility or anatomy of the gastrointestinal tract [Citation4]. A bezoar can create prolonged symptoms due to it intermittently releasing its active ingredients. Although bezoars are rare, they should be considered and if suspected, they should be investigated with endoscopy [Citation5]. Emergent endoscopy is recommended to reduce the slow release and absorption of pharmacobezoars, and hence reduce mortality and morbidity of the ingested substance.
In the case of the patient reported, we believe that the persistently elevated salicylate levels found were secondary to the formation of a pharmacobezoar. The dense opacity present in the stomach fundus on abdominal radiogram was likely a representation of the same (). Bezoars lead to delayed absorption of aspirin and hence persistently elevated salicylate levels. Other clinical features of bezoars would include local symptoms of nausea, vomiting and gastrointestinal tract obstruction [Citation5]. They often lead to the need for prolonged treatment and increase in morbidity. Our patient was on hemodialysis treatment for nearly 30 hours before we saw a decline in salicylate levels and clinical improvement. Our initial requests for endoscopy were unsuccessful which might have decreased the need for prolonged hemodialysis.
Treatment of salicylate overdose as with other intoxications, involves stabilization and then can be focused on decreasing absorption and enhancing elimination of the toxin. This would include alkalinization of urine with sodium bicarbonate infusion, activated charcoal and hemodialysis if indicated [Citation2,Citation3]. Alkalinization of urine helps reduce toxicity due to its potential of increasing the excretion of ionized salicylate [Citation1]. Hemodialysis is typically only used if there is evidence of severe toxicity in terms of end-organ injury or acute deterioration [Citation1]. It is an effective way to treat aspirin toxicity because of the drug’s molecular weight, low volume of distribution and high water solubility [Citation1]. The patient described here received repeated doses of activated charcoal along with sodium bicarbonate, and hemodialysis but had a delayed endoscopy.
3. Conclusion
The aim of this case presentation is to present a patient with severe aspirin toxicity who despite multiple treatments that included hemodialysis, continued to have rising salicylate levels. Most likely that was due to the presence of a pharmacobezoar. We emphasize that although pharmacobezoars are rare, if there is suspicion of one, an immediate endoscopy should be performed.
Graph 1. Representation of Salicylate levels and course of treatment interventions.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- Minns A, Cantrell F, Clark R. Death due to acute salicylate intoxication despite dialysis. J Emergency Med. 2011 May;40(5):515–517.
- O’Malley GF. Emergency department management of the salicylate-poisoned patient. Emerg Med Clin North Am. 2007 May;25(2):333–346.
- Fertel B, Nelson L, Goldfarb D. The underutilization of hemodialysis in patients with salicylate poisoning. Kidney Int. 2009 June 15;75(12):1349–1353.
- Stack PE, Pharmacobezoar: TE. An evolving new entity. Dig Dis. 1995;13:356–364.
- Bogacz K, Caldron P. Enteric-coated aspirin bezoar: elevation of serum salicylate level by barium study. Case report and review of medical management. Am J Med. 1987 Oct;83(4):783–786.