
ABSTRACT
Background: The COVID-19 is an emerging infectious disease that impacted HealthCare System worldwide and patients undergoing elective surgical procedures is associated with a high mortality rate and a complicated perioperative course.
Methods: A retrospective observational study, the research design was conducted utilizing the RedCap ACS COVID-19 Registry and Cerner EMR. The intent of this design is to create statistical information about confirmed COVID-19 cases admitted in an academic institution in Brooklyn, New York from March to May 2020.
Results: A total of 1413 patients were included in the final analysis. Of the 1413 patients, 520 Expired, 40.5% were males, and 33% were females, p = 0.004. Male patients had high mortality at a rate that is statistically significant. For race of those ‘Expired’, 38.3% white, 34.2% Black, 28.2% Asian, and Unknown 43.6%, showing statistical significance at p = 0.050. The most common co-morbidities for those not-Expired versus Expired: DM, 44.6% expired versus 55.6% not-expired, HTN, 77.1% versus 22.9%, and CAD, 47.9% versus 52.1%. Comparing the data of COVID-19 patients without surgery and with those who had surgery, it was observed that 53% of those who did not have surgery went ‘Home’ versus 38.6%, of those with surgery who could not. Further examining those without surgery versus those with surgery: 3.4% versus 13.3% discharge to ‘Rehab’, for ‘Other discharge’ destinations 5.9% versus 14.5%, and for ‘Expired’ 37.1% versus 31.3%. Overall, the presence of surgery had a significant impact on COVID-19 patients discharge destinations at p = < 0.001.
Conclusions: The implications of change in the setting of our current clinical practice therefore require forbearance, training, preparedness, and education to efficiently maintain our essential surgical services.
1. Background
COVID-19 created a global pandemic and New York City had more severe cases than anywhere worldwide[Citation1]. Consequently, the formidable outcome of the virus affected multiple-race populations with variations in age, race, and with comorbidities that caused interference in current clinical practice and personal lives. COVID-19 is an emerging infectious disease that has impacted healthcare systems worldwide. The effects of the disease can range from asymptomatic to mild illness, multi-organ system organ failure, and respiratory failure needing mechanical support and intensive-care management [Citation2]. Numerous preventative strategies including non- pharmaceutical interventions such as social distancing, isolation, and hand washing were implemented, while awaiting the vaccines that have been under development [Citation3].
The COVID-19 affects the current guidelines in the perioperative testing phase with considerations about patient risk factors, anesthetic procedure choice, and management of the postoperative recovery phase, that are coordinated based on the patient’s clinical history and co-morbidities prior to surgery especially for patients undertaking intermediate to high-risk surgery [Citation4]. The perioperative management changes in patients with underlying chronic disease and should be evaluated with appropriate preoperative testing. There are guidelines available that may improve outcomes that are followed by many anesthesiologists. The study hospital had 1413 cases of confirmed COVID-19 that were admitted from March to May 2020, in one of the Institution located in Brooklyn, New York. These were cases admitted through the emergency department with some discharges to the community, but with some associated mortalities. In May 2020, the hospital joined the ACS COVID −19 Registry, RedCap, a clinical data registry for COVID-19 cases. The ACS RedCap introduced a series of variables collecting important clinical patient data points for patients with and without surgical treatment. The data was abstracted from the hospital electronic health record, CERNER, with confirmed COVID-19 diagnoses admitted from March to- May of 2020. The aim of this study is to provide information to patients prior to surgery in anticipation of a better surgical outcome during the COVID-19 pandemic. The pandemic affects the current surgical process of care and planning in the peri-operative period.
In the course of the COVID-19 pandemic, the state of New York mandated that all elective surgical operations be canceled. Consideration of surgical cases was to be based on patient risk associated with COVID-19 [Citation5]. Moreover, the hospital during a pandemic was allocated for treatment of the disease and to expand the number of beds accessible for patients affected by COVID-19. The COVID-19 pandemic accordingly led to numerous questions in the acute management of patients undergoing elective procedures and emergency procedures. Patients with COVID-19, undergoing elective surgical procedures, have been found to have a high mortality rate and a complicated perioperative course [Citation6].
2. Purpose
The purpose of this study is to investigate the clinical characteristics of those confirmed admitted COVID-19 patients. Further, the result of this investigation is to utilize various evidence-based processes of care and to appropriately develop perioperative initiatives that will clearly define the clinical risk of patients with COVID-19 in the perioperative period. Apart from the clinical characteristics, the study examines various measures that are considered appropriate in preparing surgical patients prior to surgical procedures and measures that are required based on the established preoperative risk.
3. Methods
A retrospective observational study, the research design was conducted utilizing the Red Cap ACS COVID-19 Registry and Cerner EMR. The intent of this design is to create statistical information about confirmed COVID-19 cases admitted in an academic institution in Brooklyn, New York from March to May 2020. The sample size is a total of 1413 patients admitted from March 2020-May 2020 utilizing the ACS COVID-19 registry. The data collected focused on all confirmed COVID-19 patients 18 years old and above from admission to discharge. Data variables collected were patient’s demographics, severity predictors, admission information, and discharge information. The inclusion criteria included: patients older than 18 years old, male and females with confirmed diagnosis of COVID-19 utilizing PCR and antibodies. There were 100 publications identified and 30 studies were selected for quantitative analysis written in English.
The primary outcome measure of this study is to identify the clinical characteristics of COVID-19 patients with the greatest risk of mortality. Secondary outcome measures explore the differences by age, race, gender, and severity predictors for detection of disparities among affected groups.
4. Statistical analysis
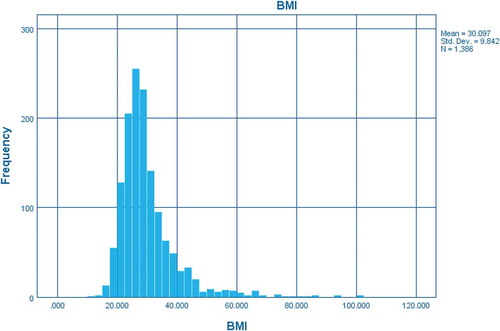
All analyses were done in SPSS, version 26. To test the categorical variables between gender, race, origin status, travel, discharge and assessment of frailty, chi-square test was used. To test the differences in means of continuous variables between body mass index (BMI) and age, t-test was used. Logistic regression was done in expiration to compare with age, sex, BMI, diabetes (DM), hypertension (HTN), coronary artery disease (CAD), and race with white as reference variables. Race odds are not so reliable due to > 200 unknown cases reported in the race categories that may not have been white.
5. Ethical considerations
The study was approved by the Institution’s Research Board. Obtaining informed or written consent was not needed. The subjects were not exposed to life threatening or anticipated risk. The participant’s privacy and confidentiality of their information were safeguarded.
6. Results
A total of 1413 patients were included in the final analysis. Gender, 40.5% males versus 33% females, p = 0.004, males had statistically significant higher mortality. For race of those ‘Expired’, 38.3% white, 34.2% Black, 28.2% Asian, and Unknown 43.6%, showing statistical significance at p = 0.050. Given that this is at the cusp of insignificance with a large percentage ‘Unknown’ race should not be deemed statistically significant without further investigation. For assessment of frailty, deaths were 66% non-ambulatory versus 31% ambulatory: the impact of level of frailty was significant at p = < 0.001. Differences in mortality assessed by BMI were achieved by creating two categories (Obese and Not Obese with a BMI of 29 as the threshold) and while the results showed statistical significance with a chi-square p-value of < 0.001. The percentage of those labeled Obese who died was 30.9%, while those Not Obese was 40%. Likewise in using a Logistic Regression, BMI had a slight (but not statistically significant) negative impact in the Odds Ratio for Death. Overall, patient’s characteristics are shown in and .
Table 1. Patient Characteristics
Figure 1. Patient Age in years
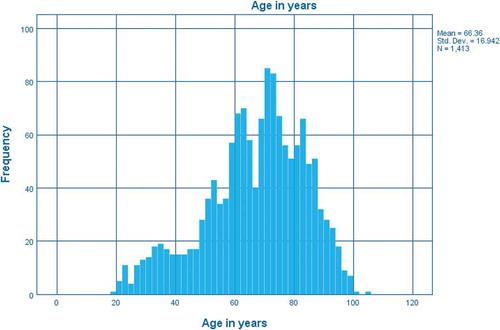
Figure 2. Patient Age in years
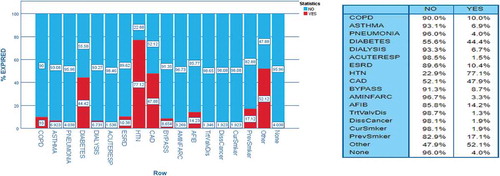
The most common co-morbidities for those not-Expired versus Expired: DM, 44.6% expired versus 55.6% not-expired, HTN, 77.1% versus 22.9%, and CAD, 47.9% versus 52.1%. Again referring to a binary logistic regression with deaths as the outcome, there is a significant impact for DM, the odds are about 1.5 times greater than for person without DM; for CAD cases, the odds were decreased to about half of the odds of someone without CAD, but overall assessment for an individual needs to be made taking all factors into account. Co-morbidities and Deaths with Co-Morbidities are exhibited in .
Figure 3. Cases with co-morbidities
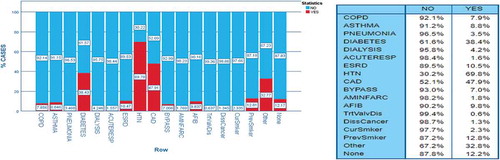
Figure 4. Deaths with co-morbidities
A total of 83 patients had surgery, out of 1413 samples. Comparing the data of COVID-19 patients without surgery and with those who had surgery, it was observed that 53% of those who did not have surgery went ‘Home’ versus 38.6%, of those with surgery who could not. Further examining those without surgery versus those with surgery: 3.4% versus 13.3% discharge to ‘Rehab’, for ‘Other discharge’ destinations 5.9% versus 14.5%, and for “Expired 37.1% versus 31.3%. Overall, presence of surgery had significant impact on COVID-19 patients discharge destinations at p = < 0.001. When controlling the relationship between surgery and discharge outcomes for key comorbidities, it was found that for patients who had surgery with asthma, the relationship between surgery and discharge was no longer significant with a chi-square p-value of 0.471. That same phenomenon holds for patients with bypass with p value of 0.88 and with CAD with p value of 0.003. Overall relationships between surgery and discharge outcomes is shown on while the layered impact of the comorbidities is shown in .
Figure 5. Surgery and discharge
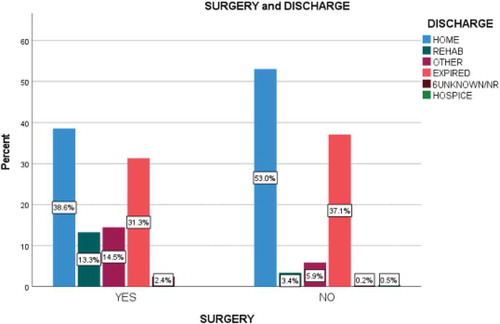
Figure 6. Surgery and discharge: total and by co-morbidity
7. Discussion
In this study, obesity was observed, but with no significant impact that suggests a deeper investigation into the role of BMI and obesity in COVID-19 death that should be undertaken. The existence of these serious co-morbid conditions and heightened by the presence of fat tissues in the thoracic area corresponds to an increased risk of severe cases of COVID-19 infections consequently can lead to an increased demand for mechanical ventilation and mortality [Citation7]. Further, in the individuals with obesity, the adipose tissues appeared serve as a reservoir for the COVID-19 virus causing systemic inflammation and an immune response [Citation8]. Obesity is a risk factor for COVID-19 management and with increased association with postoperative mortality, stroke, myocardial infarction, and respiratory difficulty [Citation9]. Moreover, obesity-related complications are an increasing issue worldwide that impact in perioperative and postoperative surgical outcomes that are generally associated with prolonged hospitalization and higher readmission rates [Citation10]. The analysis of these data suggests that obesity alone was not a significant risk factor in management and treatment of COVID-19. Respectively, obesity associated risk of mortality accumulatively higher compared to non-obesity due to obesity-related comorbidities such as DM, HTN, cardiac, and cerebrovascular disease. Since obesity is a combination of multiple diseases leading to metabolic syndrome, as a result, there is an increased need of advanced airway support [Citation11]. Therefore, it is necessary to perform a detailed preoperative evaluation, risk assessment, and counseling prior to engaging obese individuals in surgical procedures that are necessary. Moreover, obesity with ongoing co-morbidities can have a substantial impact on the peri-operative surgical outcomes. A multidisciplinary team approach is necessary in preoperative management including referral to a dietitian, a psychiatrist, a psychologist, and a bariatric surgeon if necessary [Citation12].
COVID-19 affected patients with kidney problems distinctively for individuals on hemodialysis. The population of hemodialysis patients are characterized mostly of the vulnerable and immunocompromised. Although the COVID-19 virus in severe cases causes respiratory and multiple-organ failure, it is not clear in the setting of individuals suffering from chronic kidney disease [Citation13]. 10.4% of this study were diagnosed with end stage renal disease. Furthermore, it is theorized that COVID-19 enters the human cell due to an enzyme that is copious in renal tubular cells called angiotensin-converting enzyme 2 (ACE2) [Citation13]. The complexity of COVID-19 has imparted challenges in preparing and managing CKD patients based on their perioperative complications compared with non-CKD patients [Citation14]. It was concluded in one study that patients receiving preoperative angiotensin axis blockade (AAB) undergoing major elective orthopedic surgery have increased probability of post-induction hypotension and postoperative acute kidney injury that leads to prolonged hospital length of stay [Citation15]. In the setting of COVID-19 −19, the screening is done during pre-surgical testing visit that outlines all needed specifics on how to manage a suspected COVID-19 −19 prior to surgery. This may warrant the surgical team to have strategies and requires further surveillance of patients’ condition more focused before induction of anesthesia and the increased preoperative cardiac demands of individuals with kidney dysfunction and the confirmed COVID-19 −19 patients.
Perioperative management has a significant impact on surgical outcomes. In this study, there is high mortality in males compared to females. The COVID-19 causes severe acute respiratory failure and high mortality in males, elderly and individuals with co-morbidities [Citation16]. Subsequently, patients with chronic obstructive pulmonary disease (COPD) have a high chance to have severe pneumonia with poor medical outcomes. These can be explained by having poor lung reserves and abundant ACE2 receptors in the small airways of the lungs [Citation17]. COPD patients and current smokers have increased risk of severe complications with greater mortality rates in association with COVID-19. This study found that individuals who expired had COPD (10.0%), were current smokers (1.9%), and who had a history of previous smoking (17.1%). These co-morbid conditions preoperatively require careful clinical assessments and management in order to provide better surgical outcomes. Common strategies to reduce risk of complications are smoking cessation and optimization of COPD that mainly consist of long-acting bronchodilators and pulmonary rehabilitation [Citation18]. Establishing a greater dissemination about smoking cessation, availability of alternative treatment and having a guideline that address smoking cessation treatment are crucial.
Another characteristic investigated in this study was the assessment of frailty. Understanding the geriatric physiology can provide better surgical outcomes by properly providing risk stratification in the era of COVID-19 pandemic [Citation19]. It was reported that older people regardless of their ethnicity have been unequally affected by COVID-19 and had severe clinical presentations compared to younger populations [Citation20]. These might be related to frailty and the presence of underlying medical co-morbidities that presented susceptibility to a severe clinical scenario of COVID-19 sequela. Regardless of the association of frailty, the proposed initiatives will require conscientious surveillance, testing and reporting of morbidity and mortality of all COVID-19 cases. For geriatric patients undergoing surgery, it will require a standard of care that can incorporate the issues associated with better outcomes of surgery in high-risk frail, older patients. The standard of care requires a multi-modal pre-habilitation that comprises nutrition supplementation, exercise and pulmonary optimization [Citation21].
It was concluded in the study of [Citation22] that the observed risk for venous thrombosis (VTE) is high for patients in the intensive care unit (ICU) affected by COVID-19 regardless of the pharmacologic thrombo-prophylaxis. It was reported that 50% of COVID-19 patients having severe cases had increased coagulopathy. It was theorized that the release of cytokines from direct viral effects, increase of vasoconstrictor angiotensin 11, decrease in vasodilator angiotensin and the sepsis can precipitate coagulopathy [Citation23]. Considering the deadly drawback of COVID-19, it requires an effective management and treatment of VTE in order to improve the complexity of coagulopathy onset. It is necessary to perform a comprehensive history and physical examination prior to surgery especially for those populations undergoing high-risk surgery. Although cardiovascular testing is seldom recommended with a low-risk surgery, it should be advised on patient-specific risk [Citation24].
The implications of change in the setting of our current clinical practice, therefore, require forbearance, training, preparedness, and education to efficiently maintain our essential surgical services. The unpredictability of the virus needs everyone to be vigilant requiring considerable virus testing, contact tracing, and reshaping of our current clinical practice. Additionally, this change will protect our healthcare workers and disintegration of our healthcare system during the time of COVID-19 Pandemic.
Disclosure of potential conflicts of interest
No potential conflict of interest was reported by the author(s).
Acknowledgments
The authors are thankful to Dr. Emily Mahon, PhD (WPU-Department of Sociology) for sharing her expertise in SPSS statistics, Eytan Palte, MD (Resident Physician-NYP Columbia), Michael Zingman, MD-MPH (Psychiatry Resident – NYU Langone), Benjamin Wagner, MD (Resident Physician – Beth Israel Deaconess Medical Center) and Mahavrat Srivastava-Malick, MD (Post-Doctoral Residency Fellow Department of Pathology-Columbia University) for providing assistance during ACS RedCap data abstraction.
References
- CDC COVID-19 Response Team. Geographic differences in COVID-19 cases, deaths, and incidence - USA, February 12-April 7, 2020. MMWR Morb Mortal Wkly Rep. 2020 Apr 17;69(15):465–471. PMID: 32298250; PMCID: PMC7755058.
- Greenland JR, Michelow MD, Wang L, et al. COVID-19 infection: perioperative implications: reply. Anesthesiology. 2020 Sep;133(3):678–679. PMID: 32604140.
- Nicola M, O’Neill N, Sohrabi C, et al. Evidence based management guideline for the COVID-19 pandemic - Review article. Int J Surg. 2020 May;77:206–216. Epub 2020 Apr 11. PMID: 32289472; PMCID: PMC7151371.
- Collins CS, Feely MA, Daniels PR, et al. A systematic approach to the preoperative medical evaluation of adults. Hosp Pract (1995). 2014 Feb;42(1):52–64. PMID: 24566597.
- www.ascassociation.org. (n.d.). State guidance on elective surgeries. [online]. [cited 2020 Mar 30]. Available from: https://www.ascassociation.org/asca/resourcecenter/latestnewsresourcecenter/covid-19/covid-19-state
- Flemming S, Hankir M, Ernestus RI, et al. Surgery in times of COVID-19-recommendations for hospital and patient management. Langenbecks Arch Surg. 2020 May;405(3):359–364. Epub 2020 May 8. PMID: 32385568; PMCID: PMC7205906.
- Scheen AJ. Obésité et risque de COVID-19 sévère [Obesity and risk of severe COVID-19]. Rev Med Suisse. 2020 May 27;16(695):1115–1119. French. PMID: 32462841.
- Ritter A, Kreis NN, Louwen F, et al. Obesity and COVID-19: molecular mechanisms linking both pandemics. Int J Mol Sci. 2020 Aug 12;21(16):5793. PMID: 32806722; PMCID: PMC7460849.
- Phan K, Khuong JN, Xu J, et al. Obesity and postoperative atrial fibrillation in patients undergoing cardiac surgery: systematic review and meta-analysis. Int J Cardiol. 2016 Aug 15;217:49–57.
- Poelemeijer YQM, Lijftogt N, Detering R, et al. Obesity as a determinant of perioperative and postoperative outcome in patients following colorectal cancer surgery: a population-based study (2009-2016). Eur J Surg Oncol. 2018 Dec;44(12):1849–1857. Epub 2018 Jun 6. PMID: 29937416.
- Hussain A, Mahawar K, Xia Z, et al. Obesity and mortality of COVID-19. Meta-analysis. Obes Res Clin Pract. 2020 Jul-Aug;14(4):295–300. Epub 2020 Jul 9. Retraction in: Obes Res Clin Pract. 2021 Jan-Feb;15(1):100.PMID: 32660813; PMCID: PMC7346803.
- Glatt D, Sorenson T. Metabolic and bariatric surgery for obesity: a review. S D Med. 2011;Spec No:57–62. PMID: 21721189.
- Angel-Korman A, Brosh T, Glick K, et al. COVID-19, THE KIDNEY AND HYPERTENSION. Harefuah. 2020 Apr;159(4):231–234. Hebrew. PMID: 32307955.
- You Y, Zhang Y, Qiang L, et al. Prevalence and risk factors for perioperative complications of CKD patients undergoing elective hip surgery. J Orthop Surg Res. 2019 Mar 20;14(1):82. PMID: 30894199; PMCID: PMC6425709.
- Nielson E, Hennrikus E, Lehman E, et al. Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014 May 9;(5):283–288. Epub 2014 Jan 24. PMID: 24464761
- Higham A, Mathioudakis A, Vestbo J, et al. COVID-19 and COPD: a narrative review of the basic science and clinical outcomes. Eur Respir Rev. 2020 Nov 5;29(158):200199. PMID: 33153991; PMCID: PMC7651840.
- Leung JM, Niikura M, Yang CWT, et al. COVID-19 and COPD. Eur Respir J. 2020 Aug 13;56(2):2002108. PMID: 32817205; PMCID: PMC7424116.
- Hoshikawa Y, Tochii D. Postoperative atelectasis and pneumonia after general thoracic surgery. Kyobu Geka. 2017 Jul;70(8):649–655. Japanese. PMID: 28790283.
- Khan KT, Hemati K, Donovan AL. Geriatric physiology and the frailty syndrome. Anesthesiol Clin. 2019 Sep;37(3):453–474. Epub 2019 Jun 18. PMID: 31337478.
- Andrew M, Searle SD, McElhaney JE, et al. COVID-19, frailty and long-term care: implications for policy and practice. J Infect Dev Ctries. 2020 May 31;14(5):428–432. PMID: 32525825.
- Hanna K, Ditillo M, Joseph B. The role of frailty and prehabilitation in surgery. Curr Opin Crit Care. 2019 Dec;25(6):717–722. PMID: 31689246.
- Middeldorp S, Coppens M, Van Haaps TF, et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost. 2020 Aug;18(8):1995–2002. Epub 2020 Jul 27. PMID: 32369666; PMCID: PMC7497052.
- Miesbach W, Makris M. COVID-19: coagulopathy, risk of thrombosis, and the rationale for anticoagulation. Clin Appl Thromb Hemost. 2020 Jan-Dec;26:1076029620938149. PMID: 32677459; PMCID: PMC7370334.
- Smilowitz NR, Berger JS. Perioperative cardiovascular risk assessment and management for noncardiac surgery: a review. JAMA. 2020 Jul 21;324(3):279–290. PMID: 32692391.