
Abstract
Salmonella is one of the most frequently isolated foodborne pathogens. It is a major worldwide public health concern, accounting for 93.8 million foodborne illnesses and 155,000 deaths per year. To date, over 2500 Salmonella serotypes have been identified and more than half of them belong to Salmonella enterica subsp. enterica, which accounts for the majority of Salmonella infections in humans. Salmonella infections that involve invasive serotypes are often life threatening, necessitating appropriate and effective antibiotic therapy. The emergence of multi-drug-resistant (MDR) Salmonella serotypes is having a great impact on the efficacy of antibiotic treatment, and an increasing prevalence of MDR strains may lead to an increase in mortality rates of Salmonella infections. Epidemiological studies indicate that MDR Salmonella serotypes are more virulent than susceptible strains, as reflected by increased severity and more prolonged disease in patients infected by MDR strains. Preventive measures have been proposed to eliminate the spread of Salmonella infection. While the maintenance of effective food hygiene and water sanitation remain the cornerstones, additional measures such as restriction of indiscriminate use of antibiotics in food animals are important. This review provides an overview of Salmonella infection, and discusses the nomenclature, pathogenesis, clinical manifestations, epidemiology and antibiotic resistance of Salmonella.
Introduction
Salmonella infection remains a major public health concern worldwide, contributing to the economic burden of both industrialized and underdeveloped countries through the costs associated with surveillance, prevention and treatment of disease (Crump et al. Citation2004). Gastroenteritis is the most common manifestation of Salmonella infection worldwide, followed by bacteraemia and enteric fever (Majowicz et al. Citation2010) (). Salmonella is a rod-shaped, Gram-negative facultative anaerobe that belongs to the family Enterobacteriaceae (Barlow & Hall Citation2002). Within the genus Salmonella, around 2600 serotypes have been identified with the use of the standard Kauffman–White scheme and most of these serotypes have the ability to adapt within a variety of animal hosts, including humans (Allerberger et al. Citation2003). Salmonella and Campylobacter are the most frequently isolated foodborne pathogens, and are predominantly found in poultry, eggs and dairy products (Silva et al. Citation2011). Other food sources that are involved in the transmission of Salmonella include fresh fruits and vegetables (Pui et al. Citation2011). In general, food animals such as swine, poultry and cattle are the prime sources of Salmonella infections. The major dissemination routes of the pathogens involve trade in animals and uncooked animal food products. The slaughtering process of food animals at abattoirs is considered one of the important sources of organ and carcass contamination with Salmonella (Gillespie et al. Citation2005). The emergence of antibiotic-resistant foodborne pathogens has raised the concern of the public as these pathogens are more virulent, causing an increase in the mortality rate of infected patients (Chiu et al. Citation2002).
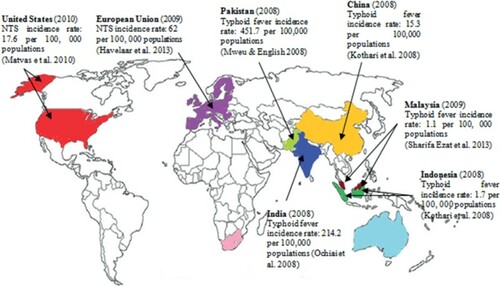
Figure 1. Incidence rate of enteric fever and gastroenteritis in different regions around the world.
Classification and nomenclature
Salmonella was first discovered and isolated from the intestines of pigs infected with classical swine fever, by Theobald Smith in 1855. The bacterial strain was named after Dr Daniel Elmer Salmon, an American pathologist who worked with Smith. The nomenclature of Salmonella is controversial and still evolving. Currently, the Centers for Disease Control and Prevention (CDC) uses the nomenclatural system of Salmonella recommended by the World Health Organization (WHO) Collaborating Centre (Popoff et al. Citation2003). According to this system, the genus Salmonella is classified into two species, Salmonella enterica (type species) and Salmonella bongori, based on differences in their 16S rRNA sequence analysis. The type species, S. enterica, can be further classified into six subspecies based on their genomic relatedness and biochemical properties (Reeves et al. Citation1989). The subspecies are denoted with roman numerals: I, S. enterica subsp. enterica; II, S. enterica subsp. salamae; IIIa, S. enterica subsp. arizonae; IIIb, S. enterica subsp. diarizonae; IV, S. enterica subsp. houtenae; and VI, S. enterica subsp. indica. Among all the subspecies of Salmonella, S. enterica subsp. enterica (I) is found predominantly in mammals and contributes approximately 99% of Salmonella infections in humans and warm-blooded animals. In contrast, the other five Salmonella subspecies and S. bongori are found mainly in the environment and also in cold-blooded animals, and hence are rare in humans (Brenner et al. Citation2000).
In addition to the classification of subspecies based on phylogeny, Kauffman and White developed a scheme to further classify Salmonella by serotype based on three major antigenic determinants: somatic (O), capsular (K) and flagellar (H) (Brenner et al. Citation2000). The heat-stable somatic O antigen is the oligosaccharide component of lipopolysaccharide located at the outer bacterial membrane. A specific serotype of Salmonella can express more than one O antigen on its surface (Hu & Kopecko Citation2003). The heat-labile H antigens are found in the bacterial flagella and are involved in the activation of host immune responses. Most Salmonella spp. contain two distinct genes that encode for the flagellar proteins; these bacteria have the special ability of expressing only one protein at a time and are, therefore, called diphasic (phase I and II). Each serotype expresses specific phase I H antigens which are responsible for its immunological identity, whereas phase II antigens are non-specific antigens that can be shared by many serotypes (McQuiston et al. Citation2008). The surface K antigens are heat-sensitive polysaccharides located at the bacterial capsular surface and are the least common antigens found in the serotypes of Salmonella. Virulence (Vi) antigens, a special subtype of K antigen, are found only in three pathogenic serotypes: Paratyphi C, Dublin and Typhi.
A formal identification of a specific serotype can be carried out by comprehensive serotyping of all the antigenic determinants of the bacterium. However, most clinical laboratories prefer to conduct simple agglutination reactions to antibodies or antisera specific to the somatic O antigens with the intention of grouping Salmonellae into six serogroups, designated A, B, C1, C2, D and E. This grouping system provides valuable information for epidemiological studies and allows genus identification of Salmonella infections (Wattiau et al. Citation2011). To date, over 2500 serotypes have been identified; more than 50% of these serotypes belong to S. enterica subsp. enterica, which accounts for most of the Salmonella infections in humans (Guibourdenche et al. Citation2010). The term ‘serovar’, which is synonymous to serotype, is commonly used in the literature. Although the species name ‘Salmonella enterica’ has been adopted by the CDC and WHO for years, it has not been accepted officially by the Judicial Commission. Therefore, the naming of a particular Salmonella serotype usually omits the subspecies; Salmonella enterica subspecies enterica serotype Typhi, for example, is shortened to Salmonella ser. Typhi or S. Typhi in the literature (Brenner et al. Citation2000).
Pathogenesis
The severity of Salmonella infections in humans varies depending on the serotype involved and the health status of the human host. Children below the age of 5 years, elderly people and patients with immunosuppression are more susceptible to Salmonella infection than healthy individuals. Almost all strains of Salmonella are pathogenic as they have the ability to invade, replicate and survive in human host cells, resulting in potentially fatal disease.
Salmonella displays a remarkable characteristic during its invasion of non-phagocytic human host cells (Hansen-Wester et al. Citation2002) whereby it actually induces its own phagocytosis in order to gain access to the host cell. The remarkable genetics underlying this ingenious strategy is found in Salmonella pathogenicity islands (SPIs), gene clusters located at the large chromosomal DNA region and encoding for the structures involved in the invasion process (Grassl & Finlay Citation2008). When the bacteria enter the digestive tract via contaminated water or food, they tend to penetrate the epithelial cells lining the intestinal wall. SPIs encode for type III secretion systems, multi-channel proteins that allow Salmonella to inject its effectors across the intestinal epithelial cell membrane into the cytoplasm. The bacterial effectors then activate the signal transduction pathway and trigger reconstruction of the actin cytoskeleton of the host cell, resulting in the outward extension or ruffle of the epithelial cell membrane to engulf the bacteria. The morphology of the membrane ruffle resembles the process of phagocytosis (Takaya et al. Citation2003).
The ability of Salmonella strains to persist in the host cell is crucial for pathogenesis, as strains lacking this ability are non-virulent (Bakowski et al. Citation2008). Following the engulfment of Salmonella into the host cell, the bacterium is encased in a membrane compartment called a vacuole, which is composed of the host cell membrane. Under normal circumstances, the presence of the bacterial foreign body would activate the host cell immune response, resulting in the fusion of the lysosomes and the secretion of digesting enzymes to degrade the intracellular bacteria. However, Salmonella uses the type III secretion system to inject other effector proteins into the vacuole, causing the alteration of the compartment structure. The remodelled vacuole blocks the fusion of the lysosomes and this permits the intracellular survival and replication of the bacteria within the host cells. The capability of the bacteria to survive within macrophages allows them to be carried in the reticuloendothelial system (RES) (Monack et al. Citation2004).
Clinical manifestations
Based on the clinical patterns in human salmonellosis, Salmonella strains can be grouped into typhoid Salmonella and non-typhoid Salmonella (NTS). In human infections, the four different clinical manifestations are enteric fever, gastroenteritis, bacteraemia and other extraintestinal complications, and chronic carrier state (Sheorey & Darby Citation2008).
Enteric fever
Salmonella Typhi is the aetiological agent of typhoid fever, while paratyphoid fever is caused by S. Paratyphi A, B and C. Since the clinical symptoms of paratyphoid fever are indistinguishable from typhoid fever, the term ‘enteric fever’ is used collectively for both fevers, and both S. Typhi and S. Paratyphi are referred as typhoid Salmonella (Connor & Schwartz Citation2005). Humans are the sole reservoir for the two strains of typhoid Salmonella. The organisms are transmitted via the ingestion of food or water contaminated with the waste of infected individuals. Enteric fever is characterized by an incubation period of one week or more, with prodomal symptoms such as headache, abdominal pain and diarrhoea (or constipation), followed by the onset of fever (Bhan et al. Citation2005). Diarrhoea is more commonly observed in children, whereas patients with immunosuppression are more likely to develop constipation (Thielman & Guerrant Citation2004). During the illness, enteric fever displays a specific fever pattern with an initial low-grade fever (> 37.5°C to 38.2°C) which slowly develops to high-grade fever (> 38.2°C to 41.5°C) in the second week. If the patient is left untreated, fever can persist for a month or more (Patel et al. Citation2010). Besides fever, infected patients may also develop myalgia, bradycardia, hepatomegaly (enlarged liver), splenomegaly (enlarged spleen), and rose spots on their chest and abdomen (Kuvandik et al. Citation2009). In endemic regions, approximately 15% of the infected patients develop gastrointestinal complications which include pancreatitis, hepatitis and cholecystitis. Haemorrhage is one of the most severe gastrointestinal complications that occur as a result of perforation of Peyer's patches, lymphatic nodules located at the terminal ileum, resulting in bloody diarrhoea. On top of that, the ability of typhoid Salmonella to survive and persist in the RES results in relapse in approximately 10% of the infected patients (Parry et al. Citation2002).
Gastroenteritis
Salmonella strains other than S. Typhi and S. Paratyphi are referred to as NTS, and are predominantly found in animal reservoirs. NTS infections are characterized by gastroenteritis or ‘stomach flu’, an inflammatory condition of the gastrointestinal tract which is accompanied by symptoms such as non-bloody diarrhoea, vomiting, nausea, headache, abdominal cramps and myalgias. Symptoms such as hepatomegaly and splenomegaly are less commonly observed in patients infected with NTS (Hohmann Citation2001). Compared to typhoid infections, NTS infections have a shorter incubation period (6–12 h) and the symptoms are usually self-limiting and last only for 10 days or less (Crump et al. Citation2008). Gastrointestinal complications of NTS infections include cholecystitis, pancreatitis and appendicitis, while the perforation of the terminal ileum has no association with NTS infections (Hohmann Citation2001). Infants, young children, elderly people and immunocompromised patients are highly susceptible to NTS infections and develop more severe symptoms than normal individuals (Scallan et al. Citation2011).
Bacteraemia and other extraintestinal complications
Salmonella bacteraemia is a condition whereby the bacteria enter the bloodstream after invading the intestinal barrier. Almost all the serotypes of Salmonella can cause bacteraemia, while S. Dublin and S. Cholearaesuis are two invasive strains that are highly associated with the manifestations of bacteraemia (Woods et al. Citation2008). Similar to enteric fever, high fever is the characteristic symptom of bacteraemia, but without the formation of rose spots as observed in patients with enteric fever. In severe conditions, the immune response triggered by bacteraemia can lead to septic shock, with a high mortality rate. The clinical manifestation of bacteraemia is more commonly seen in NTS infections than in typhoid Salmonella infections. The difference in the clinical manifestation is believed to be associated with the presence of the spv (Salmonella plasmid virulence) gene in NTS which causes non-typhoidal bacteraemia, based on genetic analysis (Guiney & Fierer Citation2011). Although the mechanism of the gene to enhance the virulence traits of NTS remains unclear, expression of the gene is required to prolong apoptotic cell death and this may allow the bacteria to persist in the host cells for a longer period (Gulig et al. Citation1993). Approximately 5% of patients infected with NTS develop bacteraemia and, in some cases, extraintestinal complications occur, with the lung being the most commonly compromised organ. Other extraintestinal complications include cellulitis, urinary tract infections, pneumonia, endocarditis and meningitis (Shimoni et al. Citation1999; Arii et al. Citation2002).
Chronic carrier state
The status of chronic carrier is defined as the shedding of bacteria in stools for more than a year after the acute stage of Salmonella infection. Since humans are the only reservoir of typhoid Salmonella, carriers of S. Typhi and S. Paratyphi are responsible for the spreading of enteric fever in endemic regions, as the common transmission route is the ingestion of water or food contaminated with the faeces of chronic carriers (Bhan et al. Citation2005). About 4% of patients with enteric fever, predominantly infants, elderly people and women, may become chronic carriers (Gonzalez-Escobedo et al. Citation2011). In contrast, the carrier state of NTS is less frequent, with an occurrence rate of 0.1% in patients with non-typhoidal salmonellosis. This is because the primary reservoir of NTS is animals, instead of humans (Hohmann Citation2001).
Epidemiology
NTS infections, which cause self-limited illness, are the most common Salmonella infections and occur worldwide. In contrast, enteric fever, caused by typhoid Salmonella, is associated with a high morbidity and mortality rate and occurs predominantly in underdeveloped countries (Hardy Citation2004).
Epidemiology for enteric fever
In 2000, the incidence of enteric fever was estimated to be 22 million cases resulting in 200,000 deaths worldwide, predominantly in underdeveloped countries (Crump et al. Citation2004). The incidence and mortality rate of enteric fever vary from region to region, but the mortality rate can be as high as 7% in spite of antibiotic therapy.
Enteric fever is endemic in many regions of the African and Asian continents as well as countries such as in Europe, South and Central America, and the Middle East. The incidence of enteric fever in the USA and some European countries is low, with the total number of Salmonella cases being less than 10 per 100,000 annually. Most of the cases reported in these countries are related to travel, with the disease being imported by foreigners or travellers returning from Africa, India or Pakistan (Molbak et al. Citation2002; Cooke et al. Citation2007). Israel has a very low incidence of enteric fever and this has further reduced from 0.42 to 0.23 cases per 100,000 from 1995 to 2003. However, the pattern of the causative organism reflects an increasing number of cases of S. Paratyphi, with this organism being isolated from 57.4% of the patients reported with enteric fever in Israel (Meltzer et al. Citation2006). This appears to match the worldwide increase in infection caused by S. Paratyphi, especially in Asian countries in which these strains are responsible for more than 50% of the incidence of enteric fever (Woods et al. Citation2006). The increase in S. Paratyphi infection raises concern over the effectiveness of the typhoid fever vaccines in use and highlights the need for more extensive epidemiological study of the pathogen.
Many Asian countries, including China, India, Vietnam, Pakistan and Indonesia, have high incidence rates of enteric fever, exceeding 100 cases per 100,000 population annually. Compared to other Asian countries, Pakistan and India have the highest incidence rates of 451.7 cases and 214.2 cases per 100,000 population, respectively (Ochiai et al. Citation2008). The incidence of enteric fever reported worldwide is actually more of an estimate as investigations of enteric fever are usually conducted on large outbreaks while isolated cases are often underreported. In many developing countries, especially in sub-Saharan Africa, the limited diagnostic resources and proper surveillance tools result in poor characterization of the burden of enteric fever.
In endemic regions, enteric fever occurs more frequently in infants, preschool and school-age children. Epidemiological studies for the past few years show that the annual incidence of enteric fever among children below 5 years old was approximately 25 per 100,000 population in China and Vietnam, while the incidence in India and Pakistan reached up to 450 per 100,000 annually (Mweu & English Citation2008).
Epidemiology for non-typhoid Salmonella infections
Gastroenteritis is the most common Salmonella infection worldwide, accounting for 93.8 million cases which result in 155,000 deaths per year (Majowicz et al. Citation2010). Based on data for 2001–2005 provided by SalmSurv (a foodborne disease surveillance network supported by WHO), the most common isolated serotype responsible for NTS infections worldwide was S. Enteriditis (65%). This was followed by S. Typhimurium and S. Newport, which contributed 12% and 4% of the clinical isolates, respectively (Galanis et al. Citation2006). Salmonella Enteriditis was the most common serotype in Asia, Latin America and Europe, accounting for 38%, 31% and 87% of the clinical isolates, respectively. In Africa, S. Enteriditis and S. Typhimurium were the two most common serotypes reported, occurrring in 26% and 25% of the isolates, respectively. In contrast to the countries mentioned previously, S. Typhimurium (29%) was most frequently reported in clinical isolates in North America, followed by S. Enteriditis (21%) (Galanis et al. Citation2006).
In spite of improvements in hygiene and sanitation, the incidence of NTS infections continues to increase, creating a burden in both industrialized and underdeveloped countries (Majowicz et al. Citation2010). The incidence of NTS-associated disease is estimated to cause 690 cases per 100,000 population in Europe while the incidence of NTS infection in Israel is around 100 cases per 100,000 annually (Weinberger & Keller Citation2005). Invasive NTS is endemic in underdeveloped countries, especially in sub-Saharan Africa, with high occurrence rates in children below 3 years old and human immunodeficiency virus (HIV)-infected patients, and these invasive strains confer a mortality rate up to 25% (Gordon et al. Citation2008). In contrast, the invasive disease caused by NTS is less frequently reported in Asia (Khan et al. Citation2010).
In the USA, data provided by the Foodborne Diseases Active Surveillance Network (FoodNet) show that NTS infections were most commonly reported in that region, with an incidence of 17.6 cases per 100,000 population annually, and these organisms have been reported as being the largest contributor to death statistics (39%) among all foodborne pathogens (Barton Behravesh et al. Citation2011). As mentioned by CDC, the most recent outbreak (2010) in the USA involved the contamination of eggs by S. Enteriditis, resulting in 1939 cases of NTS infections across 16 states. Some common factors associated with the Salmonella outbreaks include incomplete cooking of food products, improper storage and direct contact with raw ingredients (Lynch et al. Citation2006). The food products that are predominantly associated with the outbreaks include animal products such as milk, poultry and eggs, as well as food products such as chocolate and peanut butter ().
Table 1. Selected major outbreaks of Salmonella spp. from 2002 to 2014.
Unlike typhoid Salmonella, animals are the major reservoir of NTS. The transmission of NTS infection to humans can occur through the ingestion of food or water contaminated with infected animals’ waste, direct contact with infected animals or consumption of infected food animals. The worldwide incidence rate of NTS infection is high as the strains can be found naturally in the environment and in both domestic and wild animals including cats, dogs, amphibians, reptiles and rodents. The diversity of possible reservoirs of infection results in significant challenges for public health authorities to control the infections (Swanson et al. Citation2007; Dione et al. Citation2011).
Antibiotic resistance
The emergence of antimicrobial resistance in Salmonella strains is a serious health problem worldwide (Chiu et al. Citation2002). In the early 1960s, the first incidence of Salmonella resistance to a single antibiotic, namely chloramphenicol, was reported (Montville & Matthews Citation2008). Since then, the frequency of isolation of Salmonella strains with resistance towards one or more antimicrobial agents has increased in many countries, including the USA, the UK and Saudi Arabia (Yoke-Kqueen et al. Citation2008). Antimicrobial agents such as ampicillin, chloramphenicol and trimethoprim–sulfamethoxazole are used as the traditional first line treatments for Salmonella infections. Salmonella spp. resistant towards these agents are referred to as multi-drug resistant (MDR).
For many years, the phenotypic trait of MDR was widely distributed among S. Typhi and, at a lower rate, among S. Paratyphi (Rowe et al. Citation1997). Africa and Asia are two continents with a high isolation frequency of S. Typhi displaying MDR phenotype. In a surveillance study conducted in five Asian countries, India, Pakistan and Vietnam had higher rates of MDR isolates of S. Typhi than Indonesia and China (Ochiai et al. Citation2008). Other reports present similar data, with a high rate of MDR isolates of S. Typhi in Pakistan, India, Nepal and Vietnam, while in China, Indonesia and Laos the incidence rate of MDR S. Typhi is relatively low (Chuang et al. Citation2009).
With the emergence of resistance towards traditional antibiotics, fluoroquinolones and extended-spectrum cephalosporins have been introduced as the antimicrobial agents of choice in treating MDR S. Typhi (Sood et al. Citation1999). However, reports show an increase in the number of cases with typhoid Salmonella developing resistance towards fluoroquinolones. In countries with a higher incidence of MDR isolates, S. Paratyphi displays a higher level of resistance towards fluoroquinolones compared to S. Typhi (Hasan et al. Citation2008). Nalidixic acid resistance, which is used as an indicator of reduced susceptibility of ciprofloxacin and other fluoroquinolones, is displayed by isolates from Pakistan, India and Vietnam, with high incidence rates of 59%, 57% and 44%, respectively (Ochiai et al. Citation2008).
As for NTS, the number of strains developing MDR phenotype has increased in many countries since the first emergence of MDR S. Typhimurium DT104 strains in 1990 (Helms et al. Citation2005). Based on data from 2005 to 2006 presented by the National Antimicrobial Resistance Monitoring System (NARMS), 84% of clinical isolates of NTS displayed MDR phenotype and 4.1% of the isolates had reduced susceptibility to cephalosporins in the USA. NARMS presented data (from 1996–2007) which are more comprehensive, reporting the emergence of NTS isolates that are resistant to nalidixic acid and ceftriaxone. This phenomenon has raised concern among public health authorities regarding both clinical management and prevention of the infection (Crump et al. Citation2011). A surveillance study on 135,000 clinical isolates of NTS was conducted in Europe from 2000 to 2004, and the data showed that 15% of the isolates displayed MDR phenotype and 20% of the isolates were resistant to nalidixic acid (Meakins et al. Citation2008).
Spread of resistance
The emergence of Salmonella with antimicrobial resistance is mainly promoted by the use of antibiotics in animal feed to promote the growth of food animals, and in veterinary medicine to treat bacterial infections in those animals (Hyeon et al. Citation2011). This poses a high risk of zoonotic disease with the transmission of MDR Salmonella strains from animals to humans via the ingestion of food or water contaminated with the animals’ faeces, direct contact or the consumption of infected food animals (Holmberg et al. Citation1984). Moreover, MDR Salmonella strains were found in some exotic pet animals such as tortoises and turtles, as well as their water environment, and this could result in a higher risk of zoonotic infections in humans through direct contact with these animals (Trust & Bartlett Citation1979; Shane et al. Citation1990).
Mechanisms of resistance
Studies show that the serotypes of Salmonella displaying MDR phenotype have the ability to generate various types of hybrid plasmids. The majority of the gene cassettes located within these plasmids consist of resistance genes that confer the antimicrobial resistance property of the serotypes against traditional antibiotics such as chloramphenicol, tetracycline, ampicillin and streptomycin (Guerra et al. Citation2001, Citation2002). The emergence of Salmonella serotypes with reduced ciprofloxacin susceptibility is a result of chromosomal mutation at the quinolone resistance-determining regions of the gyrA gene (Chiu et al. Citation2002). Some serotypes of Salmonella have begun to develop resistance towards broad-spectrum cephalosporins as a result of mutated genes that encode for extended-spectrum β-lactamases, hydrolysing antibiotics with β-lactam rings such as cephalosporin and cephamycins (Carattoli et al. Citation2002).
Clinical relevance
The development of multi-drug resistance in the serotypes of Salmonella has a significant impact on the antibiotic treatment of Salmonella infections. Infections that involve the invasive serotypes are often life threatening and require effective antibiotic treatment. Quinolones and third generation cephalosporins have been the antibiotics of choice in treating infections with MDR Salmonella (Karon et al. Citation2007). However, the emergence of Salmonella serotypes resistant to quinolones and cephalosporin poses a new challenge in treating infected patients, and the lack of an effective antibiotic therapy may lead to an increase in the morbidity and mortality rates.
The emergence of MDR Salmonella has also resulted in the increased severity of bacterial infections in humans and animals. Epidemiological studies show that MDR Salmonella strains cause more severe or prolonged syndromes than susceptible strains, implying that the MDR strains are more virulent than the susceptible ones (Travers & Barza Citation2002). Data show that patients infected with MDR Salmonella strains are more ill and septic at the onset of the disease, and the illness is typically accompanied by high fever, enlargement of the spleen and liver, and abdominal swelling (Buch et al. Citation1994).
Prevention
Contaminated water or food is the major transmission route of enteric fever. Historically, the USA and Western Europe were endemic for enteric fever; however, the incidence of Salmonella infection decreased significantly with proper food and water sanitation, pasteurization of milk and other dairy products, and elimination of the use of human faeces in food production. A decrease in the incidence of Salmonella infections was observed in Latin America in parallel with the introduction of sanitation measures (Crump et al. Citation2004). At present, preventive measures for enteric fever concentrate on access to safe water and food, proper sanitation and the use of typhoid vaccines.
Ensuring the safety of water for consumption is the main goal for the elimination of possible transmission routes of typhoid Salmonella as well as NTS. This important measure has been successfully achieved in industrialized countries, such as in Europe and the USA, but not in developing and underdeveloped countries (Clasen et al. Citation2007). Besides water, Salmonella spp. can be found in a variety of foods, predominantly in poultry, eggs and dairy products. Proper handling and cooking of food are measures proposed to eradicate the bacterial contamination of food. In many countries, food irradiation has been greatly promoted owing to its effectiveness in reducing the risk of food contamination. Approved by several public health agencies, including the WHO and CDC, the technology of food irradiation is only partially utilized in some areas in Europe and the USA because of the risk of radioactivity (Osterholm & Norgan Citation2004). Vaccination is an effective measure in preventing enteric fever. Inactive parenteral and oral live attenuated vaccines are the two types of vaccine currently approved for the prevention of enteric fever. However, these licensed vaccines are limited to infants and they are not effective in preventing infections caused by S. Paratyphi and NTS (Lin et al. Citation2001). As for NTS, one effective measure is to restrict the inappropriate use of antibiotics in food animals and their feed (Talbot et al. Citation2006).
Conclusion
Salmonella infection remains a distressing public health concern worldwide. The genetic make-up of the Salmonella strains permits their adaptation in various environments, including human, animal and non-animal hosts. This increases the difficulty in eliminating the bacteria. Moreover, the emergence of MDR Salmonella strains poses a great challenge in terms of effective treatment of the infections caused by these strains. Several preventive measures have been proposed to stop the spread of Salmonella infection, and the restriction of indiscriminate use of antibiotics in food animals is by far one of the most effective measures.
Two vaccines have been approved for the prevention for enteric fever, but no licensed vaccines are available for S. Paratyphi and NTS infection. Further research on the development of vaccines for all Salmonella strains may potentially result in great benefits for affected countries.
Disclosure statement
No potential conflict of interest was reported by the authors.
Additional information
Funding
Related Research Data
References
- Allerberger F, Liesegang A, Grif K, Khaschabi D, Prager R, Danzl J, Hock F, Ottl J, Dierich MP, Berghold C, et al. 2003. Occurrence of Salmonella enterica serovar Dublin in Austria. Wiener medizinische Wochenschrift. 153:148–152. doi: https://doi.org/10.1046/j.1563-258X.2003.03015.x
- Arii J, Tanabe Y, Miyake M, Mukai T, Matsuzaki M, Niinomi N, Watanabe H, Yokota Y, Kohno Y, Noda M. 2002. Clinical and pathologic characteristics of nontyphoidal salmonella encephalopathy. Neurology. 58(11):1641–1645. doi: https://doi.org/10.1212/WNL.58.11.1641
- Bakowski MA, Braun V, Brumell JH. 2008. Salmonella-containing vacuoles: directing traffic and nesting to grow. Traffic. 9:2022–2031. doi: https://doi.org/10.1111/j.1600-0854.2008.00827.x
- Barlow M, Hall BG. 2002. Origin and evolution of the AmpC beta-lactamases of Citrobacter freundii. Antimicrob Agents Chemother. 46:1190–1198. doi: https://doi.org/10.1128/AAC.46.5.1190-1198.2002
- Barton Behravesh C, Jones TF, Vugia DJ, Long C, Marcus R, Smith K, Thomas S, Zansky S, Fullerton KE, Henao OL, et al. 2011. Deaths associated with bacterial pathogens transmitted commonly through food: foodborne diseases active surveillance network (FoodNet), 1996–2005. The Journal of Infectious Diseases. 204(2):263–267. doi: https://doi.org/10.1093/infdis/jir263
- Bhan MK, Bahl R, Bhatnagar S. 2005. Typhoid and paratyphoid fever. Lancet. 366(2):749–762. doi: https://doi.org/10.1016/S0140-6736(05)67181-4
- Brenner FW, Villar RG, Angulo FJ, Tauxe R, Swaminathan B. 2000. Salmonella nomenclature. J Clin Microbiol. 38:2465–2467.
- Buch NA, Hassan MU, Kakroo DK. 1994. Enteric fever – a changing sensitivity pattern, clinical profile and outcome. Indian Pediatrics. 31:981–985.
- Carattoli A, Tosini F, Giles WP, Rupp ME, Hinrichs SH, Angulo FJ, Barrett TJ, Fey PD. 2002. Characterization of plasmids carrying CMY-2 from expanded-spectrum cephalosporin-resistant Salmonella strains isolated in the United States between 1996 and 1998. Antimicrob. Agents Chemother. 46:1269–1272. doi: https://doi.org/10.1128/AAC.46.5.1269-1272.2002
- Chiu CH, Wu TL, Su LH, Chu C, Chia JH, Kuo AJ, Chien MS, Lin TY. 2002. The emergence in Taiwan of fluoroquinolone resistance in Salmonella enterica serotype choleraesuis. The New England Journal of Medicine. 346:413–419. doi: https://doi.org/10.1056/NEJMoa012261
- Chuang CH, Su LH, Perera J, Carlos C, Tan BH, Kumarasinghe G, So T, Van PH, Chongthaleong A, Hsueh PR, et al. 2009. Surveillance of antimicrobial resistance of Salmonella enterica serotype Typhi in seven Asian countries. Epidemiology and Infection. 137:266–269. doi: https://doi.org/10.1017/S0950268808000745
- Clasen T, Schmidt WP, Rabie T, Roberts I, Cairncross S. 2007. Interventions to improve water quality for preventing diarrhoea: systematic review and meta-analysis. British Medical Journal. 334(14):782. doi: https://doi.org/10.1136/bmj.39118.489931.BE
- Connor BA, Schwartz E. 2005. Typhoid and paratyphoid fever in travellers. The Lancet Infectious Diseases. 5:623–628. doi: https://doi.org/10.1016/S1473-3099(05)70239-5
- Centers for Disease Control and Prevention. 2007. Multistate outbreak of Salmonella serotype Tennessee infections associated with peanut butter – United States, 2006–2007. MMWR Morbidity and mortality weekly report. 56:521–524.
- Centers for Disease Control and Prevention. 2010. Investigation update: multistate outbreak of human Salmonella Montevideo infections.
- Centers for Disease Control and Prevention. 2012. Multistate outbreak of human salmonella infections linked to live poultry in backyard flocks (final update). Atlanta, GA, USA Page last updated.26.
- Centers for Disease Control and Prevention. 2013. Multistate outbreak of Salmonella Bareilly and Salmonella Nchanga infections associated with a raw scraped ground tuna product (final update); July 2012. Avialable from: http://www.cdc.gov/salmonella/bareilly-04-12/index.html.
- Cooke FJ, Day M, Wain J, Ward LR, Threlfall EJ. 2007. Cases of typhoid fever imported into England, Scotland and Wales (2000–2003). Transactions of the Royal Society of Tropical Medicine and Hygiene. 101:398–404. doi: https://doi.org/10.1016/j.trstmh.2006.07.005
- Crump JA, Kretsinger K, Gay K, Hoekstra RM, Vugia DJ, Hurd S, Segler SD, Megginson M, Luedeman LJ, Shiferaw B, et al. 2008. Clinical response and outcome of infection with Salmonella enterica serotype Typhi with decreased susceptibility to fluoroquinolones: a United States foodnet multicenter retrospective cohort study. Antimicrob. Agents Chemother. 52:1278–1284. doi: https://doi.org/10.1128/AAC.01509-07
- Crump JA, Luby SP, Mintz ED. 2004. The global burden of typhoid fever. Bulletin of the World Health Organization. 82:346–353.
- Crump JA, Medalla FM, Joyce KW, Krueger AL, Hoekstra RM, Whichard JM, Barzilay EJ. 2011. Antimicrobial resistance among invasive nontyphoidal Salmonella enterica isolates in the United States: national antimicrobial resistance monitoring system, 1996 to 2007. Antimicrob. Agents Chemother. 55:1148–1154. doi: https://doi.org/10.1128/AAC.01333-10
- Dione MM, Ikumapayi UN, Saha D, Mohammed NI, Geerts S, Ieven M, Adegbola RA, Antonio M. 2011. Clonal differences between non-typhoidal Salmonella (NTS) recovered from children and animals living in close contact in the Gambia. PLoS Neglected Tropical Diseases. 5:e1148. doi: https://doi.org/10.1371/journal.pntd.0001148
- Galanis E, Lo Fo Wong DM, Patrick ME, Binsztein N, Cieslik A, Chalermchikit T, Aidara-Kane A, Ellis A, Angulo FJ, Wegener HC. 2006. Web-based surveillance and global Salmonella distribution, 2000–2002. Emerging Infectious Diseases. 12:381–388. doi: https://doi.org/10.3201/eid1205.050854
- Gillespie IA, O'Brien SJ, Adak GK, Ward LR, Smith HR. 2005. Foodborne general outbreaks of Salmonella Enteritidis phage type 4 infection, England and Wales, 1992–2002: where are the risks? Epidemiology and Infection. 133:759–801. doi: https://doi.org/10.1017/S0950268805003742
- Gonzalez-Escobedo G, Marshall JM, Gunn JS. 2011. Chronic and acute infection of the gall bladder by Salmonella Typhi: understanding the carrier state. Nat Rev Microbiol. 9:9–14. doi: https://doi.org/10.1038/nrmicro2490
- Gordon MA, Graham SM, Walsh AL, Wilson L, Phiri A, Molyneux E, Zijlstra EE, Heyderman RS, Hart CA, Molyneux ME. 2008. Epidemics of invasive Salmonella enterica serovar enteritidis and S. enterica Serovar typhimurium infection associated with multidrug resistance among adults and children in Malawi. Clinical Infectious Diseases. 46(7):963–969. doi: https://doi.org/10.1086/529146
- Grassl GA, Finlay BB. 2008. Pathogenesis of enteric Salmonella infections. Current Opinion in Gastroenterology. 24:22–26. doi: https://doi.org/10.1097/MOG.0b013e3282f21388
- Guerra B, Soto S, Helmuth R, Mendoza MC. 2002. Characterization of a self-transferable plasmid from Salmonella enterica serotype typhimurium clinical isolates carrying two integron-borne gene cassettes together with virulence and drug resistance genes. Antimicrob Agents Chemother. 46:2977–2981. doi: https://doi.org/10.1128/AAC.46.9.2977-2981.2002
- Guerra B, Soto SM, Arguelles JM, Mendoza MC. 2001. Multidrug resistance is mediated by large plasmids carrying a class 1 integron in the emergent Salmonella enterica serotype [4,5,12:i:-]. Antimicrob Agents Chemother. 45:1305–1308. doi: https://doi.org/10.1128/AAC.45.4.1305-1308.2001
- Guibourdenche M, Roggentin P, Mikoleit M, Fields PI, Bockemuhl J, Grimont PA, Weill FX. 2010. Supplement 2003–2007 (No. 47) to the White–Kauffmann–Le Minor scheme. Res Microbiol. 161:26–29. doi: https://doi.org/10.1016/j.resmic.2009.10.002
- Guiney DG, Fierer J. 2011. The role of the spv genes in Salmonella pathogenesis. Frontiers in Microbiology. 2:129. doi: https://doi.org/10.3389/fmicb.2011.00129
- Gulig PA, Danbara H, Guiney DG, Lax AJ, Norel F, Rhen M. 1993. Molecular analysis of spv virulence genes of the Salmonella virulence plasmids. Mol Microbiol. 7:825–830. doi: https://doi.org/10.1111/j.1365-2958.1993.tb01172.x
- Hansen-Wester I, Stecher B, Hensel M. 2002. Type III secretion of Salmonella enterica serovar Typhimurium translocated effectors and SseFG. Infect Immun. 70:1403–1409. doi: https://doi.org/10.1128/IAI.70.3.1403-1409.2002
- Hardy A. 2004. Salmonella: a continuing problem. Postgraduate Medical Journal. 80:541–545. doi: https://doi.org/10.1136/pgmj.2003.016584
- Hasan R, Zafar A, Abbas Z, Mahraj V, Malik F, Zaidi A. 2008. Antibiotic resistance among Salmonella enterica serovars Typhi and Paratyphi A in Pakistan (2001–2006). J Infect Dev Countr. 2:289–294.
- Havelaar AH, Ivarsson S, Löfdahl M, Nauta MJ. 2013. Estimating the true incidence of campylobacteriosis and salmonellosis in the European Union, 2009. Epidemiology & Infection. 141:293–302. doi: https://doi.org/10.1017/S0950268812000568
- Helms M, Ethelberg S, Molbak K. 2005. International Salmonella Typhimurium DT104 infections, 1992–2001. Emerging Infectious Diseases. 11:859–867. doi: https://doi.org/10.3201/eid1106.041017
- Hohmann EL. 2001. Nontyphoidal salmonellosis. Clinical Infectious Disease. 15(32):263–269.
- Holmberg SD, Osterholm MT, Senger KA, Cohen ML. 1984. Drug-resistant Salmonella from animals fed antimicrobials. The New England Journal of Medicine. 311(10):617–622. doi: https://doi.org/10.1056/NEJM198409063111001
- Hu L, Kopecko DJ. 2003. Typhoid Salmonella. In: Millotis MD and Bier JW, editor. International handbook of foodborne pathogens. New York: Marcel Dekker, Inc; p. 151–165.
- Hyeon JY, Chon JW, Hwang IG, Kwak HS, Kim MS, Kim SK, Choi IS, Song CS, Park C, Seo KH. 2011. Prevalence, antibiotic resistance, and molecular characterization of Salmonella serovars in retail meat products. J Food Prot. 74:161–166. doi: https://doi.org/10.4315/0362-028X.JFP-10-327
- Karon AE, Archer JR, Sotir MJ, Monson TA, Kazmierczak JJ. 2007. Human multidrug-resistant Salmonella newport infections, Wisconsin, 2003–2005. Emerging Infectious Diseases. 13:1777–1780. doi: https://doi.org/10.3201/eid1311.061138
- Khan MI, Ochiai RL, von Seidlein L, Dong B, Bhattacharya SK, Agtini MD, Bhutta ZA, Do GC, Ali M, Kim DR, et al. 2010. Non-typhoidal Salmonella rates in febrile children at sites in five Asian countries. Tropical Medicine & International Health: TM & IH. 15:960–963. doi: https://doi.org/10.1111/j.1365-3156.2010.02553.x
- Kothari A, Amit P, Tulsi DC. 2008. The burden of enteric fever. The Journal of Infection in Developing Countries. 2:253–259. doi: https://doi.org/10.3855/jidc.196
- Kuvandik C, Karaoglan I, Namiduru M, Baydar I. 2009. Predictive value of clinical and laboratory findings in the diagnosis of the enteric fever. The New Microbiologica. 32:25–30.
- Lin FY, Ho VA, Khiem HB, Trach DD, Bay PV, Thanh TC, Kossaczka Z, Bryla DA, Shiloach J, Robbins JB, et al. 2001. The efficacy of a Salmonella typhi Vi conjugate vaccine in two-to-five-year-old children. The New England Journal of Medicine. 344(17):1263–1269. doi: https://doi.org/10.1056/NEJM200104263441701
- Lynch M, Painter J, Woodruff R, Braden C. 2006. Surveillance for foodborne-disease outbreaks – United States, 1998–2002. Morbidity and Mortality Weekly Report Surveillance Summaries (Washington, DC: 2002). 10(55):1–42.
- Majowicz SE, Musto J, Scallan E, Angulo FJ, Kirk M, O'Brien SJ, Jones TF, Fazil A, Hoekstra RM. 2010. The global burden of nontyphoidal Salmonella gastroenteritis. Clinical Infectious Diseases. 50(6):882–889. doi: https://doi.org/10.1086/650733
- Matyas B, Cronquist A, Cartter M, Tobin-D'Angelo M, Blythe D, Smith K, Lathrop S, Morse D, Cieslak P, Dunn J et al. 2010. Preliminary FoodNet data on the incidence of infection with pathogens transmitted commonly through food – 10 states, 2009. MMWR Morbidity and Mortality Weekly Report. 59:418–422.
- McQuiston JR, Fields PI, Tauxe RV, Logsdon JM Jr. 2008. Do Salmonella carry spare tyres? Trends in Microbiology. 16:142–148. doi: https://doi.org/10.1016/j.tim.2008.01.009
- Meakins S, Fisher IS, Berghold C, Gerner-Smidt P, Tschape H, Cormican M, Luzzi I, Schneider F, Wannett W, Coia J, et al. 2008. Antimicrobial drug resistance in human nontyphoidal Salmonella isolates in Europe 2000–2004: a report from the Enter-net International Surveillance Network. Microbial Drug Resistance (Larchmont, NY). 14:31–35. doi: https://doi.org/10.1089/mdr.2008.0777
- Meltzer E, Yossepowitch O, Sadik C, Dan M, Schwartz E. 2006. Epidemiology and clinical aspects of enteric fever in Israel. The American Journal of Tropical Medicine and Hygiene. 74:540–545.
- Molbak K, Gerner-Smidt P, Wegener HC. 2002. Increasing quinolone resistance in Salmonella enterica serotype Enteritidis. Emerging Infectious Diseases. 8:514–515. doi: https://doi.org/10.3201/eid0805.010288
- Monack DM, Mueller A, Falkow S. 2004. Persistent bacterial infections: the interface of the pathogen and the host immune system. Nat Rev Microbiol. 2:747–765. doi: https://doi.org/10.1038/nrmicro955
- Montville TJ, Matthews KR. 2008. Food microbiology: an introduction. 2nd ed. Washington, USA: ASM Press.
- Mweu E, English M. 2008. Typhoid fever in children in Africa. Tropical medicine & International Health. 13:532–540. doi: https://doi.org/10.1111/j.1365-3156.2008.02031.x
- Ochiai RL, Acosta CJ, Danovaro-Holliday MC, Baiqing D, Bhattacharya SK, Agtini MD, Bhutta ZA, Canh do G, Ali M, Shin S, et al. 2008. A study of typhoid fever in five Asian countries: disease burden and implications for controls. Bulletin of the World Health Organization. 86:260–268. doi: https://doi.org/10.2471/BLT.06.039818
- Osterholm MT, Norgan AP. 2004. The role of irradiation in food safety. The New England Journal of Medicine. 350(18):1898–1901. doi: https://doi.org/10.1056/NEJMsb032657
- OzFoodNet. 2006. OzFoodNet quarterly report, 1 January to 31 March 2006. Communicable Diseases Intelligence. 30:228–232.
- Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. 2002. Typhoid fever. The New England Journal of Medicine. 347:1770–1782. doi: https://doi.org/10.1056/NEJMra020201
- Patel TA, Armstrong M, Morris-Jones SD, Wright SG, Doherty T. 2010. Imported enteric fever: case series from the hospital for tropical diseases, London, United Kingdom. The American Journal of Tropical Medicine and Hygiene. 82:1121–1126. doi: https://doi.org/10.4269/ajtmh.2010.10-0007
- Popoff MY, Bockemühl J, Gheesling LL. 2003. Supplement 2001 (no. 45) to the Kauffmann–White scheme. Res Microbiol. 154(3):173–174. doi: https://doi.org/10.1016/S0923-2508(03)00025-1
- Pui CF, Wong WC, Chai LC, Nillian E, Ghazali FM, Cheah YK, Nakaguchi Y, Nishibuchi M, Radu S. 2011. Simultaneous detection of Salmonella spp., Salmonella Typhi and Salmonella Typhimurium in sliced fruits using multiplex PCR. Food Control. 22:337–342. doi: https://doi.org/10.1016/j.foodcont.2010.05.021
- Reeves MW, Evins GM, Heiba AA, Plikaytis BD, Farmer JJ 3rd. 1989. Clonal nature of Salmonella typhi and its genetic relatedness to other salmonellae as shown by multilocus enzyme electrophoresis, and proposal of Salmonella bongori comb. nov. J Clin Microbiol. 27:313–320.
- Rowe B, Ward LR, Threlfall EJ. 1997. Multidrug-resistant Salmonella typhi: a worldwide epidemic. Clinical Infectious Diseases. 24:S106–S109. doi: https://doi.org/10.1093/clinids/24.Supplement_1.S106
- Scallan E, Hoekstra RM, Angulo FJ, Tauxe RV, Widdowson MA, Roy SL, Jones JL, Griffin PM. 2011. Foodborne illness acquired in the United States – major pathogens. Emerging Infectious Diseases. 17:7–15. doi: https://doi.org/10.3201/eid1701.P11101
- Shane SM, Gilbert R, Harrington KS. 1990. Salmonella colonization in commercial pet turtles (Pseudemys scripta elegans). Epidemiology and Infection. 105:307–316. doi: https://doi.org/10.1017/S0950268800047907
- Sharifa Ezat WP, Netty D, Sangaran G. 2013. Paper review of factors, surveillance and burden of food borne disease outbreak in Malaysia. Malaysian journal of public Health Medicine. 13:98–105.
- Sheorey H, Darby J. 2008. Searching for Salmonella. Australian Family Physician. 37:806–810.
- Shimoni Z, Pitlik S, Leibovici L, Samra Z, Konigsberger H, Drucker M, Agmon V, Ashkenazi S, Weinberger M. 1999. Nontyphoid Salmonella bacteremia: age-related differences in clinical presentation, bacteriology, and outcome. Clinical Infectious Diseases. 28:822–827. doi: https://doi.org/10.1086/515186
- Silva J, Leite D, Fernandes M, Mena C, Gibbs PA, Teixeira P. 2011. Campylobacter spp. as a foodborne pathogen: a review. Frontiers in Microbiology. 2.
- Sood S, Kapil A, Das B, Jain Y, Kabra SK. 1999. Re-emergence of chloramphenicol-sensitive Salmonella typhi. Lancet. 353(9160):1241–1242. doi: https://doi.org/10.1016/S0140-6736(99)00637-6
- Swanson SJ, Snider C, Braden CR, Boxrud D, Wunschmann A, Rudroff JA, Lockett J, Smith KE. 2007. Multidrug-resistant Salmonella enterica serotype Typhimurium associated with pet rodents. The New England Journal of Medicine. 356(1):21–28. doi: https://doi.org/10.1056/NEJMoa060465
- Takaya A, Suzuki M, Matsui H, Tomoyasu T, Sashinami H, Nakane A, Yamamoto T. 2003. Lon, a stress-induced ATP-dependent protease, is critically important for systemic Salmonella enterica serovar typhimurium infection of mice. Infect Immun. 71:690–696. doi: https://doi.org/10.1128/IAI.71.2.690-696.2003
- Talbot EA, Gagnon ER, Greenblatt J. 2006. Common ground for the control of multidrug-resistant Salmonella in ground beef. Clinical Infectious Diseases. 15(42):1455–1462.
- Thielman NM, Guerrant RL. 2004. Acute infectious diarrhea. The New England Journal of Medicine. 350:38–47. doi: https://doi.org/10.1056/NEJMcp031534
- Travers K, Barza M. 2002. Morbidity of infections caused by antimicrobial-resistant bacteria. Clinical Infectious Diseases. 34:S131–S134. doi: https://doi.org/10.1086/340251
- Trust TJ, Bartlett KH. 1979. Aquarium pets as a source of antibiotic-resistant salmonellae. Can J Microbiol. 25:535–541. doi: https://doi.org/10.1139/m79-078
- Wattiau P, Boland C, Bertrand S. 2011. Methodologies for Salmonella enterica subsp. enterica subtyping: gold standards and alternatives. Applied and Environmental Microbiology. 77:7877–7885. doi: https://doi.org/10.1128/AEM.05527-11
- Weinberger M, Keller N. 2005. Recent trends in the epidemiology of non-typhoid Salmonella and antimicrobial resistance: the Israeli experience and worldwide review. Current Opinion in Infectious Diseases. 18:513–521. doi: https://doi.org/10.1097/01.qco.0000186851.33844.b2
- Werber D, Dreesman J, Feil F, van Treeck U, Fell G, Ethelberg S, Hauri A, Roggentin P, Prager R, Fisher I, et al. 2005. International outbreak of Salmonella Oranienburg due to German chocolate. BMC Infectious Diseases. 5:7. doi: https://doi.org/10.1186/1471-2334-5-7
- Woods CW, Murdoch DR, Zimmerman MD, Glover WA, Basnyat B, Wolf L, Belbase RH, Reller LB. 2006. Emergence of Salmonella enterica serotype Paratyphi A as a major cause of enteric fever in Kathmandu, Nepal. Transactions of the Royal Society of Tropical Medicine and Hygiene. 100:1063–1067. doi: https://doi.org/10.1016/j.trstmh.2005.12.011
- Woods DF, Reen FJ, Gilroy D, Buckley J, Frye JG, Boyd EF. 2008. Rapid multiplex PCR and real-time TaqMan PCR assays for detection of Salmonella enterica and the highly virulent serovars Choleraesuis and Paratyphi C. J Clin Microbiol. 46:4018–4022. doi: https://doi.org/10.1128/JCM.01229-08
- Yoke-Kqueen C, Learn-Han L, Noorzaleha AS, Son R, Sabrina S, Jiun-Horng S, Chai-Hoon K. 2008. Characterization of multiple-antimicrobial-resistant Salmonella enterica Subsp. enterica isolated from indigenous vegetables and poultry in Malaysia. Lett Appl Microbiol. 46:318–324. doi: https://doi.org/10.1111/j.1472-765X.2007.02311.x