
ABSTRACT
Early intervention and risk stratification solutions for lung cancer are limited by our understanding of how carcinogenesis transforms the pre-invasive epithelium and its microenvironment before the carcinoma stage. We describe the sequence of molecular and cellular changes leading to cancer formation and the co-evolution of the earliest immune response. We revealed that immune sensing, infiltration and activation of immune cells, immune escape, and microenvironment reorganization occur early in pre-cancer. These findings urge the need for broadening the scope of the established immunotherapy approaches toward prophylactic cancer treatment and preventive intervention. Leveraging the immune contexture and the mechanisms of immune modulation for individuals at risk of developing cancer and further to the general population will allow for early detection, chemoprevention, and risk stratification in the near future.
The window of opportunity for significantly reducing cancer mortality and potentially curing lung cancer lies in early diagnosis and early intervention. Significant effort has been centered on monitoring high-risk groups;Citation1 however, solutions for biomarker screening for early detection, chemopreventive treatment options for cancer interception, and risk stratification for avoiding overtreatment are needed. Squamous cell carcinogenesis occurs in multiple stages of transformation from normal to preinvasive (hyperplasia, metaplasia, dysplasia, and carcinoma in situ) to malignant tissue. Therefore, we analyzed nine sequential stages of lung squamous cell carcinoma development in Mascaux et al.,Citation2 seeking to identify targets and early points of intervention for reverting or intercepting the process of carcinogenesis before invasion occurs.
Timing the molecular and cellular changes in lung carcinogenesis
As normal cells transform progressively to a malignant state, they acquire fundamental oncogenic traits. Using gene expression and multiplexed imaging to profile 122 autofluorescence bronchoscopy biopsies from 77 patients, we showed that these tumor-intrinsic hallmarks occurred in a deterministic temporal order and followed specific trajectories of change.Citation2 From the earliest stages of transformation, the bronchial preinvasive epithelium acquired and sustained proliferation signaling through a continuous increase in gene expression associated with cell cycle pathways and DNA damage response. Metabolic reprogramming also manifested early through a continuous decrease in adipogenesis, an initial upregulation of fatty acid metabolism and oxidative phosphorylation in low-grade lesions consistent with previous findings,Citation3 likely due to a shift in cellular function from secretory to protective keratinization, previously described for mRNA expression.Citation4 However, these metabolic pathways were then down-regulated later in high-grade premalignancy and cancer, in line with the gradual increase of hypoxia-associated gene expression from normal to malignant cells. High-grade lesions were also distinguished by remodeling of their microenvironment. The only cancer hallmark reserved uniquely for the invasive stage of carcinogenesis was epithelial–mesenchymal transition. Timing these molecular changes could help intercept the process of carcinogenesis by targeting cancer hallmark processes at a key pivotal high-risk development stage ().
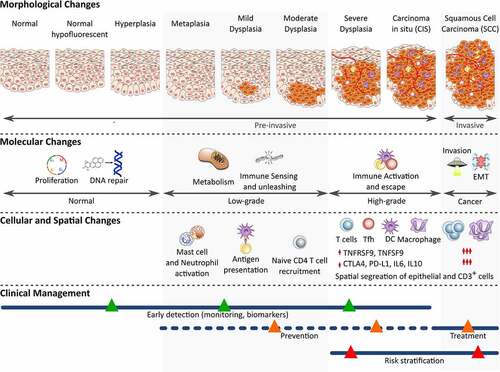
Figure 1. Timing the molecular, cellular, and spatial microenvironment changes during lung squamous premalignancy
Immune escape and microenvironment reorganization occurs early in precancer
We demonstrated that carcinogenesis was a process of co-evolution of the premalignant bronchial epithelium and the immune response. Immune sensing and unleashing were at the frontline against the earliest epithelial cell transformations in low-grade lesions, involving activation of mast cells and neutrophils, antigen processing and presentation, and the likely recruitment of naive CD4 T cells. As cells transform into high-grade lesions, the second line of immune attack deploys T cell activation, macrophage polarization (M1 macrophages), neutrophils and pan-myeloid cell recruitment. High-grade premalignancy and cancer are characterized by co-regulation of innate and adaptive immunity components, including activated T cells, memory B cells, follicular T helper cells, activated NK cells, and dendritic cells. In addition to changes in the cellular composition of the preinvasive microenvironment, there were clear shifts in immune status from naive to activated and from immature to memory cell states at specific milestones of carcinogenesis. Given that antigen recognition and activation of effector immune cells occur early in carcinogenesis, it remains to be investigated whether the immunoediting process shapes the genome and prunes immunogenic mutations in clonal expansions early on in pre-malignant transformation similarly to metastatic transformation, where we observed that nonimmunoedited tumor clones persisted, disseminated, and recurred.Citation5 If determined that immune selection and clonal immunoediting also occur before cancer initiation,Citation6 the presence of nonimmunoedited tumor clones in precancer would render the fate of a preinvasive lesion a progressive cancer.
Strikingly, we observed that immune escape occurred even before cancer at the critical transition point to tumor invasion. High-grade precancer was distinguished by an up-regulation of co-inhibitory immune checkpoint molecules (IDO1, PD-L1, CTLA4, TIGIT, and TIM3) and suppressive interleukins (IL6 and IL10). Importantly, bronchial epithelial cells were frequently spatially separated from CD3+ T cells in high-grade lesions, another escape mechanism from immune surveillance manifested through remodeling of the preinvasive microenvironment. The predictive potential of the spatial separation of the bronchial epithelium from immune effector cells and the involvement of the stromal compartment, such as extracellular matrix, fibroblasts, and pericytes, remains to be determined.
Leveraging immunomodulatory therapies for early detection and chemoprevention
Timing the events in the evolution of the immune response relative to the morphological transformation offers the possibility to identify biomarkers and employ them at opportune moments for early detection using less invasive approaches such as serological testing, nasal or buccal swaps, and even radiomic signatures and deep learning on CT scans for inferring immune compositions.Citation7
Furthermore, the finding that immune escape occurs before tumors can invade and disseminate promises great potential in scaling immunomodulatory therapeutic optionsCitation8 to intervene before reaching the largely incurable stage – cancer. Immunotherapy has transformed the clinical management of many cancer types, including those with immune checkpoint blockade in advanced non-small cell lung cancer.Citation6 The imminent question is whether we can leverage immunological advances and translate them not only to early cancer stages but further to the premalignant stage, to broaden the scope of immunotherapy toward secondary prevention approaches for individuals at high risk of development.
We previously demonstrated a spatiotemporal regulation of tumor-infiltrating immune cells, a finding that has profound implications for the development of efficient anti-cancer immunotherapies.Citation9 Expanding anti-cancer therapies, such as peptide-based vaccines,Citation10 DNA-based vaccines,Citation11 monoclonal antibodies,Citation12 oncolytic virus,Citation13 cytokines,Citation14 toll-like receptor agonists,Citation15 to the pre-cancer stage holds great promise. Furthermore, intervention at a localized pre-cancer stage could be very efficient since immune modulation will not face multiverse of immune microenvironment in multiple sites as it is the case for metastases.Citation16
Finally, for optimal, tailored chemopreventive strategies, much work remains to be done on risk assessment and outcome prediction. Recent studies have demonstrated an encouraging predictive potential of molecular and cellular features to distinguish regressive from progressive lesions. Specifically, the presence of M2 over M1 macrophages,Citation17,Citation18 decreased T cell abundance,Citation17–19 higher number of somatic mutations and chromosomal instability,Citation20 impairments in the antigen presenting machineryCitation17,Citation19 in premalignant bronchial lesions have been linked to an increased risk of progression. Moreover, TNFRSF9 (CD137), an important costimulatory molecule for T cell activation, and its high-affinity ligand TNFSF9 (CD137L, 41BBL) were the most distinguishably upregulated molecules in high-grade precancer and cancer.Citation2 Upregulation of CD137L in squamous lung premalignancy has been linked to a lower risk of progression.Citation19 Therefore, CD137 is a promising actionable candidate for promoting a prophylactic immune response by using readily available agonistic anti-CD137.
Exploiting the full potential of the latest findings in the field requires joining international and multidisciplinary expertise, as well as dissemination of data and analyses through interactive and smart interfaces, followed by prospective clinical trials on biomarkers for detection, prediction, and chemoprevention. One such great opportunity lies in the Human Tumor Atlas Network,Citation21 a multi-institutional initiative that projects to generate 3D atlases and multidimensional molecular profiling of precancers and invasive tumors in the coming years. Standardized and consensus immune biomarkers, such as Immunoscore, should be developed for pre-cancer settings.Citation6 Finally, including AI-assisted medical decision-making as a routine clinical modality would be essential to integrate the growing knowledge of morphological, molecular, and cellular transformation in premalignancies and to suggest and guide clinical decisions with respect to the temporal context of the disease.
From the earliest stages of transformation, the bronchial preinvasive epithelium sustained a continuous increase in cell cycle pathways and DNA damage response gene expression, a biphasic change associated with metabolic reprogramming, and immune sensing and unleashing of tissue resident immune cells. At a critical step before invasion in high-grade lesions and to a higher degree in cancer, innate and adaptive immunity cells are recruited, activated, and exhausted, having concomitant expression of co-inhibitory immune checkpoint molecules and suppressive interleukins and CD3 + T cells spatially segregating from the bronchial epithelium. The invasive stage of carcinogenesis was distinguished uniquely by epithelial–mesenchymal transition. EMT is an epithelial–mesenchymal transition. Timing these molecular changes could guide therapeutic targeting and intercepting cancer hallmark processes in the context of the developmental stage. In the clinical management, triangles represent potential points of intervention, and the dotted line represents potentially novel preventive options.
Declaration of interests
MA, CM, and JG have patent applications associated with the immune prognostic biomarkers and immunotherapies in pre-malignant lesions. CM received honoraria for expertise and speaker roles, being on the advisory board or attending meetings, from Boehringer Ingelheim, Bristol-Myers Squibb, AstraZeneca, Roche, Kephren, Pfizer and MSD over the last 5 years. JG is the co-founder of HalioDx biotech company. Immunoscore® a registered trademark from the National Institute of Health and Medical Research (INSERM) licensed to HalioDx.
Acknowledgments
The work was supported by INSERM, the LabEx Immuno-oncology, the Transcan ERAnet European project, the Society for Immunotherapy of Cancer (SITC), Association pour la Recherche contre le Cancer (ARC), Site de Recherche intégrée sur le Cancer (SIRIC) CAncer Research for PErsonalized Medicine (CARPEM), La Ligue contre le Cancer, The Qatar National Research Fund (QNRF) grant number NPRP11S-0121-180351, Assistance publique – Hôpitaux de Paris (AP-HP), HalioDx, Agence Nationale de la Recherche (ANR Grant TERMM ANR-20-CE92-0001), the Fund of Medical Scientific Research (Belgium), the National Fund of Scientific Research-Télévie campaign and the ASBL ‘Les Amis de l’Institut Jules Bordet’, Institut National du Cancer, France (INCa), and the Louis Jeantet Prize foundation. CM was a research fellow at the National Fund for Scientific Research (Belgium) and was supported by a grant from the Louisiana Chapter of the National Lung Cancer Partnership (USA).
Additional information
Funding
References
- De Koning HJ, Van Der Aalst CM, De Jong PA, Scholten ET, Nackaerts K, Heuvelmans MA, Lammers JWJJJ, Weenink C, Yousaf-Khan U, Horeweg N, et al. Reduced Lung-Cancer mortality with volume CT screening in a randomized trial. N Engl J Med. 2020;382(6):503–4. PMID: 31995683. doi:10.1056/NEJMoa1911793.
- Mascaux C, Angelova M, Vasaturo A, Beane J, Hijazi K, Anthoine G, Buttard B, Rothe F, Willard-Gallo K, Haller A, et al. Immune evasion before tumour invasion in early lung squamous carcinogenesis. Nature. 2019;571(7766):570–575. PMID: 31243362. doi:10.1038/s41586-019-1330-0.
- Beane J, Mazzilli SA, Tassinari AM, Liu G, Zhang X, Liu H, Buncio AD, Dhillon SS, Platero SJ, Lenburg ME, et al. Detecting the presence and progression of premalignant lung lesions via airway gene expression. Clin Cancer Res. 2017;23(17):5091–5100. PMID: 28533227. doi:10.1158/1078-0432.ccr-16-2540.
- Mascaux C, Laes JF, Anthoine G, Haller A, Ninane V, Burny A, Sculier JP. Evolution of microRNA expression during human bronchial squamous carcinogenesis. Eur Respir J PMID: 19010987. 2009;33(2):352–359. doi:10.1183/09031936.00084108.
- Angelova M, Mlecnik B, Vasaturo A, Bindea G, Fredriksen T, Lafontaine L, Buttard B, Morgand E, Bruni D, Jouret-Mourin A, et al. Evolution of metastases in space and time under immune selection. Cell. 2018;175(3):751–765 e716. PMID: 30318143. doi:10.1016/j.cell.2018.09.018.
- Galon J, Bruni D. Tumor immunology and tumor evolution: intertwined histories. Immunity PMID: 31940273. 2020;52:55–81. doi:10.1016/j.immuni.2019.12.018.
- Huang P, Lin CT, Li Y, Tammemagi MC, Brock MV, Atkar-Khattra S, Xu Y, Hu P, Mayo JR, Schmidt H, et al. Prediction of lung cancer risk at follow-up screening with low-dose CT: a training and validation study of a deep learning method. Lancet Digit Health. 2019;1(7):e353–e362. PMID: 32864596. doi:10.1016/s2589-7500(19)30159-1.
- Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov PMID: 30610226. 2019;18:197–218. doi:10.1038/s41573-018-0007-y.
- Bindea G, Mlecnik B, Angell HK, Galon J. The immune landscape of human tumors: implications for cancer immunotherapy. Oncoimmunology PMID: 24800163. 2014;3(2):e27456. doi:10.4161/onci.27456.
- Pol J, Bloy N, Buque A, Eggermont A, Cremer I, Sautes-Fridman C, Galon J, Tartour E, Zitvogel L, Kroemer G, et al. Trial watch: peptide-based anticancer vaccines. Oncoimmunology. 2015;4(4):e974411. PMID: 26137405. doi:10.4161/2162402X.2014.974411.
- Pol J, Bloy N, Obrist F, Eggermont A, Galon J, Hervé Fridman W, Cremer I, Zitvogel L, Kroemer G, Galluzzi L. Trial watch: DNA vaccines for cancer therapy. Oncoimmunology PMID: 24800178. 2014;3(4):e28185. doi:10.4161/onci.28185.
- Vacchelli E, Eggermont A, Galon J, Sautes-Fridman C, Zitvogel L, Kroemer G, Galluzzi L. Trial watch: monoclonal antibodies in cancer therapy. Oncoimmunology PMID: 23482847. 2013;2(1):e22789. doi:10.4161/onci.22789.
- Pol J, Buqué A, Aranda F, Bloy N, Cremer I, Eggermont A, Erbs P, Fucikova J, Galon J, Limacher JM, et al. Trial Watch-Oncolytic viruses and cancer therapy. Oncoimmunology. 2016;5(2):e1117740. PMID: 27057469. doi:10.1080/2162402x.2015.1117740.
- Vacchelli E, Galluzzi L, Eggermont A, Galon J, Tartour E, Zitvogel L, Kroemer G. Trial Watch: immunostimulatory cytokines. Oncoimmunology. 2015;4(4):493–506. PMID: 22754768. doi:10.4161/onci.20459.
- Iribarren K, Bloy N, Buqué A, Cremer I, Eggermont A, Fridman WH, Fucikova J, Galon J, Špíšek R, Zitvogel L, et al. Trial Watch: immunostimulation with Toll-like receptor agonists in cancer therapy. Oncoimmunology. 2016;5(3):e1088631. PMID: 27141345. doi:10.1080/2162402x.2015.1088631.
- Van Den Eynde M, Mlecnik B, Bindea G, Fredriksen T, Church SE, Lafontaine L, Haicheur N, Marliot F, Angelova M, Vasaturo A, et al. The link between the multiverse of immune microenvironments in metastases and the survival of colorectal cancer patients. Cancer Cell. 2018;34(6):1012–1026 e1013. PMID: 30537506. doi:10.1016/j.ccell.2018.11.003.
- Beane JE, Mazzilli SA, Campbell JD, Duclos G, Krysan K, Moy C, Perdomo C, Schaffer M, Liu G, Zhang S, et al. Molecular subtyping reveals immune alterations associated with progression of bronchial premalignant lesions. Nat Commun. 2019;10(1):1856. PMID: 31015447. doi:10.1038/s41467-019-09834-2.
- Merrick DT, Edwards MG, Franklin WA, Sugita M, Keith RL, Miller YE, Friedman MB, Dwyer-Nield LD, Tennis MA, O’Keefe MC, et al. Altered Cell-Cycle control, inflammation, and adhesion in high-risk persistent bronchial dysplasia. Cancer Res. 2018;78(17):4971–4983. PMID: 29997230. doi:10.1158/0008-5472.can-17-3822.
- Pennycuick A, Teixeira VH, AbdulJabbar K, Raza SEA, Lund T, Akarca AU, Rosenthal R, Kalinke L, Chandrasekharan DP, Pipinikas CP, et al. Immune surveillance in clinical regression of preinvasive squamous cell lung cancer. Cancer Discov. 2020;10(10):1489–1499. PMID: 32690541. doi:10.1158/2159-8290.cd-19-1366.
- Teixeira VH, Pipinikas CP, Pennycuick A, Lee-Six H, Chandrasekharan D, Beane J, Morris TJ, Karpathakis A, Feber A, Breeze CE, et al. Deciphering the genomic, epigenomic, and transcriptomic landscapes of pre-invasive lung cancer lesions. Nat Med. 2019;25(3):517–525. PMID: 30664780. doi:10.1038/s41591-018-0323-0.
- Rozenblatt-Rosen O, Regev A, Oberdoerffer P, Nawy T, Hupalowska A, Rood JE, Ashenberg O, Cerami E, Coffey RJ, Demir E, et al. The human tumor atlas network: charting tumor transitions across space and time at Single-Cell resolution. Cell. 2020;181(2):236–249. PMID: 32302568. doi:10.1016/j.cell.2020.03.053.