
Abstract
Health risk screenings providing personalised risk information are gaining prominence. Yet, only few studies have examined how people react to low-risk feedback yielding inconsistent results. While some studies observed a high acceptance of low-risk health feedback, others showed a lack of acceptance. The present experiment extends previous research by (1) testing whether pre-feedback expectancies moderate the response to low-risk feedback, (2) probing different types of responses to feedback (‘feedback acceptance’ and ‘perceived implications’), and (3) adding an ‘experiential-enriched' phase to the (fictitious) risk testing procedure. Specifically, participants monitored the risk measure process through the provision of ‘evolving' risk feedback, which enables real-time risk-related experiences. A total of 96 participants received computerised, personalised risk feedback about their own risk of developing a (fictitious) stress-related disease (Tucson-Fatigue-Syndrome). Afterwards, feedback acceptance and perceived implications for one's future health were assessed. Participants’ reactions to feedback valence (high- vs. low-risk status) were moderated by their pre-feedback expectancy. Unexpected low-risk feedback was associated with less acceptance and higher perceived negative consequences for the self compared to expected low-risk feedback, indicating a ‘lack of reassurance’. Thus, good news is significantly less reassuring when it is unexpected.
1. Introduction
Health risk screenings informing people about their risk status are gaining prominence within as well as outside the traditional medical setting. Thus, an increasing number of people face dealing with health risk information without professional support and counselling due to the growing number of self-assessment tools (e.g. Breast Cancer Risk Assessment Tool, National Institutes of Health) and over-the-counter screening tests (e.g. blood glucose meter). When confronted with personalised health information, an often-replicated finding is that people accept high-risk feedback to a lesser degree than low-risk feedback (e.g. Baumeister, Bratslavsky, Finkenauer, & Vohs, Citation2001; Croyle, Sun, & Hart, Citation1997; Ditto & Lopez, Citation1992; Jemmott, Ditto, & Croyle, Citation1986; for an overview see Van ‘t Riet & Ruiter, Citation2013).
However, despite broad evidence of the lower acceptance of high-risk compared to low-risk information, results from various field studies providing actual risk feedback indicate that low-risk feedback does not always lead to acceptance and reassurance (e.g. Dillard, McCaul, Kelso, & Klein, Citation2006; McCaul, Canevello, Mathwig, & Klein, Citation2003; Michie et al., Citation2002; Renner, Citation2004; Weinstein et al., Citation2004) . For example, in a study on risk perception for Alzheimer's disease, unaffected first-degree relatives of patients were informed about their Apolipoprotein E (APOE) genotype and their lifetime risk of developing Alzheimer disease. Although a majority recalled their test result correctly, 33% of these still believed that their risk was higher than that indicated by the test (Linnenbringer, Roberts, Hiraki, Cupples, & Green, Citation2010). Thus, despite having received good news, some of the participants showed a ‘lack of reassurance’, that is, devaluated low-risk feedback. This raises the question of why studies differ with regard to the acceptance of low-risk information.
We propose that a moderating factor of the relationship between feedback valence (low- vs. high-risk status) and feedback acceptance is pre-feedback expectancies. For example, Weinstein et al. (Citation2004) observed a significant effect of pre-test expectancies on the reception of actual colon cancer risk information. In a similar vein, in a community health screening providing participants with feedback about their actual cholesterol level, positive cholesterol feedback (non-elevated cholesterol level) was not met with clear acceptance and reassurance in all cases (Renner, Citation2004; also see Panzer & Renner, Citation2008). Recipients receiving unexpected low-risk cholesterol feedback showed significantly less reassurance (e.g. higher perceived personal threat for cardiovascular disease) than those receiving expected low-risk cholesterol feedback. However, the interpretation of these results is limited since the health risk feedback was not randomly assigned to the recipients but was based on the actual risk status (e.g. cholesterol readings). Accordingly, in a first web-based study systematically examining the phenomenon ‘lack of reassurance’, participants were provided with randomised risk feedback on the risk faced by an average peer and their own risk, and their prior expectancies were assessed (Gamp & Renner, Citationsubmitted). As in the studies providing actual health risk feedback, participants who expected to be at high risk but received good news (unexpected low-risk feedback) showed a ‘lack of reassurance’ in their post-feedback, comparative risk perceptions.
Moreover, previous research mainly focused on certain feedback reception responses. However, responses towards health-related risk feedback encompass conceptually different reaction types, as the Model of Illness Threat Appraisal proposes (MITA, Ditto, Jemmott, & Darley, Citation1988; Ditto & Lopez, Citation1992; Lazarus, Citation1998; Weisman, Citation1972; see also Renner & Schupp, Citation2011). The MITA model distinguishes two different types of initial reactions to illness threats. One type encompasses appraisals of to what extent the test result (e.g. high blood-pressure reading) is actually indicative of an underlying condition (e.g. hypertension). For instance, participants may be sceptical of whether the test yields accurate and representative results. Hence, these responses capture the degree of acceptance of the provided risk feedback, also called ‘acceptance of fact’ (see also Croyle, Sun, & Louie, Citation1993; Ditto & Lopez, Citation1992). A conceptually different type of reaction, the ‘acceptance of implications’, encompasses the acknowledgement of personal consequences resulting from the risk status. For example, hypertension (risk status) might be perceived as only weakly related to serious health consequences, such as cardiovascular diseases. Accordingly, the evaluation of risk feedback information unfolds on different stages within the illness threat appraisal process. Conjointly examining these different types of reactions allows a more comprehensive understanding of the phenomenon ‘lack of reassurance’.
In addition, the inconsistent results of previous studies regarding the acceptance of low-risk feedback might also reflect a discrepancy in the amount of experiences with the risk factor and testing procedure. While field studies have typically examined well-known risk factors, such as high cholesterol levels (e.g. Renner, Citation2004), experimental studies often used fictitious risk factors such as a fictitious enzyme deficiency (e.g. Jemmott et al., Citation1986; for an overview see Ditto & Croyle, Citation1995). Thus, the processing of risk information might be embedded, in the former case, in a more experience-rich mode where participants can draw upon experience with and information about the well-known risk factor. In contrast, in experimental studies providing feedback about fictitious diseases, recipients have, by definition, no personal experience with the disease. Therefore, the testing procedure and feedback experience might have been less engaging and experiential for the recipients. Therefore, the present experiment extends previous studies, which mainly relied on a single risk information feedback (e.g. Kunda, Citation1987, ‘Fibrocystic Disease') or a single risk factor test (e.g. Jemmott et al., Citation1986, ‘TAA') and thus limited experiences with the risk factor and testing procedure. Specifically, the present paradigm provides feedback about a more familiar health risk (i.e. a stress-related disease) and adds a more pronounced ‘experiential' phase to the (fictitious) risk testing procedure.
1.1. The present study
The present study aims to extend previous research on health-related risk feedback reception by (1) investigating responses in dependence of feedback valence and pre-feedback expectancies in order to examine the ‘lack of reassurance’ phenomenon, (2) examining a wider response type spectrum (‘acceptance of fact’, ‘acceptance of implications’), and (3) using an experimental design that utilises the intuitive relationship between stress and heart rate in order to increase the experiential value of the provided feedback. Stress and stress-related diseases are highly familiar to the public since being stressed is a prevalent phenomenon in all age groups in Germany (e.g. Bundespsychotherapeutenkammer, Citation2012; Gangl, Citation2009; Hapke et al., Citation2013). Accordingly, beliefs about one's own vulnerability towards stress and stress-related diseases (i.e. pre-feedback expectancy) are based on a multitude of past personal experiences.
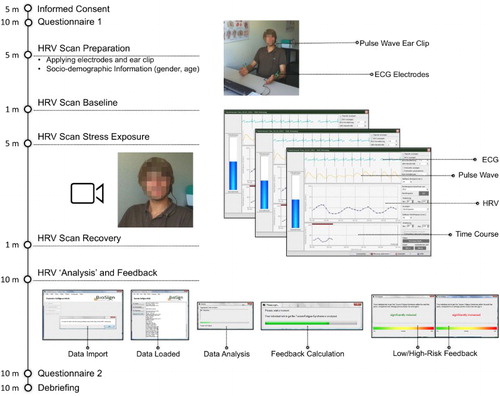
In order to facilitate an experiential value of risk feedback reception, participants’ heart rate variability (HRV) was measured, and the health feedback for a fictitious stress-related disease, ‘Tucson-Fatigue-Syndrome’ (TFS), was ostensibly based on this measure (see also ). Extending previous research, participants monitored the risk measure process by viewing the HRV measure across time and situation that reflected their response during the baseline, stress exposure, and recovery phases which created risk-related experiences in the moment. In addition, an individualised HRV summary and evaluative risk feedback was provided.
Figure 1. Study flow. Participants filled in Questionnaire 1, which assessed pre-feedback expectancies. To realise an experiential-enriched risk factor test, participants’ electrocardiogram (ECG) and pulse wave, comprising participants’ HRV, were measured in three phases (baseline, stress exposure, and recovery). Participants could track their physiological signals in real time on the computer screen (ECG, pulse wave, HRV, and time course of the measure). Following the HRV measure, participants received computerised, randomly assigned feedback about their ‘personal risk’ of developing TFS within the next 5 years. Reactions towards the risk feedback were indicated in Questionnaire 2. Afterwards, participants were debriefed and thanked.
To investigate whether participants devaluate unexpected low-risk feedback indicating a ‘lack of reassurance’, reception of low-risk feedback as a function of pre-feedback expectancies was examined. Risk feedback reception was assessed by measuring two conceptually different types of response, the ‘acceptance of fact’ and the ‘acceptance of implications’. With regard to the ‘acceptance of fact’, ‘lack of reassurance’ is indicated when low-risk feedback is less accepted if received unexpectedly (high pre-feedback expectancy) compared to expectedly (low pre-feedback expectancy). Regarding the ‘acceptance of implications’, ‘lack of reassurance’ is demonstrated when participants acknowledge greater personal implications following low-risk feedback that is received unexpectedly (high pre-feedback expectancy) compared to expectedly (low pre-feedback expectancy).
2. Method
2.1. Participants
A total of 96 participants (94 undergraduates and 2 employees of the University of Konstanz) were recruited through flyers and posters distributed at the university and attended the study in exchange for course credit or a monetary compensation of 8 Euro. One participant was excluded from analyses due to an implausible response pattern (being negatively surprised after low-risk feedback). Thus, the data of 95 participants were included in the analyses.Footnote1 Participants were on average 22.5 (SD = 5.5) years old and reported a very good health status, M (SD) = 5.0 (0.8), on a scale ranging from 1 ‘poor’ to 6 ‘excellent’. Twenty-five participants were male (26.3%) and 97.9% had no prior experience with tests measuring stress burden. The experimental conditions did not differ significantly regarding age, gender, or perceived knowledge about the fictitious stress-related disease ‘TFS' and the HRV measure (all ps > .08, ).
The study was conducted in accordance with the ethical guidelines of the German Psychological Society (Deutsche Gesellschaft für Psychologie, DGPs; http://www.dgps.de/dgps/aufgaben/003.php; see paragraph C.III), which are similar to those of the American Psychological Association (APA; see also Huebner & Gegenfurtner, Citation2012).
2.2. Procedure
Individual participants arrived at a small laboratory room at the university to participate in a study on ‘the relationship between personality characteristics and stress-related diseases’ (see also ). They were met by a female experimenter wearing a white laboratory coat who introduced herself as a medical technical assistant (MTA). The laboratory room was equipped with medical trappings, such as health-related posters, a stethoscope, and other medical paraphernalia (see Croyle & Ditto, Citation1990; Jemmott et al., Citation1986 for a similar procedure).
The cover story stated that stress-related diseases are on the rise and that certain personality characteristics may play an important role in the development of diseases resulting from stress. Thus, the relationship between personality characteristics and the risk of developing a (fictitious) stress-related disease, TSF, would be examined. This TFS was described as having mild but irritating symptoms. Participants were told that the individual risk for TFS would be determined using a HRV scanner that was introduced as a medical indicator for developing TFS. Afterwards, a detailed personality assessment would be conducted. After reading a detailed procedure protocol, participants signed a consent form.
A first questionnaire assessed demographic variables and participants’ pre-feedback expectancies regarding their TFS risk status. Next, participants were led to the HRV scanner (see also ). The HRV measure comprised a non-invasive, completely painless and easy to administer physiological measure with no side-effects. During measurement, participants’ HRV was recorded using the combined signal of participants’ heart rate and pulse wave that were measured by electrocardiogram electrodes on the wrists and an ear clip (BioSign GmbH). To realise a more experiential-based feedback and study setting, participants could track these real physiological signals (heart rate, pulse wave, and HRV) in real time on the computer screen. In order to simulate a stress adaptation process, the measure consisted of three phases: a baseline (1 minute), a stress-inducing task performance (5 minutes), and an adaptation phase (1 minute; cf. Olsson, Roth, & Melin, Citation2010). For the task performance (stress phase), participants were asked to introduce themselves in a free speech of 5 minutes while being videotaped. In order to increase the socio-evaluative threat, it was additionally noted that both voice and non-verbal behaviour would be video-analysed. Participants were not allowed to use any notes during the presentation and were prompted in a standardised way to continue talking whenever they finished their speech in less than 5 minutes (‘You still have some time left. Please continue.’, cf., ‘Trier Social Stress Test', Von Dawans, Kirschbaum, & Heinrichs, Citation2011). Following the HRV measure, participants received computerised, randomly assigned feedback about their ‘personal risk’ of developing TFS within the next 5 years: ‘Your personal risk to get Tucson-Fatigue-Syndrome within the next five years, compared to an average person of your gender and age, is clearly increased [clearly reduced]’. The words ‘clearly increased’ and ‘clearly reduced’ were highlighted in that they were coloured red and green, respectively, and emphasised regarding font size and justification (see also ). After reading their individualised feedback, participants indicated their perceived stress level during the HRV measure and revealed their reactions towards the feedback in a second questionnaire. These questions were embedded in a series of filler items. Afterwards, participants were debriefed carefully. The debriefing included an explanation of the reasons for administering a fictitious feedback. Additionally, participants were informed that the HRV data had not been and would not be analysed in the future. Finally, to avoid participants persisting in false beliefs after the debriefing, the ‘perseverance effect’ was explicitly described, which has been shown to be effective in eliminating the perseverance of false beliefs (McFarland, Cheam, & Buehler, Citation2007).
2.3. Measures
Pre-feedback expectancy: At the end of the first questionnaire, participants were asked to estimate their risk for TFS. (‘Immediately after completing this questionnaire your heart rate variability will be measured. On the basis of this measure your individual risk of developing Tucson-Fatigue-Syndrome will be analysed. What do you expect: How high will your risk of disease be?’). Responses ranged on a Likert scale from 1 ‘very low’ to 6 ‘very high’. Pre-feedback expectancy was categorised as ‘low’ for estimations ranging from 1 to 3 and ‘high’ for estimations ranging from 4 to 6. Of the 95 participants, 59 (62%) expected to receive low-risk feedback and 36 (38%) expected to receive high-risk feedback.
Acceptance of fact: The acceptance of the health risk feedback was assessed with three items, using a 6-point Likert scale ranging from 1 ‘very unlikely’ to 6 ‘very likely’ (Renner, Hahn, & Schwarzer, Citation1996; also see Croyle et al., Citation1997; Croyle & Sande, Citation1988; Renner, Citation2004). Two questions queried the perceived reliability of the feedback (‘How likely do you think it is that your screening result is wrong or inaccurate?’ – recoded and ‘How likely do you think it is that the test will yield a similar result if taken again?’). One question covered the perceived representativeness of the measurement (‘How likely do you think is it that your risk for TFS measured today is a momentary fluctuation?’ – recoded). Items were averaged to create an index called ‘acceptance of fact’, with higher scores indicating higher feedback acceptance (Cronbach's α = .77).
Acceptance of implications: The acceptance of the personal consequences of the individual feedback was assessed with three items, using a 6-point Likert scale (Renner et al., Citation1996; also see Renner, Citation2004). Estimations of the severity of TFS for one's own health were assessed by two questions (‘How serious a threat to your health is your risk for TFS?’, 1 ‘not at all serious’ – 6 ‘extremely serious’, and ‘How threatening is your risk of developing TFS for your health?’, 1 ‘not at all threatening’ – 6 ‘extremely threatening’). Perceived pressure to change was measured with a single item (‘Do you think there is a need for you to take action in order to lower your risk for TFS?’, 1 ‘not at all necessary’ – 6 ‘absolutely necessary’). Items were averaged to create an index called ‘acceptance of implications’, with higher scores indicating higher acceptance of personal consequences (Cronbach's α = .89).
In addition, perceived stress level during the HRV measure was assessed on a 6-point Likert scale ranging from ‘not at all stressed’ to ‘extremely stressed’.
3. Results
Data were analysed with 2 × 2 between-groups analyses of variance (ANOVAs). The independent variables used were ‘pre-feedback expectancy’ (low vs. high) and ‘personal risk feedback’ for TFS (low vs. high).
3.1. Control analysis
To exclude the possibility that different stress levels during the HRV measure confounded experimental effects on acceptance of fact and acceptance of implications, we analysed whether the four conditions differed in perceived stress levels. There were no significant differences in stress experienced during the measure, Fs(1, 91) < 2.2, ps > .14.
3.2. Acceptance of fact
For the acceptance of the provided health risk feedback (, left side), the ANOVA yielded a significant main effect for the factor ‘personal risk feedback’, F(1, 91) = 27.93, p < .001, . Thus, participants receiving high-risk feedback showed on average a lower feedback acceptance (M = 3.37; SD = .89) than participants receiving low-risk feedback (M = 4.52; SD = 0.99), replicating the often-found asymmetrical acceptance of positive compared to negative health information. However, this main effect was qualified by a significant interaction with ‘pre-feedback expectancy’, F(1, 91) = 9.19, p = .003,
. No other effects were statistically significant.
Figure 2. Effects of personal risk information and pre-feedback expectancy on the ‘acceptance of fact’ (left side) and the ‘acceptance of implications’ (right side, ±SE). * p < .05, *** p < .001.
To test for (lack of) reassurance, simple main effects following up the significant interaction were calculated. As the left side of shows, participants in the low-risk feedback condition showed a significantly lower acceptance of the risk feedback if the feedback was received unexpectedly (high pre-feedback expectancy) as compared to expectedly (low pre-feedback expectancy), indicating ‘lack of reassurance’ in the unexpected good news condition, F(1, 91) = 5.69, p = .019, . In the high-risk feedback condition feedback acceptance differed marginally significant between participants expecting a low- or high-risk feedback, F(1, 91) = 3.63, p = .060,
.Footnote2
3.3. Acceptance of implications
For the acceptance of personal consequences as indicated by the health risk feedback (, right side), the ANOVA yielded a significant main effect for the factor ‘personal risk feedback’, F(1, 91) = 58.05., p < .001, . Thus, participants receiving high-risk feedback perceived on average higher personal implications due to their TFS risk status (M = 3.55; SD = 1.09) than participants receiving low-risk feedback (M = 1.91; SD = 0.96), showing sensitivity to the provided risk feedback information. The main effect for the factor ‘pre-feedback expectancy’ was also significant, indicating that participants who expected to receive high-risk TFS feedback (M = 3.07; SD = 1.16) acknowledged higher personal implications than those who expected to receive low-risk TFS feedback (M = 2.54; SD = 1.36), F(1, 91) = 9.23, p = .003,
. The two main effects were qualified by a significant interaction, F(1, 91) = 5.24, p = .024,
, which was followed up by simple effects analyses.
Indicating ‘lack of reassurance’, participants receiving low-risk feedback acknowledged higher personal implications if the risk feedback was unexpected (high pre-feedback expectancy) as compared to expected (low pre-feedback expectancy), F(1, 91) = 14.41, p < .001, . In the high-risk feedback condition, however, pre-feedback expectancy groups showed no difference on the acknowledgement of personal consequences, F(1, 91) = .28, p = .601.Footnote3
4. Discussion
Using an experiential-enriched study procedure and feedback, the present findings replicate and extend previous findings since participants’ reactions to personalised feedback not only differed as a function of feedback valence but also pre-feedback expectancy, suggesting a ‘lack of reassurance’ after receiving unexpected ‘good news’. Moreover, the ‘lack of reassurance’ phenomenon following unexpected low-risk health feedback extended to a wider response spectrum leading to significantly lower ‘acceptance of fact’ and ‘acceptance of implications’.
4.1. Lack of reassurance
In line with previous findings, both types of reactions to the provided feedback differed as a function of feedback valence. Accordingly, acceptance of the given feedback (‘acceptance of fact’) was lower in the high-risk feedback condition compared to the low-risk feedback condition. That is, participants derogated the validity of the high-risk feedback, whereas low-risk feedback was comparatively accepted (e.g. Ditto & Lopez, Citation1992; Jemmott et al., Citation1986; Renner, Citation2004; for an overview see Van ‘t Riet & Ruiter, Citation2013). In addition, participants receiving high-risk feedback showed greater ‘acceptance of implications’ compared to participants receiving low-risk feedback. Thus, participants were sensitive to the given risk status and accurately related high-risk feedback to greater personal consequences (French, Hevey, Sutton, Kinmonth, & Marteau, Citation2006; French, Sutton, Marteau, & Kinmonth, Citation2004; Renner, Citation2004).
However, extending previous research, these effects were moderated by pre-feedback expectancy (Gamp & Renner, Citationsubmitted; Renner, Citation2004; Sweeny & Dillard, Citation2014; Weinstein et al., Citation2004). In line with our hypotheses, both types of responses indicated ‘lack of reassurance’: if low-risk feedback was received unexpectedly compared to expectedly, participants showed less acceptance of the all-clear feedback (lower ‘acceptance of fact’). Furthermore, participants demonstrated less reassurance regarding personal consequences of their risk status by acknowledging higher personal consequences if low-risk feedback was received unexpectedly compared to expectedly (higher ‘acceptance of implications’). As previously formed beliefs are already in place, this study provides further evidence that external information (e.g. health risk feedback) is not interpreted independently of these pre-existing beliefs (cf., Gamp & Renner, Citationsubmitted; Heiniger, Butow, Charles, & Price, Citation2015; Renner, Citation2004; Seligman, Railton, Baumeister, & Sripada, Citation2013; Weinstein et al., Citation2004). These findings concur with a recent study by Sweeny and Dillard (Citation2014), which compared a low-risk condition group who experienced positive disconfirmation and a high-risk condition group who experienced negative disconfirmation of their expected salvia toxin level. When receiving an unexpected high toxin-level reading, participants perceived a threat as more severe than when receiving an unexpected low (but otherwise equivalent) reading.
4.2. Experience-based expectancies and health risk feedback
Previous research on health risk feedback reception has primarily focused on the effect of feedback valence (e.g. Croyle et al., Citation1997; Ditto, Citation2009; French et al., Citation2006; Harris & Smith, Citation2005). The impact of information consistency with prior expectancies has been addressed in fewer studies (Ditto & Lopez, Citation1992; Ditto, Munro, Apanovitch, Scepansky, & Lockhart, Citation2003; Ditto, Scepansky, Munro, Apanovitch, & Lockhart, Citation1998; Renner, Citation2004; for an overview see Ditto, Citation2009). Yet importantly, most of these studies did not investigate the effect of expectancies on reactions to health risk feedback. Instead, expectancies about the individual risk status were held constant. However, results from the present study indicate that, in addition to feedback valence, the pre-feedback expectancies people hold about their risk status seem to be an important determinant of risk feedback reception.
In an experimental design, pre-existing beliefs can be manipulated by providing a baseline risk estimate (e.g. the overall prevalence of a risk factor; Ditto & Jemmott, Citation1989; Ditto & Lopez, Citation1992; Natter & Berry, Citation2005). Alternatively, risk expectancies that are personally generated based on past experiences can be assessed (e.g. Gamp & Renner, Citationsubmitted; Renner, Citation2004; also see Sweeny & Dillard, Citation2014). However, personally generated expectancies are more vivid and experiential than descriptive risk information, such as base rates. Accordingly, although learning by description that 20% of university students have an increased risk for a certain disease is potentially powerful, it is not the same as believing that one's own risk for that disease is 20% (Rothman & Kiviniemi, Citation1999; Weinstein, Citation1998; also see Camilleri & Newell, Citation2013; Hertwig & Erev, Citation2009; Sweeny & Dillard, Citation2014). Therefore, we asked participants to indicate their personal pre-feedback risk estimate. In order to ensure the validity of pre-feedback expectancies, the present study design used the familiar, highly self-relevant context of stress-related diseases. Thus, compared to existing experimental paradigms, such as bogus tests on a pancreatic disease, a bacterial condition, or exposure to toxins (Cioffi, Citation1991; Jemmott et al., Citation1986; Sweeny & Dillard, Citation2014), we used a fictitious disease that has a close relation to daily life and which is probably well represented. Hence, beliefs about one's own vulnerability towards stress and stress-related diseases are likely to be rather elaborate. This assessment of pre-feedback expectancies was combined with a more experiential-enriched risk factor test. This combination ensured that the high self-relevance and ecological validity commonly obtained in studies providing actual risk feedback complemented the control and internal validity of experiments providing randomly assigned risk feedback. By providing randomised health risk feedback in an experiential-enriched study setting, the present experiment could, therefore, mitigate the observed inconsistencies in previous results on the reception of low-risk health feedback. In a similar vein, it has been shown in decision-making research that decisions people make differ in dependence of their experience with the decision options; this phenomenon is called ‘description-experience gap’ (Hertwig & Erev, Citation2009; Weber, Citation2003). Experience with the decision options can result from explicitly stated (descriptive) information summarising probabilities about the possible outcomes. Alternatively, people can learn about the possible outcomes and their associated probabilities through experiential sampling over time. Depending on the mode of information acquisition, decisions on risky choices differed (Hertwig & Erev, Citation2009; Weber, Citation2003). Accordingly, experiences at the very moment seem to substantially impact responses to risk information. However, the present paradigm is a first step towards broaching the subject ‘description-experience gap’ (e.g. Camilleri & Newell, Citation2013; De Palma et al., Citation2014; Hertwig & Erev, Citation2009; Weber, Citation2003). Further research might compare a descriptive and an experience-based feedback condition in order to investigate the idea of more experience-based processing modes more directly.
4.3. Adaptivity in risk feedback reception
Conceptions about our health are central part of the self-concept (Greenwald, Citation1980; Hooker & Kaus, Citation1994; Markus, Citation1977; Rokeach, Citation1973). Information which is inconsistent with pre-existing beliefs is more likely to induce selective attention and more elaborate processing (e.g. Edwards & Smith, Citation1996; Hilton, Klein, & von Hippel, Citation1991; Lord, Ross, & Lepper, Citation1979). Accordingly, new information seems to be processed more critically (Renner, Citation2004), resulting in greater doubts about its accuracy and, in case of low-risk information, its reassuring implications. This scrutinising of unexpected information can be considered as an adaptive response since erroneously accepting a false all-clear feedback might cause substantial harm and emotional costs in the future when, for example, less preventative measures are taken (Renner, Citation2004; Renner, Gamp, Schmälzle, & Schupp, Citation2015; Renner & Schupp, Citation2011). Consequently, this ‘lack of reassurance’ following unexpected good news can protect the self in the long run despite forfeiting a positive emotional gain in the short run.
Addressing a long-term perspective is important since responses to health risks represent a dynamic process rather than a one-off snapshot (Burns & Slovic, Citation2012; Chen, Griffith, Cottrell, & Wong, Citation2013). Conjointly examining different stages within the illness threat appraisal process, such as ‘acceptance of fact’ and ‘acceptance of implications’, is therefore an important first step towards obtaining a more comprehensive picture of risk feedback reception. To deepen our understanding of how adaptivity in risk perception translates into adaptive behaviours, future research needs to realise longitudinal designs in order to explore risk perceptions in a dynamic context (Burns & Slovic, Citation2012; Renner, Schüz, & Sniehotta, Citation2008; Siegrist, Citation2013, Citation2014).
4.4. Limitations
In addition to the strengths of the present study, which result from the experimental manipulation of the provided health risk information in a highly self-relevant and experiential study situation, several limitations also need to be acknowledged. The study focused on cognitive responses to personalised health risk feedback. Showing that ‘lack of reassurance’ emerges across two different types of cognitive response measures is an important first step in examining the phenomenon ‘lack of reassurance’. In the next step, generalisability to more affect-based outcomes, as addressed by dual-process approaches on health risk feedback reception, should be investigated since recent research has shown that both cognitive considerations and affective reactions can influence risk perception and risky choice (e.g. Kahneman, Citation2003; McCaul, Peters, Nelson, & Stefanek, Citation2005; Renner & Reuter, Citation2012; Slovic, Peters, Finucane, & Macgregor, Citation2005; Van Gelder, De Vries, & Van Der Pligt, Citation2009). In a similar vein, pre-feedback illness representations regarding the implications of the disease were not assessed and thus, their impact on reactions to test results, or the impact of test results on changes in illness consequence representations could not be assessed (we thank an anonymous reviewer for this comment). However, due to the randomisation of risk feedback conditions, inter-individual differences concerning illness representations were likely balanced across conditions. However, illness representations (e.g. perceptions of disease severity) might have been affected by the individual risk feedback. Examining the impact of illness representations is certainly a promising avenue for further studies on risk feedback processing. In addition, student participants who choose to be tested are not representative of the general population and are by definition self-selected. Even though the context of stress-related diseases seems also applicable and appropriate for young participants, the degree to which the findings generalise to other age groups is limited. Additionally, one should be careful to generalise to people who refrained from testing since self-selected participants may, in part, be psychologically and behaviourally prepared for dealing with bad news. A further limitation of the present study is that the pre-feedback risk expectancy was not experimentally manipulated (but see Sweeny & Dillard, Citation2014). Thus, a priori differences between the high and low pre-feedback expectancy groups might have impaired internal validity.
4.5. Conclusion
The present experiment examined the phenomenon ‘lack of reassurance’ as shown in studies that provided participants with actual health risk feedback in an experimental study design applying randomised health risk feedback. This paradigm allowed operationalising pre-feedback expectancy, study setting, and risk feedback in a more experiential-enriched way. Reactions to the health risk feedback differed as a function of feedback valence. In addition, pre-feedback risk expectancy considerably moderated the effect of feedback valence on the acceptance of the feedback and its personal implications, indicating ‘lack of reassurance’. Thus, participants accepted low-risk feedback to a lesser degree and were less reassured with regard to personal consequences if the feedback was received unexpectedly compared to expectedly. Accordingly, the present study could mitigate the inconsistencies in previous empirical results on the reception of low-risk health feedback.
Disclosure statement
No potential conflict of interest was reported by the authors.
ORCID
Martina Gamp http://orcid.org/0000-0002-6890-9304
Additional information
Funding
Notes
1 The exclusion or inclusion of this single participant did not affect the results. All main and interaction effects remained significant with F(1, 92) > 6.9, p ≤ .015.
2 The simple main effects for feedback valence with ‘acceptance of fact’ and ‘acceptance of implications' as dependent variables were also tested. For feedback acceptance, the simple main effect for feedback valence was significant within the low pre-feedback expectancy group, F(1, 91) = 45.63, p < .001, but not within the high pre-feedback expectancy group, F(1, 91) = 2.04, p = .156. For perceived feedback implications, both simple main effects for feedback valence were significant: within low pre-feedback expectancy, F(1, 91) = 64.79, p < .001,
; within high pre-feedback expectancy, F(1, 91) = 11.43, p = .001,
. Comparing effects across dependent variables indicates that feedback valence had a greater impact on participants with low pre-feedback expectancies compared to participants with high pre-feedback expectancies (we thank an anonymous reviewer for this comment).
3 See note 2.
Related Research Data
References
- Baumeister, R. F., Bratslavsky, E., Finkenauer, C., & Vohs, K. D. (2001). Bad is stronger than good. Review of General Psychology, 5(4), 323–370. doi:10.1037//1089-2680.5.4.323
- Bundespsychotherapeutenkammer. (2012). BPtK-Studie zur Arbeitsunfähigkeit: Psychische Erkrankungen und Burnout, 1–29. Retrieved from http://www.bptk.de/uploads/media/20120606_AU-Studie-2012.pdf
- Burns, W. J., & Slovic, P. (2012). Risk perception and behaviors: Anticipating and responding to crises. Risk Analysis, 32(4), 579–582. doi:10.1111/j.1539-6924.2012.01791.x
- Camilleri, A. R., & Newell, B. R. (2013). Mind the gap? Description, experience, and the continuum of uncertainty in risky choice. Progress in Brain Research, 202, 55–71. doi:10.1016/B978-0-444-62604-2.00004-6
- Chen, F., Griffith, A., Cottrell, A., & Wong, Y.-L. (2013). Behavioral responses to epidemics in an online experiment: Using virtual diseases to study human behavior. PloS One, 8(1), e52814. doi:10.1371/journal.pone.0052814
- Cioffi, D. (1991). Asymmetry of doubt in medical self-diagnosis: The ambiguity of “uncertain wellness”. Journal of Personality and Social Psychology, 61(6), 969–980. doi:10.1037/0022-3514.61.6.969
- Croyle, R. T., & Ditto, P. H. (1990). Illness cognition and behavior: An experimental approach. Journal of Behavioral Medicine, 13(1), 31–52. doi:10.1007/BF00844898
- Croyle, R. T., & Sande, G. N. (1988). Denial and confirmatory search: Paradoxical consequences of medical diagnosis. Journal of Applied Social Psychology, 18(6), 473–490. doi:10.1111/j.1559-1816.1988.tb00030.x
- Croyle, R. T., Sun, Y., & Hart, M. (1997). Processing risk factor information: Defensive biases in health-related judgments and memory. In K. Petrie & J. Weinman (Eds.), Perceptions of health and illness: Current research and applications (pp. 267–290). Amsterdam: Harwood Academic.
- Croyle, R. T., Sun, Y., & Louie, D. H. (1993). Psychological minimization of cholesterol test results: Moderators of appraisal in college students and community residents. Health Psychology, 12(6), 503–507. doi:10.1037/0278-6133.12.6.503
- De Palma, A., Abdellaoui, M., Attanasi, G., Ben-Akiva, M., Erev, I., Fehr-Duda, H., … Weber, M. (2014). Beware of black swans: Taking stock of the description–experience gap in decision under uncertainty. Marketing Letters, 25(3), 269–280. doi:10.1007/s11002-014-9316-z
- Dillard, A. J., McCaul, K. D., Kelso, P. D., & Klein, W. M. P. (2006). Resisting good news: Reactions to breast cancer risk communication. Health Communication, 19(2), 115–123. doi:10.1207/s15327027hc1902_3
- Ditto, P. H. (2009). Passion, reason, and necessity a quantity-of-processing view of motivated reasoning. In T. Bayne & J. Fernández (Eds.), Delusion and self-deception: Affective and motivational influences on belief formation (pp. 23–53). New York, NY: Psychology Press.
- Ditto, P. H., & Croyle, R. T. (1995). Understanding the impact of risk factor test results: Insights from a basic research program. In R. T. Croyle (Ed.), Psychosocial effects of screening for disease, prevention and detection (pp. 144–181). New York, NY: Oxford University Press.
- Ditto, P. H., & Jemmott, J. B. (1989). From rarity to evaluative extremity: Effects of prevalence information on evaluations of positive and negative characteristics. Journal of Personality and Social Psychology, 57(1), 16–26. doi:10.1037/0022-3514.57.1.16
- Ditto, P. H., Jemmott, J. B., & Darley, J. M. (1988). Appraising the threat of illness: A mental representational approach. Health Psychology, 7(2), 183–201. doi:10.1037/0278-6133.7.2.183
- Ditto, P. H., & Lopez, D. F. (1992). Motivated skepticism: Use of differential decision criteria for preferred and nonpreferred conclusions. Journal of Personality and Social Psychology, 63(4), 568–584. doi:10.1037/0022-3514.63.4.568
- Ditto, P. H., Munro, G. D., Apanovitch, A. M., Scepansky, J. A., & Lockhart, L. K. (2003). Spontaneous skepticism: The interplay of motivation and expectation in responses to favorable and unfavorable medical diagnoses. Personality and Social Psychology Bulletin, 29(9), 1120–1132. doi:10.1177/0146167203254536
- Ditto, P. H., Scepansky, J. A., Munro, G. D., Apanovitch, A. M., & Lockhart, L. K. (1998). Motivated sensitivity to preference-inconsistent information. Journal of Personality and Social Psychology, 75(1), 53–69. doi:10.1037//0022-3514.75.1.53
- Edwards, K., & Smith, E. (1996). A disconfirmation bias in the evaluation of arguments. Journal of Personality and Social Psychology, 71(1), 5–24. doi:10.1037/0022-3514.71.1.5
- French, D. P., Hevey, D., Sutton, S., Kinmonth, A. L., & Marteau, T. M. (2006). Personal and social comparison information about health risk: Reaction to information and information search. Journal of Health Psychology, 11(3), 497–510. doi:10.1177/1359105306063324
- French, D. P., Sutton, S. R., Marteau, T. M., & Kinmonth, A. L. (2004). The impact of personal and social comparison information about health risk. British Journal of Health Psychology, 9(2), 187–200. doi:10.1348/135910704773891041
- Gamp, M., & Renner, B. (submitted). Reception of low-risk health feedback: Absolute and comparative Lack of Reassurance.
- Gangl, K. (2009). Kundenkompass Stress: Aktuelle Bevölkerungsbefragung: Ausmaß, Ursachen und Auswirkungen von Stress in Deutschland. Frankfurt am Main: FAZ-Institut für Management-, Markt- und Medieninformation.
- Greenwald, A. G. (1980). The totalitarian ego: Fabrication and revision of personal history. American Psychologist, 35(7), 603–618. doi:10.1037/0003-066X.35.7.603
- Hapke, D. U., Maske, U. E., Scheidt-Nave, C., Bode, L., Schlack, R., & Busch, M. A. (2013). Chronischer Stress bei Erwachsenen in Deutschland: Ergebnisse der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt - Gesundheitsforschung - Gesundheitsschutz, 56(5–6), 749–754. doi:10.1007/s00103-013-1690-9
- Harris, P. R., & Smith, V. (2005). When the risks are low: The impact of absolute and comparative information on disturbance and understanding in US and UK samples. Psychology & Health, 20(3), 319–330. doi:10.1080/08870440512331317689
- Heiniger, L., Butow, P. N., Charles, M., & Price, M. A. (2015). Intuition versus cognition: A qualitative exploration of how women understand and manage their increased breast cancer risk. Journal of Behavioral Medicine, 38(5), 727–739. doi:10.1007/s10865-015-9632-7
- Hertwig, R., & Erev, I. (2009). The description-experience gap in risky choice. Trends in Cognitive Sciences, 13(12), 517–523. doi:10.1016/j.tics.2009.09.004
- Hilton, J. L., Klein, J. G., & von Hippel, W. (1991). Attention allocation and impression formation. Personality and Social Psychology Bulletin, 17(5), 548–559. doi:10.1177/0146167291175010
- Hooker, K., & Kaus, C. R. (1994). Health-related possible selves in young and middle adulthood. Psychology and Aging, 9(1), 126–133. doi:10.1037/0882-7974.9.1.126
- Huebner, G. M., & Gegenfurtner, K. R. (2012). Conceptual and visual features contribute to visual memory for natural images. PloS One, 7(6), e37575. doi:10.1371/journal.pone.0037575
- Jemmott, J. B., Ditto, P. H., & Croyle, R. T. (1986). Judging health status: Effects of perceived prevalence and personal relevance. Journal of Personality and Social Psychology, 50(5), 899–905. doi:10.1037/0022-3514.50.5.899
- Kahneman, D. (2003). A perspective on judgment and choice: Mapping bounded rationality. The American Psychologist, 58(9), 697–720. doi:10.1037/0003-066X.58.9.697
- Kunda, Z. (1987). Motivated inference: Self-serving generation and evaluation of causal theories. Journal of Personality and Social Psychology, 53(4), 636–647. doi:10.1037/0022-3514.53.4.636
- Lazarus, R. S. (1998). The costs and benefits of denial. In R. S. Lazarus (Ed.), Fifty years of the research and theory of R.S. Lazarus: An analysis of historical and perennial issues (Vol. 1, pp. 227–251). Mahwah, NJ: Lawrence Erlbaum Associates.
- Linnenbringer, E., Roberts, J. S., Hiraki, S., Cupples, L. A., & Green, R. C. (2010). “I know what you told me, but this is what I think”: Perceived risk of Alzheimer disease among individuals who accurately recall their genetics-based risk estimate. Genetics in Medicine, 12(4), 219–227. doi:10.1097/GIM.0b013e3181cef9e1
- Lord, C. G., Ross, L., & Lepper, M. R. (1979). Biased assimilation and attitude polarization: The effects of prior theories on subsequently considered evidence. Journal of Personality and Social Psychology, 37(11), 2098–2109. doi:10.1037//0022-3514.37.11.2098
- Markus, H. (1977). Self-schemata and processing information about the self. Journal of Personality and Social Psychology, 35(2), 63–78. doi:10.1037/0022-3514.35.2.63
- McCaul, K. D., Canevello, A., Mathwig, J., & Klein, W. (2003). Risk communication and worry about breast cancer. Psychology, Health & Medicine, 8(4), 379–389. doi:10.1080/13548500310001604513
- McCaul, K. D., Peters, E., Nelson, W., & Stefanek, M. (2005). Linking decision-making research and cancer prevention and control: Important themes. Health Psychology, 24(Suppl. 4), S106–S110. doi:10.1037/0278-6133.24.4.S106
- McFarland, C., Cheam, A., & Buehler, R. (2007). The perseverance effect in the debriefing paradigm: Replication and extension. Journal of Experimental Social Psychology, 43(2), 233–240. doi:10.1016/j.jesp.2006.01.010
- Michie, S., Weinman, J., Miller, J., Collins, V., Halliday, J., & Marteau, T. M. (2002). Predictive genetic testing: High risk expectations in the face of low risk information. Journal of Behavioral Medicine, 25(1), 33–50. doi:10.1023/A:1013537701374
- Natter, H. M., & Berry, D. C. (2005). Effects of presenting the baseline risk when communicating absolute and relative risk reductions. Psychology, Health & Medicine, 10(4), 326–334. doi:10.1080/13548500500093407
- Olsson, E. M. G., Roth, W. T., & Melin, L. (2010). Psychophysiological characteristics of women suffering from stress-related fatigue. Stress and Health, 26(2), 113–126. doi:10.1002/smi.1271
- Panzer, M., & Renner, B. (2008). To be or not to be at risk: Spontaneous reactions to risk information. Psychology & Health, 23(5), 617–627. doi:10.1080/08870440701606889
- Renner, B. (2004). Biased reasoning: Adaptive responses to health risk feedback. Personality & Social Psychology Bulletin, 30(3), 384–396. doi:10.1177/0146167203261296
- Renner, B., Gamp, M., Schmälzle, R., & Schupp, H. (2015). Health risk perception. In J. Wright (Ed.), International encyclopedia of the social and behavioral sciences (2nd ed., pp. 702–709). Oxford: Elsevier.
- Renner, B., Hahn, A., & Schwarzer, R. (1996). Risiko und Gesundheitsverhalten: Dokumentation der Meßinstrumente des Forschungsprojekts “Berlin Risk Appraisal and Health Motivation Study” (BRAHMS). Berlin: Freie Universität Berlin.
- Renner, B., & Reuter, T. (2012). Predicting vaccination using numerical and affective risk perceptions: The case of A/H1N1 influenza. Vaccine, 30(49), 7019–7026. doi:10.1016/j.vaccine.2012.09.064
- Renner, B., & Schupp, H. (2011). The perception of health risks. In H. S. Friedman (Ed.), Oxford handbook of health psychology (pp. 637–665). New York, NY: Oxford University Press.
- Renner, B., Schüz, B., & Sniehotta, F. F. (2008). Preventive health behavior and adaptive accuracy of risk perceptions. Risk Analysis, 28(3), 741–748. doi:10.1111/j.1539-6924.2008.01047.x
- Rokeach, M. (1973). The nature of human values. New York, NY: Free Press.
- Rothman, A. J., & Kiviniemi, M. T. (1999). Treating people with information: An analysis and review of approaches to communicating health risk information. Journal of the National Cancer Institute. Monographs, 1999(25), 44–51. doi:10.1093/oxfordjournals.jncimonographs.a024207
- Seligman, M. E. P., Railton, P., Baumeister, R. F., & Sripada, C. (2013). Navigating into the future or driven by the past. Perspectives on Psychological Science, 8(2), 119–141. doi:10.1177/1745691612474317
- Siegrist, M. (2013). The necessity for longitudinal studies in risk perception research. Risk Analysis, 33(1), 50–51. doi:10.1111/j.1539-6924.2012.01941.x
- Siegrist, M. (2014). Longitudinal studies on risk research. Risk Analysis, 34(8), 1376–1377. doi:10.1111/risa.12249
- Slovic, P., Peters, E., Finucane, M. L., & Macgregor, D. G. (2005). Affect, risk, and decision making. Health Psychology, 24(4), S35–S40. doi:10.1037/0278-6133.24.4.S35
- Sweeny, K., & Dillard, A. (2014). The effects of expectation disconfirmation on appraisal, affect, and behavioral intentions. Risk Analysis, 34(4), 711–720. doi:10.1111/risa.12129
- Van Gelder, J. L., De Vries, R. E., & Van Der Pligt, J. (2009). Evaluating a dual-process model of risk: Affect and cognition as determinants of risky choice. Journal of Behavioral Decision Making, 22(1), 45–61. doi:10.1002/bdm.610
- Van ‘t Riet, J., & Ruiter, R. A. C. (2013). Defensive reactions to health-promoting information: An overview and implications for future research. Health Psychology Review, 7(Suppl. 1), S104–S136. doi:10.1080/17437199.2011.606782
- Von Dawans, B., Kirschbaum, C., & Heinrichs, M. (2011). The Trier Social Stress Test for Groups (TSST-G): A new research tool for controlled simultaneous social stress exposure in a group format. Psychoneuroendocrinology, 36(4), 514–522. doi:10.1016/j.psyneuen.2010.08.004
- Weber, E. U. (2003, February 13–14). Origins and functions of perceptions of risk. Presentation at NCI Workshop on “Conceptualizing and Measuring Risk Perceptions”, Columbia University, Bethesda, MD.
- Weinstein, N. D. (1998). Accuracy of smokers’ risk perceptions. Annals of Behavioral Medicine, 20(2), 135–140. doi:10.1007/BF02884459
- Weinstein, N. D., Atwood, K., Puleo, E., Fletcher, R., Colditz, G., & Emmons, K. M. (2004). Colon cancer: Risk perceptions and risk communication. Journal of Health Communication, 9(1), 53–65. doi:10.1080/10810730490271647
- Weisman, A. D. (1972). On dying and denying. New York, NY: Human Sciences Press.