
ABSTRACT
Missed opportunities for vaccination (MOV) is an important barrier hindering full immunisation coverage among eligible children. Though factors responsible for MOV are well documented in literature, little attention has been paid to the role of inequalities. The aim of this study is to examine the association between structural or compositional factors and education inequalities in MOV. Blinder-Oaxaca decomposition technique was used to explain the factors contributing to the average gap in missed opportunities for vaccination between uneducated and educated mothers in sub-Saharan Africa using DHS survey data from 35 sub Saharan African countries collected between 2007 and 2016. The sample contained 69,657 children aged 12 to 23 months. We observed a wide variation and inter-country differences in the prevalence of missed opportunity for vaccination across populations and geographical locations. Our results show that the prevalence of MOV in Zimbabwe among uneducated and educated mothers was 9% and 21% respectively while in Gabon corresponding numbers were 85% and 89% respectively. In 15 countries, MOV was significantly prevalent among children born to uneducated mothers (pro-illiterate inequality) while in 5 countries MOV was significantly prevalent among educated mothers (pro-educated inequality). Our results suggest that education-related inequalities in missed opportunities for vaccination are explained by compositional and structural characteristics; and that neighbourhood socio-economic status was the most important contributor to education-related inequalities across countries followed by either the presence of under-five children, media access or household wealth index. The results showed that differential effects such as neighbourhood socio-economic status, presence of under-five children, media access and household wealth index, primarily explained education-related inequality in MOV. Interventions to reduce gaps in education-related inequality in MOV should focus on social determinants of health.
Introduction
Despite global progress towards the goal of 90% vaccine coverage with the first dose of diphtheria-tetanus-pertussis (DTP), childhood mortality remains significantly high from vaccine preventable diseases.Citation1,Citation2 An estimated 23 million infants remain unvaccinated, under-vaccinated and unreached, of which 2–3 million children die each year despite the availability of safe, free and efficacious vaccines.Citation3 Of these deaths, 1.5 million are attributable to diphtheria, neonatal tetanus and pertussis.Citation4
The World Health Organization (WHO) considers missed opportunities for vaccination (MOV) as an important barrier hindering full immunisation coverage among eligible children. MOV occurs when an unvaccinated or partially vaccinated child eligible for vaccination makes contact with the health service but remains unvaccinated or fails to catch up with one or more required doses of the vaccines.Citation4 The WHO strategy on MOV aims to eliminate barriers and subsequently increase immunisation coverage by up to 30% in many settings where immunisation coverage is below national targets.Citation5
Despite remarkable improvement in immunisation coverage and countries adopting immunisation initiatives aimed at reducing the high incidence of MOV, progress to reduce MOV remain sub-optimal. For instance, a recent assessment conducted in Chad and Malawi reveal that “of children attending the medical facilities, 75% do not receive the required vaccines for which they are eligible.”Citation6 This contributes to low immunization coverage and consequently high child mortality.Citation7
The objective of the Global Vaccine Action Plan (GVAP) of the WHO is to end the inequalities in vaccination worldwide by ensuring equitable access to existing vaccines and reaching the unvaccinated children in underserved populations and areas.Citation5 Though factors responsible for incomplete childhood vaccination are well documented in literature (such as maternal education attainment, place of residence, wealth etc),Citation8,Citation9,Citation10,Citation11 little attention has been paid to the role of inequalities or disparities. Findings from previous research indicate that factors such as inadequate access to health services, poor access to vaccine services and socioeconomic status, which are responsible for MOV are influenced by education inequalities.Citation12 Education inequalities remain a fundamental barrier to vaccination.Citation13 Nonetheless, what explains the underlying causes of educational inequalities in missed opportunities for vaccination remain poorly understood. In order to understand what explains the education-related inequality in missed opportunities for vaccination and adapt the relevant strategies for interventions we examined the factors associated to education-related inequalities in missed opportunities for vaccination. The underlying motivation was to account for the causes and extent to which educational inequalities in missed opportunities for vaccination vary across countries in sub Saharan Africa, beyond compositional characteristics (i.e. age, sex, education and occupation).
Methods
Study design and data
This study included data from 35 recent Demographic and Health Surveys (DHS) surveys conducted between 2007 and 2016 in sub-Saharan Africa available as of December 2017. DHS data collected every five years in low- and middle-income countries are nationally representative multi-stage, stratified sampling designs with households as the sampling unit.Citation14 Within each sample household, all women and men meeting the eligibility criteria are interviewed. Because the surveys are not self-weighting, weights are calculated to account for unequal selection probabilities as well as for non-response. With weights applied, survey findings represent the full target populations. The DHS surveys include a household questionnaire, a women's questionnaire, and in most countries, a men's questionnaire. All three DHS questionnaires are implemented across countries with similar interviewer training, supervision, and implementation protocols.
Outcome variable
We used the WHO definition of MOV as the outcome variable. It is defined as a binary variable that takes the value of 1 if the child 12–23 months had any contact with health services who is eligible for vaccination but does not result in the child receiving one or more of the vaccine doses for which he or she is eligible. Contact with health services is defined using the following six variables: skilled birth attendance, baby postnatal check within 2 months, received vitamin A dose in first 2 months after delivery, has a health card and medical treatment of diarrhoea/ fever/cough.
Main determinant variable
Maternal education was categorized as no formal education or educated (at least completed primary education).
Explanatory variables
Individual level factors
The following individual-level factors were included in the models: child's age, sex of the child (male versus female), birth order, number of under five children in the household, maternal age in completed years (15 to 24, 25 to 34, 35 to 49), occupation (working or not working), and media access (radio, television or newspaper). DHS did not collect direct information on household income and expenditure. We used DHS wealth index as a proxy indicator for socioeconomic position. The methods used in calculating DHS wealth index have been described elsewhere.Citation15,Citation16 An index of economic status for each household were constructed using principal components analysis based on the following household variables: number of rooms per house, ownership of car, motorcycle, bicycle, fridge, television and telephone as well as any kind of heating device. From these criteria, the DHS wealth index quintiles (poorest, poorer, middle, richer and richest) were calculated and used in the subsequent modelling.
Neighbourhood-level factors
We used the term neighbourhood to describe clustering within the same geographical living environment. Neighbourhoods were based on sharing a common primary sample unit within the DHS data. The sampling frame for identifying primary sample unit in the DHS is usually the most recent census. This unit of analysis was chosen for two reasons. First, primary sample unit is the most consistent measure of neighbourhood across all the surveys,Citation17 and thus the most appropriate identifier of neighbourhood for this cross-region comparison. Second, for most of the DHS conducted, the sample size per cluster meets the optimum size with a tolerable precision loss.Citation18 We considered neighbourhood socioeconomic disadvantage as a community-level variable in this study. Neighbourhood socioeconomic disadvantage was operationalized with a principal component comprised of the proportion of respondents with: no education (illiterate), unemployed, rural resident, and living below the poverty level (asset index below 20% poorest quintile). A standardized score with mean score of 0 and standard deviation 1 was generated from this index; with higher scores indicative of lower social economic position and vice versa. We divided the resultant scores into five quintiles to allow for nonlinear effects and to enable us provide results that were more readily interpretable in the policy arena.
Statistical analyses
The analytical approach included descriptive statistics, univariable analysis and Blinder-Oaxaca decomposition techniques using logistic regressions. We used descriptive statistics to show the distribution of respondents by the key variables. Values were expressed as absolute numbers (percentages) and means (standard deviation) for categorical and continuous variables respectively. We calculated the risk difference in missed opportunities between the two groups, children born to uneducated or educated mothers. A risk difference greater than 0 suggests that missed opportunities are prevalent among children born to uneducated mothers (pro-illiterate inequality). Conversely, a negative risk difference indicates that missed opportunities for vaccination are prevalent among children born to educated mothers (pro-educated inequality). Finally, we adopted logistic regression method using the pooled cross-sectional data to conduct the Blinder-Oaxaca decomposition analysis.
The Blinder-Oaxaca decompositionCitation19,Citation20 was a counterfactual method with an assumption that children born to uneducated mothers had the same characteristics as their educated counterparts. The Blinder-Oaxaca method allows for the decomposition of the differences in an outcome variable between 2 groups into 2 components. The first component is the “explained” portion of that gap that captures differences in the distributions of the measurable characteristics (referred to as the “compositional” or “endowments”) of these groups. Using this method, we can quantify how much of the gap between the “advantaged” and the “disadvantaged” groups is attributable to differences in specific measurable characteristics. The second component is the “unexplained” part, or structural component which captures the gap due to the differences in the regression coefficients and the unmeasured variables between the two groups. This reflects the remainder of the model not explained by the differences in measurable, objective characteristics. The “unexplained” portion arises from differentials in how the predictor variables are associated with the outcomes for the two groups. This portion would persist even if the disadvantaged group were to attain the same average levels of measured predictor variables as the advantaged group.
Results
Survey and sample characteristics
A total of 69, 657 participants drawn from 35 sub-Saharan African countries participating in the DHS surveys between 2007 and 2016 were included in the analysis. The countries, year of data collection, number of children, MOV and mothers without education are presented in . The median number of children aged 12 to 23 months was 1847 (range: 370 to 5893). Mothers with no formal education ranged from 1% in Zimbabwe to as high as 82% in Burkina Faso.
Table 1. Description of Demographic and Health Surveys data by countries, in sub-Saharan Africa, 2007 to 2016.
presents the descriptive statistics for the final pooled sample. Half of the children were male. The average age of the children was 17 months. About 46% of the mothers were between 25 to 34 years old and about 41% had no formal education. One third of the mothers were not working at the time of the survey.
Table 2. Summary of pooled sample characteristics of the Demographic and Health Surveys data in sub-Saharan Africa.
MOV among the educated and uneducated mothers
shows the rate of MOV among mothers with and without formal education across the 35 countries. The rate of MOV among uneducated mothers ranged from 9.1% in Zimbabwe to 84.8% in Gabon, while it ranged from 19.4% in Burkina Faso to 89.3% in Gabon among educated mothers.
Figure 1. Description of Demographic and Health Surveys data by countries, in sub-Saharan Africa, 2007 to 2016.
Magnitude and variations in education inequality in MOV
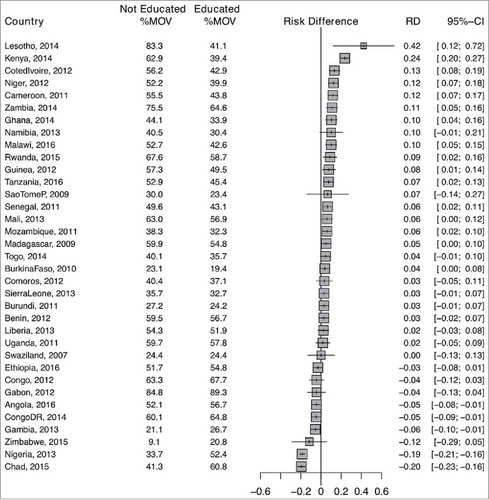
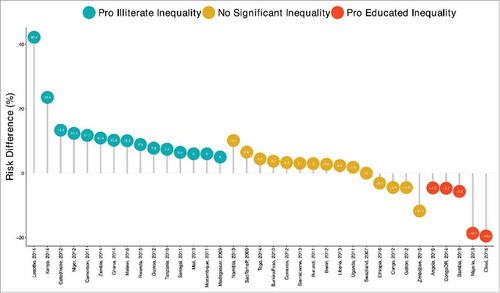
(also see ) shows the risk difference (measure of inequality) between illiterate and educated mothers across the countries studied. Out of the 35 countries included in this analysis, 15 countries showed pro-illiterate inequality (i.e. MOV is prevalent among the illiterate mothers), 5 showed pro-educated inequality (i.e. MOV is prevalent among the educated mothers) and remaining 15 countries showed no statistically significant inequality. Among the countries with statistically significant pro-illiterate inequality, the risk difference ranged from 5% to 42.2%.
Figure 2. Risk difference between children born to uneducated and educated mothers in missed opportunities for vaccination by countries.
Relationship between rate of MOV and inequality
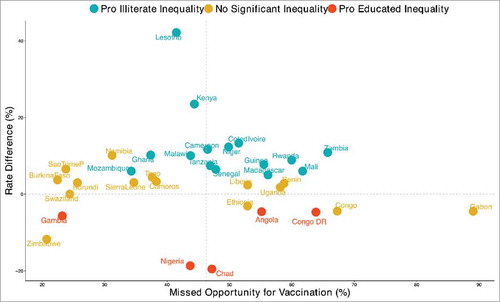
plot the relationship between rate of MOV and inequality for all countries. We grouped countries into four distinct categories:
high MOV and high pro-illiterate inequality such as Zambia
high MOV and high pro-educated inequality such as Gabon
low MOV and high pro-illiterate inequality such as Mozambique
low MOV and high pro-educated inequality such as Nigeria
Figure 3. Scatter plot of rate of missed opportunities for vaccination and risk difference children born to uneducated and educated mothers in sub-Saharan Africa.
Decomposition of education inequality in MOV
and show the detailed decomposition of the part of the inequality that was caused by compositional effects of the determinants. The important factors responsible for the inequality varied across the countries. On average, neighbourhood socio economic status (SES) was the most important factor in most countries. In Tanzania, the largest contributions to the inequality in MOV was neighbourhood SES followed by birth order, media access, household wealth index and under-five children, while in Mozambique the largest contribution was neighbourhood SES followed by household wealth index and media access. However, Mali neighbourhood SES, media access and maternal age were narrowing the inequality in MOV between uneducated and educated mothers.
Figure 4. Contributions of differences in the distribution ‘compositional effect’ of the determinants of missed opportunities for vaccination to the total gap between children born to uneducated and educated mothers.
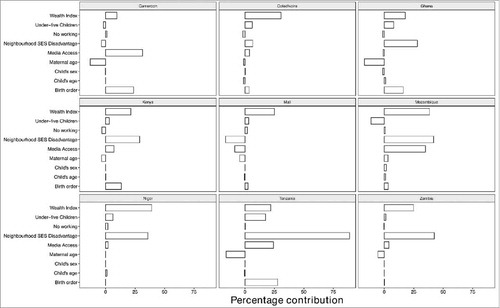
show contributions of differences in the distribution of ‘compositional effect’ of the determinants of missed opportunities for vaccination to the total gap between children born to uneducated and educated mothers.
Discussion
In this study, we used the DHS data to analyse and decompose education related inequalities in 35 sub Saharan African countries. The aim of the study was to improve our understanding of the compositional and structural factors associated with education inequalities in missed opportunities for vaccination. Our results show significant education-related differences in missed opportunities that could be explained by structural and compositional factors nested within neighborhoods and at the national level. Furthermore, the results revealed a wide geographic variation (or) inter-country differences in prevalence of MOV. These inter country differences are probably due to differences in country characteristics, policies, strategies and intervention that target missed opportunities. Previous research has found similar variance in missed opportunity patterns compared to our study.Citation21
Our results show unequal distribution in the missed opportunities for vaccination between educated and uneducated mothers, suggesting the presence of education inequalities. In 15 countries, missed opportunities for vaccination were significantly prevalent among children born to uneducated mothers (pro-illiterate inequality) while in 5 countries MOV was significantly among educated mothers (pro-educated inequality). Our measure of inequality (risk difference) among countries with statistically significant pro-illiterate inequalities show that 50 to 422 per 1000 of children born to uneducated mothers will miss opportunities for vaccination compared to educated mothers. Our interpretation of the risk difference in pro-educated inequalities suggest a decrement of risk of 195 per 1000 and 46 per 1000 in Chad and Angola respectively. Overall educational characteristics are an important factor in the determination of MOV. This finding corresponds to previous studies that found children whose mothers were educated were associated to a range of positive outcomes such as child immunisation.Citation8 It is therefore important for countries to develop public health policies and programmes that target illiterate mothers on the benefits of vaccination. These strategies however demand targeted messages that could be communicated in local languages, political will and involvement of the local community leaders.
In our study, compositional effects of the determinants were mainly responsible for most of the inequality in MOV between the uneducated and educated mothers in Tanzania, Zambia and Mozambique. While in Mali and Côte d'Ivoire structural effects of the determinants were responsible for most of the inequality in MOV. Due to our limitations in the model of analysis, we were unable to explain the precise predicator variables associated to the outcome measure. However, the decomposition of the analysis have shown that compositional factors such as neighbourhood SES was most important contributor to education-related inequalities across countries followed by either under-five children, media access or household wealth index. Reducing education inequalities in MOV require understanding the connection between composition and the context in which people live. Focusing only on compositional factors at an individual level ignoring structural effects generates conceptual and practical problems. This finding underscores the importance of improving compositional and structural characteristic that exists such as neighbourhood SES, number of under-five children in the household, media access or household wealth index in order to reduce education-related inequality in missed opportunities for vaccination. Results from previous studies illustrate the importance of this nuance of individual, neighbour and national factors in MOV.Citation22
Mapping out relationships between rate of MOV and inequality, we interestingly found that some countries such as Mozambique had a low MOV and high pro-illiterate inequality while Zambia had a high MOV and high pro-illiterate inequality. These are probably explained by several factors such as geographical access to health services (e.g. proximity to the health facility), non-availability of vaccines and neighbourhoods with high or low employment status (e.g. able to afford or unable to take days off from work when a child is ill). It does not necessarily indicate that educated mothers with high MOV were under the influence of uneducated mothers within their neighbourhoods, but we believe that this may prove to be the case if educated mothers adopted the norms, values and behaviour prevailing in the neighbourhood. There is need for further research to examine behaviours of educated mothers and the reasons why they refrain from taking their child to a vaccination session or whether this has any connection between loss of economic costs and long waiting hours at the health facility.
Previous studies have shown children of mothers who are educated and dwelling in rural or low income areas are unlikely to immunise their children.Citation23,Citation24 It might seem counterintuitive but some studies have found that the highly educated folks who knows more about the role of vaccines often erodes vaccination efforts because they decide not to vaccinate, or choose to vaccinate their children partially.Citation25,Citation26
Overall, our findings are consistent with the literature on compositional and structure effects, which has shown that residents in high socioeconomic areas have more positive outcomes-related neighbourhood characteristics than residents of low socioeconomic areas.Citation27,Citation28 This finding highlight the need for countries with high MOV yet with high pro-illiterate inequalities to rethink their national policies by learning from other countries with a low MOV and pro-educated inequalities. For example, what is it that Zimbabwe (i.e. low MOV and pro-education inequalities) is doing different from Zambia (i.e. high MOV and high inequalities)? By identifying these factors, public-health officials may be able to design better strategies that address some of the differences.
Our research has several limitations. First, this study solely accounted for six variables (e.g. skilled birth attendance, baby postnatal check within 2 months, received vitamin A dose in first 2 months after delivery, has a health card and received medical treatment for diarrhoea/ fever/cough) in its definition of missed opportunities for vaccination. We deliberately excluded possible variables such as family planning related visits, antenatal visits and anaemia referrals from the definition because these variables were unlikely to establish missed opportunities if a child was left behind during their visit to the health facility. In light of this, the burden of missed opportunities for vaccination may be under-estimated. Second, the DHS survey questionnaire does not contain data on household income or expenditure as a result, we used assets-based wealth index as a proxy indicator of household economic status. The implication of this is that our results may not be generalizable in settings where direct measurements of income and expenditure are collected. Third, while multilevel analysis is now considered as the most appropriate method to understand disparities and to monitor health care performance,Citation29 Blinder-Oaxaca decomposition analysis does not clearly allow causal interpretation of the results. However, it provides robust evidence on the disparities after controlling for target factors. Thus, future research that use survey data are needed to fully examine the association of structural and compositional factors to education inequalities in MOV. In this way, analysis of the survey data may give a true and reliable reflection of the outcomes under study opposed to theorising the causes of education inequalities in MOV.
In summary, this study found that education related inequality are relatively high among children whose mothers were educationally disadvantaged. Furthermore, neighbourhood social economic status, media access, under five children and wealth index are limiting factors for missed opportunities. It is important that affected countries focus on addressing these factors to avert missed opportunities and create an end to the existing inequality in vaccination and reaching unvaccinated children in underserved populations. While location-specific enquiry is needed, lessons could be drawn from countries like Zimbabwe where missed opportunities and inequality are low. The key question to ask is what is it that Zimbabwe is doing that other countries like Zambia with high missed opportunities for vaccination and high inequality are not doing?
Declarations
Ethics approval and consent to participate
This study was based on an analysis of existing survey data with all identifier information removed. The survey was approved by the Ethics Committee of the ICF Macro at Fairfax, Virginia in the USA and by the National Ethics Committees in their respective countries. All study participants gave informed consent before participation and all information was collected confidentially.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Authors' contribution
OAU and CSW conceived the study. OAU and CSW obtained funding for the study. OAU collected and analysed initial data. AA, ABW, CSW, DN, EZS, ABW and OAU participated contributed in refining the data analysis. OAU and EZS wrote the first manuscript. AA, ABW, CSW, DN, EZS, GB, JO, OAU, TO and SY contributed to further analysis, interpreting and shaping of the argument of the manuscript and participated in writing the final draft of the manuscript. All the authors read and approved the final manuscript.
KHVI_A_1460985_Supplemental.docx
Download MS Word (121.2 KB)Acknowledgments
The authors are grateful to DHS Program for providing them with the survey data. Olalekan Uthman is supported by the National Institute of Health Research using Official Development Assistance (ODA) funding. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research.
Additional information
Funding
References
- Centers for Disease Control and Prevention (CDC). Global routine vaccination coverage, 2010. MMWR Morb Mortal Wkly Rep. 2011 November 11;60(44):1520–2.
- Machingaidze S, Wiysonge CS, Hussey GD. Strengthening the expanded programme on immunization in Africa: Looking beyond 2015. PLoS Medicine. 2013;10(3):e1001405. doi:10.1371/journal.pmed.1001405. PMID:23526886.
- Global Elimination of Measles. [Internet]; c2009 [cited 2017 January/11]. Available from: http://apps.who.int/ gb/ebwha/pdf_files/EB125/B125_4-en.pdf.
- Missed Opportunities for Vaccination (MOV) Strategy. [Internet]; c2017 [cited 2018 January/11]. Available from: http://www.who.int/immunization/programmes_systems/policies_strategies/MOV/en/.
- World Health Organization. Global vaccine action plan 2011–2020. Global Vaccine Action Plan 2011–2020. 2013.
- Meeting of the Strategic Advisory Group of Experts on immunization, October 2015 – conclusions and recommendations [Internet]; c2015 [cited 2018 January/11]. Available from: http://www.who.int/immunization/policy/sage/en/.
- McGovern ME, Canning D. Vaccination and all-cause child mortality from 1985 to 2011: Global evidence from the demographic and health surveys. Am J Epidemiol. 2015;182(9):791–8. doi:10.1093/aje/kwv125. PMID:26453618.
- Adedokun ST, Uthman OA, Adekanmbi VT, Wiysonge CS. Incomplete childhood immunization in nigeria: A multilevel analysis of individual and contextual factors. BMC Public Health. 2017;17(1):236. doi:10.1186/s12889-017-4137-7. PMID:28270125.
- Abdulraheem I, Onajole A, Jimoh A, Oladipo A. Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children. Journal of Public Health and Epidemiology. 2011;3(4):194–203.
- Jani JV, De Schacht C, Jani IV, Bjune G. Risk factors for incomplete vaccination and missed opportunity for immunization in rural mozambique. BMC Public Health. 2008;8(1):161. doi:10.1186/1471-2458-8-161. PMID:18485194.
- Santoli JM, SziIagyi PG, Rodewald LE. Barriers to immunization and missed opportunities. Pediatr Ann. 1998;27(6):366–74. doi:10.3928/0090-4481-19980601-11. PMID:9648171.
- Pfeffer FT. Persistent inequality in educational attainment and its institutional context. Eur. Sociol. Rev. 2008;24(5):543–65. doi:10.1093/esr/jcn026.
- Esposito S, Principi N, Cornaglia G. Barriers to the vaccination of children and adolescents and possible solutions. Clin Microbiol Infect. 2014;20(s5):25–31. doi:10.1111/1469-0691.12447. PMID:24354949.
- Rutstein SO, Rojas G. Guide to DHS statistics. Calverton, MD: ORC Macro; 2006.
- Montgomery MR, Gragnolati M, Burke KA, Paredes E. Measuring living standards with proxy variables. Demography. 2000;37(2):155–74. doi:10.2307/2648118. PMID:10836174.
- Vyas S, Kumaranayake L. Constructing socio-economic status indices: How to use principal components analysis. Health Pol. Plan. 2006;21(6):459–68. doi:10.1093/heapol/czl029. PMID:17030551.
- Griffiths P, Madise N, Whitworth A, Matthews Z. A tale of two continents: A multilevel comparison of the determinants of child nutritional status from selected African and Indian regions. Health Place. 2004;10(2):183–99. doi:10.1016/j.healthplace.2003.07.001. PMID:15019912.
- Kravdal Ø. A. simulation-based assessment of the bias produced when using averages from small DHS clusters as contextual variables in multilevel models. Demogr. Res. 2006;15:1–20. doi:10.4054/DemRes.2006.15.1.
- Blinder AS. Wage discrimination: Reduced form and structural estimates. J Hum Resour. 1973;8(4):436–455. doi:10.2307/144855.
- Oaxaca R. Male-female wage differentials in urban labor markets. International Economic Review. 1973;14(4):693–709. doi:10.2307/2525981.
- Restrepo-Méndez MC, Barros AJ, Wong KL, Johnson HL, Pariyo G, Wehrmeister FC, Victora CG. Missed opportunities in full immunization coverage: Findings from low-and lower-middle-income countries. Global Health Action. 2016;9(1):30963. doi:10.3402/gha.v9.30963. PMID:27146444.
- Wiysonge CS, Uthman OA, Ndumbe PM, Hussey GD. Individual and contextual factors associated with low childhood immunisation coverage in sub-Saharan Africa: A multilevel analysis. PLoS One. 2012;7(5):e37905. doi:10.1371/journal.pone.0037905. PMID:22662247.
- Kim SS, Frimpong JA, Rivers PA, Kronenfeld JJ. Effects of maternal and provider characteristics on up-to-date immunization status of children aged 19 to 35 months. Am J Public Health. 2007;97(2):259–66. doi:10.2105/AJPH.2005.076661. PMID:17194865.
- Pearce A, Law C, Elliman D, Cole TJ, Bedford H, Millennium Cohort Study Child Health Group. Factors associated with uptake of measles, mumps, and rubella vaccine (MMR) and use of single antigen vaccines in a contemporary UK cohort: Prospective cohort study. BMJ. 2008 April 05;336(7647):754–7. doi:10.1136/bmj.39489.590671.25.
- Ogilvie G, Anderson M, Marra F, McNeil S, Pielak K, Dawar M, McIvor M, Ehlen T, Dobson S, Money D. A population-based evaluation of a publicly funded, school-based HPV vaccine program in British Columbia, Canada: Parental factors associated with HPV vaccine receipt. PLoS Medicine. 2010;7(5):e1000270. doi:10.1371/journal.pmed.1000270. PMID:20454567.
- Kien VD, Van Minh H, Giang KB, Mai VQ, Tuan NT, Quam MB. Trends in childhood measles vaccination highlight socioeconomic inequalities in Vietnam. Int J Public Health. 2017;62(1):41–9. doi:10.1007/s00038-016-0899-4. PMID:27695901.
- Lee K, Han K, Kim JY, Nam GE, Han B, Shin K, Lee A, Ko BJ. Socioeconomic status and other related factors of seasonal influenza vaccination in the South Korean adult population based on a nationwide cross-sectional study. PLoS One. 2015;10(2):e0117305. doi:10.1371/journal.pone.0117305. PMID:25646847.
- Martens PJ, Chateau DG, Burland EM, Finlayson GS, Smith MJ, Taylor CR, Brownell MD, Nickel NC, Katz A, Bolton JM. The effect of neighborhood socioeconomic status on education and health outcomes for children living in social housing. Am J Public Health. 2014;104(11):2103–13. doi:10.2105/AJPH.2014.302133. PMID:25211758.
- Merlo J, Gerdtham UG, Eckerlund I, Hakansson S, Otterblad-Olausson P, Pakkanen M, Lindqvist PG. Hospital level of care and neonatal mortality in low- and high-risk deliveries: Reassessing the question in Sweden by multilevel analysis. Med Care. 2005 Nov;43(11):1092–100. doi:10.1097/01.mlr.0000182484.14608.b9.