
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Background: Specification of vaccination cost of children would help policymakers in determining the nation-wide budget needed for the maintenance of the vaccination program. The budget came these days under scrutiny due to the imposed sanctions tightening the public funds. This study aims at estimating the cost of vaccination in southeastern Iran for obtaining more accurate budget projections.
Methods: Fifty-two healthcare centers from 10 cities in south-east Iran participated in using a quota sampling method for their selection. A bottom-up method determined the human resource use, the consumption, and the overhead costs to estimate the cost of vaccination. Data collection used a standard tool that was adjusted to local conditions. Sensitivity analyses were performed.
Results: The overall vaccination cost for the region was estimated at around 5,984,000 USD for the year 2015. Salaries took the largest part of the cost estimate (64%), while vaccine cost and its equipment were much lower (22%). The average cost per vaccine dose administrated was 40.94 USD. Sensitivity analysis of the population and inflation rate indicates that the vaccination cost may fluctuate between 37% and 53% over 6 years (2021) from the data of 2015.
Conclusion: Maintaining vaccination has a substantial cost. The results of the study will support the budget planning and decision making and will define more precisely the resource allocation needed for maintaining the vaccination at a high level across the country. It may also help to facilitate the assessment of cost-benefit and cost-effectiveness analysis when new vaccines should be introduced.
KEYWORDS:
Introduction
Suppressing contagious diseases in childhood through an Expanded Program of Immunization (EPI) is one of the most cost-efficient interventions in public health.Citation1,Citation2 The first EPI-program in Iran was initiated in 1974. It recommended vaccines against six diseases including tuberculosis, poliomyelitis, diphtheria, tetanus, measles, and whooping cough. In 1998, the vaccination against hepatitis B was added following the recommendations of the World Health Organization (WHO). The program should approximately avoid 2 to 3 million deaths of children per year in Iran.Citation3
This achievement was only possible having an extended primary health-care organization in place across the country by which vaccination is implemented in Iran. The organization has a network of health houses in small villages, rural health centers in larger villages, urban-rural health centers for mixed city-villages, and urban health centers serving only the urban populations.Citation4–6 The national vaccination program has been quite successful for the country, achieving important goals of disease control, elimination, and eradication of infections such as measles, rubella, and neonatal tetanus. It provides stable free situations of poliomyelitis, and it controls the spread of diphtheria and hepatitis B. The Ministry of Health and Medical Education (MoHME) was able to obtain very high vaccine coverage rates of 99%, putting also in place a permanent monitoring system of vaccine-preventable diseases and guaranteeing a suitable cold chain program for transporting the vaccines throughout the country.Citation7
Because Iran is under international sanctions for several years, public funds are getting tight and experiences from the past about vaccination expenses cannot be utilized anymore for projecting the vaccination cost of the next decade for the country. Therefore, new determination of those expenditures is urgently needed. Since the country is a vast territory, trying to include in the study all the different parts of the country were not feasible. The region where vaccination activities were best operational was therefore selected and that region is the southeastern territories of Iran.
Cost estimate of vaccination can be very different across countries. It highly depends on several parameters such as facilities available, volume of vaccines consumed and wasted, logistics for transporting the vaccines to the centers where they will be administrated, and the vaccine prices, to name a few ones.Citation8 With the introduction of the new vaccines, it is also expected that the overall cost will dramatically increase.Citation8,Citation9 Reported by the WHO is the expense of immunizing children in low-income countries that have significantly increased from 1.1 billion USD in 2000 to 2.5 billion USD in 2005.Citation10 For our study here we followed a method of evaluation done by a group of experts who recently assessed the vaccination cost in low and middle-income countries focusing their evaluation on routine and supplemental immunization activities.Citation11 Our approach has evaluated the former type of vaccination cost only.
Methods
The study is descriptive and retrospective in its design measuring the cost of vaccination over 1 year, namely for the year 2015. The population includes the children attending the different types of the participating health centers in the region. The first selection of 100 health centers of the 490 available was made in 10 cities through quota sampling. Since vaccines were not administrated in all of the rural centers, along with a lack of cooperation of some centers, only 52 centers participated in the study. Four were urban centers, 5 urban-rural, 4 rural, and 39 were health houses.Citation9,Citation12
The seven vaccines considered in this evaluation include Bacillus Calmette-Guerin (BCG) against tuberculosis, the hepatitis B vaccine at birth, the oral polio vaccine (OPV), the inactivated polio vaccine (IPV), the pentavalent combination vaccine against diphtheria, tetanus, pertussis, Haemophilus influenza type B, and hepatitis B (DTP-HepB-Hib) at month 2, 4, and 6, the triple combination vaccine DTP at month 18 and 6 years and the combination vaccine against measles, mumps, and rubella (MMR).
A bottom-up approach was used for measuring the cost. Its advantage is the possibility to allocate for each activity in the organization a shared cost related to vaccination within each health-care unit under study.Citation11 The following six steps were applied using interviews and observational methods to collect the information: identifying and defining all the activities at each center; type of activity and operation related to vaccination; output of those latter activities through the vaccines given; direct cost estimates of these activities; attributing cost of shared activities in each center (overhead costs); cost estimate per output using cost per activity + shared activities.
Data on personnel salary, equipment, and number of vaccine doses were collected in each participating center.Citation13 Data on cost of consumer goods (e.g. vaccines, syringes, and safety boxes), of human resources (e.g. vaccine administration, headquarter supervision, and ambulance units), and shared cost at the unit (e.g. transportation and fuel, repair and maintenance of vehicles and buildings, energy, depreciation of the equipment employed for the cold chain, vehicles, buildings, and other equipment) were all considered (see ). Costs were converted in USD according to the currency exchange rate at the time of doing the study.Citation14
Table 1. Type of centers, cost variables, and units for sharing activities to estimate cost of the different activities in a health center
Data collection and analysis
Data collection used a standard, pre-tested tool developed by the Bill and Melinda Gates Foundation,Citation15 that was adjusted to the local conditions. The modifications added to the tool were first approved by the Ministry of Health before its general use. The data were collected studying local documents and performing local interviews and observations. The researchers determined the duration of vaccination activities via in-person studies using the technique of time and motion observation. Using an expert-panel approach, the participants were asked to state their opinion regarding the times obtained. They were accordingly adjusted if large discrepancies were noted. The proportion of time dedicated to vaccination was determined from the working hours split by the time devoted to the different vaccination activities. If in 1 h work time, 3 activities were devoted to vaccination related to 3 min, 7 min and 15 min, that working hour was assigned for 25 min to the vaccination program. Overall income of the personnel who participated in the vaccination process was divided by the vaccination activities according to the annual paid hours. Again, if the 25 min assigned to the 3 activities of vaccination were performed by 3 different people with a different salary, each activity was adjusted in cost, related to the salary of the person doing the job. All the data were stored into one database and analyzed using the statistical software package, STATA 14.
The output selected for the study is the cost measured per vaccine dose given that is vaccine type-specific and context-specific per health center type. The cost of vaccination is reported per child up to the age of 6 years (cost per capita) as this is the period during which he/she will receive all the different vaccines. The overall cost of vaccination per year for the region is the sum of all the children at the age of 6 years in the region who received the full vaccination schedule at that age, multiplied by the cost of vaccination that includes all the cost of administration and handling with the cost of the vaccines. We report the overall cost for the region with the relative split of the cost items in different categories including personnel cost, vaccines, and equipment, building, transportation, and fuel, cold chain infrastructure and overhead cost. Cost will also be reported by the age-group in the children and by health center type.
Estimating the future cost of vaccination
Predictions for the vaccination cost of children <6 years old for the year 2021 was carried out in two steps. First, estimates of the birth cohort for the year 2021 were calculated using time-series data of the birth cohort in 2015. In a second step the estimated child population of the year 2021 is multiplied by the cost of vaccination one child (0 to 6 year) using the following formula:
sum of the cost of vaccination one child from birth to age 6 years old in 2015,
i: inflation rate, 11.9% for 2015Citation16
n: number of years
To generalize the results across the country, sensitivity analysis was performed on the variables of inflation rate and under-6 years old population. In sensitivity analysis, parameters were tested of the population growth rate of children <6 years old along with a range of change of ±20% and of the inflation rate at 20% and 25% instead of 11.9% now.
Results
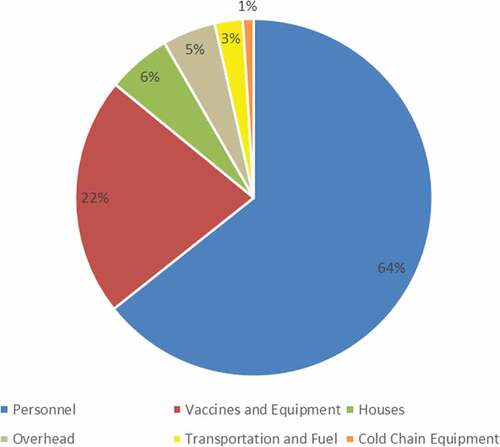
and summarize the share of the different cost items from the overall cost in the health centers assessed. The share of salary cost, vaccine, and equipment cost, and other costs were 64%, 22%, and 14% of the overall cost, respectively. The overall cost of vaccination for the region was estimated at 5,984,191.59 USD. Surprisingly, the cost of the cold chain infrastructure was only 1%.
Table 2. Cost-sharing of each cost items for different vaccine
Figure 1. The share of the different cost items as part of the overall cost of vaccination
specifies the vaccine cost per dose and per vaccine type for different age groups. Vaccines for children at 18 months old had the highest cost, due to the high number of vaccines to be given and the high price for combination vaccines. The lowest cost was for the age-group at 12 months old. The overall cost of vaccination from birth to 1-year-old was 443.02 USD. Finally, the overall cost per child under the age of 6 years old is 655.11 USD. The average cost per dose is given 40.94 USD ().
Table 3. Cost of vaccination per dose per vaccine type and for different age groups (USD)
reports the cost per vaccine dose and per vaccine type for the different health center types, urban, urban-rural, rural, and health houses. The highest overall vaccination costs are for urban centers (923,982 USD). The cost of vaccination per child is the highest in health houses (884.88 USD). The cost per dose and per vaccine type (except for BCG and Hepatitis B, which were not administrated in all centers) were the same in urban, urban-rural, and rural centers.
Table 4. Cost per vaccine dose and per vaccine type for the different health centers (USD)
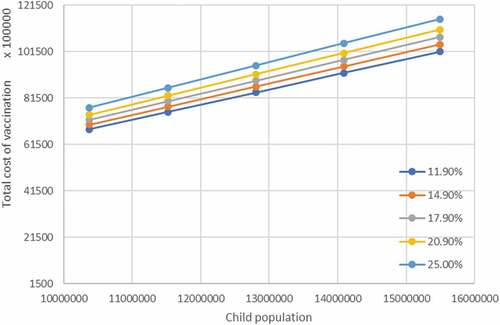
reports the total cost estimates for vaccination of the region 6 years from 2015. The population sensitivity analysis indicates that in comparison to the base case (n = 12,806,622 children), the cost may vary between −25% and +17% if we expect −20 to +20 growth rate. The sensitivity results for the inflation rate indicate that the costs may vary between 37% and 52%. We combined the results in the two-way sensitivity analysis .
Table 5. One-way sensitivity analysis on uncertain parameters of the projection cost
Figure 2. Two-way sensitivity analysis changing the child population size and the inflation rate on cost (hypothetical numbers)
Discussion
Seven different vaccines are administrated today in the national vaccination program in Iran. The results indicated that in the studied region with high vaccine coverage, the total vaccination cost of children up to the age of 6 years old is 5,984,191.6 USD. The average cost per dose is estimated at 40.94 USD. The question raises whether this cost is high or not? Can we do a comparison with other countries that are equivalent to Iran? Several studies have investigated the costs of routine vaccination including studies in Rwanda, Moldova, Honduras, Ghana, Gambia, Benin, and Zambia.Citation1,Citation9,Citation12,Citation17–20 summarizes the cost results and we included the cost of Iran from our study here (last row).
Table 6. Results of the vaccination cost of different countries (USD)
As indicated in , the cost per vaccine dose in Iran is much higher than in other countries. Even though the difference was decreased by adjusting the vaccination cost in the other countries to that of the year 2015, in Iran it is still much higher. One explanation for that big difference is the provision of services to the many health houses in the country. While the number of people visiting those places is low, the price to pay for getting and maintaining the vaccination program in those places could be very high which increases the overall cost of service provision. Other reasons are high geographical distribution of the study area and the long distance between health houses. The problem becomes more serious when considering that the vaccine is used for children in different doses and ages, which need more travel by health houses’ personnel. However, all vaccine-related costs have been taken from the Iranian Ministry of Health and Medical Education, which is the only available source in Iran for this information.
As indicated in the study, 64% of the total vaccination cost is related to the salary, while only 22% to vaccine cost and equipment. These percent costs are in accordance with other studies. A study in Ghana confirmed that the proportion of salary cost and vaccine and equipment cost to the overall vaccination cost were 61% and 19%, respectively.Citation19 Another study in Honduras also revealed that salaries (54%) and vaccines and equipment (25%) had the highest share of the total vaccination cost.Citation18 A study in Zambia indicated that salaries and vaccines and equipment cost were responsible for 49% and 17% of the total vaccination costs, respectively.Citation9 Variations in the % across the different countries are possibly due to differences in payment methods, in unit costs and in differences of the health-care systems of the countries studied.
Meanwhile, the average vaccination cost per capita in Iran was 443 USD for a child less than 1y old. That absolute number is not in accordance with the other studies. It could be that the search for getting a 100% coverage rate of vaccination in Iran, may also explain the big difference in cost as it increases the service providers’ costs.
In urban-rural health centers and in health houses, the share of vaccination cost to the overall cost of the center was the highest, because the focus of those centers is on prevention and control of diseases in their catchment area. These centers do not provide other clinical services. Therefore, the fact that the vaccination cost is high in those centers, shouldn’t be such a surprise.
The analysis of the future financial cost of vaccination suggests that the per capita cost of vaccination could be estimated between 1040 and 1370 USD in 2021. However, due to the high inflation rate in Iran, a different variation range was considered.
Though the vaccination cost seems high, another recent study about vaccination in Iran indicated that the cost imposed on society by having no vaccination in place could approximate $31 million, which is at least twice the cost measured for implementing vaccination.Citation21
Our estimations can provide great support for political decision-makers in health care to finance and plan the vaccination cost that maintains a high coverage rate.
The current study has limitations. First and foremost, the region under study may not be the best representative one for all of Iran. Since the area of study is vast, with scattered cities and villages, the costs of service providers could be very high. Another limitation was using timing to determine vaccination activities only for some, not all centers, and therefore using this timing for other centers. Another issue is that the oral polio vaccine was the only form of vaccine prescribed to children at the time of the study, but now according to WHO and national policies to eradicate poliomyelitis cases, both oral and injectable forms of the vaccine are used for vaccinating children.
Conclusion
This study provides reference information about the current cost of vaccination in Iran. Those estimates are possibly impacted by what is happening at the international level of getting imposed sanctions for the country that reduce the availability of enough public funds. However, having those data now available, it could help the planning for optimum utilization of the limited resources. It may also help in assessing the cost-benefit and cost-effectiveness evaluation of new vaccines to be introduced.
The estimated cost of vaccination is substantial for maintaining the vaccination status at a high level as it is now in the country. For the better planning, it was, therefore, necessary to get a proper evaluation of all the different aspects related to the correct implementation of vaccination.
Abbreviations
| EPI | = | Expanded program of immunization |
| WHO | = | World Health Organization |
| CRS | = | Congenital rubella syndrome |
| RI | = | Routine immunization |
| BCG | = | Bacillus Calmette-Guerin |
| OPV | = | Oral Polio Vaccine\ |
| IPV | = | Inactivated Polio Vaccine |
| DTP | = | Diphtheria–Tetanus–Pertussis |
| MMR | = | Measles–Mumps–Rubella |
Authors’ contributions
RG, MTG, SA, and MN contributed to the conception and design of the CRCT. RG and MTG contributed to the acquisition of the data. RG and MTG performed the analysis. All authors contributed to the interpretation of the results. MTG drafted the manuscript. All authors revisited the manuscript critically. All authors read and approved the final manuscript.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Availability of data and materials
The datasets used and analyzed are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Goguadze K, Chikovani I, Gaberi C, Maceira D, Uchaneishvili M, Chkhaidze N, Gotsadze G. Costs of routine immunization services in Moldova: findings of a facility-based costing study. Vaccine. 2015;33(Suppl 1):A60–5. doi:10.1016/j.vaccine.2014.12.034.
- Geng F, Suharlim C, Brenzel L, Resch SC, Menzies NA. The cost structure of routine infant immunization services: a systematic analysis of six countries. Health Policy Plan. 2017;32:1174–84. doi:10.1093/heapol/czx067.
- Nikfarjam A, Shamshiri A, Hasanpour Z, Khalili M. Status of vaccination coverage in children 24 months to 6 years in urban and high risk areas covered by Tehran University of medical sciences. Iran J Epidemiol. 2016;11:10–19. [In Persian].
- World Health Organization. Health system profile, Islamic Republic of Iran. Regional health systems observatory, WHO eastern Mediterranean regional office. 2006.
- Asadi-Lari M, Sayyari AA, Akbari ME, Gray D. Public health improvement in Iran–lessons from the last 20 years. Public Health. 2004;118:395–402. doi:10.1016/j.puhe.2004.05.011.
- Tabrizi JS, Pourasghar F, Gholamzadeh Nikjoo R. Status of Iran’s primary health care system in terms of health systems control Knobs: A review article. Iran J Public Health. 2017;46:1156–66.
- Moradi-Lakeh M, Esteghamati A. National immunization program in Iran: whys and why nots. Hum Vaccin Immunother. 2013;9:112–14. doi:10.4161/hv.22521.
- Brenzel L, Young D, Walker DG. Costs and financing of routine immunization: approach and selected findings of a multi-country study (EPIC). Vaccine. 2015;33(Suppl 1):A13–20. doi:10.1016/j.vaccine.2014.12.066.
- Schütte C, Chansa C, Marinda E, Guthrie TA, Banda S, Nombewu Z, Motlogelwa K, Lervik M, Brenzel L, Kinghorn A, et al. Cost analysis of routine immunisation in Zambia. Vaccine. 2015;33:A47–A52. doi:10.1016/j.vaccine.2014.12.040.
- Wolfson LJ, Gasse F, Lee-Martin S-P, Lydon P, Magan A, Tibouti A, et al. Estimating the costs of achieving the WHO-UNICEF global immunization vision and strategy, 2006–2015. Bull World Health Organ. 2008;86:27–39. doi:10.2471/BLT.07.045096.
- Chapko MK, Liu CF, Perkins M, Li YF, Fortney JC, Maciejewski ML. Equivalence of two healthcare costing methods: bottom‐up and top‐down. Health Econ. 2009;18:1188–201. doi:10.1002/hec.1422.
- Ahanhanzo CD, Huang XX, Le Gargasson J-B, Sossou J, Nyonator F, Colombini A, Gessner BD. Determinants of routine immunization costing in Benin and Ghana in 2011. Vaccine. 2015;33:A66–A71. doi:10.1016/j.vaccine.2014.12.069.
- Drummond MF, Sculpher MJ, Claxton K, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes. Oxford: Oxford University Press; 2015.
- Central bank of the islamic republic of iran. Exchange rate.
- Brenzel L. Common approach to the costing and financing analyses for routine immunization and New Vaccine Introduction (NUVI). Washington DC: Bill & Melinda Gates Foundation; 2014.
- Central bank of the islamic republic of iran. CPI and Inflation.
- Ngabo F, Levin A, Wang SA, Gatera M, Rugambwa C, Kayonga C, Donnen P, Lepage P, Hutubessy R. A cost comparison of introducing and delivering pneumococcal, rotavirus and human papillomavirus vaccines in Rwanda. Vaccine. 2015 Dec 16;33(51):7357–63. doi:10.1016/j.vaccine.2015.10.022.
- Janusz CB, Castaneda-Orjuela C, Molina Aguilera IB, Felix Garcia AG, Mendoza L, Diaz IY, Resch SC. Examining the cost of delivering routine immunization in Honduras. Vaccine. 2015;33(Suppl 1):A53–9. doi:10.1016/j.vaccine.2015.01.016.
- Le Gargasson JB, Nyonator FK, Adibo M, Gessner BD, Colombini A. Costs of routine immunization and the introduction of new and underutilized vaccines in Ghana. Vaccine. 2015;33(Suppl 1):A40–6. doi:10.1016/j.vaccine.2014.12.081.
- Usuf E, Mackenzie G, Lowe-Jallow Y, Boye B, Atherly D, Suraratdecha C, Griffiths UK. Costs of vaccine delivery in the Gambia before and after, pentavalent and pneumococcal conjugate vaccine introductions. Vaccine. 2014;32:1975–81. doi:10.1016/j.vaccine.2014.01.045.
- Mousavi Jarrahi Y, Zahraei SM, Sadigh N, Esmaeelpoor Langeroudy K, Khodadost M, Ranjbaran M, Sanjari Moghaddam A, Besharat M, Mosavi Jarrahi A. The cost effectiveness of rotavirus vaccination in Iran. Hum Vaccin Immunother. 2016;12:794–800. doi:10.1080/21645515.2015.1087626.
Appendix
Table A1. Cost item of employees salary