
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Objective: Hand, foot, and mouth disease (HFMD) is an important public health issue in China. Although efficacy has been demonstrated by randomized controlled trials, the evidence for effectiveness of the monovalent Enterovirus 71 (EV71) vaccine against HFMD remains unknown. This study aimed to assess the vaccine effectiveness for HFMD in Guangzhou, China.
Methods: Routinely collected vaccination and HFMD surveillance data were captured from the China Information System for Disease Control and Prevention. We estimated the EV71 vaccine effectiveness using spatial ecologic and time-series analysis approaches.
Results: A total of 174,002 HFMD cases under 5 years of age were reported to the Guangzhou, China surveillance system from January 2016 to December 2018. A total of 408,664 children completed a two-dose EV71 vaccination series. In an ecologic analysis, a two-dose EV71 vaccination rate above the median conferred lower HFMD risk relative to a vaccination rate below the median (ratio ratio = 0.955, 95% confidence interval (CI): 0.949, 0.962; P < .001). In the time-series approach, 0.9% fewer HFMD cases were associated with a 1% increase in the two-dose EV71 vaccination rate, but without statistical significance (P = .094). However, we detected statistically significant protective associations for HFMD among children 3 years of age (0.9% fewer HFMD cases with a 1% increased vaccination rate; P = .046), and for EV71 (1.4%; P = .012) and “other viruses” (1.3%; P = .002), although not for Coxsackievirus A16 (CVA16).
Conclusion: Our findings, based on real-world data, provide evidence of EV71 vaccine effectiveness for preventing EV71 and “other” viruses associated with HFMD. An expanded program of EV71 vaccination is urgently needed.
Introduction
Hand, foot, and mouth disease (HFMD) is a common viral infection that usually affects children, but can also occur in adolescents and adults.Citation1 HFMD is caused by enterovirus infection, including EV71, CVA16, CVA6, CVA9 and others, and usually begins with a low-grade fever, and progresses to red spots or blisters that appear a few days later on the hands, the bottoms of the feet, and the mouth and throat.Citation2 HFMD is an important public health issue in China. Since a 2008 outbreak, HFMD has been the most common of all notifiable diseases in China.Citation3 The increase in HFMD health effect index, a measure of hazard combining morbidity and mortality, was the most significant among all infectious diseases in China from 2004 to 2013.Citation4 There is no effective treatment available for HFMD at present.Citation5
A monovalent vaccine against EV71, the most common cause of severe and fatal HFMD cases,Citation6 has been available in China since 2016 and remains the only available vaccine.Citation7 Since there is no effective treatment for HFMD, prevention is especially important. EV71 vaccination is not currently included in the Chinese government’s Expanded Program on Immunization. This vaccine is given in two doses, administered 4 weeks apart, to children aged 6 to 59 months. However, some children received only a signle dose for unknown reasons. Despite the introduction of the EV71 vaccine, the number of HFMD cases remained substantial in China in 2017 and 2018.Citation3 Furthermore, the EV71 vaccine may offer cross-protectivity to other HFMD-associated enteroviruses, although findings have been inconsistent. For example, investigators reported cross antiviral activity between EV71 immunoglobulin and CVA16 in vitro.Citation8 However, others did not.Citation9–11 Another laboratory study reported a weak cross-neutralization effect of EV71 vaccine on CVA6, CVA9, and other enteroviruses.Citation12 To help to address this data gap, evidence from population-based studies is needed.
The monovalent EV71 vaccine is the only HFMD vaccine available in China at present. Although randomized controlled trails (RCTs) established the efficacy of the vaccine among research subjects,Citation13 this may not reflect the impact under “real world” conditions in the general population. In RCTs, EV71 vaccine efficacy was estimated using groups with 100% vaccination, which does not reflect vaccination coverage in the greneral Chinese population. It is thus important to evaluate the effectiveness of the EV71 vaccine against HFMD among the general population.
Cost-effectiveness analysis is essential for new vaccines, including the EV71 vaccine. Vaccine effectiveness, which differs from vaccine efficacy, is one of the most important parameters sought by researchers conducting comprehensive literature reviews. Vaccine efficacy does not account for the impact of herd immunity and so using vaccine efficacy under the assumption of high vaccine coverageCitation14 will underestimate its cost-effectiveness.
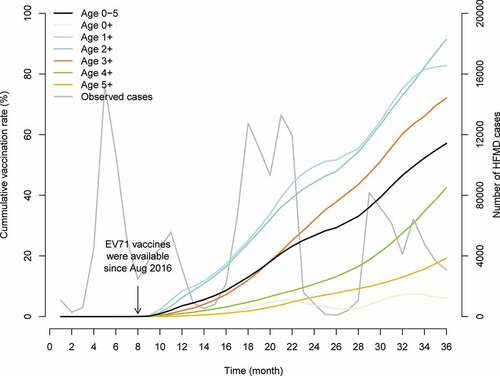
The current EV71 vaccination rate in Guangzhou is relatively low, about 60% for two-dose among children under 5 years old (). Evidence on EV71 vaccine effectiveness is urgently needed to promote public knowledge to increase the vaccination rate. We therefore assessed EV71 vaccine effectiveness for preventing HFMD in the general population of Guangzhou, China, following its August 2016 introduction. We hypothesized that EV71 vaccine, especially the two-dose, would decrease HFMD incidence.
Figure 1. Vaccination rates and HFMD cases in Guangzhou, China, 2016–2018
Materials and methods
Ethical approval
Data were collected from the official HFMD surveillance system in China. No confidential information was involved. The research study protocol was approved by the Institutional Review Board at Sun Yat-sen University School of Public Health.
Data collection
Study site
Guangzhou, located in 22°26ʹ to 23°56ʹ N and 112°57ʹ to 114°3ʹ E in southern China, is a low-latitude, high temperature and high humidity area with a population of approximately 15 million. Guangzhou is divided into 11 districts (i.e., Yuexiu, Haizhu, Liwan, Tianhe, Baiyun, Huangpu, Huadu, Panyu, Nansha, Conghua, and Zengcheng).
Case definition
A probable case of HFMD was defined as a patient with papular or vesicular rash on hands, feet, mouth, or buttocks, with or without fever. A confirmed case was defined as a probable case with laboratory evidence of enterovirus infection (including EV71, CVA16, or other enterovirus). Patients with HFMD, whether probable or confirmed, were classified as severe cases if there was a severe complication; otherwise, patients were categorized as mild cases.
HFMD data
China established a national enhanced surveillance system for notifiable diseases in 2004. As a notifiable disease, all probable and confirmed HFMD cases are reported online to the surveillance system within 24 hours of diagnosis using a standardized form. We used routinely collected surveillance data reported to the China Information System for Disease Control and Prevention managed by the Guangzhou, China Center for Disease Control (CDC), from January 2016 to December 2018. The CDC collects data for all HFMD diagnoses by law, including name, gender, birth date, residential address, and virus types. The virus types of the earliest 5 cases (at least) per month from each sentinel site (i.e., comprehensive medical institutions at or above the county level) are determined using fluorescence quantitative PCR. All HFMD cases under 5 years of age in Guangzhou were included in the current analysis.
Vaccination data
We also obtained vaccination data using the China Information System for Disease Control and Prevention. The CDC collects name, gender, birth date, residential address, vaccine name and manufacturer, vaccination date, vaccination location/institution, and cumulative vaccine dose for all inoculations administered in Guangzhou under a legal mandate. HFMD cases data and vaccination data were linked by the calendar date.
Demographic data
We also captured annual total population data for Guangzhou, each year from 2016 to 2018, using the China Information System for Disease Control and Prevention. We used the Guangzhou Province Statistical Yearbook to capture the annual number of live births each year from 2016 to 2018 in Guangzhou.Citation15 The vaccination rates were computed by dividing the monthly number of vaccinations by the population under 5 years of age in each year.
Climate data
We adjusted for meteorological data, including air temperature (°C) and relative humidity (%), in our time-series models. These data were collected from the China Meteorological Data Service Center (CMDC, http://data.cma.cn/en). Daily data from two national monitoring stations in Guangzhou were aggregated into monthly average data for use in the statistical models.
Statistical analysis
We first characterized the distribution of HFMD cases and vaccinations according to year, age, sex, and HFMD virus. Next, in spatial ecologic analysis, we divided all 11 city districts into high and low vaccination rates according to the median EV71 vaccination rates for one-dose (17.63%) and two-dose (69.00%), from 2016 to 2018. We computed case proportions as case number after vaccination (year 2017–2018) divided by the total case number (year 2016–2018), defined as “proportion 1” for high vaccination rate districts and “proportion 2” for low vaccination rate counties. The HFMD rate ratios for high vaccination rate districts relative to low vaccination rate counties were calculated as proportion 1 divided by proportion 2. Ratios smaller than 1, indicated a lower disease burden in high vaccination rate districts.
We then used a time-series approach to model the distribution of HFMD cases as a function of vaccination rates,Citation16 such that:
where t = 1, …, 36 reflects time (in months) and ε is the residual error. We used the log of the monthly number of HFMD cases (y) as the response variable, calculated the monthly vaccination rate (x, %) as the number of vaccinations divided by the population of the respective age group, and used the offset(log(births)) as the exposure period (e.g., denominator). In addition, the temperature and relative humidity were controlled as confounding factors were adjusted in our model. Because a log-transformation is used, the effect of x should be interpreted in multiplicative fashion (i.e. exp(β1)). Furthermore, we controlled for seasonal trends using f(t), the Fourier componentsCitation17 (combining sine and cosine terms), with periods of 6 months and 12 months (e.g. f(1) = f(7) and f(1) = f(13)). We performed a sensitivity analysis to determine the final model, fitting the two-dose vaccination with different regression components, such as semiannual and annual periodicities and climate factors (see supplementary Table S1 and Figure S1). For models of different virus types, we also included the total number of detected cases as the offset. We defined vaccine effectiveness as:
where v is the vaccination rate used to calculate the vaccine effectiveness, and v = 100% was selected in our study.
We conducted subgroup analyses by age, sex, and virus type. No data were missing data. We defined statistical significance as P < .05 for a two-tailed test and all statistical analyses were performed using R version 3.6.2 (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Basic data
presents the number of HFMD cases and EV71 vaccinations in Guangzhou, China from 2016 to 2018. A total of 174,002 HFMD cases under 5 years of age were reported to the Guangzhou CDC surveillance system from January 2016 to December 2018. A statistically significant decrease (from 32.69% or 41.27% to 26.04%) in the proportion of HFMD cases was observed in 2018. Most HFMD cases were diagnosed in children at one year of age (31.85%) and among males (60.44%). A total of 408,664 (79.12%) children completed a two-dose of EV71 vaccine. An increasing number of children completed EV71 vaccinations from 2016 to 2018, for both one-dose and two-dose. Consistent with the pattern for HFMD cases, the majority of vaccinated children were one year of age (one-dose: 37.65% and two-dose: 46.88%) and male (53.34% and 53.00%). There were 1,294,500, 1,516,300, and 1,439,800 live births in Guangzhou in 2016, 2017, and 2018, respectively.
Table 1. Number (%) of HFMD cases and EV71 vaccinations in Guangzhou, China, 2016–2018
shows the trend of cumulative vaccination rates and observed cases as a function of time (months). The number of HFMD cases decreased across the study period. The cumulative two-dose vaccination rates increased for all age groups, from August 2016 (when the EV71 vaccine became available) to December 2018. The cumulative two-dose vaccination rate was approximately 60% at the end of 2018.
Spatial ecologic analysis
presents ratios for high and low HFMD vaccination rate districts in Guangzhou, China from 2016–2018. Compared with the low vaccination rate districts, high vaccination rate districts had a lower proportion of HFMD (one-dose: 66.31% vs. 68.41%, two-dose: 65.51% vs. 68.57%). The ratios were statistically significant with a precise 95% confidence intervals (CI) (e.g., the ratio of two-dose: 0.955, 95%CI: 0.949–0.962, P < .001).
Table 2. Ratios of HFMD cases for high to low EV71 vaccination rate districts in Guangzhou, China, 2016–2018
Time-series analysis
presents the results of the time-series regression models fitting HFMD cases as a function of EV71 two-dose vaccination rate. All regression coefficients were negative, except for CVA16, for the total study population and population subgroups, meaning that a greater vaccination rate was associated with fewer HFMD cases. For example, the regression coefficient for two-dose was −0.009 in total population, indicating each 1% increase in vaccination rate was associated with a 0.9% (i.e., 1-e−0.009) decrease in HFMD cases. Statistical associations between HFMD cases and two-dose vaccination rates were found in subgroups from children at 3 years of age (0.9% decreases in HFMD cases per each 1% increase in vaccination rate), EV71 infection speciffically (1.4%) and infection with “other” viruses (1.3%). Similar effects were found in the total population and 3 years old, EV71 infection and other virus infection subgroups for one-dose (Table S2). Under the assumption of 100% two-dose vaccination rate coverage, the vaccination effectiveness will be 59.93% for children at 3 years of age, 75.17% for EV71 infection and 73.76% for other HFMD virus infection according to our models (). Greater effectiveness, although less precise in regression coefficients, were found for the one-dose vaccination (Table S2).
Table 3. Associations between two-dose EV71 vaccination rate and HFMD cases in Guangzhou, China, 2016–2018
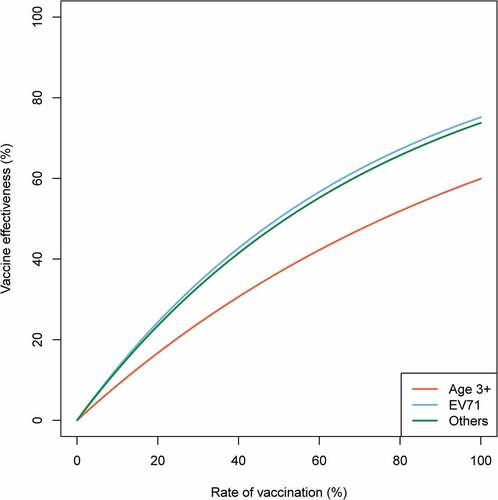
shows the relationship between two-dose vaccination rate and effectiveness in statistically significant subgroups. With a greater two-dose vaccination rate, vaccine effectiveness will increase sharply at first and slow down later. When the two-dose vaccination rate reaches 100%, vaccine effectiveness will achieve about 60% in children at 3 years of age. Different subgroups have different vaccine effectiveness trajectories as a function of vaccination rate. As expected, the EV71 HFMD infection achieves greater vaccine effectiveness at smaller vaccination rates than the other subgroups.
Figure 2. Vaccine effectiveness as a function of two-dose vaccination rate in statistically significant subgroups
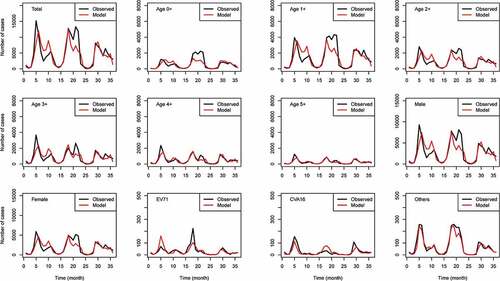
shows the observed values compared to fitted values from the time-series regression models of HFMD cases as a function of the two-dose vaccination rate, in the total population and according to subgroups. All 12 models had the similar numbers of observed and fitted cases, underscoring the validity of our model fitting strategy. With the exception of a 2017 EV71 HFMD case peak (~18 months), the observed and fitted case number decreased over time. The adjusted R-squared values in suggest that our model explained about 80% of HFMD case variability in the total population and in subgroups, with the examples of children at 3 years of age (79%), EV71 (79%), and “other” viruses (93%).
Figure 3. Observed and fitted HFMD cases in Guangzhou, China, 2016–2018
Discussion
In this EV71 HFMD effectiveness study, we showed that the HFMD risk decreased in the total population, although it was not statistically associated with greater one-dose or two-dose EV71 vaccination rate. However, we found that the association between HFMD and vaccination rate varied for different population subgroups, with the greatest effectiveness achieved among children at 3 years of age and for preventing infection with EV71. To our knowledge, this is the first study to demonstrate the effectiveness of the HMFD EV71 vaccination in the general population of Guangzhou, China, underscoring the population targeting of vaccine effectiveness.
The China CDC recommends two doses of EV71 vaccine before 5 years of age (i.e., during 6 months to 5 years).Citation18 Li et al. estimated that the overall vaccine effectiveness as 85.4% (95% CI: 53.2 to 95.4) for fully vaccinated (i.e., two-dose) children and 63.1% (95%CI: 13.1 to 84.3) for partly vaccinated (i.e., one-dose) children.Citation19 Wang et al. reported 1-dose and 2-dose adjusted vaccine effectiveness estimates as 69.8% and 83.7% for mild cases were, respectively.Citation20 In contrast, the results of our study suggested 75.17% effectiveness against EV71-associated HFMD with a 100% two-dose vaccination rate. The pooled effect from both one-dose and two-dose vaccinations may account in part for the modest underestimate in our study.
In this study, we also found greater two-dose vaccine effectiveness for children at 3 years of age than among children of other ages. This might be due to a higher geometric mean titer and seroconversion rate for children at 3 years of age than at other ages.Citation20 Most Chinese children attend kindergarten at 3 years of age,Citation21 which is a common site of HFMD outbreaks, given close daily contact among members of a susceptible population. The largest proportion of HFMD cases were among children at 1 year, for whom we found comparatively poor vaccine effectiveness, possibly due to very low vaccination rates in the total population and a lower immune response level. A previous study using hospital data also reported lower partial vaccination (i.e., one-dose) effectiveness for children aged 6–23 months (40.8%, 95%CI: −71.1 to 79.5) than for children aged 24–71 months (77.9%, 95%CI: 4 · 3 to 94 · 9).Citation19
Neither males nor females had a statistical benefit from EV71 vaccination in the current study, although we found modestly greater vaccine effectiveness among males than among females. In a previous studies, we reported that males had a higher risk than females for severe HFMD,Citation22 although, EV71 infection caused more cases than other viruses in both sexes. Thus, vaccination coverage should be increased in both sexes.
Greater vaccination rates were associated with lower numbers of HFMD cases caused by EV71 and “other” viruses, but not CVA16. That was, EV71 vaccine didn’t appear to have cross-protection for CVA16 in this study, but it did for “other” viruses. Yang et al. reported that EV71 vaccination cannot effectively control HFMD overall because the vaccine cannot cross-protect against CVA16 infection.Citation11 Therefore, a separate vaccine for CVA16 or a EV71/CVA16 bivalent vaccine is urgently needed. For “other” viruses, Liang et al. reported that EV71 vaccination provided cross-protection against CVA6, CVA9, CB4, ECHO6, ECHO11, ECHO14, ECHO30 and ECHO33.Citation12 However, a phase 3 randomized controlled trial, Zhu et al. found that the EV71 vaccine offered no protection against HFMD caused by CVA16 or other enterovirus serotypes.Citation23 The indirect vaccine effectiveness of EV71 vaccination may explain in part these inconsistent findings. Thus, virus serotypes besides EV71 and CVA16 should be considered in HFMD settings with decreasing EV71.
While our study offers several strengths, including the longitudinal nature of the study design and the large sample size, there were also several important limitations. First, we could not isolate the one-dose and two-dose associations from each other. This might have overestimated the effects of both doses, especially for the effect of one-dose. Second, cases were randomly sampled for laboratory confirmation/viral serotyping. However, this sampling information was condidered to be representative of all HFMD cases. Third, we could not rule out surveillance bias from potential overdiagnosis or underdiagnosis, because it was difficult to distinguish HFMD with varicella infection. However, the technical capacity of the physicians in one city was stable and the trends of HFMD incidence used in our study should be consistent with the truth. Finally, we could not distinguish vaccine effectiveness between the mild and severe cases due to the limited number of severe cases (only 6 cases) during our study period. Our findings could be applied to the settings with similar socio-economic conditions and population contact patterns where both the direct and indirect effects of vaccination might be similar and could be captured.
Conclusion
Our findings on population-level vaccine effectiveness suggest that the 2016 introduction of two-dose EV71 vaccination was an effective intervention to prevent HFMD in Guangzhou, China, especially among children 3 years of age. The results of this study also suggest the urgent need for bivalent EV71/CVA16 vaccine and for continued expansion of EV71 vaccine coverage in Guangzhou, China.
Authors’ contributions
ZD and YH participated in the design, performed data analysis and interpretation, and drafted the manuscript. MB, ZZ, ZY, and JL participated in the design and results interpretation, and helped to finalize the manuscript. JX and YH participated in the design and supervised the study, participated in interpretation of results, and helped to finalize the manuscript. All authors have read and approved the contents of the final version.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Supplemental Material
Download MS Word (36 KB)Acknowledgments
We thank the Guangzhou Center for Disease Control and Prevention for providing the data of notified hand, foot, and mouth disease cases and EV71 vaccinations.
Data availability
The cases data and vaccination data are available from Guangzhou, China CDC (http://www.gzcdc.org.cn/), which were used under license and not publicly available.
Supplementary material
Supplemental data for this article can be accessed online at http://dx.doi.org/10.1080/21645515.2020.1763076.
Additional information
Funding
References
- WHO Western Pacific. Hand, foot, and mouth disease. WHO; 2019 April 23 [accessed 2020Mar 25]. https://www.who.int/westernpacific/emergencies/surveillance/archives/hand-foot-and-mouth-disease.
- Cox B, Hand LF. Foot, and mouth diseasehand, foot, and mouth diseasehand, foot, and mouth disease. JAMA. 2018;320(23):2492. doi:10.1001/jama.2018.17288.
- Department of Disease Prevention and Control. Epidemic situation of notifiable infectious diseases in China (in Chinese). National Health Commission of the People’s Republic China; 2019 April 24 [accessed 2020 Mar 25]. http://www.nhc.gov.cn/wjw/rdts/list.shtml.
- Zhang R, Dai T, Jia X, Li Y. Comprehensive evaluation of health effect of notifiable infectious diseases in China (in Chinese). China Med Her. 2015;12(12):50–53.
- Health CFP. Hand, foot and mouth disease. Hong Kong, China: Department of Health; 2019 June 27 [accessed 2020 Mar 25]. https://www.chp.gov.hk/en/healthtopics/content/24/23.html.
- Shimizu H, Nakashima K. Surveillance of hand, foot, and mouth disease for a vaccine. Lancet Infect Dis. 2014;14(4):262–63. doi:10.1016/S1473-3099(13)70330-X.
- Mao QY, Wang Y, Bian L, Xu M, Liang Z. EV71 vaccine, a new tool to control outbreaks of hand, foot and mouth disease (HFMD). Expert Rev Vaccines. 2016:1–8. doi:10.1586/14760584.2016.1138862.
- Gao E, Wu S, Xu Q, Zeng Y, Tan N, He S, Yang Y, Wei J. Enterovirus type 71‑immunized chicken egg yolk immunoglobulin has cross antiviral activity against coxsackievirus A16 in vitro. Exp Ther Med. 2019;18:332–41. doi:10.3892/etm.2019.7529.
- Yang T, Li H, Yue L, Song X, Xie T, Ma S, Meng H, Zhang Y, He X, Long R, et al. A comparative study of multiple clinical enterovirus 71 isolates and evaluation of cross protection of inactivated vaccine strain FY-23 K-B in vitro. Virol J. 2017;14(1):206. doi:10.1186/s12985-017-0872-8.
- Huang J, Liao Q, Ooi MH, Cowling BJ, Chang Z, Wu P, Liu F, Li Y, Luo L, Yu S, et al. Epidemiology of recurrent hand, foot and mouth disease, China, 2008-2015. Emerg Infect Dis. 2018;24(3):432–42. doi:10.3201/eid2403.171303.
- Yang L, Liu Y, Li S, Zhao H, Lin Q, Yu H, Huang X, Zheng Q, Cheng T, Xia N. A novel inactivated enterovirus 71 vaccine can elicit cross-protective immunity against coxsackievirus A16 in mice. Vaccine. 2016;34(48):5938–45. doi:10.1016/j.vaccine.2016.10.018.
- Liang S Cross-protection of Enterovirus 71 vaccine and construction of its gene recombinant mycobacterium smegmatis (in Chinese) [dissertation]. Guilin (China): Guilin Medical University; 2018.
- Zhu F, Meng F, Li J, Li X, Mao Q, Tao H, Zhang Y, Yao X, Chu K, Chen Q, et al. Efficacy, safety, and immunology of an inactivated alum-adjuvant enterovirus 71 vaccine in children in China: a multicentre,randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2013;381(9882):2024–32. doi:10.1016/S0140-6736(13)61049-1.
- Wang W, Song J, Wang J, Li Y, Deng H, Li M, Gao N, Zhai S, Dang S, Zhang X, et al. Cost-effectiveness of a national enterovirus 71 vaccination program in China. Plos Neglect Trop D. 2017;11(9):e5899. doi:10.1371/journal.pntd.0005899.
- Comprehensive statistical office. Statistical yearbook of Guangdong. Statistics Bureau of Guangdong; 2019 Sep 29 [accessed 2020 Mar 25]: http://stats.gd.gov.cn/gdtjnj/index.html.
- Hohle M, Siedler A, Bader HM, Ludwig M, Heininger U, Von Kries R. Assessment of varicella vaccine effectiveness in Germany: a time-series approach. Epidemiol Infect. 2011;139(11):1710–19. doi:10.1017/S0950268810002815.
- Kiyono K. Establishing a direct connection between detrended fluctuation analysis and Fourier analysis. Phys Rev E Stat Nonlin Soft Matter Phys. 2015;92(4):42925. doi:10.1103/PhysRevE.92.042925.
- Experts from China CDC. Core information of prevention and control of hand, foot and mouth disease (in Chinese). China CDC; 2018 Mar 26 [accessed 2020 Mar 25]. http://www.chinacdc.cn/jkzt/crb/bl/szkb/zstd/201803/t20180326_159976.html.
- Li Y, Zhou Y, Cheng Y, Wu P, Zhou C, Cui P, Song C, Liang L, Wang F, Qiu Q, et al. Effectiveness of EV-A71 vaccination in prevention of paediatric hand, foot, and mouth disease associated with EV-A71 virus infection requiring hospitalisation in Henan, China, 2017-18: a test-negative case-control study. Lancet Child Adolesc Health. 2019;3(10):697–704. doi:10.1016/S2352-4642(19)30185-3.
- Wang X, An Z, Huo D, Jia L, Li J, Yang Y, Liang Z, Wang Q, Wang H. Enterovirus A71 vaccine effectiveness in preventing enterovirus A71 infection among medically-attended hand, foot, and mouth disease cases, Beijing, China. Hum Vacc Immunother. 2019;15(5):1183–90. doi:10.1080/21645515.2019.1581539.
- InterNations GO. The Chinese education system. InterNations GO; 2020 Jan 30 [accessed 2020 Mar 25]. https://www.internations.org/go/moving-to-china/education.
- Du Z, Zhang W, Zhang D, Yu S, Hao Y. Epidemiological characteristics of severe cases of hand, foot, and mouth disease in Guangdong, China. Biostatistics Epidemiol. 2018;2(1):99–114. doi:10.1080/24709360.2018.1469809.
- Zhu F, Xu W, Xia J, Liang Z, Liu Y, Zhang X, Tan X, Wang L, Mao Q, Wu J, et al. Efficacy, safety, and immunogenicity of an enterovirus 71 vaccine in China. New Engl J Med. 2014;370(9):818–28. doi:10.1056/NEJMoa1304923.