
ABSTRACT
The world is experiencing a pandemic of Coronavirus Disease (COVID-19) caused by type-2 Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2). Vaccination is the only option to prevent future surges of the disease. Efforts for developing an effective vaccine are underway, but the timeline for the widespread availability of safe and effective vaccines is unknown. Some ecological reports have linked regional universal use of the Bacillus Calmette-Guerin (BCG) vaccine with reduced morbidity and mortality of COVID-19. BCG protects from non-tuberculous diseases through ‘non-specific’ effects mediated by the modulation of innate immunity. This commentary provides details of the immunological mechanism of BCG-induced ‘trained innate immunity’ responsible for its nonspecific protective effects. A probable role of the BCG vaccine in the current pandemic is also examined.
The Coronavirus disease (COVID-19) pandemic, caused by type 2 Severe Acute Respiratory Syndrome Coronavirus (SARS-CoV-2) virus, has caused disease in virtually every country in the world in millions of subjects of which hundreds of thousands have died.Citation1 There is no effective treatment available to date. Even though there are more than 100 candidate vaccines shortlisted currently, there is no specific vaccine available against the SARS-CoV-2 virus.Citation2,Citation3 Seven of these vaccines have reached the human clinical trial stage.Citation4 However, the timing for the widespread availability of safe and effective vaccines remains unknown. Of the seven, three are being tested by the Chinese companies. They include an inactivated alum-adjuvanted vaccine, PiCoVacc by Sinovac, a non-replicating viral vector, adenovirus Type 5 vector (Ad5-nCoV) vaccine by CanSino Biological in collaboration with the Beijing Institute of Biotechnology, and another inactivated Vero-cell-derived vaccine by the Wuhan Institute of Biological Products. The AstraZeneca with the University of Oxford in the UK is also testing another non-replicating viral vector (adenovirus), ChAdOx1 nCoV-19 vaccine. The US companies are testing two nucleic acid-based vaccines. Moderna Inc. has completed a phase I trial of its mRNA-1273 vaccine with the National Institute of Allergy and Infectious Diseases while Inovio Pharmaceuticals, Pennsylvania has also begun testing its DNA platform vaccine. The seventh vaccine, termed as BNT162 and includes four vaccine candidates, each represent different mRNA formats and target antigens, is being developed by the German biotech company BioNTech and Pfizer.Citation4
Much of interest is being generated after the publication of few ‘non-peer reviewed’ preprints on the probable protective role of the Bacillus Calmette-Guerin (BCG) vaccine on COVID-19 incidence and severity. Few countries like Netherland, Australia, UK, and Germany have started BCG trials among healthcare workers to assess its protective effects if any.Citation5,Citation6 Some experts are also exploring the utility of other live-attenuated vaccines like oral polio vaccine (OPV) and measles against the disease.Citation7,Citation8 Furthermore, three premier institutes in India are soon going to start prospective randomized trials of an old killed leprosy vaccine, Mycobacterium w (Mw) referred to as Mycobacterium indicus pranii, to study the nonspecific immunomodulatory effects of the vaccine in hospitalized Covid-19 patients.Citation9
The universal use of BCG vaccine and impact on COVID-19
The preliminary report exhibiting protective effects of childhood BCG vaccine on the incidence of COVID-19 in the countries which are routinely using this vaccine in their national immunization programs is only ecological reports that suggest mere association and not a ‘cause-effect’ relationship. However, correlation does not imply causation. There are issues with their study design (population-level observation is equated with exposures at the individual level), study timing (a pandemic is still evolving in many countries using universal BCG), testing potential (many BCG-using low-middle income countries (LMICs) have conducted comparatively fewer tests than high-income non-BCG using countries, hence underestimation of cases/deaths in latter), and missed/misclassification of deaths in LMICs using universal BCG vaccination. Apart from these, there are some other ‘confounders’ like demographic characteristics (BCG vaccine using South East Asia and African population are comparatively young than Europeans, where the disease is far more prevalent in older population), and prevalence of comorbidities, and the peculiar tropical environment in most LMICs employing universal BCG vaccination. Moreover, the hot and humid climatic conditions resist intense transmission of respiratory viruses and may suppress the severity of the current pandemic.Citation10 Another argument against this hypothesis is the waning of BCG-induced immunity. According to many studies, the BCG induced protection against TB wanes following infant immunization, and some studies have shown that it almost completely disappears by 10–15 years of age.Citation11 There is still inadequate evidence to prove that the BCG induced non-tuberculous protective immunity persists for an exceedingly long time, i.e. till adulthood.Citation12
BCG vaccine-induced heterologous, nonspecific effects
BCG vaccine mainly works through induction of cell-mediated immunity whereas almost all other childhood vaccines offer protection primarily through induction of humoral immunity, i.e. production of antibodies. BCG is only moderately efficacious against pulmonary TB,Citation11 but it is known to provide ‘non-specific’ (heterologous) protection against certain respiratory infections and sepsis caused by viruses (e.g. vaccinia virus, herpes, and influenza), bacteria (e.g. Shigella flexneri), and protozoa (e.g. malaria).Citation11–21 In Guinea-Bissau, vaccination with BCG reduced neonatal mortality in low birth weight babies by 48%.Citation13,Citation14 In Spain, the BCG vaccine reduced non-TB hospital admissions in infants by 32% for respiratory infections and by 53% for sepsis.Citation16 Additionally, it has been shown that BCG vaccination was responsible for the reduction of all-cause mortality by approximately 50% among under-5-year old children.Citation18
Most of the studies on nonspecific effects of BCG were done by Abay P et al. mainly in Guinea-Bissau.Citation13–15 Some of these studies were observational, non-randomized with questionable methodology, hence, with low-level evidence. The WHO had also reviewed these trials and concluded that BCG appeared to lower overall mortality in children but graded the evidence as ‘low’. It suggested the need for more randomized trials to demonstrate these effects.Citation11 It was only after a few recent studies mainly by Netea MG et al.Citation20,Citation21 that provided evidence on the nonspecific effects of the BCG through human studies with the explanatory mechanism. In 2018, Netea MG et al. conducted a randomized placebo-controlled human challenge study in which it was shown that the BCG induced genome-wide epigenetic reprogramming of monocytes and offered protection against experimental infection with an attenuated yellow fever virus vaccine strain.Citation20,Citation21 Additionally, it has been shown that BCG administration enhances immune responses of other vaccines like hepatitis-B, poliovirus type-1, IPV, PCVs, with significantly higher production of antibodies.Citation22
Protective effects of BCG in adults
BCG is found useful in many non-TB conditions of adults also. This vaccine has been licensed for the treatment of superficial bladder cancer, for which it also exerts nonspecific effects.Citation23 Thus far, it has not been surpassed by any other drug in terms of its ability to reduce disease recurrence and progression. BCG provides anti-tumor effects by a complex immune cascade that induces antitumor activity (via cytokine release) mediated by cytotoxic T lymphocytes, natural killer cells, neutrophils, and macrophages.Citation23 BCG has also been shown to be useful in some autoimmune disorders such as Insulin-dependent diabetes mellitus (IDDM) and multiple sclerosis.Citation11 In a study from Harvard Medical School, adults with longstanding Type-I diabetes showed a remarkable recovery of serum HbA1c levels to near normal with no episodes of severe hypoglycemia at the end of three years which remained stable for the next five years.Citation24 It has been previously documented that regulatory T cells (Tregs) play a key role in preventing various autoimmune disorders. The BCG vaccine probably works by upregulating these Tregs.Citation24 Some observational studies suggest BCG-vaccination is associated with some protection against allergies, eczema, and asthma, although these findings have been inconsistent.Citation11 Additionally, BCG has also been shown to be associated with protection against melanoma and may play a role in its treatment.Citation11 Recently, a retrospective review has shown a lower risk of development of lung cancer among those who had received BCG vaccination during childhood.Citation25
The mechanism behind the generation of BCG-induced nonspecific effects
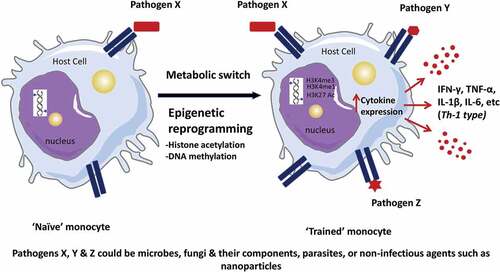
Unlike the ‘adaptive’ immunity, the ‘innate’ immune system is supposed to have no memory responses. But BCG, which can remain alive in the human skin for up to several months, triggers not only Mycobacterium-specific memory B and T cells but also stimulates the cells of the innate system (monocytes, neutrophils, macrophages, natural killer, dendritic cells, etc.) for a prolonged period. The process by which BCG imparts immune memory to the innate system is known as ‘trained innate immunity’ which in turn is elicited by a phenomenon known as ‘epigenetic effect’.Citation26,Citation27 The ‘epigenetic effect’ is produced by the modification of gene expression rather than alteration of the genetic code or nucleotide sequencing. This effect is brought about by two main mechanisms, DNA methylation and histone modifications, that alter innate immunity.Citation27,Citation28 BCG does epigenetic reprogramming in the training of innate cells, particularly monocytes. Upon pathogen X recognition by a receptor, ‘naïve’ monocytes undergo epigenetic reprogramming and a metabolic shift and convert into ‘trained’ monocytes, primed to respond more vigorously to nonspecific (Pathogens X, Y, and Z) secondary stimulation. Unlike antigen-specific memory of the adaptive immune system, the second stimulation does not have to be with the same pathogen or antigen.Citation27 Later on, these ‘trained’ monocytes have a significantly higher production of several proinflammatory cytokines like interferon-gamma (IFN-γ), TNF-alfa, interleukins (IL-1β, IL-6, etc.) upon heterologous challenges, particularly T helper cell type 1 polarizing and typically monocyte-derived proinflammatory cytokines that helps in rapid clearance of infection ().Citation12,Citation26,Citation27 These modified, activated, ‘trained’ cells can be stimulated by various non-related infectious (viruses, bacteria, fungi and their components, parasites) or noninfectious agents such as nanoparticles which leads to potent immune memory responses.Citation28 This response explains the BCG nonspecific protection against sepsis, pneumonia, and other pathogens. Both epigenetic changes and increased nonspecific immune responses could be detected up to one year after BCG vaccination.Citation12
Figure 1. ‘Trained Innate Immunity’–Epigenetic reprogramming of monocytes. Upon pathogen X recognition by a receptor, naive monocytes undergo epigenetic reprogramming and a metabolic shift and become primed to respond more robustly to nonspecific (Pathogens X, Y and Z) secondary stimulation (Adapted with permission from reference number 27).
Effect of BCG strains and scar rates on its nonspecific effects
The BCG vaccine strains that are employed in the immunization programs of different countries vary widely. Over the years, more than 14 sub-strains of BCG have been used as BCG vaccine in different parts of the world.Citation11 Not all strains of BCG have similar potential to induce ‘trained immunity’ in vaccinated individuals; as a result, they have different propensities to induce ‘non-specific’ effects.Citation29 Most of the studies on beneficial effects of BCG against sepsis and pneumonia were done with Danish strain.Citation13–15 Whether other strains do have similar ‘non-specific’ responses is not yet ascertained. The ‘nonspecific effects’ of BCG are greater when there is a scar. Different strains of BCG have different scar rates. Scar formation rate is higher around >90% with BCG-Danish and BCG-Tokyo strains whereas it is only 52% with BCG–Moscow.Citation30 Among BCG-vaccinated children in a setting with low scar prevalence, having a scar is associated with lower mortality and morbidity. Revaccination with BCG confers little or no extra protection against TB, but it may increase the beneficial nonspecific effects of BCG.Citation30
Can BCG offer any protection against ongoing COVID-19 pandemic?
Even after almost 100 years of its invention, it is still a mystery, how exactly the BCG vaccine works.Citation31 It would be ironic if we were to discover that BCG protects against TB via a ‘nonspecific’ effect mediated by innate immunity. Nevertheless, at least we know that BCG elicits heterologous, ‘non-specific’ effects against a variety of infectious diseases, and SARS-CoV-2 shall not be an exception. Its beneficial effects are also well documented in adults albeit with some potential for toxicity.Citation23,Citation24 Notwithstanding the recent statement of WHO that there is no evidence of BCG-induced protection against SARS-CoV-2 infection,Citation32 still, the BCG may have some utility owing to the induction of strong, ‘non-specific’, innate immune responses in the vaccinated subjects. BCG may not be able to exert significant inhibitory responses against the SARS-CoV-2 virus, but even ‘stopgap’ protection and some attenuation of the disease may be expected. An extra dose of BCG to the healthcare workers and older people with comorbid conditions would be worth investigating. BCG is generally safe and well tolerated; however, it is contraindicated in immunocompromised individuals, so one needs to be extra careful while administering BCG to these individuals. Apart from safety, there are other issues like the selection of proper strain of the vaccine, and quantum of the immune responses elicited in older and high-risk individuals in comparison to the young and healthy population that need deliberation before employing the vaccine in these groups. One argument against the protective effects of childhood BCG vaccination on COVID-19 susceptibility is the waning of BCG-induced immunity. However, if the heterologous, ‘non-specific’ effects persist even for a few months, they should be able to offer some protection through modulation of innate immunity to the front-line health workers and high-risk individuals till a specific anti-SARS-CoV-2 vaccine becomes available.
Conflicts of interest
None
Disclosure of potential conflicts of interest
I hereby declare that there exist no commercial or financial relationships that could, in any way, lead to a potential conflict of interest.
Acknowledgments
The author would like to acknowledge Dr Stanley A. Plotkin for his intellectual inputs in developing the manuscript.
Additional information
Funding
References
- World Health Organization. Coronavirus disease (COVID-19) pandemic; 2020 [accessed 2020 May 28]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
- Thanh Le T, Andreadakis Z, Kumar A, Román RG, Tollefsen S, Saville M, Mayhew S. The COVID-19 vaccine development landscape. Nat Rev Drug Discov. 2020;19:305‐06.
- Ella KM, Mohan VK. Coronavirus vaccines: light at the end of the tunnel. Indian Pediatr. 2020;57(5):407‐10. doi:10.1007/s13312-020-1812-z.
- Mahase E. Covid-19: what do we know so far about a vaccine? BMJ. 2020;369:m1679. doi:10.1136/bmj.m1679.
- Reducing health care workers absenteeism in Covid-19 pandemic through BCG vaccine (BCG-CORONA); 2020 [accessed 2020 Apr 14]. https://clinicaltrials.gov/ct2/show/NCT04328441.
- BCG vaccination to protect healthcare workers against COVID-19 (BRACE); 2020 [accessed 2020 Apr 14]. https://clinicaltrials.gov/ct2/show/NCT04327206.
- Austell J. Can an oral polio vaccine help stop COVID-19? [blog]. Global Virus Network (GVN); 2020 [accessed 2020 Apr 14]. https://gvn.org/dr-robert-gallo-exclusive-broadcast-interview-with-walter-isaacson-of-amanpour-co/.
- Shanker V. Measles immunization: worth considering containment strategy for SARS-CoV-2 global outbreak. Indian Pediatr. 2020;57(4):380. doi:10.1007/s13312-020-1804-z.
- PGI to test leprosy vaccine on Covid-19 patients.2020. Hindustan Times. 2020 Apr 22 [accessed 2020 Apr 27]. https://www.hindustantimes.com/chandigarh/pgi-to-test-leprosy-vaccine-on-covid-19-patients/story-0DHH4GS8mANbUZNRZj2kYK.html.
- Wu Y, Jing W, Liu J, Ma Q, Yuan J, Wang Y, Du M, Min Liu M. Effects of temperature and humidity on the daily new cases and new deaths of COVID-19 in 166 countries. Sci Total Environ. 2020;729:139051. doi:10.1016/j.scitotenv.2020.139051.
- World Health Organization. SAGE working group on BCG vaccines and WHO secretariat. Report on BCG vaccine use for protection against mycobacterial infections including tuberculosis, leprosy, and other nontuberculous mycobacteria (NTM) infections; 2017 [accessed 2020 Apr 18]. https://www.who.int/immunization/sage/meetings/2017/october/1_BCG_report_revised_version_online.pdf.
- Uthayakumar D, Paris S, Chapat L, Freyburger L, Poulet H, De Luca K. Non-specific effects of vaccines illustrated through the BCG example: from observations to demonstrations. Front Immunol. 2018;9:2869. doi:10.3389/fimmu.2018.02869.
- Aaby P, Roth A, Ravn H, Napirna BM, Rodrigues A, Lisse IM, Stensballe L, Diness BR, Lausch KR, Lund N, et al. Randomized trial of BCG vaccination at birth to low-birthweight children: beneficial nonspecific effects in the neonatal period? J Infect Dis. 2011;204(2):245–52. doi:10.1093/infdis/jir240.
- Biering-Sørensen S, Aaby P, Napirna BM, Roth A, Ravn H, Rodrigues A, Whittle H, Benn CS. Small randomized trial among low-birth-weight children receiving bacillus Calmette-Guérin vaccination at first health center contact. Pediatr Infect Dis J. 2012;31(3):306–08. doi:10.1097/INF.0b013e3182458289.
- Aaby P, Kollmann TR, Benn CS. Nonspecific effects of neonatal and infant vaccination: public-health, immunological and conceptual challenges. Nat Immunol. 2014;15(10):895–99. doi:10.1038/ni.2961.
- de Castro MJ, Pardo-Seco J, Martinón-Torres F. Nonspecific (Heterologous) protection of neonatal BCG vaccination against hospitalization due to respiratory infection and sepsis. Clin Infect Dis. 2015;60(11):1611–19. doi:10.1093/cid/civ144.
- Jensen KJ, Larsen N, Biering-Sørensen S, Andersen A, Eriksen HB, Monteiro I, Hougaard D, Aaby P, Netea MG, Flanagan KL, et al. Heterologous immunological effects of early BCG vaccination in low-birth-weight infants in Guinea-Bissau: a randomized-controlled trial. J Infect Dis. 2015;211(6):956–67. doi:10.1093/infdis/jiu508.
- Higgins JP, Soares-Weiser K, López-López JA, Kakourou A, Chaplin K, Christensen H, Martin NK, Sterne JAC, Reingold AL. Association of BCG, DTP, and measles containing vaccines with childhood mortality: systematic review. BMJ. 2016;355:i5170. doi:10.1136/bmj.i5170.
- Pollard AJ, Finn A, Curtis N. Non-specific effects of vaccines: plausible and potentially important, but implications uncertain. Arch Dis Child. 2017;102(11):1077–81. doi:10.1136/archdischild-2015-310282.
- Arts RJW, Moorlag SJCFM, Novakovic B, Li Y, Wang SY, Oosting M, Kumar V, Xavier RJ, Wijmenga C, Joosten LAB, et al. BCG vaccination protects against experimental viral infection in humans through the induction of cytokines associated with trained immunity. Cell Host Microbe. 2018;23(1):89–100. doi:10.1016/j.chom.2017.12.010.
- Moorlag SJCFM, Arts RJW, van Crevel R, Netea MG. Non-specific effects of BCG vaccine on viral infections. Clin Microbiol Infect. 2019;25(12):1473–78. doi:10.1016/j.cmi.2019.04.020.
- Zimmermann P, Curtis N. The influence of BCG on vaccine responses - a systematic review. Expert Rev Vaccines. 2018;17(6):547–54. doi:10.1080/14760584.2018.1483727.
- Fuge O, Vasdev N, Allchorne P, Green JS. Immunotherapy for bladder cancer. Res Rep Urol. 2015;7:65–79. doi:10.2147/RRU.S63447.
- Kühtreiber WM, Tran L, Kim T, Dybala M, Nguyen B, Plager S, Huang D, Janes S, Defusco A, Baum D, et al. Long-term reduction in hyperglycemia in advanced type 1 diabetes: the value of induced aerobic glycolysis with BCG vaccinations. NPJ Vaccines. 2018;3(1):23. doi:10.1038/s41541-018-0062-8.
- Usher NT, Chang S, Howard RS, Martinez A, Harrison LH, Santosham M, Aronson NE. Association of BCG vaccination in childhood with subsequent cancer diagnoses: A 60-year follow-up of a clinical trial. JAMA Netw Open. 2019;2(9):e1912014. doi:10.1001/jamanetworkopen.2019.12014.
- Saeed S, Quintin J, Kerstens HHD, Rao NA, Aghajanirefah A, Matarese F, Cheng SC, Ratter J, Berentsen K, van der Ent MA, et al. Epigenetic programming during monocyte to macrophage differentiation and trained innate immunity. Science. 2014;345(6204):1251086. doi:10.1126/science.1251086.
- Mehta S, Jeffrey KL. Beyond receptors and signaling: epigenetic factors in the regulation of innate immunity. Immunol Cell Biol. 2015;93(3):233–44. doi:10.1038/icb.2014.101.
- Italiani P, Boraschi D. Induction of innate immune memory by engineered nanoparticles: a hypothesis that may become true. Front Immunol. 2017;8:734. doi:10.3389/fimmu.2017.00734.
- Brosch R, Gordon SV, Garnier T, Eiglmeier K, Frigui W, Valenti P. Genome plasticity of BCG and impact on vaccine efficacy. Proc Natl Acad Sci U S A. 2007;104(13):5596–601. doi:10.1073/pnas.0700869104.
- Shann F. Editorial commentary: different strains of bacillus calmette–guérin vaccine have very different effects on tuberculosis and on unrelated infections. Clin Infect Dis. 2015;61(6):960–62. doi:10.1093/cid/civ454.
- Moliva JI, Turner J, Torrelles JB. Immune responses to Bacillus Calmette-Guérin vaccination: why do they fail to protect against mycobacterium tuberculosis? Front Immunol. 2017;8:407. doi:10.3389/fimmu.2017.00407.
- World Health Organization. Bacille Calmette-Guérin (BCG) vaccination and COVID-19. Scientific Brief, 12 April 2020; 2020 [accessed 2020 April 14]. https://www.who.int/news-room/commentaries/detail/bacille-calmette-gu%C3%A9rin-(bcg)-vaccination-and-covid-19.