
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.ABSTRACT
Achieving complete vaccination for children has been challenging in Nigeria. Yet, addressing Nigeria’s completeness of vaccination requires ethno-cultural diversity consideration rather than nationally population based. This study explored patterns and determinants of complete vaccination among children of Hausa/Fulani, Igbo and Yoruba, the predominant ethnicities in Nigeria. The study used a cross-sectional data involving 3980 children aged 12–23 months extracted from the 2018 Nigeria Demographic and Health Survey dataset. In this study, complete vaccination is defined as a child who received all recommended vaccinations. A generalized linear mixed model applied to clustered data was used for data analysis (α = 0.05). The prevalence of complete vaccinations was 56.3%, 40.8% and 18.2% among Igbo, Yoruba and Hausa/Fulani children, respectively. The likelihood of complete vaccination was higher among children who were of Igbo (aOR = 1.38; CI: 1.20–1.59) compared with Hausa/Fulani. Predictors of complete vaccination were maternal age-at-childbirth, education, prenatal-care attendant and place of delivery among Hausa/Fulani; place of residence and perceived access to self-medical help, among Igbo; while prenatal-care attendance, among Yoruba. The odds of complete vaccination were higher among Hausa/Fulani (aOR = 1.65; CI: 1.04–2.61), Igbo (aOR = 2.55; CI: 1.20–5.44) and Yoruba (aOR = 4.22; CI: 1.27–13.96) children from higher wealth-quintile households compared to those from poor households. There was evidence of variability in the likelihood of complete vaccination in all the ethnic groups. The Hausa/Fulani tribe had the lowest complete vaccination coverage for children aged 12–23 months. Context-specific program intervention to improve complete vaccination is needed to ensure that the SDG target for vaccination is met.
Introduction
Vaccine-preventable childhood infectious diseases like tuberculosis, poliomyelitis, measles, meningitis, pneumonia, pertussis, tetanus and diphtheria contribute largely to high child morbidity and mortality.Citation1,Citation2 Vaccination is the most cost-effective public health intervention against these diseases, to promote the health, wellbeing and survival of children.Citation1,Citation3 Globally, about two to three million deaths are prevented annually with vaccination and over one billion children have been vaccinated over the last decade.Citation4
Many countries of the world have achieved the target for Sustainable Development Goal – 3 by attaining more than 90% coverage of all basic vaccinations among children aged 12–23 months.Citation5 According to the World Health Organization (WHO),Citation6 85% of infants received 3 doses of diphtheria-tetanus-pertussis (DTP3) vaccine in 2019 globally. However, about 19.7 million infants did not receive the basic vaccines. Of note, over 60% of these unvaccinated children live in Nigeria and other nine countries mostly from sub-Sahara Africa (SSA) and southeast Asia.
Achieving complete vaccination for children has been a huge challenge in Nigeria and this has caused vaccine-preventable infectious diseases to remain a serious public health issue in the country. The National Programme on Immunization has been making frantic efforts toward increasing vaccination coverage and ensuring the availability of vaccines in the country over the last three decades.Citation7 One of the gains of this effort is the recent declaration of Nigeria as a Polio-free country by the WHO in June 2020.Citation8 However, Nigeria is still far from close to attaining the recommended 90% coverage for all the basic vaccinations. Consequently, there is still a high incidence of childhood illness from preventive diseases with attendant morbidity and mortality. Currently, the infant and under-five mortalities are 67/1000 and 132/1000 live births, respectively, and over 51% of these deaths were associated with avoidable diseases and infections.Citation9,Citation10
Several studies have examined factors affecting vaccination coverage in Nigeria in terms of utilization of immunization services and vaccination completion.Citation1,Citation11 These challenges are multifactorial, which include poor health service delivery in terms of shoddy health infrastructure, limited access to vaccination, inadequate skilled manpower and declining resources available for healthcare.Citation1,Citation12 Emergence and reemergence of infectious diseases, insecurity, ravaging poverty, the continual occurrence of wars and conflicts in some regions of the country also limit access to vaccination.Citation13,Citation14 Additionally, some research findings have isolated socioeconomic factors including maternal education, maternal age, parental occupation, household wealth, religion, etc., as predictors of complete vaccination.Citation7,Citation15–18 One important factor that is yet to be fully explored in Nigerian childhood vaccination research is ethnicity.
Nigeria is one of the most populous ethnically diverse countries worldwide. Nigeria is divided into six geopolitical zones with more than 250 ethnic groups.Citation9 In Nigeria, ethnicity is a complicated construct in that ethnic affinity has become an important form of identity.Citation19,Citation20 As a major cultural factors, ethnicity has shown great influence on the uptake of health programs including vaccination. Hausa/Fulani, Igbo and Yoruba are the predominant ethnic groups and these ethnic groups have diverse socio-cultural ideals and practices which impact on childcare and health outcome.Citation21 For instance, some aspects of culture consider the male child to be superior to the female child which influences the kind of attention the children get from the parents.Citation22 The magnitude of this variation and disparity in child health-care utilization and health outcome in Nigeria is of great public health importance. This ethnic diversity constitutes a shortfall in achieving the goal of SDG – 10 which is to “reduce inequality within and among countries”.Citation5
Vaccination is still sub-optimal despite the improvement in vaccination coverage in the last 10 years. Studies have reported disparities in vaccination coverage across the geopolitical regions in Nigeria, which was basically classified and aligned with ethnic groups.Citation17,Citation18 Variations and inequalities have also been observed at the individual level.Citation7,Citation17,Citation23 Wide disparities in vaccination within a country has a significantly negative impact on the country’s health indicators. It is pertinent to understand these variations for proper interventions that may affect child survival to be instituted within specific micro units in Nigeria. With limited research regarding the influence of ethnicity on complete vaccination among children aged 12–23 months in Nigeria, this study was designed to fill the gap. Identification of such predictors may boost efforts to increase vaccination coverage among the affected ethnic groups. The study will also provide an assessment of how close Nigeria is toward achieving SDG 3 – on health for all, and SDG 10 – on the reduction of inequalities within countries.
Methods
Study design, area and population
The present analysis was conducted using the 2018 Nigeria Demographic Health Survey (NDHS) data. The NDHS is a population-based cross-sectional design aimed at providing maternal and child health indicators to assist policymakers and programme managers in designing and evaluating programs and strategies for improving the health of the country’s population.Citation9 Nigeria is the most populated country in Africa with the population figure of about 200 million, of whom 17% were under-five children in 2018. Administratively, Nigeria has 36 states including a Federal Capital Territory zoned into six geopolitical groups. Of over 250 ethnic compositions, Hausa/Fulani, Igbo and Yoruba are predominant. The six regions in Nigeria are mainly defined by these three ethnic groups. While the Yoruba and Igbo women predominantly have formal education, only a few of such women are found in Hausa/Fulani ethnic groups. The Hausa/Fulani women mostly belong to Islamic religion. Contrariwise, the Igbo and Yoruba women are mainly Christians.
Two-stage cluster sampling technique was employed for the survey using the sampling frame containing the enumeration areas (EAs) of the 2006 Nigeria Population and Housing Census (NPHC). At the first stage, 1400 EAs (referred to as clusters) were selected as the primary sampling units; the second stage involved the selection of 40,427 households as the secondary units for the survey. The detailed description of the sampling design and strategies has been reported in the 2018 NDHS report.Citation9
In the present study, data of children aged 12–23 months, who had valid information on the basic recommended vaccines, belonged to eligible women of childbearing age who were residents of the selected households within the clusters, and either of the Hausa/Fulani or Igbo or Yoruba tribes. Children with missing information or ‘don’t know’ records were excluded from the analysis. A total of 3980 met all these criteria. In this study, the term ‘cluster’ was used in DHS to describe the ‘neighborhood’ where children live.
Study variables
The outcome of interest was the complete vaccination status of children aged 12–23 months as at a year old. Going by WHO recommendations, a child who received one dose of Bacille Calmette–Guerin (BCG), one dose of measles, three doses of polio, and three doses of diphtheria, tetanus and pertussis (DPT) vaccines by the age of 12 months has a complete vaccination.Citation9,Citation16 Therefore, children who have been immunized with all these basic vaccines are deemed to have complete vaccinations – this is coded “1”; and “0” if otherwise.
The key independent variable was ethnicity. The analysis was restricted to the three most prominent ethnic groups: Hausa/Fulani, Igbo and Yoruba in Nigeria.Citation24 Other independent variables were included to define child/maternal, household and health characteristics according to empirical literature.Citation25,Citation26 These include child sex, birth order, maternal age-at-birth, employment, education, marital status, region, place of residence, religion, household wealth status, media exposure, health insurance coverage, health decision-involvement, perceived access to self-medical help, place of delivery and prenatal-care assistance.
A media exposure variable was derived and classified as exposed if a household had access to at least one of radio, television or newspaper; otherwise, not exposed. The wealth index variable was derived from the generated weighted factor score using principal component analysis as contained in the recode file. These scores were categorized into low, middle, and high wealth quintiles. Health decision-involvement’s variable is premised on women’s ability to decide on personal health care, household purchases and visitation to relatives. These related variables are coded as 2 (if she decides alone), 1 (if joint decision) and 0 (if she took no part), respectively. The aggregated scores were classified as 0 (no involvement), 1–3 (low) and 4–6 (high). Similarly, perceived access to self-medical help’s variable is derived subject to a woman opinion on the following dichotomized variables: obtaining permission to visit a health facility, getting the required treatment fee, distance to a health facility, or being accompanied to the health facility – 0 score implied no problem; otherwise, the problem.
Statistical methods of analysis
Frequencies, percentages and charts were used as descriptive measures at the univariate stage. The chi-square test was used to assess the association between the outcome variable and the individual independent variables at the bivariate stage. Asides, both simple and multiple GLMMs with a binomial random distribution and logit link function are used to explore the predictors of children’s complete vaccination. As clustering of children’s complete vaccination may ensue if characteristics within clusters are alike, failure to account for such clustered or nested nature of the data often lead to biased parameter estimates of the fixed effects. The method also supports the dependence structure of data for units within these clusters and estimates the magnitude of such correlation after taking into consideration the inclusion of explanatory variables.Citation27
Model description
An extension of generalized linear models is the GLMM that accounts for all contextual information. The model appropriately estimates fixed- and random-effects for nested data. In brief, the model is as follows:
Let be the complete vaccination status of ith child in the jth cluster defined as
For , the GLMM can be described as follows:
where
p-variable is the level-1 denoted by (which varies within and between clusters); r-variable is the level-2 denoted by
(varies only between clusters); and the random intercept is
At the bivariate level, GLMM was used to identify the respective explanatory variable’s influence on child complete vaccination. Also, it was used to identify predictors of complete vaccinations among children aged 12–23 months using a 4-stage approach at the multivariate level for the pooled data. The adopted 4-stage random intercept was premised on the classification of explanatory variables such that models 1, 2 and 3, respectively, included variables to define child/maternal, household and health characteristics, irrespective of their significance status at the bivariate level. Thereafter, significant factors from models 1–3 were included in the final model 4. Also, correlates of children’s complete vaccinations peculiar to each of the ethnic groups were identified using the significant factors (p < .05) in any of the simple models for each of the ethnicity. The odds ratios (OR) including their CIs and the intra-neighborhood correlation coefficient (ICC) which quantifies the proportion of variance explained due to hierarchical data clustering effect are reported. In each of the models, ICC was computed using the estimated random intercept variance and ICC ≥ 2% is deemed to have a significant neighborhood effect which calls for a multilevel approach.Citation28 Akaike Information Criteria (AIC) values are also reported for model comparison; the model with the least value was adjudged as being more adequate.Citation29 All analyses were carried out at 5% level of significance, using STATA 14 SE (StataCorp LP, College Station, USA).
Ethical approval
Ethical approval for the parent study was obtained from the Nigeria National Ethics Committee. Informed consent and all other international ethical standards of confidentiality and anonymity were certified. The details of the ethical approval have been reported earlier.Citation9 The Demographic and Health Surveys Program approved the utilization of the dataset for the present analysis.
Results
Participants’ characteristics
Weighted percentages of participants’ demographic, household and health characteristics classified by complete vaccination status are presented in . Most children were of Hausa/Fulani (62.9%), followed by Igbo (19.5%) and Yoruba (17.6%) extraction. Males (52.2%) were slightly more than females; the same pattern was exhibited in each of the tribes. The most and least proportion of children were those whose mothers were young adults (46.0%) and teenage (13.3%) mothers at the time of their birth, respectively. While similar distribution was observed among Igbo and Yoruba, the least percentage of children were those whose mothers were adults (15.4%) among the Hausa/Fulani ethnic group ().
Table 1. Distribution of participants and prevalence of complete vaccination according to child/maternal, household and health characteristics
Children aged 12–23 months who have completed vaccinations were equally likely distributed by sex in all the tribes. The least and most proportion who have completed vaccinations were observed among teenage mothers at childbirth and young adults, respectively, in all the tribes. The higher the level of education attained, the higher the prevalence of complete vaccinations which cut across the ethnics. Specifically, complete vaccinations were more common among the secondary/tertiary education in Hausa/Fulani (34.0%), Igbo (64.2%) and Yoruba (45.7%). Similarly, the richer the household, the higher the proportion of complete vaccinations. Among rural resident mothers, 15.1%, 41.6% and 30.6% of the Hausa/Fulani, Igbo and Yoruba children, respectively, received complete vaccinations. The more the mother’s empowerment to make decisions, the higher the proportion of complete vaccinations ().
Pattern of children’s vaccinations by ethnicity
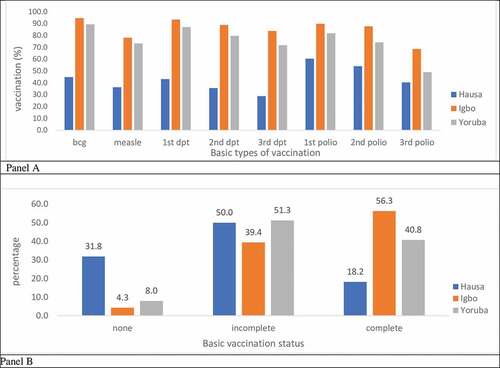
reveals the pattern of all the basic and recommended vaccinations received by the children as well as the complete vaccination status. The prevalence of BCG, measles and three doses of DPT and three doses of polio vaccines were respectively the highest among Igbo, followed by Yoruba (Panel A). Of note, 31.8% of the children among the Hausa/Fulani ethnic group received none of the basic and required vaccines compared to Igbo (4.3%) and Yoruba (8.0%). Children of Igbo (56.3%) extraction had the highest prevalence of complete vaccinations, followed by Yoruba (40.8%) and the least, Hausa/Fulani (18.2%) (Panel B).
Figure 1. Percentage distribution of the recommended basic vaccines (Panel A) and complete vaccination (Panel B) by ethnicity
Factors influencing complete vaccination among children aged 12-23 months by ethnicity
The determinants of complete vaccination among the Hausa/Fulani children were maternal age at childbirth, education, household wealth, place of delivery and prenatal-care attendance. Place of residence, household wealth and perceived access to self-medical help significantly influenced the tendency of complete vaccination among the Igbo; only household wealth and prenatal-care attendance factors were identified as significant predictors of complete vaccination among the Yoruba children. Household wealth was observed as the only common predictor of complete vaccination across all the ethnic groups. The odds ratio increases as the level of wealth increases. Specifically, the odds of complete vaccination were about 2, 3 and 4 times higher among Hausa/Fulani (aOR = 1.65; CI: 1.04–2.61), Igbo (aOR = 2.55; CI: 1.20–5.44) and Yoruba (aOR = 4.22; CI: 1.27–13.96) children, respectively, from household in the rich wealth category compared to those from households in the poor wealth category. Meanwhile, only the GLMM model for Hausa/Fulani ethnic group shows a significant clustering effect explained by neighborhood characteristics. About 18% of the variance in the likelihood of being vaccinated with complete vaccination occurred across clusters ().
Table 2. Adjusted odds ratios of complete vaccination by ethnicity in Nigeria
Predictors of complete vaccination among children aged 12-23 months
The unadjusted and adjusted odds of complete vaccination with child/maternal, household and health characteristics using the pooled data are presented in . Igbo (OR = 6.51; CI: 4.99–8.48) and Yoruba (OR = 3.99; CI: 3.01–5.29) children were about 7 and 4 times significantly more likely to receive complete vaccinations relative to their Hausa/Fulani counterparts. These odds, however, reduced in models 1, 2 & 3 when child/maternal, household and health utilization factors were controlled for, respectively. Corresponding to models 1, 2 & 3, the odds of complete vaccination were 2.1 (aOR = 2.13; CI: 3.01–5.29) and 1.3 (aOR = 1.31; CI: 0.95–1.82), 2.9 (aOR = 2.91; CI: 1.86–4.57) and 1.7 (aOR = 1.65; CI: 1.16–2.35), 2.8 (aOR = 2.78; CI: 2.08–3.70) and 1.7 (aOR = 1.68; CI: 1.24,2.28) times higher among Igbo and Yoruba children, respectively, compared to Hausa/Fulani.
Table 3. Crude and adjusted odds ratios of complete vaccination in Nigeria
In Model 4 (with the least AIC = 3604.2), the odds of being vaccinated with all the basic vaccinations was higher among children of Igbo descendants (aOR = 1.49; CI: 1.08–2.06) compared with Hausa/Fulani. Although not statistically significant, the adjusted odds of complete vaccination was about 12% less likely among Yoruba compared to Hausa/Fulani children. Other additional significant factors influencing complete vaccination among children aged 12–23 months were maternal age at childbirth, education, place of residence, household wealth, decision-making involvement, perceived access to self-medical help, place of delivery and prenatal-care attendance. In all the models, the reported ICC suggests the appropriateness of the choice of our model. In particular, a significant (ICC = 15.2%; p < .05) variation in children complete vaccination was attributed to the clustering effect at neighborhood level (Model 4, ).
Discussion
Completeness of vaccination among children aged 12 to 23 months is a major public health challenge in Nigeria which has accounted for an inadequate reduction in childhood morbidity and mortality associated with the prevailing vaccine-preventable infectious diseases. Ethnic diversity is one of the important factors mitigating against this goal, especially in a populous and an ethnically diverse population like Nigeria. This study explored the effect of ethnicity on children’s complete vaccination.
Our study showed a significant relationship between ethnicity and complete vaccination. Children of Igbo ethnic extraction had the highest prevalence of complete vaccinations, followed by Yoruba and the least, Hausa/Fulani. Previous reports in Nigeria showed that children in the northern geopolitical zone which mostly consists of the Hausa/Fulanis have a lower rate of complete vaccinations as compared with those in the south where the Yorubas and Igbos reside.Citation9,Citation30 This could be attributed to the belief of the Hausa/Fulanis that vaccines, for example, the polio vaccines are contaminated with anti-fertility agents.Citation31,Citation32 Hence, the refusal to get their children vaccinated.
The higher the level of education attained and the richer the household is, the higher the likelihood of complete vaccinations which cut across the three ethnic groups as observed in this study. These factors are among other social determinants of health which previous studies reported to contribute to disparities in vaccination completion.Citation1,Citation11,Citation23 Family wealth and literacy, especially mother’s education, is known to contribute significantly to child survival.Citation12,Citation25 Also, this has been reported by WHOCitation18 in the course of exploring the inequality in childhood vaccination for other countries in SSA. A mother’s understanding of the safety of vaccines, importance and benefits of vaccination impact the health of the children and family. In addition, our study noted that a third of the children among the Hausa/Fulani ethnic group received none of the basic and required vaccines compared to Igbo and Yoruba. Vaccination acceptance and coverage has been consistently low in the Northern region where the Hausa/Fulanis normally reside.Citation32 Some studies have attributed this low coverage, which can be as low as 4% in some northern states where Hausa/Fulanis reside, to poor education and most importantly trust lacking in the vaccinators and fear of the vaccines.Citation31,Citation32
Our study consistently showed that complete vaccination is lowest among Hausa/Fulani children. The determinants of complete vaccination according to this current study among the children in this tribe were maternal age at childbirth, education, household wealth, place of delivery and prenatal attendance. Child marriage is common among the Hausa/Fulani ethnic group than the other ethnic groups. This leads to childbirth at a young age with the possibility of no knowledge and experience about childcare and a low sense of responsibility compared with older mothers.Citation33 They often have low education, most often not currently working with associated financial insecurity. Poverty is recognized as an important factor causing low vaccination uptake.Citation3,Citation17 All these factors impact on complete vaccination of children, as the mothers may have little or no knowledge, information and finances to improve childcare and survival.
The significant predictors of complete vaccination among the Igbo ethnic group were the place of residence, household wealth and perceived access to self-medical help, while household wealth and prenatal attendance factors were identified as significant predictors of complete vaccination among the Yoruba children. Generally, household wealth was observed as the only common predictor of complete vaccination across all the ethnic groups. Coverage of full vaccination has been observed to be higher among the children of the wealthy population in the country.Citation16,Citation17 This highlights the pervasion in inequality associated with wealth status, as children from poor households are less likely to receive complete vaccinations than those in rich households.
In addition, our finding showed the likelihood of a child being vaccinated with all the basic vaccinations (one dose of BCG, one dose of measles, three doses of polio, and three doses of DPT vaccines) by the age of 12 months was higher among children of Igbo and Yoruba ethnic groups compared with Hausa/Fulani children. Studies have identified gaps in vaccination completion in Northern Nigeria among the Hausa/Fulani children.Citation32,Citation34 Reasons highlighted were poor or no education about the vaccines and vaccination services, insufficient knowledge about the vaccine safety and importance of vaccines among mothers and caretakers.
This study emphasizes the effect of ethnic inequality on child complete vaccination. However, a few limitations were observed. Firstly, insecurity issues prohibiting fieldwork may affect data collection in the North and other regions of the country that are affected, as documented in the 2018 NDHS report presented by the originators of the data used for this study.Citation9 The causal association may be difficult to establish considering the cross-sectional nature of the study.
Conclusions
This study showed that children from the Hausa/Fulani ethnic group had a significantly lower tendency of vaccination completion. Three of every five Igbo children had complete vaccination compared to only two of every five Yorubas and one of every five Hausa/Fulani children. This is evident that the vaccination rate is generally low in Nigeria, varied significantly across different ethnic groups and worse among the Hausa/Fulanis. We have identified the drivers of complete vaccination peculiar to each of the ethnicities; and observed that household wealth status is a major driver of complete vaccination irrespective of a child’s ethnic group. Ethnic inequality is a strong social-cultural determinant of complete vaccination in Nigeria.
Recommendations
We therefore recommend that policymakers and programme implementers in the region where the Hausa/Fulanis are resident should understudy the factors that promote completeness of vaccination in the Igbo-dominated region. Knowledge of these factors can be used to develop specific interventions that could help increase vaccination coverage among the Hausa/Fulanis. The higher vaccination coverage among the Igbos and the Yorubas notwithstanding, there are needs to increase vaccination access across all parts of Nigeria. Interventions to eliminate disparities in vaccination completion are of utmost importance if Nigeria will achieve 90% vaccination coverage and, consequently, a reduction in child death. This must specifically target the affected ethnic group.
Authors’ contribution
ASA and RFA conceived the study. RFA analyzed the data while RFA, ASA and AFF interpreted the analyzed data. RFA and MMS drafted the original manuscript. RFA, MMS, BMG, ATS, AFF and ASA reviewed and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors appreciate DHS Program for granting free access to the data used for the study.
Additional information
Funding
References
- Odusanya OO, Alufohai EF, Meurice FP, Ahonkhai VI. Determinants of vaccination coverage in rural Nigeria. BMC Public Health [Internet] 2008 [accessed 2020 Oct 17]; 8:381.Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-8-381.
- Hosseinpoor AR, Bergen N, Schlotheuber A, Gacic-Dobo M, Hansen PM, Senouci K, Boerma T, Barros AJD. State of inequality in diphtheria-tetanus-pertussis immunisation coverage in low-income and middle-income countries: a multicountry study of household health surveys. Lancet Glob Heal [Internet] 2016 [accessed 2020 Oct 18]; 4:e617–26. Available from: http://www.who
- Balraj V, Mukundan S, Samuel R, John TJ. Factors affecting immunization coverage levels in a district of india. Int J Epidemiol [Internet] 1993 [accessed 2020 Oct 18]; 22:1146–53. Available from: https://academic.oup.com/ije/article/22/6/1146/650231
- Vaccines and immunization [Internet]. [cited 2020 Oct 18]; Available from: https://www.who.int/health-topics/vaccines-and-immunization#tab=tab_1
- United Nations. Transforming our World: The 2030 Agenda for Sustainable Development; 2015.
- Immunization coverage [Internet]. WHO; 2020 [accessed 2020 Oct 18]; Available from: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage
- Oleribe O, Kumar V, Awosika-Olumo A, Taylor-Robinson SD. Individual and socioeconomic factors associated with childhood immunization coverage in Nigeria. Pan Afr Med J. 2017;26.
- WHO a veritable partner in achieving Nigeria’s Polio-free status, ED of NPHCDA affirms [Internet]. WHO; 2020 [accessed 2020 Oct 18]; Available from: https://www.afro.who.int/news/who-veritable-partner-achieving-nigerias-polio-free-status-ed-nphcda-affirms
- National Population Commission (NPC) [Nigeria] and ICF International. Nigeria demographic and health survey 2018 [Internet]. Abuja (Nigeria, and Rockville, Maryland, USA); 2019 [accessed 2019 Nov 5]. Available from: www.DHSprogram.com
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, Cousens S, Mathers C, Black RE. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet [Internet] 2015 [accessed 2020 Oct 7]; 385:430–40. Available from: http://www.thelancet.com/article/S0140673614616986/fulltext
- Antai D. Inequitable childhood immunization uptake in Nigeria: A multilevel analysis of individual and contextual determinants. BMC Infect Dis. 2009;9:9. doi:10.1186/1471-2334-9-181.
- Rainey JJ, Watkins M, Ryman TK, Sandhu P, Bo A, Banerjee K. Reasons related to non-vaccination and under-vaccination of children in low and middle income countries: findings from a systematic review of the published literature, 1999-2009. Vaccine. 2011;29:8215–21. doi:10.1016/j.vaccine.2011.08.096.
- The global risks report 2018 13th edition insight report [Internet]; 2018 [accessed 2020 Oct 18]. Available from: http://wef.ch/risks2018
- Koumaré AK, Traore D, Haidara F, Sissoko F, Traoré I, Dramé S, Sangaré K, Diakité K, Coulibaly B, Togola B, et al. Evaluation of immunization coverage within the expanded program on immunization in kita circle, mali: a cross-sectional survey. BMC Int Health Hum Rights [Internet] 2009 [accessed 2020 Oct 18]; 9:S13.Available from: /pmc/articles/PMC3226232/?report=abstract
- Adedokun ST, Uthman OA, Adekanmbi VT, Wiysonge CS. Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors. BMC Public Health. 2017;17:1–10. doi:10.1186/s12889-017-4137-7.
- Adebowale A, Obembe T, Bamgboye E. Relationship between household wealth and childhood immunization in core-North Nigeria. Afr Health Sci [Internet] 2019 [accessed 2020 Aug 20]; 19:1582–93.Available from: /pmc/articles/PMC6531962/?report=abstract
- Ataguba JE, Ojo KO, Ichoku HE. Explaining socio-economic inequalities in immunization coverage in Nigeria. Health Policy Plan [Internet] 2016 [accessed 2020 Oct 18]; 31:1212–24. Available from: https://academic.oup.com/heapol/article/31/9/1212/2452986
- WHO. Explorations of inequality: childhood immunization. WHO [Internet]; 2019 [accessed 2020 Oct 18]; Available from: http://www.who.int/gho/health_equity/report_2018_immunization/en/
- Reed HE, Mberu BU. Ethnicity, religion, and demographic behavior in Nigeria [Internet]. Dordrecht: Springer; 2015 [accessed 2020 Nov 25]. p. 419–54. Available from: https://link.springer.com/chapter/10.1007/978-90-481-8891-8_21
- Obi-Ani NA, Pan O-AP. Africanism and the rising ethnic distrust in Nigeria: an assessment. Ianna J Interdiscip Stud. 2019;1:65–75.
- Griffiths P, Madise N, Whitworth A, Matthews Z. A tale of two continents: A multilevel comparison of the determinants of child nutritional status from selected African and Indian regions. Heal Place. 2004;10:183–99. doi:10.1016/j.healthplace.2003.07.001.
- Ahoo TJ. Culture and the education of female children in gwer west local government area of Benue state. Ianna J Interdiscip Stud. 2019;1:45–55.
- WHO. State of inequality: childhood immunization. WHO [Internet]; 2019 [accessed 2020 Oct 18]; Available from: http://www.who.int/gho/health_equity/report_2016_immunization/en/
- Adedini SA, Odimegwu C, Imasiku ENS, Ononokpono DN. Ethnic differentials in under-five mortality in Nigeria. Ethn Heal [Internet] 2015 [accessed 2020 Aug 18]; 20 145–62. Available from: /pmc/articles/PMC4337727/?report=abstract
- Soura AB, Mberu B, Elungata P, Lankoande B, Millogo R, Beguy D, Compaore Y. Understanding Inequities in child vaccination rates among the urban poor: evidence from nairobi and ouagadougou health and demographic surveillance systems. J Urban Heal. 2015;92:39–54. doi:10.1007/s11524-014-9908-1.
- Bago BJ, Terefe W, Mirutse G. Individual and community level factors associated with defaulting of immunization among 12-59 months children in Ethiopia: multilevel modeling analysis using 2011Ethiopia demographic and health survey. Curr Pediatr Res [Internet] 2018 [accessed 2019 Oct 16]; 22:95–110. Available from: https://www.alliedacademies.org/articles/individual-and-community-level-factors-associated-with-defaulting-ofimmunization-among-1259-months-children-in-ethiopia-multilevel-10004.html.
- Andersson N, Lamothe G. Clustering and meso-level variables in cross-sectional surveys: an example of food aid during the Bosnian crisis. BMC Health Serv Res. 2011;11.
- Gebru KF, Haileselassie WM, Temesgen AH, Seid AO, Afework Mulugeta B. Determinants of stunting among under-five children in Ethiopia: a multilevel mixed-effects analysis of 2016 Ethiopian demographic and health survey data. BMC Pediatr. [Internet] 2019 [accessed 2019 Jun 22]; 19:1–13. doi:10.1186/s12887-019-1545-0.
- Fagbamigbe AF, Afolabi RF, Yussuf K, Adebowale AS, Yusuf BO. Unobserved heterogeneity in the determinants of under-five mortality in Nigeria: frailty modeling in survival analysis. Afr J Appl Stat. 2019;6:565–83. doi:10.16929/ajas/2019.565.231.
- National Population Commission (Nigeria) and ICF International. Nigeria demographic and health survey 2013. Abuja (Nigeria): The Demographic and Health Surveys (DHS) Program; 2014. [accessed 2019 Nov 5]. http://www.dhsprogram.com/
- Renne E. Perspectives on polio and immunization in Northern Nigeria. Soc Sci Med. 2006;63:1857–69. doi:10.1016/j.socscimed.2006.04.025.
- Yahya M. Polio vaccines - “no thank you!” barriers to polio eradication in Northern Nigeria. Afr Aff (Lond) [Internet] 2007 [accessed 2020 Oct 18]; 106:185–204. Available from: https://academic.oup.com/afraf/article/106/423/185/50647
- Rahman M, Obaida-Nasrin S Factors affecting acceptance of complete immunization coverage of children under five years in rural Bangladesh; 2010.
- Gunnala R, Ogbuanu IU, Adegoke OJ, Scobie HM, Uba BV, Wannemuehler KA, Ruiz A, Elmousaad H, Ohuabunwo CJ, Mustafa M, et al. Routine vaccination coverage in northern Nigeria: results from 40 district-level cluster surveys, 2014-2015. PLoS One [Internet] 2016 [cited 2020 Oct 18]; 11:e0167835. Available from: https://dx.plos.org/10.1371/journal.pone.0167835