
ABSTRACT
Vaccinated or not? This is an attitude survey for ‘approach-avoidance conflict’ under uncertainty. Therefore, measuring people’s attitude toward COVID-19 vaccination is relatively distinctive from an attitude over a general conflict. An online survey of 3123 respondents from 30 provincial-level regions — out of 31 — on the Chinese mainland was conducted from January 22 to 27, 2021 to measure their willingness to be vaccinated. We found that over half of the respondents chose the options ‘not to be vaccinated now’ and ‘wait and see before making a vaccination decision,’ thereby indicating that people’s willingness to be vaccinated is not as optimistic as anticipated in the early stage of vaccination in China. Hence, investigators should carefully select the measuring method to assess the ‘true’ levels of willingness to accept COVID-19 vaccines. Lastly, the relevant departments should fully predict obstacles to achieve immunity coverage and prepare for the ‘vaccine hesitancy’ of people in need.
1. Introduction
COVID-19 has produced catastrophic consequences, although the largest and most rapid global arrangement of vaccines is currently under way.Citation1 Presently, people around the world have to face a difficult choice: to be vaccinated or not? This situation is an ‘approach-avoidance conflict’ under uncertainty. Given that the major concerns include vaccine safety and effectiveness,Citation2 the gains (e.g. vaccine efficiency) we obtained and losses (unsafety of vaccines) we avoided are uncertain in reality.
Previous research has established that people are generally uncertainty averse.Citation3 Uncertainty averse agents prefer betting on events with known probability compared with betting on those with unknown probability.Citation4 The new problem imposed by uncertainty is that uncertain gains (e.g. vaccine efficiency) will be less attractive, whilst uncertain losses (unsafety of the vaccine) will be more repulsive, thereby making people more hesitant to make a decision and tend to wait and see before making such a decision. Consequently, numerous individuals during the 2009 H1N1 pandemic did not seek vaccination immediately but decided to ‘wait and see’ until further information was available on vaccination costs.Citation5 The tendency of people to delay accepting or refusing vaccines despite the availability of vaccination services is a global phenomenon called vaccine hesitancy.Citation6 The World Health Organization (WHO) identified vaccine hesitancy as one of the top 10 global health threats in 2019 (https://www.who.int/news-room/spotlight/ ten-threats-to-global-health-in-2019). Therefore, we conjecture that measuring people’s willingness to be vaccinated has its particularity. If we simply adopt the conventional attitude survey method, then we will be unable to measure people’s real willingness to be vaccinated.
A study recently published in Nature Medicine has reported the acceptance of COVID-19 vaccination amongst 13,426 people in 19 countries. The result shows that 71.5% of the respondents reported that they would be very or somewhat likely to take a COVID-19 vaccine. Differences in acceptance rates ranged from nearly 90% (i.e. China) to under 55% (i.e. Russia).Citation7
Nevertheless, further analysis of the report reveals that the findings are questionable.
Firstly, the aforementioned study’s conclusion is derived by presenting the following premise: ‘If a COVID-19 vaccine is proven safe and effective and is available to me, I will take it.’Citation7 Note that the safety and efficiency of any COVID-19 vaccine on the market remains in an uncertain state; hence, even the reported clinical data (probability/frequency) on safety and efficiency have a ‘changeability’ feature that may play a major role in preparing for uncertainty.Citation8,Citation9
Secondly, only residents’ acceptance of a ‘safe and effective’ vaccine was measured. The likelihood that people may hesitate or wait and see before making a decision was overlooked intentionally or unintentionally. Note that research on behavioral decision-making has shown that many seemingly insignificant choices architectures that force the reversal of choice results. Examples include the positive–negative framework for the description of results,Citation10 acceptance–rejection response modeCitation11 and default–optional option setting.Citation12 Li et al (2020) revealed that the addition of a third option (Not decided yet) can narrow the proportion difference of two options of a binary choice (e.g., remain a member of the European Union or leave the European Union) and even shift the majority vote.Citation13
Thus, the purpose of this survey, which was conducted in a random sampling from the population of China, is twofold. The first objective is to extend the work of Lazarus et al. (2021) by assessing the acceptance rate under a condition that the premise of ‘a COVID-19 vaccine is proven safe and effective and is available’ is NOT provided. Then, the second goal is to improve the measurement of COVID-19 vaccination intention by adding a third option of ‘wait and see.’ We are optimistic that the improvement can comprehensively and accurately measure respondents’ attitude toward COVID-19 vaccination.
2. Method
An online survey of 3123 respondents from 30 provincial-level regions — out of 31 — on the Chinese mainland was conducted from January 22 to 27, 2021, to measure their willingness to be vaccinated by using the sample service of WenJuanXing (www.sojump.com), an online crowdsourcing platform in China. The sampling across 30 provincial-level regions — out of 31 — on the Chinese mainland was determined and carried out by WenJuanXing with a task requirement of a roughly even area/gender balance and a distinctive age distribution (people who are 18–60 could be eligible for vaccination in China).
2.1. Measuring vaccination acceptability
Firstly, to make our results comparable to those of Lazarus et al. (2021), we chose the precise same measurement scale they used in their global survey of potential acceptance of a COVID-19 vaccine. The item and instruction to measure vaccination acceptability are as follows.
Currently, a coronavirus vaccine (COVID-19 vaccine) is available in your area, please indicate your level of agreement with the following statements: ‘Completely agree, Somewhat agree, Neutral/No opinion, Somewhat disagree, Completely disagree.’
Secondly, considering that some clinical studies already provided some efficacy/effectiveness results at the time our survey was conducted, we used a between-participant experimental design. In this design, each participant was asked to rate the ‘willingness to get vaccinated’ and ‘willingness to wait and see,’ given (a) that knowing COVID-19 vaccine has side effects, (b) that knowing COVID-19 vaccine has no side effects and (c) that they did not know whether COVID-19 vaccine has side effects or not.Citation14 Each participant was assigned to one of the three conditionsFootnote1 only. We administered three versions of the questionnaire to the respondents, and these versions differed only in the phrases inside the parentheses. The rating task and instruction to rate are as follows:
Imagine that you (know that COVID-19 vaccine has side effects/know that COVID-19 vaccine has no side effects/do not know whether COVID-19 vaccine has side effects or not), please indicate your decision by dragging to the slide-bar or directly entering a number in the text box to rate your ‘willingness to get vaccinated’ and ‘willingness to wait and see’ separately (0 for very reluctant to and 100 for very willing to).
2.2. Measuring vaccine hesitancy
Apart from the preceding measuring of vaccination acceptability, we added the measurement of vaccine hesitancy, which was inspired by the study of approach-avoidance conflict and the third option.Citation13
Items to measure vaccine hesitancy are shown as follows.
Item 1: Please indicate when you think you can decide whether or not to get vaccinated by dragging to slide bar on a 6-point scale, ranging from completely sure to make a decision now (1) to completely sure to make a decision after wait-and-see (6).
Item 2:Please indicate your present decision by ticking one of the following three options:
get vaccinated now
not get vaccinated
wait and see
2.3. Querying reasons for hesitancy
To query the reasons why the respondents choose to wait and see (hesitancy), they were asked to respond to the following instruction: ‘Now you have chosen to wait and see, please write down in the box that you will make a decision until when/under what circumstances.’
The wording was recorded and counted. The word frequency of all answers were to be analyzed to determine the main factors that caused people to choose the ‘wait and see’ (hesitancy) option.
3. Result
We conducted a random sampling online survey of 3123 respondents from 30 provincial-level regions — out of 31 — on the Chinese mainland from January 22 to 27, 2021. The sample sizes were estimated using G*Power,Citation15 which assumed a medium effect size of 0.25 (characteristic of most social-psychological findings). Our design could achieve 95% power with 400 participants. shows the demographic characteristics of the respondents.
Table 1. Characteristics of survey respondents (n = 3123)
3.1. Vaccination acceptability
3.1.1. Under the condition of not mentioning that COVID-19 vaccine is safe and effective
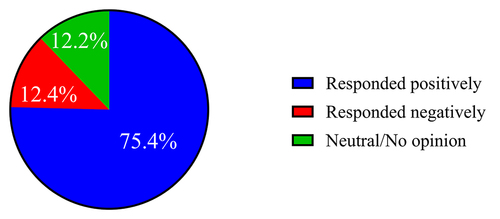
Under the condition of not mentioning that vaccines are safe and effective (i.e., a COVID-19 vaccine is available in your area), we found that 75.4% [completely agree (43.9%) + somewhat agree (31.5%)] of respondents in China would take a COVID-19 vaccine, 12.2% would take a neutral/no opinion, 12,4% [somewhat disagree (9.2%) + completely disagree (3.2%)] would not take a COVID-19 vaccine () using the same measuring as that used by Lazarus et al. (2021). Such a percentage is apparently lower than that (i.e. 88.6%) surveyed by Lazarus et al. (2021) under the condition of ‘a COVID-19 vaccine is proven safe and effective and is available.’
Figure 1. COVID-19 vaccination acceptability in China under the condition of the safety and efficiency of the vaccine is unknown (not provided). According to Lazarus et al.’s (2021) definition, ‘completely agree’ + ‘somewhat agree’ = responded positively; Neutral/No opinion = Neutral/No opinion; ‘somewhat disagree’ + ‘completely disagree’ = responded negatively.
3.1.2. Under conditions of know that COVID-19 vaccine has side effect/know that COVID-19 vaccine has no side effect/do not know whether COVID-19 vaccine has side effect or not
shows our participants’ vaccination acceptability.
Figure 2. Mean ratings of the respondents’ ‘willingness to get vaccinated’ and ‘willingness to wait and see’ in conditions of know that COVID-19 vaccine has side effect/know that COVID-19 vaccine has no side effect/do not know whether COVID-19 vaccine has side effect or not (0 for very reluctant to and 100 for very willing to). Left bar represents ‘willingness to get vaccinated,’ whilst the right bar represents ‘willingness to wait and see.’
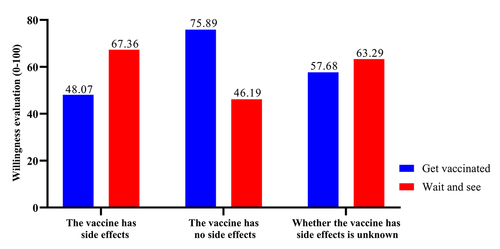
A one-way MANCOVA revealed significant differences in the mean ratings of ‘willingness to get vaccinated’ across the three decision situations (F (2, 3122) = 294.36, p < .001, partial η2 = .159) after statistically controlling for gender, age, education level, income level, health level and participants’ concern level of their own health. Respondents’ mean rating of ‘willingness to get vaccinated’ under the condition of ‘do not know whether COVID-19 vaccine has side effect or not’ (M = 57.68) was less than that under the condition of ‘know that COVID-19 vaccine has no side effect’ (M = 75.89) but greater than that under the condition of ‘know that COVID-19 vaccine has side effect’ (M = 48.07).
Differences in the mean ratings of ‘willingness to wait and see’ across the three decision situations are also significant (F (2, 3122) = 146.71, p < .001, partial η2 = .087) after statistically controlling for gender, age, education level, income level, health level and concern level of their own health. Respondents’ mean rating of ‘willingness to wait and see’ under the condition of ‘do not know whether COVID-19 vaccine has side effect or not’ (M = 63.26) was less than that under the condition of ‘know that COVID-19 vaccine has side effect’ (M = 46.19) but greater than that under the condition of ‘know that COVID-19 vaccine has no side effect’ (M = 67.36).
The results are as follows: (1) under condition of knowing that COVID-19 vaccine has no side effect, respondents’ mean ratings of ‘willingness to get vaccinated’ was the highest, whilst their mean ratings of ‘willingness to wait and see’ was the lowest; (2) under the condition of knowing that COVID-19 vaccine has side effect, respondents’ mean ratings of ‘willingness to get vaccinated’ was the lowest, whilst their mean ratings of ‘willingness to wait and see’ was the highest and (3) under the condition of not knowing whether COVID-19 vaccine has side effect or not, respondents’ mean ratings of ‘willingness to get vaccinated’ and their mean ratings of ‘willingness to wait and see’ fell between the mean ratings of the other two conditions. The resultant findings do not demonstrate a ‘disjunction effect’ that violates Savage’s sure-thing principle.Citation15–17
By contrast, the degree of vaccination acceptability was in a descending order of under condition of mentioning that COVID-19 vaccine is safe and effective (88.6% No. of respondents, Lazarus et al., 2021) > under condition of that the safety and efficiency of the vaccine is unknown (not provided) (75.4% No. of respondents) ≈ under condition of knowing COVID-19 vaccine has no side effect (75.89 mean rating) > under condition of not knowing whether that COVID-19 vaccine has side effect or not (57.68 mean rating) > under condition of knowing COVID-19 vaccine has side effect (48.07 mean rating).
3.2. Vaccine hesitancy
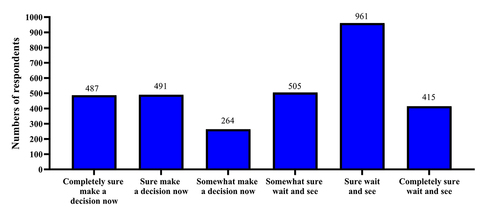
The frequency of evaluating results on a 6-point scale for Item 1 is shown in (Item 1: you will make a decision until when/under what circumstances). Note that the number of respondents who chose ‘wait and see’ (505 + 961 + 415 = 1881) was larger than those who chose ‘make a decision now’ (487 + 491 + 264 = 1242).
Figure 3. The frequency of evaluating results on a 6-point scale ranging from completely sure to make a decision now (1) to completely sure to make a decision after wait-and-see (6). Numbers above the bars represent the number of respondents in each scale who responded to the item ‘Please indicate when you think you can decide whether or not to get vaccinated.’
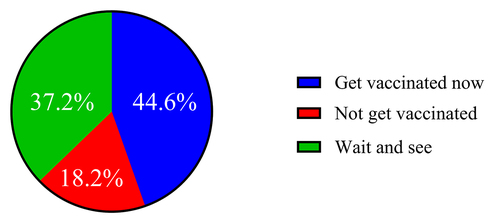
When respondents were asked to choose amongst ‘get vaccinated now,’ ‘not get vaccinated’ and ‘wait and see,’ we found that the percentage of respondents who chose ‘get vaccinated now,’ ‘not get vaccinated’ and ‘wait and see’ are 44.6%, 18.2% and 37.2%, respectively ().
Figure 4. Percentage of respondents who chose ‘get vaccinated now,’ ‘not get vaccinated’ or ‘wait and see.’
3.3. Reasons for hesitancy by querying
What respondents wrote for ‘you will make a decision until when/under what circumstances’ were recorded and counted by using word-frequency analysis. The results are shown in .
Figure 5. Analysis of the reasons why people chose not to be vaccinated and ‘wait and see.’
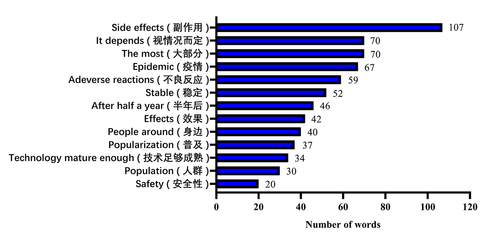
The results showed that for those who chose ‘wait and see,’ what they filled in the blank for ‘you will make a decision until when/under what circumstances’ is mainly on ‘side effect’ (under what circumstances) and ‘half a year’ (when). Vaccine safety is the primary consideration of those who chose the ‘wait and see’ option. That is, respondents would like to wait and see until the information they collected is moved from ‘uncertainty’ to ‘certainty’ before making a vaccination decision.
4. Discussion
Vaccination is a cost-effective strategy for reducing morbidity and mortality from numerous infectious diseases,Citation18 and countries currently have the tools to end these diseases based on the largest and most rapid global deployment of vaccines.Citation1 Different from the clinical development of the majority of the known epidemic vaccines, the clinical development of COVID-19 vaccine has the characteristic of ‘rushing to meet the challenge’ (i.e. rushing to meet the challenge when new variants emerge), and the safety and efficiency of the vaccine have yet to be confirmed.
The aforementioned uncertainty makes the worldwide ‘vaccine hesitancy’ considerably challenging. Vaccine hesitancy is defined as a ‘delay in acceptance or refusal of vaccination despite availability of vaccination services’ by the WHO Strategic Advisory Group of Experts on Immunization.Citation19 Therefore, identifying and addressing vaccine acceptance,Citation20 vaccine hesitance and resistanceCitation21 to a vaccine for COVID-19 is a potentially important step to ensure the rapid and requisite uptake of an eventual vaccine.Citation22
Notably, in China, the government’s policy plays an important role in the prevention and control of an epidemic, but vaccine hesitation is still prevalent. Although China provided free vaccines to residents who were divided into ‘necessary to be vaccinated’ and ‘unnecessary to be vaccinated’ groups, vaccination is voluntary rather than compulsory. China encourages voluntary COVID-19 vaccinations and works to ensure that all people eligible for vaccination have access to it.Citation23 Thus, when people are offered the opportunity to be vaccinated, ‘get vaccinated,’ ‘not get vaccinated’ and ‘wait and see’ are their real-life options.
Our survey revealed that the method of measuring attitude matters to the levels of willingness to take the COVID-19 vaccine. The resulting measures were relatively optimistic when measuring under the condition that vaccine is safe and effective. If considering additional realistic conditions (e.g. not mentioning that vaccine is safe and effective or, mentioning its side effect), then the resulting measures are not that optimistic. If measuring vaccine hesitancy was added, the levels of willingness to take the COVID-19 vaccine will turn out to be pessimistic. That is, less than half of the respondents will get vaccinated now. Overall, our findings suggested that current levels of willingness to take the COVID-19 vaccine in China are not optimistic to meet the requirements for community immunity.
Therefore, researchers should carefully select the measuring method to investigate the ‘true’ levels of willingness to take the COVID-19 vaccine. Moreover, the relevant departments should fully predict obstacles to achieve immunity coverage and prepare for the ‘vaccine hesitancy’ of the people in need. Thus, a targeted public health publicity can be carried out on this basis.
Our study has a significant number of limitations. The first limitation concerns the representativeness of the sample. We assumed that each respondent was independent and a representative sample from the general population. The second limitation is that, as part of a larger online survey, the respondents may not have devoted sufficient attention to the task. The third limitation is that it should be noted that all public surveys of the type reported here are snapshots taken at a point in time. This particular survey was conducted in the context of a highly dynamic and changing landscape, with daily variations in perceived disease threat and the COVID-19 vaccine development itself. As a cross-sectional study, this research was unable to assess the relationship between vaccine hesitancy and actual vaccination uptake, but plans to collect this information in future studies.
Disclosure of potential conflicts of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence this research.
Acknowledgments
The authors are grateful to Rao Li-Lin, Zheng Rui and Xu Ming-Xing for their contributions to the initial ideas behind this paper, and Kuang Yi and Huang Yuan-Na for their help in survey question design and data collation. All of their suggestions that have significantly improved this study.
Additional information
Funding
Notes
1 The three conditions described in Savage’s sure-thing principle (Savage, 1954). This principle states that if event E is known to occur, the decision maker will take action A. Knowing that event E will not occur, the decision maker will take action A. Accordingly, the decision maker will take action A without knowing whether event E will occur or not. That is, their preference of a over b is independent of their state of knowledge of x (see also Wang, Li, & Fang, 2011; Li, Jiang, Dunn, & Wang, 2012).
References
- Koff WC, Berkley SF. A universal coronavirus vaccine. Science. 2021;371(6531):759. PMID: 33602830. doi:10.1126/science.abh0447.
- Wagner AL, Huang Z, Ren J, Laffoon M, Ji M, Pinckney LC, Sun X, Prosser LA, Boulton ML, Zikmund-Fisher BJ. Vaccine hesitancy and concerns about vaccine safety and effectiveness in Shanghai, China. Am J Prev Med. 2021;60(1):S77–S86. PMID: 33189502. doi:10.1016/j.amepre.2020.09.003.
- Morton TA, Rabinovich A, Marshall D, Bretschneider P. The future that may (or may not) come: how framing changes responses to uncertainty in climate change communications. Global Environ Chang. 2011;21(1):103–09. doi:10.1016/j.gloenvcha.2010.09.013.
- Saito K. Preferences for flexibility and randomization under uncertainty. Am Econ Rev. 2015;105(3):1246–71. doi:10.1257/aer.20131030.
- Bhattacharyya S, Bauch CT. “Wait and see” vaccinating behaviour during a pandemic: a game theoretic analysis. Vaccine. 2011;29(33):5519–25. PMID: 21601606. doi:10.1016/j.vaccine.2011.05.028.
- Dubé E, Gagnon D, Nickels E, Jeram S, Schuster M. Mapping vaccine hesitancy - Country-specific characteristics of a global phenomenon. Vaccine. 2014;32(49):6649–54. PMID: 25280436. doi:10.1016/j.vaccine.2014.09.039.
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–28. PMID: 33082575. doi:10.1038/s41591-020-1124-9.
- Du XL, Liu SH, Xu JH, Rao LL, Jiang CM, Li S. When uncertainty meets life: the effect of animacy on probability expression. Judgm Decis Mak. 2013;8:425–38.
- Wang Y, Du XL, Rao LL, Li S. Probability expression for changeable and changeless uncertainties: an implicit test. Front Psychol. 2014;5:1313. PMID: 25431566. doi:10.3389/fpsyg.2014.01313.
- Tversky A, Kahneman D. The framing of decisions and the psychology of choice. Science. 1981;211(4481):453–58. PMID: 7455683. doi:10.1126/science.7455683.
- Shafir E. Choosing versus rejecting: why some options are both better and worse than others. Mem Cognit. 1993;21(4):546–56. PMID: 8350746. doi:10.3758/bf03197186.
- Johnson EJ, Goldstein D. Do defaults save lives? Science. 2003;302(5649):1338–39. PMID: 14631022. doi:10.1126/science.1091721.
- Li S, Li Y-X, Kuang Y, Hu Y-Q, Zheng R. RE: a third small box that can change the course of history; 2019 October 18 [accessed 2018 Oct 3]. https://science.sciencemag.org/content/re-third-small-box-can-change-course-historyExample .
- Wang Z-J, Li S, Fang Y. Re-examining reasons leading to violations of Savage’s sure-thing principle under uncertainty. J Psychol Sci. 2011;34(6):1463–68. In Chinese.
- Faul F, Erdfelder E, Lang AG, Buchner A. G* Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–91.
- Tversky A, Shafir E. The disjunction effect in choice under uncertainty. Psychol Sci. 1992;3(5):305–10. doi:10.1111/j.1467-9280.1992.tb00678.x.
- Li S, Jiang C-M, Dunn JC, Wang Z-J. A test of “reason-based” and “reluctance-to-think” accounts of the disjunction effect. Inform Sci. 2012;184(1):166–75. doi:10.1016/j.ins.2011.09.002.
- Maurer KA, Chen HF, Wagner AL, Hegde ST, Patel T, Boulton ML, Hutton DW. Cost-effectiveness analysis of pneumococcal vaccination for infants in China. Vaccine. 2016;34(50):6343–49. PMID: 27810315. doi:10.1016/j.vaccine.2016.10.051.
- MacDonald NE; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–64. PMID: 25896383. doi:10.1016/j.vaccine.2015.04.036.
- Habersaat KB, Jackson C. Understanding vaccine acceptance and demand—and ways to increase them. Bundesgesundheitsblatt-Gesundheitsforschung-Gesundheitsschutz. 2020;63:32–39. PMID: 31802154. doi:10.1007/s00103-019-03063-0.
- Larson HJ, Jarrett C, Eckersberger E, Smith DM, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. 2014;32(19):2150–59. PMID: 24598724. doi:10.1016/j.vaccine.2014.01.081.
- Murphy J, Vallières F, Bentall RP, Shevlin M, McBride O, Hartman TK, Hyland P, Bennett K, Mason L, Gibson-Miller J. Psychological characteristics associated with COVID-19 vaccine hesitancy and resistance in Ireland and the United Kingdom. Nat Commun. 2021;12(1):1–15. PMID: 33397962. doi:10.1038/s41467-020-20226-9.
- Xinhua, China encourages voluntary COVID-19 vaccination: official, Chinadaily, 2021 Apr 12 [accessed 2021 June 28]. https://www.chinadaily.com.cn/a/202104/12/WS6073a294a31024ad0bab4ce6.html .