
ABSTRACT
Rotavirus gastroenteritis (RVGE) poses a substantial clinical, economic, and humanistic burden globally. While predominantly affecting children, the burden of RVGE extends to caregivers and families but is often overlooked. In this systematic literature review, we aim to identify and summarize methods and estimates of RVGE associated caregiver burden. Of the 190 publications identified, 10 were included. Four studies used the EuroQoL-5 Dimension instrument and its associated Visual Analog Scale and reported a decrease in caregiver health related quality of life when a child contracted RVGE, with the greatest reduction observed in caregivers of hospitalized children. Other studies utilized surveys to assess impacts on caregivers’ quality of life. Caregivers of RVGE patients experienced multiple impacts beyond financial costs related to productivity and absenteeism, with disruptions to daily routines and anxiety/stress frequently reported. This review highlights the importance of including RVGE caregiver burden when evaluating interventions, such as vaccination, to decrease RVGE burden.
Introduction
Rotavirus gastroenteritis (RVGE) is highly contagious and is characterized by severe to mild vomiting, watery diarrhea, and dehydration, which, in severe cases, can lead to hospitalization and death.Citation1,Citation2 Prior to the introduction of vaccination, most children in the United States would have been infected with rotavirus by the age of five, resulting in substantial clinical and economic burden.Citation1,Citation3 In the United States, total RVGE associated medical and productivity costs were estimated to be close to 1 billion USD annually before the introduction of vaccination.Citation1,Citation4 A study in Israel found that caregivers incurred significant out-of-pocket non-medical expenses due to pediatric RVGE hospitalizations, with $1.1 million (2008 USD) spent on extra diapers, over-the-counter medications, and special dietary requirements.Citation2 Another study conducted in the United Kingdom reported that parents lost up to 7.5 workdays per child’s episode of RVGE treated in a primary-care setting, and incurred non-medical out-of-pocket expenses of up to $1,061 (2009 USD) per episode if their child was hospitalized.Citation5
In addition to financial burden, infectious diseases, such as RVGE, affect not only the quality of life of patients, but also the quality of life of caregivers and other individuals close to the infant, so called “spillover effects”. Spillover effects are defined as the impact of illness on the quality of life of individuals other than the infected child who may experience disruption and detriment to their routine and well-being due to the disease.Citation6,Citation7 A comprehensive literature review conducted by Lavelle et al., recommended the consideration of spillover effects in economic analyses of interventions, to ensure that the burden of childhood illnesses is not undervalued and to support accurate decision-making for public health policies.Citation8 However, spillover effects, and specifically the effects of pediatric diseases on caregivers’ quality of life are not well quantified nor consistently included in economic and cost-effectiveness analyses.Citation7 Spillover effects are particularly important to consider when discussing a pediatric disease such as RVGE, where caregivers and family members play a vital role in the patient’s treatment and recovery.
We sought to identify and summarize methods and estimates of RVGE associated caregiver burden via a comprehensive systematic literature review. The findings of this literature review will be important for modelers, infectious disease experts, and public health policy makers interested in ascertaining the humanistic burden of RVGE and incorporating these estimates into cost-effectiveness analyses of preventive RVGE strategies such as vaccination.
Methods
We conducted a systematic literature review on caregiver burden of RVGE in PubMed and Scopus in June 2020. A combination of medical subject headings (MESH) and free-text search terms were employed, including terms related to rotavirus, caregivers and family, and burden (). We included terms encompassing both broad and specific burden outcomes of interest to ensure all relevant publications were captured. Limits for English language publications and “humans” were applied to the search; no limit on publication date was applied.
Table 1. Search terms for Scopus and PubMed
Publications were screened for eligibility using predefined inclusion and exclusion criteria (). Publications that reported outcomes related to the subjective experience of caregivers, specifically descriptions on emotional, health-related, stress or descriptions of caregiver experience with RVGE, were included. Publications focused solely on financial burden or costs were not included. The study design of retrieved publications was reviewed to include only studies that estimated or conveyed the impact of RVGE on caregivers via interviews, administration of surveys or instruments.
Table 2. PICOS criteria
Results
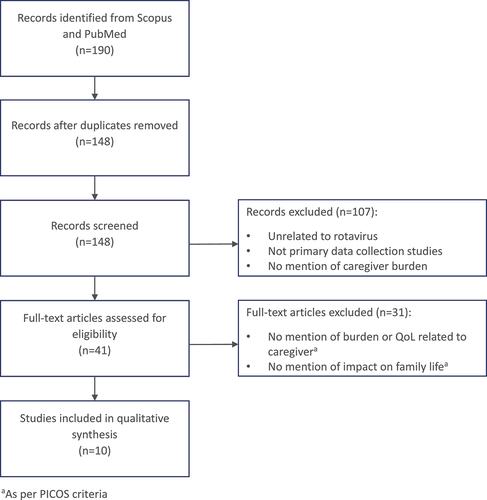
A total of 190 relevant publications were identified by the search, totaling 148 after duplicate removal. These were screened based on the inclusion criteria included in . At full-text review, 41 publications were further screened for mention of caregiver burden or impact on family life, leaving 10 studies that reported on the caregiver burden of RVGE to be included in qualitative synthesis ().
Figure 1. PRISMA of included studies related to caregiver burden.
Study characteristics
Studies identified in the review presented data from countries in Europe, North America and Southeast Asia (). Participants were enrolled from hospital wards, general physician clinics, outpatient clinics, primary-care facilities, and emergency and pediatric hospital departments, with studies ranging in duration from 2 to 33 months. The instruments most frequently used to quantify caregiver burden were the EuroQoL-5 Dimension (EQ-5D) and its associated Visual Analogue Scale (VAS), which were utilized in four observational studies conducted in Thailand, the United Kingdom, Denmark, and Canada.Citation9–12 Other studies used questionnaires, interviews, and diaries to track symptoms and potential RVGE transmission, as well as emotional distress and financial impact on caregivers. Laizane et al., for example, conducted caregiver questionnaires to assess the emotional well-being, economic and social burden of RVGE, while Diez-Domingo et al., O’Brien et al. and Mast et al. used in-depth interviews to assess caregiver burden and quantify parental emotions.Citation13–15
Table 3. Design of included studies that quantify caregiver burden (n = 10).Citation9–18
Impact of rotavirus on caregivers
The studies identified in the qualitative synthesis consistently found that RVGE caused disruption to the lives of caregivers, resulting in parental distress and significant economic and emotional burden. A total of four studies used the EQ-5D and its associated VAS to report caregiver health related quality of life.Citation9–12,Citation16 One study did not report results at baseline for either instrument; therefore health related caregiver quality of life could not be compared during and after the RVGE episode.Citation11 For the remaining three studies, caregiver health related quality of life at the time of RVGE episode decreased compared to baseline, where health related quality of life at baseline was characterized by a response to the same instrument after the RVGE episode had resolved ().
Figure 2. Caregiver utility for caring for rotavirus gastroenteritis patients, as captured with the EQ-5D.Citation9–12
Decreases in health related quality of life seemed to be associated with disease severity (). The greatest decrease in caregiver utility value was reported by Rochanathimoke et al. in Thailand, for caregivers of children hospitalized with RVGE between May 2013 and February 2014 (EQ-5D caregiver health related quality of life reduction from .96 to .61).Citation9 Brisson et al. showed the smallest decrease (.95 baseline to .88 at time of RVGE episode), for caregivers of patients visiting outpatient clinics in Canada from January to June 2005.Citation12
Brisson et al. and Rochanathimoke et al. also reported results by EQ-5D health dimention. The EQ-5D-5 L dimensions most affected were usual activities, pain/discomfort, and anxiety/depression.Citation9,Citation12 In particular, Rochanathimoke et al. found that 96.4% of caregivers of hospitalized patients reported some problem or a severe problem with anxiety/depression.Citation9 Brisson et al. found similar effects by health dimension, albeit with a less severe impact on caregivers in the outpatient settings. Anxiety/depression was reported as a problem by 26% of caregivers in outpatient clinics.Citation12
Similarly, across the three studies where the EQ-5D VAS scores versus baseline were reported, caregiver VAS scores decreased at the time of RVGE episode compared to baseline (). As with EQ-5D, caregivers of hospitalized patients stated the greatest decrease in VAS score followed by those in hospital emergency departments, with caregivers of patients in outpatient clinics reporting the smallest decrease. This is shown through the decrease in VAS caregiver score from a baseline of .97 to .63 in Thai hospitalized patients reported by Rochanathimoke et al., compared to a decrease of 9.9% in caregivers of patients in Canadian outpatient clinics reported by Brisson et al.Citation9,Citation12,Citation18
Figure 3. EQ-5D associated VAS caregiver score for caring for rotavirus gastroenteritis patients.Citation9–12
Although six of the studies identified did not utilize the EQ-5D and its associated VAS, alternative approaches demonstrated caregiver burden was related to high levels of stress, fear, and anxiety for the child with RVGE.Citation13–18 Investigators developed unique questionnaires and carried out interviews and focus groups, consistently identifying that RVGE caused disruption to the lives of caregivers, resulting in parental distress and significant economic and emotional burden.
Van der Wielen reported mean parental stress levels of greater than 5 on a 10-point visual analogue scale.Citation16 Higher levels of anxiety and parental distress were also reported in hospital settings, with parents particularly concerned by the severity of symptoms and the effect these had on their child.Citation9,Citation10,Citation13,Citation15,Citation17,Citation19 Laizane et al. reported that in a sample of children hospitalized with RVGE, parents were negatively affected; of note, their emotional (feelings of distress, exhaustion and helplessness), social (disruption of schedules and restrictions on daily life), and economic (lost working days and increased expenditure on nappies) burden was affected, regardless of the severity of the health status of their child.Citation13 Parents in Vietnam had little knowledge of RVGE, and so were particularly worried about preventing the disease in the future.Citation15
In addition to the emotional burden of RVGE on caregivers, studies identified through this literature review also reported other impacts of disease. Laizane et al. found 75.2% of caregivers incurred extra expenditures related to their child having RVGE such as drugs to combat symptoms and diapers. Additionally 79% of parents changed their daily routine due to the illness.Citation13
The impact of rotavirus on productivity loss was also noted. Mast et al. found that parents in the United States often missed several days of work to care for their child, but the economic impact of this was minimal for many families as it was covered by their employer’s absence policies.Citation17 Hoffman et al. found that work days lost ranged from two in France for hospitalized patients, to seven in the UK for patients receiving primary-care.Citation11 The possible effect of household transmission on productivity was also suggested in additional analyses. Daily symptom diaries were completed by participants in a study lead by Marlow et al. and showed that at least one other member of the household developed a secondary case of gastroenteritis in 52% of cases. This caused 69% of these caregivers to miss a mean 2.8 (95% CI 2.3–3.4) days of work.Citation10
Discussion
We found that RVGE impacted caregiver health related quality of life. Results were obtained for different countries and spanned different continents, including North America (United States and Canada), Asia-Pacific (Thailand, Vietnam, Taiwan), and Europe (United Kingdom, Denmark, Italy). The studies utilized different techniques to assess caregiver burden, including qualitative surveys, stress scales, and specific interview guides. Across all the studies, the most frequently used instruments to assess caregiver burden were the EQ-5D and its associated VAS. Caregivers of hospitalized children reported the greatest decrease in quality of life, as measured by the EQ-5D.
Spillover effects of pediatric infectious diseases have previously been reviewed. Wittenberg et al. reviewed studies measuring caregiver utilities for pediatric infectious diseases. The review showed that caregivers of children with RVGE experienced a similar level of burden to that experienced by caregivers of children with other pediatric diseases such as meningitis. Wittenberg et al. also concluded that the most severe RVGE cases where a child required hospitalization had a more significant effect on caregivers’ reduction in health related quality of life.Citation7
The EQ-5D was used in four out of ten studies identified by this review. The EQ-5D is a standartized instrument and is available in multiple countries and languages.Citation20 As a generic utility measure, the EQ-5D can be used across diseases to quantify health-related quality of life and generate quality-adjusted life years (QALYs) over five dimensions including mobility, self-care, usual activities, pain/discomfort and anxiety/depression.Citation8 Previously, researchers have used the EQ-5D to evaluate caregiver burden for conditions such as Alzheimer’s disease and Duchenne muscular dystrophy. This and other studies have demonstrated the EQ-5D is an effective technique to assess caregiver burden as it provides qualitative data that can be easily interpreted and presented consistently across studies within a country.Citation7,Citation21 An additional advantage of the EQ-5D is that it allows for calculating the disutility associated with caregiver burden and for combining it with infant health utility in cost-utility analyses.Citation7
From the studies identified, only Brisson et al. and Rochanathimoke et al. reported EQ-5D results by health dimension, with greater impact on usual activities, pain/discomfort, and anxiety/depression in caregivers of children with RVGE.Citation9,Citation12 Additionally, analysis of the utility decrements identified by the literature review suggest that caring for children who needed emergency care or hospitalization had the greatest impact on caregiver quality of life. In particular, the decrease in caregiver EQ-5D utility was −.35 when caring for a hospitalized infant, which was greater than the average change in EQ-5D utility for patients suffering from mixed anxiety depressive disorder (−.13).Citation9,Citation22 However, utility estimates are country specific and comparison across all studies is limited by differences in geography. Therefore, health economic models created and assessments made are only valid in the country of data collection. Moreover, EQ-5D may not adequately capture all important dimensions that are relevant to the caregiver, such as impoverishment or household transmission. Additional questionnaires may be required to capture these aspects. Therefore, along with generic utility measures such as EQ-5D, additional survey questions directed toward quality of life impacts on caregivers should also be included as part of a standard patient assessment to further understand the burden of RVGE on caregivers.
In addition to the emotional impact of caring for a child with RVGE, caregivers may also need to care for other family members due to rotavirus transmission within a household. In the United States, 16% of pediatric rotavirus-positive cases were followed by a member of the same household developing gastroenteritis symptoms. More than half of these individuals were aged 18 or over, who may incur costs in the form of additional medical expenses and lost productivity, thus adding to the overall burden on caregivers of children with RVGE.Citation23,Citation24 The same was reported in Ecuador, in a study quantifying RVGE household transmission. Fifty-five percent of household contacts became infected with rotavirus, with transmission particularly high when vomiting occurred in children less than 18 months of age who shared a room with another child of less than 10 years old.Citation25 Household transmission was discussed in several of the identified studies, again reinforcing the additional burden of caring for, and sharing a household with, RVGE patients.Citation10,Citation11,Citation15,Citation17
Our study has some limitations. First, only four studies identified within the review measured caregiver burden with a comparable instrument (EQ-5D and VAS), whereas other studies used surveys or questionnaires. The limited number of studies available which used the same methods makes it difficult to analyze burden across different settings and between different countries.
Secondly, most frequently, the analyses did not consider multiple family members, with some studies instead focusing on the primary caregiver which was most frequently the mother.Citation10,Citation15 However, an episode of illness has been shown to impact multiple caregivers.Citation6 Future analyses could consider reporting RVGE burden on multiple caregivers to better inform economic evaluations of interventions.Citation6,Citation8
Finally, the specific search term of ‘stress’ was used within the systematic literature search strategy to target this particular element of emotional burden. The use of such a specific term may have eliminated publications utilizing broader emotional burden terms. However, the broad search terms of ‘impact’ and ‘burden’ were also used to capture as many relevant publications as possible.
We were also unable to find references discussing stress/anxiety related to impoverishment due to RVGE medical costs or the additional financial impact that household transmission may have had on caregivers’ due to their own illness. RVGE imposes significant financial burden to families, associated with non-medical costs (e.g. extra diapers, transport costs, additional childcare or prescribed formula), as well as the disparities in direct medical expenses depending on public or private insurance coverage of these costs.Citation15–17 In Malaysia, in a study beyond the scope of this literature review, the financial burden of RVGE hospitalization differed between wealthier urban areas and poorer rural areas. Costs associated with RVGE hospitalization were significantly higher in urban areas, and this resulted in 6% of study participants in these areas being pushed into poverty.Citation26
We provided an overview of estimates and methods that captured caregiver burden of RVGE pediatric patients. Caregivers of RVGE patients experienced multiple impacts from this contagious infectious disease. The health related quality of life of caregivers decreased during the RVGE episode, with standard quality of life instruments suggesting that the reduction was driven by impacts on mobility and anxiety/depression. Future studies may consider burden across multiple family members, and diverse family impacts from RVGE. Economic evaluations of RVGE prevention strategies should consider the quality of life impact of RVGE on caregivers for a comprehensive value assessment.
Acknowledgements
The authors would like to thank Adelphi Values PROVE for providing medical writing support.
Disclosure statement
Cristina Carias, Tianyan Hu and Ya-Ting Chen are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA and hold stocks of Merck & Co., Inc., Kenilworth, NJ, USA.
Additional information
Funding
References
- Pindyck T, Tate JE, Parashar UD. A decade of experience with rotavirus vaccination in the United States - vaccine uptake, effectiveness, and impact. Expert Rev Vaccines. 2018;17(7):593–7. doi:10.1080/14760584.2018.1489724.
- Khoury H, Ogilvie I, El Khoury AC, Duan Y, Goetghebeur MM. Burden of rotavirus gastroenteritis in the Middle Eastern and North African pediatric population. BMC Infect Dis. 2011;11(1):9. doi:10.1186/1471-2334-11-9.
- Glass RI, Kilgore PE, Holman RC, Jin S, Smith JC, Woods PA, Clarke MJ, Ho MS, Gentsch JR. The epidemiology of rotavirus diarrhea in the United States: surveillance and estimates of disease burden. J Infect Dis. 1996;174 Suppl 1:S5–11. doi:10.1093/infdis/174.Supplement_1.S5.
- Tucker AW, Haddix AC, Bresee JS, Holman RC, Parashar UD, Glass RI. Cost-Effectiveness analysis of a rotavirus immunization program for the United States. Jama. 1998;279(17):1371–76. doi:10.1001/jama.279.17.1371.
- Ogilvie I, Khoury H, Goetghebeur MM, El Khoury AC, Giaquinto C. Burden of community-acquired and nosocomial rotavirus gastroenteritis in the pediatric population of Western Europe: a scoping review. BMC Infect Dis. 2012;12(1):62. doi:10.1186/1471-2334-12-62.
- Al-Janabi H, van Exel J, Brouwer W, Coast J. A framework for including family health spillovers in economic evaluation. Med Decis Making. 2016;36(2):176–86. doi:10.1177/0272989X15605094.
- Wittenberg E, James LP, Prosser LA. Spillover effects on Caregivers’ and family members’ utility: a systematic review of the literature. Pharmacoeconomics. 2019;37(4):475–99. doi:10.1007/s40273-019-00768-7.
- Lavelle TA, D’-Cruz BN, Mohit B, Ungar WJ, Prosser LA, Tsiplova K, Vera-Llonch M, Lin P-J. Family spillover effects in pediatric cost-utility analyses. Appl Health Econ Health Policy. 2019;17(2):163–74. doi:10.1007/s40258-018-0436-0.
- Rochanathimoke O, Riewpaiboon A, Postma MJ, Thinyounyong W, Thavorncharoensap M. Health related quality of life impact from rotavirus diarrhea on children and their family caregivers in Thailand. Expert Rev Pharmacoecon Outcomes Res. 2018;18(2):215–22. doi:10.1080/14737167.2018.1386561.
- Marlow R, Finn A, Trotter C. Quality of life impacts from rotavirus gastroenteritis on children and their families in the UK. Vaccine. 2015;33(39):5212–16. doi:10.1016/j.vaccine.2015.07.012.
- Hoffmann T, Iturriza M, Faaborg-Andersen J, Kraaer C, Nielsen CP, Gray J, Hogh B. Prospective study of the burden of rotavirus gastroenteritis in Danish children and their families. Eur J Pediatr. 2011;170(12):1535–39. doi:10.1007/s00431-011-1465-y.
- Brisson M, Sénécal M, Drolet M, Mansi JA. Health-Related quality of life lost to rotavirus-associated gastroenteritis in children and their parents: a Canadian prospective study. Pediatr Infect Dis J. 2010;29(1):73–75. doi:10.1097/INF.0b013e3181b41506.
- Laizane G, Kivite A, Stars I, Cikovska M, Grope I, Gardovska D. Health-Related quality of life of the parents of children hospitalized due to acute rotavirus infection: a cross-sectional study in Latvia. BMC Pediatr. 2018;18(1):114. doi:10.1186/s12887-018-1086-y.
- Diez Domingo J, Patrzalek M, Cantarutti L, Arnould B, Meunier J, Soriano-Gabarro M, Meyer N, PirçPirçOn J-Y, Holl K. The impact of childhood acute rotavirus gastroenteritis on the parents’ quality of life: prospective observational study in European primary care medical practices. BMC Pediatr. 2012;12(1):58. doi:10.1186/1471-2431-12-58.
- O’-Brien MA, Rojas-Farreras S, Lee HC, Lin LH, Lin CC, Hoang PL, Pedros M, Lara N. Family impact of rotavirus gastroenteritis in Taiwan and Vietnam: an ethnographic study. BMC Infect Dis. 2015;15:240. doi:10.1186/s12879-015-0968-y.
- Van der Wielen M, Giaquinto C, Gothefors L, Huelsse C, Huet F, Littmann M, et al. Impact of community-acquired paediatric rotavirus gastroenteritis on family life: data from the REVEAL study. BMC Fam Pract. 2010;11(1):22. doi:10.1186/1471-2296-11-22.
- Mast TC, DeMuro-Mercon C, Kelly CM, Floyd LE, Walter EB. The impact of rotavirus gastroenteritis on the family. BMC Pediatr. 2009;9(1):11. doi:10.1186/1471-2431-9-11.
- Marchetti F, Vetter V, Conforti G, Esposito S, Bonanni P. Parents’ insights after pediatric hospitalization due to rotavirus gastroenteritis in Italy. Hum Vaccin Immunother. 2017;13(9):2155–59. doi:10.1080/21645515.2017.1336271.
- Van Damme P, Van der Wielen M, Ansaldi F, Desgrandchamps D, Domingo JD, Sanchez FG, Gray J, Haditsch M, Johansen K, Lorgelly P, et al. Rotavirus vaccines: considerations for successful implementation in Europe. Lancet Infect Dis. 2006;6(12):805–12. doi:10.1016/S1473-3099(06)70657-0.
- Gerlinger C, Bamber L, Leverkus F, Schwenke C, Haberland C, Schmidt G, et al. Comparing the EQ-5D-5L utility index based on value sets of different countries: impact on the interpretation of clinical study results. BMC Res Notes. 2019;12(1):18. doi:10.1186/s13104-019-4067-9.
- Prosser LA, Wittenberg E. Advances in methods and novel applications for measuring family spillover effects of illness. PharmacoEconomics. 2019;37(4):447–50. doi:10.1007/s40273-019-00794-5.
- Roberts J, Lenton P, Keetharuth AD, Brazier J. Quality of life impact of mental health conditions in England: results from the adult psychiatric morbidity surveys. Health Qual Life Outcomes. 2014;12(1):6. doi:10.1186/1477-7525-12-6.
- Wikswo ME, Parashar UD, Lopman B, Selvarangan R, Harrison CJ, Azimi PH, Boom JA, Sahni LC, Englund JA, Klein EJ, et al. Evidence for household transmission of rotavirus in the United States, 2011–2016. J Pediatric Infect Dis Soc. 2020;9(2):181–87. doi:10.1093/jpids/piz004.
- Quee FA, de Hoog MLA, Schuurman R, Bruijning-Verhagen P, de Hoog MLA. Community burden and transmission of acute gastroenteritis caused by norovirus and rotavirus in the Netherlands (RotaFam): a prospective household-based cohort study. Lancet Infect Dis. 2020;20(5):598–606. doi:10.1016/S1473-3099(20)30058-X.
- Lopman B, VicuñVicuñA Y, Salazar F, Broncano N, Esona MD, Sandoval C, Gregoricus N, Bowen MD, Payne D, Vaca M, et al. Household transmission of rotavirus in a community with rotavirus vaccination in Quininde, Ecuador. PLoS One. 2013;8(7):e67763. doi:10.1371/journal.pone.0067763.
- Loganathan T, Lee WS, Lee KF, Jit M, Ng CW, Wang Y. Household catastrophic healthcare expenditure and impoverishment due to rotavirus gastroenteritis requiring hospitalization in Malaysia. PLoS One. 2015;10(5):e0125878. doi:10.1371/journal.pone.0125878.