
ABSTRACT
Vaccine hesitancy is one of the top ten global health threats and the first threat to fighting COVID-19 through vaccination. With the increasing level of COVID-19 vaccine hesitancy amidst the rising level of confirmed cases and death tolls, this paper provides rapid systematic literature reviews on the measurement of COVID-19 vaccine hesitancy, key determinants and evidence-based strategies to prevent COVID-19 vaccine hesitancy. The findings reveal three standard measures of vaccine hesitancy: optional response questions, Likert scale, and linear scale measurements. Factors such as sociodemographic/economic factors, occupational factors, knowledge on the vaccine, vaccine attributes, conspiracy belief and psychological factors are the major predictors of COVID-19 vaccine hesitancy. Evidence-based findings identified measures such as effective education on the vaccine, clear and consistent communication to build public confidence and trust, health education on vaccination and its social benefit, outreach program and targeted messaging to minimize COVID-19 vaccine hesitancy.
1. Introduction
Following the outbreak of Coronavirus disease (COVID-19), an infectious disease caused by the SARS-CoV-2 which has affected over 100 millions people, claimed 2 million lives globally, collapsed businesses and economy,Citation1–4 bold steps and actions by governments and entities resulted in production of COVID-19 vaccines as ultimate intervention against the deadly virus. The purpose of this milestone achievement in the production of COVID-19 vaccines is to make these vaccines accessible or distributed across every country especially where cases of COVID-19 infections were confirmed. The effectiveness of any vaccination effort is contingent on the percentage of the population that is willing to be vaccinated, and according to current projections, it is possible that up to three-quarters of the population will need immunization in order to put the pandemic to a close.Citation5–7 Empirical and anecdotal evidence from global and country levels studies, however, show an increasing level of hesitancy of COVID-19 vaccine ranging from 20 to 80% and declining level of vaccine acceptance ranges from about 7 to 50% and this raises an important challenge to public health.
Vaccine hesitancy is defined by the World Health Organization (WHO) Strategic Advisory Group of Experts on Immunization as a “delay in acceptance or refusal of vaccination despite availability of vaccination services,”Citation8–12 which may take on different forms and intensities depending on when and where it happens, as well as the vaccine that is involved.Citation13 WHOCitation10 has highlighted vaccine hesitancy as one of the top ten global health problems for 2019; in fact, it was named as one of the top ten global health hazards in 2018. Anti-vaccine sentiment and disinformation are major hurdles to increasing vaccination coverage and community immunity in many countries.Citation7,Citation14 According to models with a vaccine efficacy of 80%, the percentage of the population that needs to be vaccinated to reach herd immunity ranges from 75 to 90% (depending on factors such as the basic reproduction number, vaccine-induced immunity duration, and whether vaccines prevent transmission).Citation15 A considerable proportion of the world’s population report that they are hesitant to get vaccinated, and although vaccine hesitancy varies from country to country, it remains alarmingly high in many areas. As a consequence, and despite recent advances in certain countries, the rates of vaccination intention continue to be below the proportion necessary for herd immunity in the majority of nations, and rates of vaccination intention are declining and this has received a global attention in research and policy direction.
While a plethora of studies exist on COVID-19 vaccine hesitancy, there is a scanty of systematic review in the literature on COVID-19 vaccine hesitancy. For instanceCitation5 review compared trends and synthesized findings in vaccination receptivity over time across US and international polls. Robinson et al.Citation6 review analyzed trends and consolidated data in vaccine receptivity over time across surveys conducted in the United States and elsewhere. The goal of theCitation6 study was to estimate the percentage of the global population wanting to get vaccinated versus the proportion of the global population planning to reject a vaccination when COVID-19 vaccines become available and how this tendency has evolved over time, using large and nationally representative samples. One key interest to policymakers is the evidence-based findings on how to minimize COVID-19 vaccine hesitancy, that is hesitancy corrective measure (to maximize public patronage) yet this has not been systematically reviewed in the extant literature. Additionally, there is a need to go beyond trend analysis and demographic predictors to emerging and updated findings on other characteristics that predict vaccine hesitancy and measurement. Consequently, there is an urgent need for a more updated and nuanced understanding of factors determining vaccine hesitancy and corrective measures in the context of the COVID-19 pandemic. This systematic review therefore seeks to address the following research questions: What is the standard measurement of hesitancy of COVID-19 vaccine in the literature? What are the predictors (up to date) of hesitancy of COVID-19 vaccine? What are the evidence-based measures in the literature to prevent vaccine hesitancy and promote public patronage of COVID-19 vaccine? Addressing these critical questions will not only contribute to the field of research but also help policymakers, healthcare workers, and other authorities to plan ahead toward minimizing the impact on public health from vaccine hesitancy by improving the global vaccination program. As the first step, we conducted a systematic review of all the studies related to hesitancy of COVID-19 vaccine. The aim of this review is to identify the measurement of hesitancy, key emerging predictors and hesitancy corrective measures that promote public patronage of COVID-19 vaccine.
Following this introduction and background section, is Section 2 that highlights the method used for the review. Section 3 presents the results while Sections 4 and 5, respectively, document the discussions of the results and conclusions based on the findings.
2. Method
This section covers study selection strategy, study design, eligibility, inclusive and exclusive criteria, and quality of assessment and synthesis.
2.1 Study selection strategy
Peer-reviewed studies were selected (from 2020 to 2021) for systematic reviews according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to ensure reproducibility and transparency of our findings. The selection of literature is informed by the key research questions; What is the standard measurement of hesitancy of COVID-19 vaccine in the literature? What are the predictors (up to date) of hesitancy of COVID-19 vaccine? What corrective measures are available to minimize vaccine hesitancy to promote public patronage of COVID-19 vaccine? To do this, a comprehensive literature (from the year 2020 to 2021) was conducted from the following electronic databases: MEDLINE (via LitCOVID in PubMed), Google scholar, Cochrane Library, African Index Medicus, and EBSCOhost. Primary concepts such as “vaccine hesitancy,” “COVID-19 vaccine hesitancy,” “willingness to be vaccinated,” “acceptance of COVID-19 vaccine,” “receptivity for COVID-19 vaccine,” “confidence in COVID-19 vaccine,” “trust in COVID-19 vaccine,” “measurement of vaccine hesitancy,” “predictors of vaccine hesitancy,” “factors associated with vaccine hesitancy,” and “promoting public vaccination” were used for the search. The subject and text word search were performed separately in all the databases and then combined with Boolean operators “OR” and “AND.” For a more thorough search, reference lists of pertinent publications and associated documents from databases by the World Health Organization (WHO) and the African Centers for Disease Control and Prevention (Africa CDC) were also checked for possibly relevant articles. To assess eligibility, two researchers reviewed the titles and abstracts of the search results before doing full-text reviews. Any differences were handled by reaching an agreement among the two researchers. When a possible survey was mentioned in an article, the author searched the original press release or official report to verify the information. To be eligible for inclusion, publications at minimum had to report on the measurement of COVID-19 vaccine hesitancy, predictors, or factors associated with COVID-19 vaccine hesitancy and empirical measures to minimize vaccine hesitancy and promote public vaccination. Details of eligibility criteria, quality assessment, and synthesis are provided in the following sections.
2.2 Study design eligible inclusion and exclusion criteria
To be eligible, studies were required to include questions that measure hesitancy/intentions/willingness to use a vaccine for COVID-19 when one becomes available (e.g. ‘I would use a vaccine for COVID-19 when it becomes available’), predict hesitancy of COVID-19 vaccine, and evidence-based findings on minimizing vaccination hesitancy and promoting public vaccination. For the purposes of this review, only research written in the English language that satisfied the inclusion criteria were taken into consideration. Other criteria for inclusion were peer-reviewed scientific publications published in peer-reviewed journals; survey studies of the general public, health-care professionals, students, or parents/guardians; and studies of the general public, health-care workers, students, or parents/guardians. The exclusion criteria were: (1) unpublished manuscripts (preprints); (2) the article did not aim to measure, predict and minimize COVID-19 hesitancy/ acceptance/hesitancy; and (3) publication language was not English.
2.3 Quality of assessment
The quality assessment of the studies as stipulated in the PRISMA-P statement in relation to the screening process was performed. The protocol of the screening process involved looking into the research aim of each study and if it answered any of the research questions of this study. Secondly, the quality assessment also focused on the measurement of hesitancy, predictors/factors, and evidence-based findings on minimizing COVID-19 vaccine hesitancy (that is promoting public vaccination). Furthermore, to facilitate a rapid review and address limitations posed by the observational nature of surveys, study quality was assessed by survey administration, sample size, nature of study, study design, and the research questions sought to address. Finally, the sample size of these studies was reduced as some studies failed to meet this quality assessment procedure. Following the inclusion and exclusion criteria, two reviewers worked together to independently evaluate the titles and abstracts for appropriateness. These two reviewers assessed the possibility of bias and extracted data; discrepancies were resolved via discussion. The other 350 papers were subjected to full-text screening using the same criteria. It was necessary to repeat the individual screening procedure in order to verify for consistency, and no discrepancies were discovered. A quality score out of ten was assigned using the Critical Appraisal Skills Programme.Citation16
2.4 Synthesis
A range of techniques were employed to form the synthesis of the evidence, based on the recommendation by.Citation17 Findings were synthesized narratively and provide thematic classification according to the objective of the review, tabulate the summarized results, and explore relationships with discussions. For the sake of maintaining consistency with primary-order outcomes and avoiding duplication of the authors’ interpretations, only data from the findings and results section were used. The remaining 25 papers were reviewed by both reviewers, who each made unique notes on the major significant topics. Inductive categorization was used throughout the screening process, therefore there were no disagreements.
3. Results
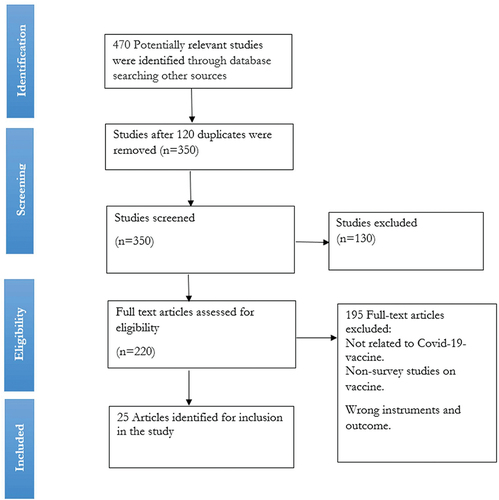
In this rapid systematic review, a sample of 25 studies were used and the geographical precinct of these studies is not restricted to a particular area, but rather there are studies from Saudi Arabia, USA, France, UK, Israel, Italy, Canada, Nigeria, China, and few global studies. The search and selection criteria included peer-reviewed publications, which were identified using the search criteria terms as described above. During the search, 470 potential studies were identified, 130 titles and abstracts were excluded as nonscientific. 340 papers were retrieved which reduced to 220 after removing duplicates and ultimately, 18 papers were left after thorough assessment of the papers using the inclusion and exclusion criteria. This process is fully illustrated in on PRIMA flow diagram.
Figure 1. Prisma flow diagram of study search and selection.
3.1 Study characteristics
3.1.1 Location
The empirical studies on the COVID-19 hesitancy literature cover different locations/countries often associated with different socio-cultural backgrounds and characteristics. Three studies focused on global contextCitation5,Citation9,Citation18 others were on specific countries from the developed countries such as USA, where about nine studies were conducted,Citation8,Citation19–26 Saudi Arabia,Citation27 France,Citation28 UK,Citation29 Israel,Citation30 Italy,Citation31,Citation32 Canada,Citation33 Nigeria,Citation34 and China.Citation35,Citation36
3.1.2 Aims of the studies
The review is based on carefully selected studies that focus on the research questions in this study. It includes studies that aim in understanding the correlates of COVID-19 vaccine hesitancy and the reasons why individuals intend to refuse to a COVID-19 vaccine,Citation8,Citation19 prevalence of the acceptance of COVID-19 vaccine and their determinants,Citation27 the frequency and variables associated with COVID-19 vaccineCitation20 and understand COVID-19 vaccine hesitancy in an ethnically diverse and deprived population.Citation29 Other studies sought to study vaccine attitudes and the variables that influence vaccine intent in the context of the COVID-19 pandemic,Citation37 as well as to assess the adoption of COVID-19 vaccination in China and provide recommendations for vaccination strategies.Citation36
3.2 Study methodology
3.2.1 Sample
The sample size used varies across different studies in the literature depending on target participants, study area, design, and the purpose of the study. Thus, no standard sample size has been established in the literature. The largest study sample size was 58,656 which was a study done in the global context.Citation9,Citation37 Study by Lin et al.Citation5 was a systematic review studies with 126 selected studies or reports. Other studies with relatively larger samples of 32,361, 7662, and 3479, were conducted in various countries such as UK,Citation37 seven European countries,Citation18 and USA,Citation25 respectively.
3.2.2 Nature of study and design
The existing studies on the measurement of vaccine hesitancy, predictors and hesitancy preventive measures are largely the combination of qualitative and quantitative studies with survey designCitation8,Citation19,Citation22,Citation27 and one exploratory study.Citation33
3.3 Findings
provides summary of studies on COVID-19 hesitancy (measurements, predictors, and hesitancy preventive measures) that have been validated for use in this review. Here, we present findings on each aspect of interest, that is, measurements of COVID-19 vaccine hesitancy, predictors or factors associated with COVID-19 vaccine hesitancy and preventive measures for COVID-19 vaccine hesitancy.
Table 1. Summary of studies on the COVID-19 vaccine hesitancy: measurement, key predictors, and prevention.
3.3.1 Measurements of COVID-19 vaccination hesitancy
The existing literature used three standard measures for hesitancy in relation to COVID-19 vaccination: optional response questions (for instance, yes or no or not sure), Likert scale, and linear scale measurements. Concerning options, questions were posed on one’s willingness to take the vaccine with the following options; Yes/No/ Not sure to determine one willingness to vaccinate.Citation8–18–Citation19–25–Citation27–29–Citation34 Likert scale with different points to measure one’s likelihood of getting vaccinated with responses such as Very likely/likely/not likely/not at all likely were also used.Citation21,Citation22 Finally, others use linear scale such as a scale ranging from 1 to 100, to measure how likely one is to receive a COVID-19 vaccination, where 1 (denoting very unlikely or not interested in being vaccinated) to finite number (most likely or most interested to be vaccinated).Citation33
3.3.2 Predictors of COVID-19 vaccination hesitancy
The review identified key predictors of COVID-19 vaccination hesitancy which can be categorized as sociodemographic/economic factors, occupational factors, knowledge on the vaccine, conspiracy belief, vaccine attribute, and psychological factors. For instances, some studies identified sociodemographic factors such as sex (female less likely to be vaccinated, that, high hesitancy), age (older people more likely to be vaccinated-less hesitant), education (educated people more likely to be vaccinated),Citation19,Citation21,Citation27 black/Hispanic, lower income, larger household, rural, are less likely to be vaccinated.Citation8 Similarly, Robinson et al.Citation6 argued in their systematic review that factors such as lower income, level of educational attainment, and belonging to an ethnic minority group were significantly less likely to intend to vaccinate. Studies such as Shekhar et al.Citation25 and Wang et al.Citation35 found that some occupation, for instance health workers such as medical doctors and nurses (especially those who deal with COVID-19 patients), are less hesitant to COVID-19 vaccination (that is, they are more likely to be vaccinated). Paul et al. (2021) reported that low knowledge about COVID-19 also increases vaccination hesitancy. Pivetti et al.Citation32 found that conspiracy beliefs negatively predicted general attitudes toward vaccines. The attributes of the vaccine such as increased efficacy and protection duration, decreased in adverse effect are associated with less hesitancy.Citation23 The psychological factors that affect COVID-19 vaccination hesitancy include trust (which is also affected by rural location and low income) in the vaccine, fear of side effect.Citation18,Citation20
3.3.3 Hesitancy corrective measures (Measures to reduce hesitancy)
The review identifies evidence-based finding on ways to minimized COVID-19 vaccination hesitancy and to promote public vaccination. Lazarus et al.Citation9 documented that a clear and consistent communication by government officials is crucial to building public confidence in vaccine programs and that effective campaign on the effectiveness of COVID-19 vaccine is necessary to build trust in the vaccine among the populace. This also includes designing health message targeted at hesitant group.Citation19 Kreps et al.Citation23 and Lackner and WangCitation33 also revealed that public health authorities should consider outreach strategies and targeted messaging campaigns for each unique context to address the specific concerns of older adults and minority communities that have been more susceptible to COVID-19. In the related study,Citation20 indicated that the COVID-19 related health literacy should be improved in students of university considering socio-cultural background. Additionally, a multi-organizational strategy to addressing disbelief in the vaccination program is also necessary to ensure a successful and fair implementation of the vaccination program.Citation29 Dickerson et al.Citation29 and Fisher et al.Citation8 confirmed this, reporting that educational campaigns aimed at sustaining future vaccination programs, as well as health engagement promotion and targeted and multipronged efforts, is required to increase acceptance of a COVID-19 vaccine when one is made availableCitation21 stated that addressing COVID-19 conspiracy beliefs, including via strategies that leverage-trusted sources of COVID-19 information (e.g., doctors), may promote the uptake of COVID-19 vaccines when they become available, continued public health message in mainstream media, particularly politically conservative publications that have backed COVID-related conspiracy theories. Concerning sociodemographic factorsCitation27 recommended that addressing sociodemographic characteristics related to COVID-19 vaccination may enhance adoption of the global vaccination program in order to combat future pandemics. The authors also said that focused health education efforts are required to enhance adoption of the COVID-19 vaccination. Similarly, according to,Citation37 public health campaigns aimed at increasing COVID-19 vaccine uptake should focus on educating and increasing trust in both those who are uncertain and those who are unwilling about the safety, efficacy, and side effect profile of vaccines, as well as spreading convincing evidence and clear communication about vaccine safety and effectiveness.Citation32
4. Discussion
The review process undertakes a synthesis of COVID-19 vaccine hesitancy in terms of measurement, key predictors, and preventive measures. The hesitancy of COVID-19 vaccine has been consistently measured by optional response, Likert or linear scaleCitation19,Citation27,Citation28 irrespective of geographical location, and study characteristics. The variation in measurements approach can be attributed to the purpose and nature of the study. In their study on the assessment of COVID-19 vaccine hesitancy using Likert scale with 4-points (very likely, somewhat likely, not likely, definitely not) in USA,Citation22 reported through their multiple regression analyses that vaccine hesitancy was significantly influenced by factors such as gender, education, employment, income, having children at home, political affiliation, and the perceived threat of contracting COVID-19 in the next 1 year. The authors asserted that, given the high prevalence of COVID-19 vaccine hesitancy in the United States, evidence-based communication strategies, massmedia strategies, and policy measures must be implemented across the country in order to convert vaccines into vaccinations and mass immunization, with particular attention paid to the groups identified in this study. Similarly,Citation25 andCitation35 in their separate studies in USA and China, respectively, using both qualitative and quantitative approach found that some occupation, for instance health workers such as medical doctors and nurses (especially those who deal with COVID-19 patients) are less hesitant to COVID-19 vaccination (that is, they are more likely to be vaccinated. However,Citation30 found that healthcare professionals who do not care for COVID-19 positive patients tend to have less trust in the COVID-19 vaccination than the general community, with nurses being more vaccine-averse than doctors. Although nurses had somewhat higher rates of yearly influenza immunization than the general population, they have more knowledge regarding COVID-19 vaccine. This low vaccination acceptance rate among nurses may have a detrimental effect on future vaccination compliance for persons who interact or engage with vaccine-hesitant nurses.
Campo-Arias and Pedrozo-PupoCitation20 and Neumann-Böhme et al.Citation18 found in their separate studies that the psychological factors that affect COVID-19 vaccination hesitancy include trust in the vaccine, fear of side effect. A similar study byCitation37 found that vaccine mistrust was no different between people with and without long-term health conditions. These findings could indicate that there will be a demand for the vaccine even among people who do not have physical health conditions, which may necessitate careful management of the vaccine supply and distribution. In addition, persons from poorer socio-economic backgrounds are more likely than others to be unsure or reluctant to get vaccination, which might increase already existing inequities over exposure to and experience of the virus in the United Kingdom. It is possible that those who are unsure will be a more favorable population for prospective treatments.Citation38 The researchers found that although some indicators show reluctance but not doubt (such as education, age, and residing in a rural area), it is very difficult to distinguish those individuals that are just unsure. In order to increase COVID-19 vaccine uptake, public health campaigns should focus on educating and building trust in both those who are unsure and those who are unwilling about the safety, efficacy, and side effect profile of vaccines.Citation38,Citation39 In their study to explore the role played by antecedents of COVID-related conspiracy beliefs in Italy,Citation32 found that conspiracy beliefs negatively predicted general attitudes toward vaccines. Additionally, the authors demonstrated that in order to mitigate the adverse effects of conspiracy beliefs, exposure to anti-conspiracy arguments both before to and after exposure to conspiracy theories may help recover vaccination intentions.Citation40,Citation41 Additionally, an experimental research showed that presenting reasonable reasons, in conjunction with providing mocking arguments, was a good technique for reducing conspiracy ideas. Given the beneficial benefits of analytical thinking on conspiracy belief reduction, exposing the logical errors of conspiracy ideas may be an effective method of discrediting them.Citation42
Neumann-Böhme et al.Citation18 investigated the willingness to be vaccinated (using binary response measures of Yes/No) in seven European countries (Denmark, France, Germany, Italy, Portugal, the Netherlands, and the UK) found that fear of side effect, and safety, gender (more female fear than the male). The authors argued that targeting those in the population who are currently hesitant seems most promising and cost-effective, but this requires convincing evidence and clear communication on the safety and effectiveness of the vaccine. A campaign emphasizing the social benefits of vaccination could increase the willingness to be vaccinated among those amenable to such pro-social motives. Their finding also reveal that a sizable proportion of the population indicates not to be open to vaccination. This group may remain at risk of spreading the virus and contracting the disease, even after herd immunity has been achieved.
Further, Lazarus et al.Citation9 reinforce the same finding that clear and consistent communication by government officials is crucial to building public confidence in vaccine progam. This includes explaining how vaccines work, as well as how they are developed, from recruitment to regulatory approval based on safety and efficacy. Effective campaigns should also aim to carefully explain a vaccine’s level of effectiveness, the time needed for protection (with multiple doses, if required) and the importance of population-wide coverage to achieve community immunity. It also includes preparing the public and leaders of civic, religious, and fraternal organizations that are respected within various sectors of society and local communities, as well as the private sector, for a mass vaccination program with credible spokespeople, local engagement, accurate information and technological support. Additionally, Thunstrom et al.Citation26 reported that knowing about COVID-19 vaccine avoidance before a vaccine is available can help government agencies, healthcare workers, and other authorities mitigate the impact of vaccine avoidance. Such efforts may involve developing policies and a preparedness for the vaccine avoidance. It might also involve public information campaigns designed to increase confidence in the effectiveness and safety of the vaccine. The authors also found that distrust in the government is higher amongst those who decline the vaccine. To address COVID-19 vaccine hesitancy, broader public health campaigns may therefore be less effective. Instead, efforts might focus on reaching out to healthcare providers (the most trusted source of vaccine safety information, see e.g Freed et al.Citation43) and local authorities, including religious leaders. Al-Mohaithef and PadhiCitation27 revealed in from their study in Saudi Arabia that participants’ perceived risk and trust in the health system were found to be significant predictors toward the intention of the COVID-19 vaccine. They proposed further study to corroborate their findings with public health promotion interventions.
Dickerson et al.Citation29 concluded from their studies in the United Kingdom that a broader and more precisely focused response is necessary to enhance vaccination acceptance throughout the country, especially among ethnic minorities and those living in impoverished neighborhoods. They attended that message must comfort people who are unsure or hesitant to consider vaccinations. This message must be culturally relevant, non-technical, and sensitive to the degrees of uncertainty and discomfort experienced by individuals. Additionally, they emphasized the need of communicating from trustworthy sources, noting a lack of confidence in the government and local council, but high levels of trust in the NHS, local hospitals, and schools. However, individuals least likely to get the vaccination also had suspicions about the NHS. When appropriate, the use of trustworthy organizations other than the NHS (e.g., schools), as well as trusted community and church leaders, may assist to build trust and encourage people who are unwilling to receive the vaccination. Olomofe et al.Citation34 conducted cross-sectional research to determine the parameters influencing COVID-19 vaccination uptake in Nigeria and found that sociodemographic characteristics such as respondents’ gender and religion had a statistically significant relationship with their desire to accept the vaccination. Other characteristics, such as the belief that vaccinations are either beneficial or harmful, prior vaccination history, and awareness of COVID-19, were also shown to have a statistically significant connection with desire to get the vaccine. The authors emphasized the need of public education in order to persuade people who are undecided or resistant to taking COVID-19 vaccinations.
5. Conclusion
In sum, this study provides rapid systematic literature reviews on COVID-19 vaccine hesitancy, which is a major threat to the fight against the virus through vaccination by addressing the following critical research questions; What is the standard measurement of hesitancy of COVID-19 vaccine in the literature? What are the key predictors (up to date) of hesitancy of COVID-19 vaccine? What are the evidence-based measures in the literature to minimize COVID-19 vaccine hesitancy and promote public patronage of the vaccine? A sample of 25 studies out of 470 potential studies were used after a comprehensive literature search and rigorous assessment based on PRISMA-P guidelines on the subject. The findings reveal three standard measures of vaccine hesitancy: optional response questions, Likert scale, and linear scale measurements. Factors such as sociodemographic/economic factors, occupational factors, knowledge on the vaccine, vaccine attributes, conspiracy belief and psychological factors are the major predictor of COVID-19 vaccine hesitancy. Evidence-based findings identified the following measures to eliminate COVID-19 vaccine hesitancy (1) providing a clear and consistent communication and effective campaign to build public confidence and trust in the vaccine; (2) providing outreach strategies and targeted messaging campaigns for each unique context; (3) A campaign emphasizing the social benefits of vaccination; (4) framing careful, empathetic messaging, targeting those whom it will benefit the most, and a multi-organizational approach to address issues; (5) Increasing the knowledge (vaccination literacy) in schools, institutions, organizations (formal and informal) and media; (6) conspiracy beliefs, including via strategies that leverage trusted sources of COVID-19 information. Targeted health education interventions are needed to increase the uptake of the future COVID-19 vaccine educating and increasing trust in both those who are uncertain and those who are unwilling on the safety, efficacy, and side effect profile of vaccines and spreading convincing evidence and clear communication on the safety and effectiveness of vaccines (7) explaining how vaccines work, as well as how they are developed, from recruitment to regulatory approval based on safety and efficacy. Effective campaigns should also aim to carefully explain a vaccine’s level of effectiveness, the time needed for protection.
Ethical considerations
This article followed all ethical standards for research without direct contact with human or animal subjects.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Anakpo G, Mishi S. Business response to COVID-19 impact: effectiveness analysis in South Africa. Southern African J Entrepreneurship Small Bus Manage. 2021;13(1):7. doi:10.4102/sajesbm.v13i1.397.
- Tshabalala N, Anakpo G, Mishi S. Ex ante vs ex post asset-inequalities, internet of things, and COVID-19 implications in South Africa. Africagrowth Agenda. 2021;18:18–12.
- Jafta K, Anakpo G, Mishi S. 2022. Income and poverty implications of Covid-19 pandemic and coping strategies: the case of South Africa. Africagrowth Agenda.
- Komanisi E, Anakpo G, Mishi S. Vulnerability to COVID-19 impacts in South Africa: analysis of the socio-economic characteristics. Africagrowth Agenda. 2022.
- Lin C, Tu P, Beitsch LM. Confidence and receptivity for covid‐19 vaccines: a rapid systematic review. Vaccines. 2021;9(1):1–32. doi:10.3390/vaccines9010016.
- Robinson E, Jones A, Lesser I, Daly M. International estimates of intended uptake and refusal of COVID-19 vaccines: a rapid systematic review and meta-analysis of large nationally representative samples. Vaccine. 2021;39(15):2024–34. doi:10.1016/j.vaccine.2021.02.005.
- Pogue K, Jensen J, Stancil C, Ferguson D, Hughes S, Mello E, Burgess R, Berges B, Quaye A, Poole B. Influences on attitudes regarding potential COVID-19 vaccination in the United States. Vaccines. 2020;8(4):582. doi:10.3390/vaccines8040582.
- Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes toward a potential SARS-CoV-2 vaccine: a survey of U.S. adults. Ann Intern Med. 2020;173(12):964–73. doi:10.7326/M20-3569.
- Lazarus JV, Ratzan SC, Palayew A, Gostin LO, Larson HJ, Rabin K, Kimball S, El-Mohandes A. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–28. doi:10.1038/s41591-020-11.
- World Health Organization (2019). World Health Organization Ten threats to global health in 2019. Retrieved on September 22, 2021 from https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 .
- Mac Donald N. Vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33(34):4161–64. doi:10.1016/j.vaccine.2015.04.036.
- SAGE. Report on SAGE Working Group on vaccine hesitancy. 2014. Retrieved on August 24, 2021 from https://cdn.who.int/media/docs/default-source/immunization/sage/2014/october/sage-working-group-revised-report-vaccine-hesitancy.pdf?sfvrsn=240a7c1c_4 .
- Reiter P, Pennell M, Katz M. Acceptability of a COVID-19 vaccine among adults in the United States: how many people would get vaccinated? Vaccine. 2020;38(42):6500–07. doi:10.1016/j.vaccine.2020.08.043.
- Machingaidze S, Wiysonge C. Understanding COVID-19 vaccine hesitancy. Nat Med. 2021;27(8):1338–39. doi:10.1038/s41591-021-01459-7.
- Chevallier C, Hacquin AS, Mercier H. COVID-19 vaccine hesitancy: shortening the last mile. Trends Cogn Sci. 2021;25(5):331–33. doi:10.1016/j.tics.2021.02.002.
- CASP. Critical appraisal skills programme. 2019 [accessed 2019 March]. https://casp-uk.net/wp-content/uploads/2018/01/CASP-Qualitative-Checklist-2018.pdf .
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Duffy S. Guidance on the conduct of narrative synthesis in systematic reviews. A product from the ESRC methods programme version. 2006;1(1):b92.
- Neumann-Böhme S, Varghese NE, Sabat I, Barros PP, Brouwer W, van Exel J, Schreyögg J, Stargardt T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Health E. 2020;21(7):977–82. doi:10.1007/s10198-020-01208-6.
- Callaghan T, Moghtaderi A, Lueck JA, Hotez P, Strych U, Dor A, Fowler EF, Motta M. Correlates and disparities of COVID-19 vaccine hesitancy. Rochester: Social Science Research Network. Washington, DC, United States; 2020. Available at SSRN: https://ssrn.com/abstract=3667971 .
- Campo-Arias A, Pedrozo-Pupo JC. COVID-19 vaccine distrust in Colombian university students: frequency and associated variables. MedRxiv. 22. 2021. Retrieved on September 18, 2021 from https://www.medrxiv.org/content/10.1101/2021.03.07.21253080v1.full .
- Earnshaw VA, Eaton LA, Kalichman SC, Brousseau NM, Hill EC, Fox AB. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl Behav Med. 2020;10(4):850–56. doi:10.1093/tbm/ibaa090.
- Khubchandani J, Sharma S, Price JH, Wiblishauser MJ, Sharma M, Webb FJ. COVID-19 vaccination hesitancy in the United States: a rapid national assessment. J Community Health. 2021;46(2):270–77. doi:10.1007/s10900-.
- Kreps S, Prasad S, Brownstein JS, Hswen Y, Garibaldi BT, Zhang B, Kriner DL. Factors associated with US adults’ likelihood of accepting COVID-19 vaccination. JAMA network open. 2020;3(10):e2025594–e2025594. doi:10.1001/jamanetworkopen.2020.25594.
- Romer D, Jamieson KH. Social science & medicine conspiracy theories as barriers to controlling the spread of COVID-19 in the U. S. Soc Sci Med. 2020;263:113356. doi:10.1016/j.socscimed.2020.113356.
- Shekhar R, Sheikh AB, Upadhyay S, Singh M, Kottewar S, Mir H, Barrett E, Pal S. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines. 2021;9(2):1–18. doi:10.3390/vaccines9020119.
- Thunstrom L, Ashworth M, Finnoff D, Newbold S. Hesitancy towards a COVID-19 vaccine and prospects for herd immunity. SSRN Electron J. 2020;35:1–50. doi:10.2139/ssrn.3593098.
- Al-Mohaithef M, Padhi BK. Determinants of covid-19 vaccine acceptance in Saudi Arabia: a web-based national survey. J Multidiscip Healthcare. 2020;13:1657–63. doi:10.2147/JMDH.S276771.
- Detoc M, Bruel S, Frappe P, Tardy B, Botelho-nevers E, Gagneux-brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. vaccine. 2020;38(45):7002–06. doi:10.1016/j.vaccine.2020.09.041.
- Dickerson J, Lockyer B, Moss RH, Endacott C, Kelly B, Bridges S, Crossley KL, Bryant M, Sheldon TA, Wright J, et al. COVID-19 vaccine hesitancy in an ethnically diverse community: descriptive findings from the Born in Bradford study. Wellcome Open Res. 2021;6:23. doi:10.12688/wellcomeopenres.16576.1.
- Dror AA, Eisenbach N, Taiber S, Morozov NG, Mizrachi M, Zigron A, Srouji S, Sela E. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775–79. doi:10.1007/s10654-020-00671-y.
- Graffigna G, Palamenghi L, Boccia S, Barello S. Relationship between citizens’ health engagement and intention to take the covid-19 vaccine in Italy: a mediation analysis. Vaccines. 2020;8(4):1–11. doi:10.3390/vaccines8040576.
- Pivetti M, Melotti G, Bonomo M, Hakoköngäs E. Conspiracy beliefs and acceptance of covid‐vaccine: an exploratory study in Italy. Soc Sci. 2021;10(3):108. doi:10.3390/socsci10030108.
- Lackner CL, Wang CH. Demographic and psychological correlates of SARS-CoV-2 vaccination intentions in a sample of Canadian families MedRxiv. 2020;100091. doi:10.1101/2020.11.04.20226050.
- Olomofe C, Victor Soyemi K, Felicia Udomah B, Olabisi Owolabi A, Eziashi Ajumuka E, Chukwudum Igbokwe M, Uriel Ashaolu O, Ayodele Adeyemi O, Bolatito Aremu-Kasumu Y, Folasade Dada O, et al. Predictors of uptake of a potential Covid-19 vaccine among Nigerian adults. medRxiv, 2020-12. 2021;12(1):1000442. https://www.medrxiv.org/content/10.1101/2020.12.28.20248965v1 .
- Wang K, Lai E, Wong Y, Fai K, Wai A, Cheung L, Ying E, Chan Y, Kiong E, Yeung S, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: a cross-sectional survey. Vaccine. 2020;38(45):7049–56. doi:10.1016/j.vaccine.2020.09.021.
- Wang J, Jing R, Lai X, Zhang H, Lyu Y, Knoll MD, Fang H. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. 2020;8(3):482.
- Paul E, Steptoe A, Fancourt D. Attitudes towards vaccines and intention to vaccinate against COVID-19: implications for public health communications. The Lancet Reg Health - Eur. 2021;1:100012. doi:10.1016/j.lanepe.2020.100012.
- Habersaat K, Betsch C, Danchin M, Sunstein CR, Böhm R, Falk A, Brewer NT, Omer SB, Scherzer M, Sah S. Ten considerations for effectively managing the COVID- 19 transition. Nat Hum Behav. 2020;4(7):677–87. doi:10.1038/s41562-020-0906-x.
- Rhodes A, Hoq M, Measey MA, Danchin M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 2021;21(5):110.
- Jolley D, Douglas KM. Prevention is better than cure: addressing antivaccine conspiracy theories. J Appl Soc Psychol. 2017;47(8):459–69. doi:10.1111/jasp.12453.
- Lyons B, Merola V, Reifler J. Not just asking questions: effects of implicit and explicit conspiracy information about vaccines and genetic modification. Health Commun. 2019;34(14):1741–50. doi:10.1080/10410236.2018.1530526.
- Orosz G, Kreko P, Paskuj B, Toth-Kiraly I, Böthe B, Roland-Levy C. Changing conspiracy beliefs through rationality and ridiculing. Front Psychol. 2016;7:1525. doi:10.3389/fpsyg.2016.01525.
- Freed G, Clark S, Butchart A, Singer D, Davis M. Sources and perceived credibility of vaccine-safety information for parents. Pediatrics. 2011;127(Supplement 1):S107–S112. doi:10.1542/peds.2010-1722P.