
ABSTRACT
We performed a systematic literature review in PubMed and Embase (2016–2021) to investigate the drivers of and barriers to routine vaccination in adults aged 50 and older globally. A thematic assessment identified three categories across 61 publications: sociodemographic, health-related, and attitudinal. The most common sociodemographic determinants (factors identified in studies; n = 47) associated with vaccination uptake were economic status, age, education, and household composition, which had mixed effects on vaccine uptake. For health-related determinants (n = 27), individuals with comorbidities and health care consumption were the most common factors, both increased vaccine uptake. The most common attitudinal factors (n = 42) were self-efficacy, provider or other’s recommendations, and vaccine-preventable disease awareness; across studies, all attitude factors had a positive effect, unlike the sociodemographic and health status categories. Findings suggest that patient and provider awareness and education campaigns are effective ways to increase uptake of routine vaccinations in older adults.
Introduction
Older adults (65 years or older) constitute a large and growing proportion of the world’s population.Citation1 The World Health Organization (WHO) estimates that between 2015 and 2050, the population aged ≥60 years will nearly double globally.Citation2 With age comes immunosenescence, leading to increased vulnerability to infectious diseases and a need to boost immunity in this population.Citation3,Citation4 Vaccination is one of the most life-saving and cost-saving interventions in the history of health care.Citation5 Each year in the United States, influenza vaccination prevents more than 7 million illnesses and 90,000 hospitalizations, the latter mostly in older adults (ages ≥65).Citation6 Vaccines also provide economic benefits; one review estimated that for every euro spent on influenza vaccination for older adults in the United Kingdom, €1.35 was saved by reduced medical spending elsewhere in the health care system.Citation7
The United States Centers for Disease Control and Prevention (CDC) recommends routine vaccination against tetanus/diphtheria/pertussis (Tdap) and seasonal influenza for adults of all ages, herpes zoster for adults aged 50 years and older, and pneumococcus for adults aged 65 years and older.Citation8 However, there is much variation globally in recommendations for adult vaccination. For example in January 2022, of the 30 nations in the European Union/European Economic Area, 29 officially recommend influenza vaccine, 21 recommend pneumococcal vaccine, 19 recommend tetanus vaccine, and 7 recommend herpes zoster vaccine.Citation9 Additionally, the situation in low- and middle-income countries (LMICs) is unique, because public health policies, medical conditions and costs, health awareness, and vaccine availability differ from high income countries. There is a lack of epidemiologic information in many LMICs,Citation10 which precludes robust estimations of cost-effectiveness of vaccination,Citation11 leading to a lack of concrete guidance on vaccination practices.Citation12–14 However, available data indicate that some vaccine-preventable diseases have a greater burden in LMICs,Citation10,Citation14 creating an impetus for developing vaccine delivery systems in these countries. Ortiz and Neuzil offer several suggestions for facilitating the implementation of influenza vaccination programs in LMICs, including development of vaccines that require fewer healthcare resources to administer, conducting clinical trials in LMIC settings to evaluate vaccine efficacy in terms of locally relevant outcomes, and integration of vaccine administration into current systems of primary care.Citation15
Despite the demonstrated value of vaccines, adult vaccination rates in many countries remain suboptimal, even where there are publicly funded programs. For example, in the United States, the Healthy People 2020 goals for adult vaccination rates were 80% for influenza (for ages 18–64 years; 90% in adults over 65 years), 30% for herpes zoster, and 60% for pneumococcus (for ages 18–64 years at increased risk; 90% in adults over 65 years).Citation16 However, despite vaccination rate goals, based on data from the 2017–2018 National Health Interview Survey in the United States, influenza vaccination coverage among adults aged 50–64 years and those 65 years and over was 48% and 72%, respectively.Citation17 Only 23% of adults aged 19–64 years at increased risk and 69% of adults aged 65 years and over received the pneumococcal vaccine.Citation17 The goal for herpes zoster vaccine was met, with 35% of adults aged 60 years and over vaccinated.Citation17
The goal set by the WHO resolution WHA56.19 for countries in the European region was 75% influenza vaccination coverage by 2010,Citation18 and this goal was adopted by the European Union for the 2014–2015 season.Citation19 In surveys conducted by the Vaccine European New Integrated Collaboration Effort (VENICE) consortium, the Netherlands was the only European country to meet the WHO goal for influenza vaccination by 2010. Vaccination rates for influenza in the 33 countries reporting coverage data for older adults in 2014–2015 ranged from 0.03% to 76.3%, with a median of 34%.Citation20 A slight improvement was observed during the 2016–2017 season, with a median coverage rate of 47%.Citation21 Studies from other countries report influenza vaccine coverage rates of less than 50% in adults aged 60 years and older in Australia,Citation22 China,Citation23 and Iran.Citation24 Over the past two years, the COVID-19 pandemic has adversely affected adult vaccination uptake, as indicated by a survey of 28,400 respondents from 26 middle- and high-income countries.Citation25
To narrow the gap between vaccination rate targets and actual vaccination rates, a better understanding of the factors influencing vaccination uptake in older adults is needed. Recent systematic reviews of the factors affecting adult vaccination rates have covered specific interventions,Citation26,Citation27 health care settings,Citation28 and world regions.Citation29 A comprehensive overview of adult vaccination barriers and drivers is lacking. Thus, we performed a systematic review of the literature on routine adult vaccinations, limited only by age (50 years or older), with the goal of identifying the drivers of and barriers to vaccine uptake in this population.
Methods
The review was conducted in accordance with the principles of narrative synthesis in systematic reviewsCitation30 and is presented in accordance with the extension of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines on scoping reviews.Citation31
We conducted an electronic search on 1 February 2021, going back to 1 January 2016, using PubMed and Embase. The search algorithms are shown in Supplementary Table S1. We compiled all identified articles into a screening file, removed duplicates, and screened the remaining articles for eligibility using the inclusion and exclusion criteria outlined in . The primary inclusion criterion was the reporting of determinants (either drivers or barriers) of routine adult vaccination uptake. Article selection is illustrated in . We selected articles based on their titles and abstracts during the first phase of screening; we then read each selected publication in a second phase of screening, and articles were included or excluded based on the full text. All selections and rejections were confirmed by two different reviewers.
Figure 1. Flowchart of study selection process. One article fit into both final categories. Individual/provider-related articles (n = 61) were the subject of the current review.
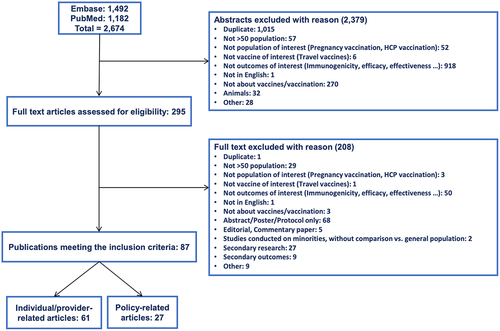
Table 1. Inclusion and exclusion criteria for literature review study selectiona.
Items extracted from each selected article were as follows: title, authors, country/countries of origin, study design, study setting, number of subjects, and analysis type. Additional items of particular interest for this review were the vaccine(s) type being studied and the outcomes reported, including quantitative data on vaccination uptake and qualitative data on patient attitudes and experiences. Data were extracted into an Excel spreadsheet by one reviewer and checked for accuracy by a second reviewer.
We grouped determinants of routine adult vaccination into three categories: sociodemographic factors, health-related factors, and attitudinal factors (). Sociodemographic factors included items such as age, gender, ethnicity, education level, employment status, and health insurance coverage. Health-related factors included habits such as smoking, alcohol intake, and physical activity, as well as general functional status, the presence of comorbidities, and use of health care services. Attitudinal factors encompassed individual perceptions of the risk of disease and the benefits and risks of vaccination, as well as measures of self-efficacy (the ability to exercise control over one’s own health) and social interactions with friends, family, and health care providers (HCPs) regarding vaccines.
Table 2. Categorization of themes and associated factors influencing routine adult vaccination.
Results
The search and screening process identified 87 publications (), which we grouped according to whether they reported individual/provider-related determinants (n = 61) or policy/programmatic-related determinants of vaccination uptake (n = 27). Articles describing the individual/provider-related determinants are the subject of this manuscript.
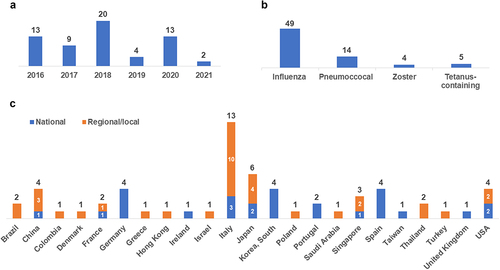
The summary characteristics of the 61 studies included in this review are listed in Supplementary Table S2, including the author, study location, vaccines investigated, study population, study design, analysis type, and a summary of the results for each factor affecting vaccination. The majority of studies had a cross-sectional design (n = 46), while 14 were database analyses or medical records reviews, and one used mixed methods (cross-sectional and prospective components). Among these studies, 22 categories of factors affecting vaccine uptake were identified, which were organized into the three thematic categories shown in . Some studies contained multiple factors, with 47 studies reporting on sociodemographic factors,Citation32–78 27 reporting on health-related factors,Citation32–34,Citation36,Citation37,Citation40–42,Citation45,Citation46,Citation48,Citation50,Citation53,Citation54,Citation57,Citation61,Citation62,Citation72-81 and Citation42 reporting on attitudinal factors.Citation33,Citation34,Citation36,Citation37-39,Citation40,Citation43–45,Citation47,Citation53-55,Citation57,Citation59,Citation61,Citation66–76,Citation78–92 Four studies gathered data from HCPs, as opposed to individual adults.Citation54,Citation59,Citation82,Citation91 Descriptive statistics for the 61 studies are shown in . Most studies reported determinants of influenza vaccination (n = 49), and most originated in European countries (Italy had 13 publications), through the Middle East, the Far East, and North and South America were also represented. Ten studies were from LMICs: Brazil,Citation40,Citation77 China,Citation38,Citation39,Citation72,Citation78 Columbia,Citation32 Thailand,Citation47 and Turkey.Citation55,Citation90
Figure 2. Descriptive statistics of included studies by (a) year, (b) vaccine, and (c) geographic location. Categories in panel B were not mutually exclusive, so the sum is >61.
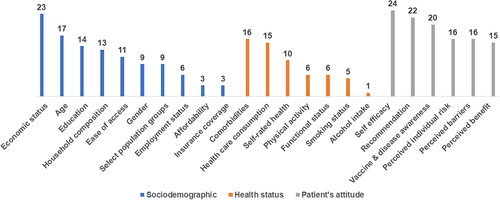
The determinants of routine older adult vaccination were categorized as sociodemographic, health-related factors, and attitudinal factors (). Economic status was the most frequently reported sociodemographic factor (in terms of the number of studies), while having a comorbidity and health care consumption were the most often reported health-related factors. Self-efficacy and recommendations about vaccination were the most frequent attitudinal factors documented in our review.
Figure 3. Distribution of studies by the factors impacting routine adult vaccination. The factors correspond to those listed in .
The heterogeneity of the studies in terms of designs, populations, and analyses precluded a quantitative meta-analysis. For this reason, a narrative synthesis of findings is reported for each factor category. In each synthesis, the primary focus is on data from individual subjects, and data from HCPs is highlighted separately.
Sociodemographic factors
In studies assessing age and vaccination status, the association between age and vaccination varied by vaccine type. All influenza vaccination studies except oneCitation45 found that older age was statistically significantly associated with greater vaccination uptake.Citation32,Citation37,Citation38,Citation41,Citation46,Citation48,Citation62,Citation67-70,Citation73,Citation76 Self-reported pneumococcal vaccination was positively correlated with increasing age in two studies.Citation32,Citation67 However, herpes zoster vaccine acceptability (i.e., being “in favor” of vaccination) was associated with younger age among individuals 50 or older,Citation43 and findings for tetanus vaccines were mixed.Citation32,Citation67
The association between gender and vaccination is unclear. Four studies found that being male was associated with higher influenza vaccination rates,Citation39,Citation44,Citation61,Citation70 while two studies found that females were more likely to be vaccinated against influenza.Citation62,Citation73 The latter studies were corroborated by two studies reporting that females had higher influenza vaccination rates than males.Citation57,Citation74 Del Signore et al. 2020 found being a male to be positively associated with herpes zoster vaccination in France.Citation71
Studies of select population groups and communities (terms to present results for these groups are derived from the original studies) generally found that immigrant populations, resident foreigners, and ethnic minority groups had lower vaccination uptake than native-born citizens or ethnic majority groups.Citation33,Citation35,Citation49,Citation51,Citation56,Citation60,Citation65,Citation70,Citation74 A series of four studies from Italy found that the percentage of “foreigners and stateless persons” residing in a census district was associated with lower influenza vaccine coverage among adults aged 65 or older.Citation51,Citation56,Citation60,Citation65 A national-level study from Italy found that African immigrants (but not immigrants from Europe, Asia and Oceania, or America) had a lower influenza vaccine coverage ratio than Italian citizens.Citation35 Similarly, among adults aged 65 or older in Spain, the “foreigner” population was less likely than those of Spanish nationality to be vaccinated against influenza.Citation70 A comparison of influenza vaccination in Medicare recipients (aged 65 or older) in the United States highlighted racial disparities, with vaccination rates of 49% for Whites, 48% for Asians, 33% for Blacks, and 29% for Hispanics.Citation74 Racial disparities were also seen in individuals aged 70 in England, where White-British, Indian, and Bangladeshi individuals received the zoster vaccine at rates of 55–61%, while vaccination rates were significantly lower in Black and mixed White/Black or White/Asian individuals.Citation49 Among older people (aged 65 or older) with disabilities in Taiwan, aboriginal descent was a significant predictor of non-vaccination against influenza.Citation33
In assessments of household composition, most studies (11 of 13) showed that being married or living in a larger household (more than two people), compared with living alone, was associated with being vaccinated against influenza.Citation33,Citation34-37,Citation46-51,Citation53-56,Citation60-65,Citation77 However, two studies from Singapore found that being married was negatively associated with influenza vaccination and that having previously been married (i.e., currently separated, divorced, or widowed) was positively associated with pneumococcal vaccination.Citation41,Citation50
Findings were also mixed with regard to education levels. Education was defined in a variety of ways across the studies in this group, and what was considered a “high” level of education differed by local context. Ten studies demonstrated a positive association between higher levels of education and vaccination.Citation33,Citation37,Citation38,Citation47,Citation50,Citation55,Citation66,Citation72,Citation73,Citation78 Of these, seven were conducted in Asian countries.Citation33,Citation37,Citation38,Citation47,Citation50,Citation72,Citation78 In contrast, four studies found a negative relationship between higher levels of education and vaccination.Citation44,Citation53,Citation61,Citation65 In South Korea, a high school or college-level education (vs. middle school) was negatively associated with influenza vaccination for individuals aged 50–64.Citation53 In Spain, lower levels of education (none vs. any primary, secondary, or university education) were positively associated with vaccination,Citation44 and in France, having a bachelor’s degree (but not a master’s or higher degree, and not a high school education) was positively associated with vaccine hesitancy (hesitancy was defined as refusal or delay of vaccination, or vaccination despite having doubts about efficacy).Citation61
Four studies found an association between employment status, specifically unemployment or retirement, and higher vaccination rates.Citation40,Citation41,Citation53,Citation73 Conversely, two studies conducted at a local level in Italy found a negative correlation between living in an area with an increasing unemployment rate and vaccination rates of individuals aged ≥65.Citation52,Citation65 One study from Korea noted a negative association of vaccination with blue-collar vs. white-collar positions.Citation53
Economic status was the most frequently identified sociodemographic factor, but the results regarding its association with vaccination were mixed. Ten studies reported a positive relationship between higher income status or socioeconomic class and vaccination (or, conversely, a negative relationship between greater deprivation or lower income and vaccination).Citation36,Citation40,Citation41,Citation49,Citation50,Citation54–56,Citation60,Citation75,Citation78 Seven studies found the opposite – that higher economic status was associated with decreased likelihood of vaccination.Citation32,Citation38,Citation39,Citation44,Citation51,Citation52,Citation65 One study analyzed data separately for men and women of different age groups (50–64 and ≥65)Citation53 and found that, among men aged 50–64, moderate-high (vs. low) family income had a statistically significant negative association with influenza vaccination. The results in women differed by age group, with moderate-high (vs. low) family income being negatively associated with influenza vaccination among women aged 50–64, but high family income (vs. low) having a positive association with vaccination among women aged ≥65.Citation53
Three studies conducted in various municipalities in Italy found that vaccination coverage was lowest at the two extremes of the socioeconomic and health deprivation index, a 5-tier classification system that defines socioeconomic status based on factors such as demographics, housing conditions, and occupational status.Citation58,Citation63,Citation64 The authors explained this phenomenon as potentially the result of anti-vaccination campaigns, which may have produced an exaggerated perception of potential vaccine risks in the higher socioeconomic classes,Citation64 or as the effect of different responses to recommendations on disease prevention, probably due to different cultural norms.Citation58 However, several similarly designed Italian studies observed linear trends of higher vaccination with higher deprivationCitation52,Citation65 or lower vaccination with higher deprivation,Citation56,Citation60 as noted above.
A positive association between insurance coverage and vaccination against influenza, pneumococcus, and tetanus was established in three studies.Citation32,Citation42,Citation78 Affordability was also influential in increasing vaccination uptake, as high cost was given as a reason for non-vaccination among individuals in Poland,Citation45 and no-cost vaccination access was shown to be a facilitator of vaccination in Ireland.Citation36 From the HCP perspective, free vaccination was noted by nurses in Israel as a facilitator of influenza vaccination.Citation54
There was no clear trend in vaccination uptake between rural and urban areas. Studies from Poland, the United States, and Turkey reported higher vaccination rates in individuals in urban centers compared to rural areas,Citation45,Citation55,Citation74 while individuals in rural areas had greater vaccination uptake in China, South Korea, and Portugal.Citation38,Citation39,Citation62,Citation76 For studies looking at overall ease of access, convenience was found to be positively related to vaccination in adult individuals,Citation45,Citation47,Citation54,Citation59,Citation71 with nurses mentioning on-site vaccination and priority lines as facilitators and difficulty going to the clinic and lack of vaccine availability as barriers to vaccination.Citation54
Health-related factors
Among health-related factor studies, a positive relationship between influenza vaccine uptake and the presence of comorbidities (vs. the absence of comorbidities) was observed in 13 out of 15 studies.Citation34,Citation40,Citation41,Citation45,Citation46,Citation62,Citation70,Citation73–76,Citation78 Three studies found a proportional correlation between the absolute number of comorbidities and the likelihood of vaccination.Citation32,Citation62,Citation70 Individuals with specific comorbidities including chronic lung disease,Citation72,Citation73 cardiovascular disease,Citation73,Citation78 metabolic disorders,Citation73 cancer,Citation73 and mental health diagnosesCitation75 were more likely to receive influenza vaccination. In contrast, two studies from the United States reported a negative association between the presence of comorbidities and influenza vaccination.Citation42,Citation75 Regarding other vaccines, Cano Gutierrez et al. 2016 established that individuals with comorbidities were more likely to self-report pneumococcal vaccination in Colombia, but the results were inconclusive for tetanus vaccination.Citation32 Watanabe et al. 2020 found the presence of chronic respiratory diseases to be positively associated with pneumococcal vaccination in Japan.Citation81
Studies evaluating the association between health care consumption and adult vaccination unanimously reported a positive relationship for both influenza (n = 12) and pneumococcal (n = 2) vaccination.Citation33,Citation34,Citation40,Citation41,Citation46,Citation48,Citation50,Citation57,Citation68,Citation74-77,Citation79 Seven studies showed that vaccination was significantly positively associated with increased general practitioner (GP)/doctor visits, increased contacts with primary care, or having a regular GP to consult.Citation34,Citation41,Citation48,Citation50,Citation68,Citation75,Citation79 One study reported this positive association specifically in patients with chronic obstructive pulmonary disease,Citation48 while another reported a positive association of vaccination with outpatient visits in a disabled population aged 65 and older.Citation33 Two studies confirmed an increased frequency of vaccination when there was an increase in physician visits and government-subsidized prescriptionsCitation74 or when contact with a GP increased via telephone consultations and office or home visits.Citation57
Self-rated health was found to influence vaccination status in different ways. Five studies found a positive association with vaccination when individuals perceived their health as poor,Citation70,Citation73,Citation80 or a negative association when it was perceived as good.Citation37,Citation53 Machado et al. 2020 showed that Portuguese women with poor self-rated health presented higher vaccination prevalence than those with good self-rated health.Citation76 From the HCP perspective, nurses interviewed in Israel reported that an individual’s feeling of general good health was associated with an unwillingness to get vaccinated.Citation54 Three studies found contrasting results in adult individuals, where poor perceived health levels were negatively associated with vaccination or were associated with increased vaccine hesitancy.Citation41,Citation50,Citation61
A positive relationship between influenza vaccination and physical activity was observed in five out of six studies.Citation37,Citation40,Citation41,Citation53,Citation77 Physical activity was most often defined as being active at least 150 minutes per week in the reviewed studies.Citation40,Citation41,Citation77 Byeon et al. 2018 (Korea) observed a stronger association between influenza vaccination and physical activity as individuals’ age increased.Citation53 Regarding activity frequency, Kwon et al. 2016 (Korea) found moderate activity (self-defined physical activity at least once per week) to be significantly associated with vaccination while everyday activity was not significant.Citation37 In contrast, Hellfritzsch et al. 2017 (Denmark) found that physical activity was less common among vaccinated people in comparison to unvaccinated people.Citation46
Five studies found a positive relationship between vaccination and increased independence and functional status.Citation32–34,Citation73,Citation79 A variety of measures were used to quantify independence and functional status: the Lawton scale, which assigns a score from 0 to 8 based on the ability to accomplish activities of daily living such as using the telephone, taking medications, managing finances, preparing meals, etc.;Citation32 the Barthel index, which assigns a score ranging from 0 (complete dependence) to 100 (complete independence);Citation34,Citation79 and some categorical measures based on type and severity of disabilityCitation33 or living in a nursing home.Citation73 However, Hellfritzsch et al. 2017 found that increased dependence and support was more frequent among vaccinated individuals in Denmark.Citation46 Along with these findings, the authors noted that in Denmark there are policies including no-cost in-house vaccination for providers or patients.
A negative relationship between influenza vaccination and current smoking (vs. never or former smoking) was observed in four studies,Citation37,Citation40,Citation53,Citation76 but no association was observed in one study.Citation46 One study from Korea reported a negative impact of alcohol use on vaccination, with an 11–16% reduction in influenza vaccination in women aged ≥50 who drank alcohol (compared to those who did not, amount unspecified in study) and a 19% reduction in men aged 50–64.Citation53
Attitudinal factors
Among all the factors included in this review, the most frequently studied was self-efficacy, i.e., a person’s belief that they have power over their own health. Manifestations of self-efficacy included previous acceptance of vaccines and preventive health behaviors such as completing health screenings. Twenty-four studies demonstrated that a history of previous vaccination,Citation33,Citation34,Citation54,Citation57,Citation72,Citation74-75,Citation79,Citation80,Citation83-87,Citation89-91 having a positive attitude toward vaccination,Citation43,Citation45,Citation61,Citation68,Citation71,Citation92 and adopting preventive behaviorsCitation37,Citation53,Citation70,Citation76 were associated with a positive influence on vaccine uptake. Regarding previous vaccination, seven studies showed that having a vaccine record and/or previous vaccination had a positive association with vaccination in the future against the same or a different vaccine-preventable disease.Citation33,Citation34,Citation75,Citation79,Citation80,Citation87,Citation91 In two studies conducted in the United States and China, individuals with previous pneumococcal vaccination presented higher influenza vaccination coverage rates than those without.Citation72,Citation74 A study in the Netherlands showed that vaccination in the previous year had the strongest impact on predicting influenza vaccination uptakeCitation83 Among studies of attitudes toward vaccination, results showed that willingness or intent to receive the influenza vaccine, or a generally positive/confident attitude toward vaccination, was positively associated with vaccination against influenza,Citation45,Citation68 herpes zoster,Citation43,Citation71 and pneumococcus.Citation92 Consistent with these findings, one study found that being vaccine hesitant was negatively associated with influenza vaccination uptake.Citation61 Finally, studies of preventive behaviors all found that the practice of having health screenings had a positive association with vaccination.Citation37,Citation53,Citation70,Citation76 Health screenings varied across studies and included clinical and laboratory measurements of blood pressure, cholesterol, and glucose as well as colonoscopy, prostate, and breast exams.
Among the 22 studies examining the impact of a recommendation to vaccinate by a HCP, 17 found a positive effect.Citation36,Citation39,Citation40,Citation43-45,Citation54,Citation68,Citation69,Citation80,Citation82,Citation84,Citation85,Citation87,Citation89-91 Eight of the studies found that recommendations from relatives had a positive influence on vaccination.Citation45,Citation54,Citation68,Citation78,Citation88,Citation89,Citation91,Citation92 Conversely, five studies indicated lack of recommendation from HCPsCitation35,Citation81,Citation85 had a negative correlation with vaccination and two studies found discouragement from an HCP was the main reason for not vaccinating.Citation67,Citation90 From the HCP perspective, three studies surveyed HCPs on providing recommendations for vaccinations;Citation54,Citation82,Citation91 among them it was found that doctors who regularly prescribed pneumococcal vaccination also encouraged revaccinationCitation91 in Japan, where there are guidelines for HCPs to revaccinate adults aged 65 years and older.Citation93 Additionally, non-vaccination of patients was associated with providers not regularly advising vaccination (i.e., at the first visit within an accounting period) or when the provider reported neutral (as opposed to positive or negative) feelings about vaccination counseling.Citation82
Twenty studies showed that awareness of the vaccine and associated disease were positively associated with vaccination uptake.Citation36,Citation39,Citation40,Citation43,Citation45,Citation47,Citation54,Citation55,Citation59,Citation66,Citation67,Citation73,Citation78,Citation80-82,Citation85,Citation89,Citation91,Citation92 Four studies showed that being knowledgeable about the vaccine or the infectious disease had a positive association with vaccination.Citation80,Citation85,Citation91,Citation92 Seven studies described the reasons why people did not get vaccinated; these included forgetting about the vaccine,Citation36,Citation40 not being aware of an existing vaccine,Citation43 and lack of knowledge/understanding of the vaccine or the disease.Citation45,Citation66,Citation78,Citation85 Six studies Citation39,Citation47,Citation67,Citation80,Citation81,Citation92 found that being exposed to vaccine-related information through television, social media, leaflets, or mail notifications was positively associated or correlated with vaccination. However, in one study from the HCP perspective, nurses expressed that bad media coverage related to the vaccine could also be a barrier to vaccination.Citation54 From the individual perspective, personal knowledge of someone who was at risk for a vaccine-preventable diseaseCitation73 or who had the diseaseCitation43 was positively associated with vaccination. From the provider perspective, a lack of clear information on a vaccination campaign or on official recommendations was reported to hinder trust and limit vaccination promotion to patients.Citation59,Citation82
Perceived individual risk of the infectious disease or its severity was positively associated with vaccine uptake.Citation36,Citation39,Citation40,Citation43,Citation55,Citation59,Citation78,Citation80,Citation82,Citation84-89,Citation92 The perceived risk of disease was associated with increased vaccination in three studies.Citation43,Citation89,Citation92 Conversely, when individuals did not consider themselves at risk for the disease, it was associated with non-vaccination.Citation36,Citation43,Citation84,Citation89 Perceptions of the severity of pneumonia were associated with pneumococcal vaccination,Citation87 while perceptions that shingles or influenza infections were mild correlated with non-vaccination.Citation43,Citation89 As expected, believing vaccination to be “important” was associated with uptake,Citation80 whereas those who did not believe in vaccines was associated with non-vaccination.Citation86 Feeling healthy, feeling too old, or believing that illness is inevitable were included as reasons for not seeing the necessity of vaccination.Citation39,Citation55,Citation89 From the provider perspective, a study of German HCPs found that they may not recommend vaccination if they think patients are not at risk,Citation82 and in Italy, only half of surveyed GPs felt influenza vaccination was a priority.Citation59
A primary perceived barrier to vaccination is the experience or expectation of side effects. Across 16 studies, previous experience of vaccine-related side effects or fear of vaccines was shown to negatively influence a patient’s vaccination status.Citation39,Citation40,Citation43,Citation45,Citation54,Citation55,Citation61,Citation66,Citation69,Citation82-86,Citation89,Citation92 Fear of side effects or the belief that the vaccine had an unfavorable risk-benefit balance was associated with non-vaccination in 10 studies. Citation39,Citation43,Citation45,Citation55,Citation61,Citation69,Citation85,Citation86,Citation89,Citation92 In three studies, individuals reported a previous adverse reaction to a vaccine, and in each case this was shown to impact influenza vaccination uptake.Citation40,Citation45,Citation83 From the provider perspective, GPs in Germany who did not perceive that the “benefit of officially recommended pneumococcal vaccine exceeds its potential harms” were statistically less likely to advise vaccination.Citation82 Also from the provider perspective, patients’ fear of a vaccine’s side effects was identified by nurses in Israel as a barrier to vaccination.Citation54
Unsurprisingly, perceived benefits of vaccination were associated with higher vaccination uptake in 15 studies.Citation43,Citation45,Citation47,Citation54,Citation66,Citation69,Citation71,Citation78,Citation82,Citation83,Citation85,Citation86,Citation88,Citation91,Citation92 Several studies demonstrated that a perception of benefit for oneself or for others,Citation47,Citation92 perceived effectiveness,Citation69,Citation85 and thinking that vaccination is a good prevention toolCitation71 had a positive influence on vaccination rates. In contrast, doubts about a vaccine’s effectiveness discouraged patients from being vaccinated.Citation86 Effectiveness or lack of effectiveness was stated as a main reason for getting vaccinated or not getting vaccinated, respectively, in several analyses of patient-reported data.Citation45,Citation78,Citation88 Several studies reported the provider perspective on this factor. Among HCPs in Japan, belief that the benefits of pneumococcal revaccination exceed the risks caused them to administer the second dose of the vaccine to their adult patients.Citation91 Conversely, a common explanation given by German GPs for not advising vaccination was “doubts on its effectiveness.”Citation82 A similar lack of faith in the effectiveness of vaccination hindered patient vaccination, as reported by nurses in Israel.Citation54
Discussion
Based on 61 included studies, we found that sociodemographic factors (economic status, age, education, and household composition), health-related factors (comorbidities and health care consumption), and attitudinal factors (self-efficacy, provider or other recommendation, and awareness of the disease and respective vaccination) all played a part in routine adult vaccination uptake.
Among the determinants covered in this review, several stood out as being consistent drivers of or barriers to vaccination. Attitudinal factors, regardless of study design and setting, were the most consistent factor category that demonstrated an association with higher vaccine uptake. Self-efficacy, a recommendation to vaccinate, awareness of the vaccine and the disease it prevents, understanding the importance of vaccination based on disease severity, and understanding the benefits of vaccination were all associated with increased vaccination uptake. Discrete choice experiments like the one described by de Bekker-Grob et al. 2018 have shown that individual attitudinal factors influence vaccine acceptance even more than vaccine characteristics.Citation83 The impact of such factors can be maximized by HCPs focusing on educating individuals who have not been previously vaccinated or who have experienced side effects. Recommendations to vaccinate from HCPs have consistently been found to be important across the reviewed literature. To help increase provider recommendations, educational initiatives targeting HCPs both practicing and during academic studies prior to practice could help them understand how important their role is in vaccination and could be used to improve communication tactics with patients to increase vaccine confidence.Citation94 Simplification of vaccination guidelines may also facilitate recommendations to vaccinate, as described in an analysis of the cost-effectiveness of pneumococcal vaccination of adults aged 50–64 years under different scenarios, including universal vaccination based on age regardless of comorbidity status.Citation95
Within the health status category, health care consumption consistently had a positive impact on vaccination, which is important because increased interactions with HCPs may result in more consistent recommendations. Studies of individuals with comorbidities commonly attributed higher vaccination uptake in this group to increased health care consumption and thus increased opportunities for both recommendation and actual vaccination.Citation32,Citation33,Citation40,Citation70,Citation74
For the sociodemographic factors, affordability and insurance coverage consistently had a positive impact on vaccination. Increasing access to vaccination by ensuring affordability, either through insurance coverage or by publicly funding national immunization programs, will remove at least some of the cost barriers. Nationwide, government-subsidized vaccination policies have been shown to increase adult vaccine uptake in the United Kingdom and Spain.Citation96 However, public programs are lacking in many countries for older adults.
Studies on ease of access found that convenience, as described by both individual adults and HCPs, was a consistent facilitator of vaccination uptake. Measures of convenience included geographical proximity (e.g., in-house vaccine administration, a vaccine clinic close to home) and procedural simplicity (e.g., priority waiting lines, ready vaccine availability, ambulatory vs. inpatient setting). Policy makers can maximize convenience for vaccine recipients by expanding the scope of practice laws to allow for a broader range of vaccinators, such as pharmacists, which has been found to increase vaccination coverage rates, in part due to increased convenience with longer hours of operation.Citation97–99 Geographical proximity of local pharmacies should also be considered, as it may explain why some studies found vaccination rates to be higher in urban areas.
Our review consistently highlighted that there is an important need for targeted vaccination campaigns for older adults from select population groups, specifically racial or ethnic minority groups and foreign-born persons. Undervaccination of the older adults in these groups has been documented in other reviews at both national (United States)Citation100 and global levels.Citation96,Citation101,Citation102 Reaching these groups with COVID-19 vaccines has also been a challenge,Citation103 and although this was out of scope for the current review, it highlights the importance of increased support for different types of communities. Strategies proposed for reaching individuals in these types of communities include: (i) at the individual level, HCP efforts to provide accurate information and correct misconceptions around vaccines, establishing long-term trusted relationships with HCPs, and having tailored conversations the include a sympathetic exploration of patient-related health beliefs; (ii) at the health care system level, implementing vaccination reminders and providing translated written information; and (iii) at the policy/governance level, addressing issues of access including proximity, convenience, and cost.Citation102
Many other factors reviewed in this study showed mixed results, in that they sometimes had a positive association with vaccination uptake and other times a negative association. Sociodemographic factors with mixed findings included economic status, age, education level, household composition, and employment status. Across these factor categories there was much heterogeneity in the studies, limiting the comparability, and both local context and individual study definitions must be considered to further understand the mixed results. For example, two employment status studies found lower vaccination rates in regions with higher unemployment rates,Citation52,Citation65 while other studies in this category found higher vaccination rates in those labeled unemployed. These findings must be considered in light of the fact that individuals in the included studies are at an age where retirement comes into play, so employment status may not be as important as in younger adults. Also, employment status is closely linked with educational levels and thus socioeconomic status, so it may be difficult to obtain clear findings on each of these individual factors in the absence of studies designed to mitigate the confounding among them. For example, current income may not reflect the previous earning potential of retirement age subjects,Citation104 and thus their actual socioeconomic status may differ from their status as defined by current employment or income level.
Similarly, educational level is determined at a much earlier stage of life than that being assessed in this review,Citation40 meaning that its effects on health care decisions such as vaccination may be indirect. In addition, as noted by Kwon et al., although higher education and household income ensure greater access to health services, greater wealth also allows individuals in this socioeconomic class to live alone more frequently, which introduces the role of household composition.Citation37 At the same time, educational attainment is often associated with greater health literacy and greater participation in technical occupations,Citation72,Citation104 both of which tend to ensure that people with more education are exposed to information about and opportunities for vaccination. In the case of pneumococcal disease, one concern that has been raised is that in communities with lower educational attainment, and correspondingly low vaccine coverage rates, individuals tend to also have increased risk of disease or disease complications.Citation105 Also in these communities, pediatric pneumococcal vaccine coverage may be lower, and in the context of a known protective community benefit for older adults,Citation106 this can create infection “reservoirs” leading to some of the health disparities commonly linked to socioeconomic status.
Studies of economic status (i.e., income level, social class, and deprivation status) showed a mixed effect with both positive and negative associations with vaccination uptake. These variations existed even within different studies conducted in the same country but in different regions; for example, in both China and Italy, different studies in our review concluded that having a higher income status was associated with increased vaccination uptake in some studies and low uptake in other studies. There are several possible confounding variables that may affect economic status associations. For example, higher income groups may have greater exposure to anti-vaccination campaigns that result in lower uptake or greater access to health care resources (more HCP recommendations to vaccinate) that result in higher uptake. On the other hand, low-income groups may more readily qualify for state-subsidized insurance or be more likely to take advantage of government funded vaccination programs, both of which were found in this review to lead to better vaccination uptake. Ang et al. 2017 described conflicting evidence on economic status from various parts of the world and concluded that the association between income and vaccination has to be examined in the context of “financing policy,” i.e., how the cost of vaccination is covered.Citation41 Free (government-subsidized) vaccination or free access to vaccination via insurance should offset the effects of income. However, McLaughlin et al. 2019 point out the clear relationship between higher pneumococcal vaccination uptake and increasing household income in the United States, despite the fact that all US adults aged ≥65 have access to the vaccine with zero out-of-pocket costs due to Medicare coverage.Citation105 They conclude, along with Abbas et al. 2018, that the relationship between local socioeconomic measures and vaccination outcomes is complex, encompassing not only the cost of vaccination but also factors such as transportation and the ability to take time off from work.Citation105,Citation107
The impact of age on the uptake rate of vaccinations was found to be somewhat dependent upon the vaccine, with both influenza and pneumococcal vaccines having increased uptake in individuals of more advanced age within the older adult age groups (e.g., adults 70 to 75 years old demonstrated higher uptake than adults aged 65 to 69 years old). Of the vaccine-preventable diseases in older adults, pneumococcal disease and influenza have been found to cause the highest disease burden compared to herpes zoster and pertussis,Citation108 which may be prompting stronger recommendations from HCPs and greater overall disease awareness for individuals, which were factors our review found to be consistently associated with increasing vaccination uptake.
Among the factors related to health status, comorbidities and self-rated health were found to have mixed effects on vaccination uptake. Comorbidities (i.e., higher comorbidity score or a greater number of comorbidities) were found to be associated with greater vaccination uptake in 13 out of 15 studies. Of the two studies presenting the opposing results, one reported a small effect size (5% decrease in odds of influenza vaccination per unit increase in comorbidity score)Citation75 and the other was confined to a single comorbidity, asthma.Citation42 Thus, while there were some outliers among the results, comorbidities might be expected to be positively associated with vaccination, as studies have found that individuals with comorbidities may be disproportionately affected by influenza and pneumococcal infections;Citation109,Citation110 additionally, care for their conditions may result in higher healthcare consumption, which our review found to be consistently independently positively associated with vaccination uptake.
With regard to self-rated health, the mixed findings were observed across different world regions, suggesting that attitudes about personal health and the need for vaccination are not based in individual cultures. When poor self-rated health predicted vaccination uptake, study authors attributed it to the presence of comorbidities, which would prompt an older individual to be vaccinated,Citation70 or conversely, to older adults who regarded themselves as healthy lacking the motivation to receive a vaccination.Citation37 When good self-rated health predicted vaccination uptake, it was attributed to a positive attitude toward preventive health services and/or a greater inclination to maintain physical well-being.Citation41,Citation50
The factors that exhibited mixed results in our review highlight some of the gaps in evidence regarding adult vaccination. One that was alluded to above is the need for studies that analyze individual factors simultaneously in a way that addresses the confounding among them. Such studies can help to dissect the interplay between factors such as age and employment status, and socioeconomic status and education level. Another need is for studies that examine regional context more closely, i.e., geographical and cultural specificities, as well as features of local and national health care systems that either promote or discourage adult vaccination. An example of this is an analysis by La et al., who assessed vaccination by state within the United States and found that state-level variations in vaccination coverage persisted even after adjusting for individual-level factors associated with vaccination.Citation111 Finally, there is a lack of interventional data on many of the factors assessed in this review. The included studies were all observational, and there is a need for more information on implementation strategies that will effectively maximize adult vaccination rates.
This study has several limitations related to its design. The field of adult vaccination is a broad one, and only studies identified by our search terms (see Supplementary Table S1) were included; other studies that reported on drivers of and barriers to adult vaccination may be present in the literature and offer additional insights into this topic. Because the majority of included studies reported on influenza vaccination, the findings on influenza are more robust than for pneumococcal, herpes zoster, and tetanus vaccination. Heterogeneity of the study designs and settings, in terms of scope (local vs. national), national economic status, and national vaccination practices, precluded a meta-analysis and presents a caveat when grouping the results of different studies. In addition, data on adult vaccination rates are lacking in many parts of the world, so the current literature is, by definition, an incomplete dataset. Finally, the determinants of uptake of routine older adult vaccines are multifactorial and interrelated, so causality of individual factors cannot be inferred from a topical synthesis such as this one.
In conclusion, adult vaccination is becoming a cornerstone of preventive care in an aging global population.Citation112,Citation113 This narrative synthesis of the literature on factors affecting vaccination uptake in older adults provides insights into the best ways to improve vaccination coverage. Attitudinal factors were the factors most consistently associated with vaccination status, which suggests that awareness and education campaigns for both individuals and HCPs might be important initiatives to increase vaccination coverage. However, there is still a need for increased understanding of factors that impact vaccine uptake, which is critical for guiding decision makers toward using their resources for evidence-based practices to increase vaccine uptake in older adult populations.
Supplemental Material
Download Zip (152.1 KB)Acknowledgement
The authors thank Melissa Stauffer, PhD, in collaboration with ScribCo, for medical writing assistance.
Disclosure statement
ALE is currently an employee at Merck Sharp & Dohme LLC, a subsidiary of Merck & Co, Inc., Rahway, NJ, USA and a shareholder in Merck & Co., Inc., Rahway, NJ, USA. The company manufactures and sells vaccines used in routine immunization programs globally. MN was an employee at Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA and a shareholder in Merck & Co., Inc., Rahway, NJ, USA when the study was performed. JB reported that the International Federation on Aging has agreements with Bayer, AbbVie, BioGen, Pfizer Inc., GSK, Seqirus, and Merck & Co., Inc.
Supplementary material
Supplemental data for this article can be accessed on the publisher’s website at https://doi.org/10.1080/21645515.2022.2127290
Additional information
Funding
References
- United Nations. Department of economic and social affairs, population division. World population ageing 2019: Highlights (ST/ESA/SER.A/430). New York: United Nations.
- World Health Organization. Ageing and Health. [accessed 2022 Apr 13]. https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
- Centers for Disease Control and Prevention. Flu & People 65 Years and Older [accessed 2022 Mar 1]. https://www.cdc.gov/flu/highrisk/65over.htm.
- Haq K, McElhaney JE. Immunosenescence: influenza vaccination and the elderly. Curr Opin Immunol. 2014 Aug;29:1–13. doi:10.1016/j.coi.2014.03.008.
- Remy V, Zollner Y, Heckmann U. Vaccination: the cornerstone of an efficient healthcare system. J Mark Access Health Policy. 2015;3:27041. doi:10.3402/jmahp.v3.27041.
- Reed C, Kim IK, Singleton JA, Chaves SS, Flannery B, Finelli L, Fry A, Burns E, Gargiullo P, Jernigan D, et al. Estimated influenza illnesses and hospitalizations averted by vaccination--United States, 2013-14 influenza season. MMWR Morb Mortal Wkly Rep. 2014 Dec 12;63(49):1151–54.
- Scuffham PA, West PA. Economic evaluation of strategies for the control and management of influenza in Europe. Vaccine. 2002 Jun 7;20(19–20):2562–78. doi:10.1016/S0264-410X(02)00154-8.
- Centers for Disease Control and Prevention. Recommended Adult Immunization Schedule for ages 19 years or older, United States. 2021 [accessed 2021 Jun 12]. https://www.cdc.gov/vaccines/schedules/hcp/imz/adult.html.
- European Centre for Disease Prevention and Control. Vaccine schedules in all countries in the EU/EEA. [accessed 2022 Mar 21]. https://vaccine-schedule.ecdc.europa.eu/.
- Sauer M, Vasudevan P, Meghani A, Luthra K, Garcia C, Knoll MD, Privor-Dumm L. Situational assessment of adult vaccine preventable disease and the potential for immunization advocacy and policy in low- and middle-income countries. Vaccine. 2021 Mar 12;39(11):1556–64. doi:10.1016/j.vaccine.2021.01.066.
- Ott JJ, Klein Breteler J, Tam JS, Hutubessy RC, Jit M, de Boer MR. Influenza vaccines in low and middle income countries: a systematic review of economic evaluations. Hum Vaccin Immunother. 2013 Jul;9(7):1500–11. doi:10.4161/hv.24704.
- World Health Organization. Vaccines against influenza, WHO position paper. Weekly Epidemiological Rec. 2012;87(47):461–76.
- World Health Organization. Varicella and herpes zoster vaccines: wHO position paper. Weekly Epidemiological Rec. 2014;89(25):265–88.
- World Health Organization. Considerations for pneumococcal vaccination in older adults. Weekly Epidemiological Rec. 2021;96(23):217–28.
- Ortiz JR, Neuzil KM. Influenza immunization in low- and middle-income countries: preparing for next-generation influenza vaccines. J Infect Dis. 2019 Apr 8;219(Suppl_1):S97–S106. doi:10.1093/infdis/jiz024.
- US Department of Health and Human Services. Immunization and infectious diseases: objectives. [accessed 2022 Jul 1]. https://www.healthypeople.gov/2020/topics-objectives/topic/immunization-and-infectious-diseases.
- Lu PJ, Hung MC, Srivastav A, Grohskopf LA, Kobayashi M, Harris AM, Dooling KL, Markowitz LE, Rodriguez-Lainz A, Williams WW, et al. Surveillance of vaccination coverage among adult populations —United States, 2018. MMWR Surveill Summ. 2021 May 14;70(3):1–26. doi:10.15585/mmwr.ss7003a1.
- World Health Organization. Seasonal vaccination policies and coverage in the European Region. [accessed 2022 Dec 1]. https://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination/seasonal-vaccination-policies-and-coverage-in-the-european-region.
- Council of the European Union. Council Recommendation of 22 December 2009 on seasonal influenza vaccination. [accessed 2022 Mar 21]. https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32009H1019&from=EN.
- Jorgensen P, Mereckiene J, Cotter S, Johansen K, Tsolova S, Brown C. How close are countries of the WHO European Region to achieving the goal of vaccinating 75% of key risk groups against influenza? Results from national surveys on seasonal influenza vaccination programmes, 2008/2009 to 2014/2015. Vaccine. 2018 Jan 25;36(4):442–52. doi:10.1016/j.vaccine.2017.12.019.
- European Centre for Disease Prevention and Control. Seasonal influenza vaccination and antiviral use in EU/EEA Member States: overview of vaccine recommendations for 2017–2018 and vaccination coverage rates for 2015–2016 and 2016–2017 influenza seasons. [accessed 2022 Mar 21]. https://www.ecdc.europa.eu/sites/default/files/documents/seasonal-influenza-antiviral-use-2018.pdf.
- Badmus D, Menzies R. Using general practice data to monitor influenza vaccination coverage in the medically at risk: a data linkage study. BMJ Open. 2019 Sep 17;9(9):e031802. doi:10.1136/bmjopen-2019-031802.
- Wu S, Su J, Yang P, Zhang H, Li H, Chu Y, Hua W, Li C, Tang Y, Wang Q, et al. Factors associated with the uptake of seasonal influenza vaccination in older and younger adults: a large, population-based survey in Beijing, China. BMJ Open. 2017 Sep 25;7(9):e017459. doi:10.1136/bmjopen-2017-017459.
- Taheri Tanjani P, Babanejad M, Najafi F. Influenza vaccination uptake and its socioeconomic determinants in the older adult Iranian population: a national study. Am J Infect Control. 2015 May 1;43(5):e1–5. doi:10.1016/j.ajic.2015.02.001.
- Shapiro GK, Gottfredson N, Leask J, Wiley K, Ganter-Restrepo FE, Jones SP, Menning L, Brewer NT. COVID-19 and missed or delayed vaccination in 26 middle- and high-income countries: an observational survey. Vaccine. 2022 Feb 7;40(6):945–52. doi:10.1016/j.vaccine.2021.12.041.
- Murray E, Bieniek K, Del Aguila M, Egodage S, Litzinger S, Mazouz A, Mills H, Liska J. Impact of pharmacy intervention on influenza vaccination acceptance: a systematic literature review and meta-analysis. Int J Clin Pharm. 2021 Oct;43(5):1163–72. doi:10.1007/s11096-021-01250-1.
- Jacobson Vann JC, Jacobson RM, Coyne-Beasley T, Asafu-Adjei JK, Szilagyi PG. Patient reminder and recall interventions to improve immunization rates. Cochrane Database Syst Rev. 2018 Jan 18;1(1):Cd003941. doi:10.1002/14651858.CD003941.pub3.
- Travers JL, Schroeder KL, Blaylock TE, Stone PW. Racial/ethnic disparities in influenza and pneumococcal vaccinations among nursing home residents: a systematic review. Gerontologist. 2018 Jul 13;58(4):e205–e217. doi:10.1093/geront/gnw193.
- Guzman-Holst A, DeAntonio R, Prado-Cohrs D, Juliao P. Barriers to vaccination in Latin America: a systematic literature review. Vaccine. 2020 Jan 16;38(3):470–81. doi:10.1016/j.vaccine.2019.10.088.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, Britten N, Roen K, and Duffy S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme. 2006. Published Last Modified Date|. Accessed Dated Accessed|. https://www.lancaster.ac.uk/media/lancaster-university/content-assets/documents/fhm/dhr/chir/NSsynthesisguidanceVersion1-April2006.pdf.
- Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, Moher D, Peters MDJ, Horsley T, Weeks L, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Intern Med. 2018 Oct 2;169(7):467–73. doi:10.7326/M18-0850.
- Cano Gutierrez C, Reyes-Ortiz C, Borda MG, Arciniegas A. Self-Reported vaccination in the elderly: sABE Bogota study, Colombia. Colomb Med (Cali). 2016 Mar 30;47(1):25–30. doi:10.25100/cm.v47i1.2107.
- Chang YC, Tung HJ, Hsu SW, Chen L-S, Kung P-T, Huang K-H, Chiou S-J, Tsai W-C. Use of seasonal influenza vaccination and its associated factors among elderly people with disabilities in Taiwan: a population-based study. PLoS One. 2016;11(6):e0158075. doi:10.1371/journal.pone.0158075.
- Dominguez A, Soldevila N, Toledo D, Godoy P, Castilla J, Force L, Morales M, Mayoral JM, Egurrola M, Tamames S, et al. Factors associated with influenza vaccination of hospitalized elderly patients in Spain. PLoS One. 2016;11(1):e0147931. doi:10.1371/journal.pone.0147931.
- Fabiani M, Riccardo F, Di Napoli A, Gargiulo L, Declich S, Petrelli A. Differences in influenza vaccination coverage between adult immigrants and Italian citizens at risk for influenza-related complications: a cross-sectional study. PLoS One. 2016;11(11):e0166517. doi:10.1371/journal.pone.0166517.
- Giese C, Mereckiene J, Danis K, O’Donnell J, O’Flanagan D, Cotter S. Low vaccination coverage for seasonal influenza and pneumococcal disease among adults at-risk and health care workers in Ireland, 2013: the key role of GPs in recommending vaccination. Vaccine. 2016 Jul 12;34(32):3657–62. doi:10.1016/j.vaccine.2016.05.028.
- Kwon DS, Kim K, Park SM. Factors associated with influenza vaccination coverage among the elderly in South Korea: the Fourth Korean National Health and Nutrition Examination Survey (KNHANES IV). BMJ Open. 2016 Dec 28;6(12):e012618. doi:10.1136/bmjopen-2016-012618.
- Li T, Lv M, Lei T, Wu J, Pang X, Deng Y, Xie Z. Who benefits most from influenza vaccination policy: a study among the elderly in Beijing, China. Int J Equity Health. 2016 Mar 8;15:45. doi:10.1186/s12939-016-0332-x.
- Lv M, Fang R, Wu J, Pang X, Deng Y, Lei T, Xie Z. The free vaccination policy of influenza in Beijing, China: the vaccine coverage and its associated factors. Vaccine. 2016 Apr 19;34(18):2135–40. doi:10.1016/j.vaccine.2016.02.032.
- Neves RG, Duro SM, Tomasi E. Influenza vaccination among elderly in Pelotas-RS, Brazil, 2014: a population-based study. Epidemiol Serv Saude. 2016;25(4):755–66. doi:10.5123/S1679-49742016000400009.
- Ang LW, Cutter J, James L, Goh KT. Factors associated with influenza vaccine uptake in older adults living in the community in Singapore. Epidemiol Infect. 2017 Mar;145(4):775–86. doi:10.1017/S0950268816002491.
- Chiu APY, Dushoff J, Yu D, He D. Patterns of influenza vaccination coverage in the United States from 2009 to 2015. Int J Infect Dis. 2017 Dec;65:122–27. doi:10.1016/j.ijid.2017.10.004.
- Valente N, Lupi S, Stefanati A, Cova M, Sulcaj N, Piccinni L, Gabutti G. Evaluation of the acceptability of a vaccine against herpes zoster in the over 50 years old: an Italian observational study. BMJ Open. 2016 Oct 18;6(10):e011539. doi:10.1136/bmjopen-2016-011539.
- Dios-Guerra C, Carmona-Torres JM, Lopez-Soto PJ, Morales-Cane I, Rodriguez-Borrego MA. Prevalence and factors associated with influenza vaccination of persons over 65 years old in Spain (2009-2014). Vaccine. 2017 Dec 18;35(51):7095–100. doi:10.1016/j.vaccine.2017.10.086.
- Ganczak M, Gil K, Korzen M, Bazydlo M. Coverage and influencing determinants of influenza vaccination in elderly patients in a country with a poor vaccination implementation. Int J Environ Res Public Health. 2017 Jun 20;14(6):665. doi:10.3390/ijerph14060665.
- Hellfritzsch M, Thomsen RW, Baggesen LM, Larsen FB, Sorensen HT, Christiansen CF. Lifestyle, socioeconomic characteristics, and medical history of elderly persons who receive seasonal influenza vaccination in a tax-supported healthcare system. Vaccine. 2017 Apr 25;35(18):2396–403. doi:10.1016/j.vaccine.2017.03.040.
- Praphasiri P, Ditsungnoen D, Sirilak S, Rattanayot J, Areerat P, Dawood FS, Lindblade KA. Predictors of seasonal influenza vaccination among older adults in Thailand. PLoS One. 2017;12(11):e0188422. doi:10.1371/journal.pone.0188422.
- Shin HY, Hwang HJ, Chung JH. Factors influencing influenza vaccination among patients with chronic obstructive pulmonary disease: a population-based cross-sectional study. Asia Pac J Public Health. 2017 Oct;29(7):560–68. doi:10.1177/1010539517735415.
- Ward C, Byrne L, White JM, Amirthalingam G, Tiley K, Edelstein M. Sociodemographic predictors of variation in coverage of the national shingles vaccination programme in England, 2014/15. Vaccine. 2017 Apr 25;35(18):2372–78. doi:10.1016/j.vaccine.2017.03.042.
- Ang LW, Cutter J, James L, Goh KT. Epidemiological characteristics associated with uptake of pneumococcal vaccine among older adults living in the community in Singapore: results from the National Health Surveillance Survey 2013. Scand J Public Health. 2018 Mar;46(2):175–81. doi:10.1177/1403494817720105.
- Arghittu A, Dettori M, Masia MD, Azara A, Dempsey E, Castiglia P. Social deprivation indexes and anti-influenza vaccination coverage in the elderly in Sardinia, Italy, with a focus on the Sassari municipality. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E45–E50. doi:10.15167/2421-4248/jpmh2018.59.4s2.1077.
- Bechini A, Pieralli F, Chellini E, Martini A, Dugheri G, Crescioli F, Scatena T, Baggiani L, Lillini R, Fiaschi P, et al. Application of socio-economic-health deprivation index, analysis of mortality and influenza vaccination coverage in the elderly population of Tuscany. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E18–E25. doi:10.15167/2421-4248/jpmh2018.59.4s2.1116.
- Byeon KH, Kim J, Choi B, Choi BY. The coverage rates for influenza vaccination and related factors in Korean adults aged 50 and older with chronic disease: based on 2016 Community Health Survey data. Epidemiol Health. 2018;40:e2018034. doi:10.4178/epih.e2018034.
- Ellen M. Factors that influence influenza vaccination rates among the elderly: nurses’ perspectives. J Nurs Manag. 2018 Mar;26(2):158–66. doi:10.1111/jonm.12528.
- Erdogdu H, Catak B. Influenza, pneumococcal and herpes zoster vaccination rates amongst people aged 65 years and older and related factors. Turk Geriatri Dergisi. 2018;21:498–506.
- Fortunato F, Iannelli G, Cozza A, Del Prete M, Pollidoro FV, Cocciardi S, DI Trani M, Martinelli D, Prato R. Local deprivation status and seasonal influenza vaccination coverage in adults ≥ 65 years residing in the Foggia municipality, Italy, 2009-2016. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E51–E64. doi:10.15167/2421-4248/jpmh2018.59.4s2.1167.
- Heins MJ, Hooiveld M, Korevaar JC. Healthy elderly and influenza vaccination. Hum Vaccin Immunother. 2018;14(12):2987–89. doi:10.1080/21645515.2018.1504525.
- Lai A, Pisanu L, Casula L, Minerba L, Lillini R, Vercelli M. Influenza vaccination coverage and deprivation among the elderly in the municipality of Cagliari: results and perspectives. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E65–E70. doi:10.15167/2421-4248/jpmh2018.59.4s2.1197.
- Levi M, Bonanni P, Biffino M, Conversano M, Corongiu M, Morato P, Maio T. Influenza vaccination 2014–2015: results of a survey conducted among general practitioners in Italy. Hum Vaccin Immunother. 2018 Jun 3;14(6):1342–50. doi:10.1080/21645515.2018.1430543.
- Restivo V, Cernigliaro A, Palmeri S, Sinatra I, Costantino C, Casuccio A. The Socio-Economic Health Deprivation Index and its association with mortality and attitudes towards influenza vaccination among the elderly in Palermo, Sicily. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E26–E30. doi:10.15167/2421-4248/jpmh2018.59.4s2.1074.
- Rey D, Fressard L, Cortaredona S, Bocquier A, Gautier A, Peretti-Watel P, Verger P. Vaccine hesitancy in the French population in 2016, and its association with vaccine uptake and perceived vaccine risk–benefit balance. Euro Surveill. 2018 Apr;23(17). doi:10.2807/1560-7917.ES.2018.23.17.17-00816.
- Seo J, Lim J. Trends in influenza vaccination coverage rates in South Korea from 2005 to 2014: effect of public health policies on vaccination behavior. Vaccine. 2018 Jun 14;36(25):3666–73. doi:10.1016/j.vaccine.2018.05.024.
- Stefanati A, Lupi S, Lillini R, Matteo G, Perrone P, Masetti G, Brosio F, Ferretti S, Gabutti G. Identifying Ferrara’s elderly people with low influenza immunization rates: the contribution of a local socio-economic deprivation index. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E38–E44. doi:10.15167/2421-4248/jpmh2018.59.4s2.1033.
- Vercelli M, Lillini R, Arata L, Zangrillo F, Bagnasco A, Sasso L, Magliani A, Gasparini R, Amicizia D, Panatto D, et al. Analysis of influenza vaccination coverage among the elderly in Genoa (Italy) based on a deprivation index, 2009-2013. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E11–E17. doi:10.15167/2421-4248/jpmh2018.59.4s2.1171.
- Vukovic V, Lillini R, Asta F, Chini F, De Waure C. Analysis of influenza vaccination coverage among the elderly living in Rome, based on a deprivation index, 2009-2013. J Prev Med Hyg. 2018 Dec;59(4 Suppl 2):E31–E37. doi:10.15167/2421-4248/jpmh2018.59.4s2.1142.
- Alotaibi FY, Alhetheel AF, Alluhaymid YM, Alshibani MG, Almuhaydili AO, Alhuqayl TA, Alfayez FM, Almasabi AA. Influenza vaccine coverage, awareness, and beliefs regarding seasonal influenza vaccination among people aged 65 years and older in Central Saudi Arabia. Saudi Med J. 2019 Oct;40(10):1013–18. doi:10.15537/smj.2019.11.24587.
- Biasio LR, Giambi C, Fadda G, Lorini C, Bonaccorsi G, D’Ancona F. Validation of an Italian tool to assess vaccine literacy in adulthood vaccination: a pilot study. Ann Ig. 2020 May-Jun;32(3):205–22. doi:10.7416/ai.2020.2344.
- Dardalas I, Pourzitaki C, Manomenidis G, Malliou F, Galanis P, Papazisis G, Kouvelas D, Bellali T. Predictors of influenza vaccination among elderly: a cross-sectional survey in Greece. Aging Clin Exp Res. 2020 Sep;32(9):1821–28. doi:10.1007/s40520-019-01367-4.
- Kajikawa N, Kataoka Y, Goto R, Maeno T, Yokoya S, Umeyama S, Takahashi S, Maeno T. Factors associated with influenza vaccination in Japanese elderly outpatients. Infect Dis Health. 2019 Nov;24(4):212–21. doi:10.1016/j.idh.2019.07.002.
- Portero de la Cruz S, Cebrino J. Trends, coverage and influencing determinants of influenza vaccination in the elderly: a population-based National Survey in Spain (2006-2017). Vaccines (Basel). 2020 Jun 19;8(2). doi:10.3390/vaccines8020327.
- Del Signore C, Hemmendinger A, Khanafer N, Thierry J, Trépo E, Martin Gaujard G, Chapurlat R, Elias C, Vanhems P. Acceptability and perception of the herpes zoster vaccine in the 65 and over population: a French observational study. Vaccine. 2020 Aug 18;38(37):5891–95. doi:10.1016/j.vaccine.2020.07.004.
- Fan J, Cong S, Wang N, Bao H, Wang B, Feng Y, Lv X, Zhang Y, Zha Z, Yu L, et al. Influenza vaccination rate and its association with chronic diseases in China: results of a national cross-sectional study. Vaccine. 2020 Mar 4;38(11):2503–11. doi:10.1016/j.vaccine.2020.01.093.
- Giacomelli A, Galli M, Maggi S, Pagani G, Antonelli Incalzi R, Pedone C, Di Bari M, Noale M, Trevisan C, Bianchi F, et al. Missed opportunities of flu vaccination in Italian target categories: insights from the online EPICOVID 19 Survey. Vaccines (Basel). 2020 Nov 9;8(4):669. doi:10.3390/vaccines8040669.
- Hall LL, Xu L, Mahmud SM, Puckrein GA, Thommes EW, Chit A. A map of racial and ethnic disparities in influenza vaccine uptake in the medicare fee-for-service program. Adv Ther. 2020 May;37(5):2224–35. doi:10.1007/s12325-020-01324-y.
- Lawrence T, Zubatsky M, Meyer D. The association between mental health diagnoses and influenza vaccine receipt among older primary care patients. Psychol Health Med. 2020 Oct;25(9):1083–93. doi:10.1080/13548506.2020.1717557.
- Machado A, Santos AJ, Kislaya I, Larrauri A, Nunes B. Understanding influenza vaccination among Portuguese elderly: the social ecological framework. Health Promot Int. 2020 Dec 1;35(6):1427–40. doi:10.1093/heapro/daaa011.
- Sato APS, Andrade FB, Duarte YAO, Antunes JLF. Vaccine coverage and factors associated with influenza vaccination in the elderly in the city of Sao Paulo, Brazil: SABE Study 2015. Cad Saude Publica. 2020;36 Suppl(2):e00237419. doi:10.1590/0102-311x00237419.
- Yan S, Wang Y, Zhu W, Zhang L, Gu H, Liu D, Zhu A, Xu H, Hao L, Ye C, et al. Barriers to influenza vaccination among different populations in Shanghai. Hum Vaccin Immunother. 2021 May 4;17(5):1403–11. doi:10.1080/21645515.2020.1826250.
- Dominguez A, Soldevila N, Toledo D, Godoy P, Torner N, Force L, Castilla J, Mayoral JM, Tamames S, Martín V, et al. Factors associated with pneumococcal polysaccharide vaccination of the elderly in Spain: a cross-sectional study. Hum Vaccin Immunother. 2016 Jul 2;12(7):1891–99. doi:10.1080/21645515.2016.1149661.
- Klett-Tammen CJ, Krause G, Seefeld L, Ott JJ. Determinants of tetanus, pneumococcal and influenza vaccination in the elderly: a representative cross-sectional study on knowledge, attitude and practice (KAP). BMC Public Health. 2016 Feb 4;16:121. doi:10.1186/s12889-016-2784-8.
- Watanabe K, Asai Y, Tsurikisawa N, Oshikata C, Kaneko T. Factors associated with pneumococcal vaccine uptake in elderly subjects referred to the respiratory department. Nagoya J Med Sci. 2020 Aug;82(3):469–76. doi:10.18999/nagjms.82.3.469.
- Klett-Tammen CJ, Krause G, von Lengerke T, Castell S. Advising vaccinations for the elderly: a cross-sectional survey on differences between general practitioners and physician assistants in Germany. BMC Fam Pract. 2016 Jul 29;17:98. doi:10.1186/s12875-016-0502-3.
- de Bekker-Grob EW, Veldwijk J, Jonker M, Donkers B, Huisman J, Buis S, Swait J, Lancsar E, Witteman CLM, Bonsel G, et al. The impact of vaccination and patient characteristics on influenza vaccination uptake of elderly people: a discrete choice experiment. Vaccine. 2018 Mar 7;36(11):1467–76. doi:10.1016/j.vaccine.2018.01.054.
- Santos AJ, Kislaya I, Machado A, Nunes B. Beliefs and attitudes towards the influenza vaccine in high-risk individuals. Epidemiol Infect. 2017 Jul;145(9):1786–96. doi:10.1017/S0950268817000814.
- Higuchi M, Narumoto K, Goto T, Inoue M. Correlation between family physician’s direct advice and pneumococcal vaccination intention and behavior among the elderly in Japan: a cross-sectional study. BMC Fam Pract. 2018 Sep 5;19(1):153. doi:10.1186/s12875-018-0841-3.
- Rikin S, Scott V, Shea S, LaRussa P, Stockwell MS. Influenza vaccination beliefs and practices in elderly primary care patients. J Community Health. 2018 Feb;43(1):201–06. doi:10.1007/s10900-017-0404-x.
- Sakamoto A, Chanyasanha C, Sujirarat D, Matsumoto N, Nakazato M. Factors associated with pneumococcal vaccination in elderly people: a cross-sectional study among elderly club members in Miyakonojo City, Japan. BMC Public Health. 2018 Oct 12;18(1):1172. doi:10.1186/s12889-018-6080-7.
- Chinzorig T, Sugiyama K, Aida J, Tsuboya T, Osaka K. Are social inequalities in influenza vaccination coverage in Japan reduced by health policy? Prev Med Rep. 2019 Dec;16:100959. doi:10.1016/j.pmedr.2019.100959.
- Teo LM, Smith HE, Lwin MO, Tang WE. Attitudes and perception of influenza vaccines among older people in Singapore: a qualitative study. Vaccine. 2019 Oct 16;37(44):6665–72. doi:10.1016/j.vaccine.2019.09.037.
- Yuruyen M, Ayan G, Demirdag F, Kara Z, Avci S, Yavuzer H, Döventaş A, and Erdincler D. Why is vaccination frequency low in elderly patients? J Clin Anal Med. 2018;9(2):138–42.
- Nakamura A, Kawakami K, Wakana A, Folaranmi TA, Iino T. A Japanese nationwide survey of 23-valent pneumococcal capsular polysaccharide vaccine (PPSV23) revaccination coverage rate among elderly adults aged 65 and older and physician’s attitude. Hum Vaccin Immunother. 2020 Sep 1;16(9):2292–99. doi:10.1080/21645515.2020.1717184.
- Wang Z, Fang Y, Ip M, Lau M, Lau JTF. Facilitators and barriers to completing recommended doses of pneumococcal vaccination among community-living individuals aged >/=65 years in Hong Kong - a population-based study. Hum Vaccin Immunother. 2021 Feb 1;17(2):527–36. doi:10.1080/21645515.2020.1776545.
- The Japanese Association for Infectious Diseases (JAID)Guidance for revaccination of pneumococcal vaccine (revised edition). J Jpn Assoc Infect Dis. 2017;91(4):543–52.
- Kerneis S, Jacquet C, Bannay A, May T, Launay O, Verger P, Pulcini C, Abgueguen P, Ansart S, Bani-Sadr F, et al. Vaccine education of medical students: a Nationwide Cross-sectional Survey. Am J Prev Med. 2017 Sep;53(3):e97–e104. doi:10.1016/j.amepre.2017.01.014.
- Wateska AR, Nowalk MP, Lin CJ, Harrison LH, Schaffner W, Zimmerman RK, Smith KJ. An intervention to improve pneumococcal vaccination uptake in high risk 50-64 year olds vs. expanded age-based recommendations: an exploratory cost-effectiveness analysis. Hum Vaccin Immunother. 2019;15(4):863–72. doi:10.1080/21645515.2018.1564439.
- Bach AT, Kang AY, Lewis J, Xavioer S, Portillo I, Goad JA. Addressing common barriers in adult immunizations: a review of interventions. Expert Rev Vaccines. 2019;18(11):1167–85. doi:10.1080/14760584.2019.1698955.
- Goad JA, Taitel MS, Fensterheim LE, Cannon AE. Vaccinations administered during off-clinic hours at a national community pharmacy: implications for increasing patient access and convenience. Ann Fam Med. 2013;11(5):429–36. doi:10.1370/afm.1542.
- Papastergiou J, Folkins C, Li W, Zervas J. Community pharmacist-administered influenza immunization improves patient access to vaccination. Can Pharm J (Ott). 2014 Nov;147(6):359–65. doi:10.1177/1715163514552557.
- Isenor JE, Edwards NT, Alia TA, Slayter KL, MacDougall DM, McNeil SA, Bowles SK. Impact of pharmacists as immunizers on vaccination rates: a systematic review and meta-analysis. Vaccine. 2016 Nov 11;34(47):5708–23. doi:10.1016/j.vaccine.2016.08.085.
- Elekwachi O, Wingate LT, Clarke Tasker V, Aboagye L, Dubale T, Betru D, Algatan R. A review of racial and ethnic disparities in immunizations for elderly adults. J Prim Care Community Health. 2021 Jan-Dec;12:21501327211014071. doi:10.1177/21501327211014071.
- Nagata JM, Hernandez-Ramos I, Kurup AS, Albrecht D, Vivas-Torrealba C, Franco-Paredes C. Social determinants of health and seasonal influenza vaccination in adults >/=65 years: a systematic review of qualitative and quantitative data. BMC Public Health. 2013 Apr 25;13:388. doi:10.1186/1471-2458-13-388.
- Bhanu C, Gopal DP, Walters K, Chaudhry UAR. Vaccination uptake amongst older adults from minority ethnic backgrounds: a systematic review. PLoS Med. 2021 Nov;18(11):e1003826. doi:10.1371/journal.pmed.1003826.
- Nguyen LH, Joshi AD, Drew DA, Merino J, Ma W, Lo CH, Kwon S, Wang K, Graham MS, Polidori L, et al. Racial and ethnic differences in COVID-19 vaccine hesitancy and uptake. medRxiv. 2021 Feb 28.
- Sangster AV, Barratt JM. Towards ending immunization inequity. Vaccines (Basel). 2021 Nov 24;9(12). doi:10.3390/vaccines9121378.
- McLaughlin JM, Swerdlow DL, Khan F, Will O, Curry A, Snow V, Isturiz RE, Jodar L. Disparities in uptake of 13-valent pneumococcal conjugate vaccine among older adults in the United States. Hum Vaccin Immunother. 2019;15(4):841–49. doi:10.1080/21645515.2018.1564434.
- Tsaban G, Ben-Shimol S. Indirect (herd) protection, following pneumococcal conjugated vaccines introduction: a systematic review of the literature. Vaccine. 2017 May 19;35(22):2882–91. doi:10.1016/j.vaccine.2017.04.032.
- Abbas KM, Kang GJ, Chen D, Werre SR, Marathe A. Demographics, perceptions, and socioeconomic factors affecting influenza vaccination among adults in the United States. PeerJ. 2018;6:e5171. doi:10.7717/peerj.5171.
- Kristensen M, van Lier A, Eilers R, McDonald SA, Opstelten W, van der Maas N, van der Hoek W, Kretzschmar ME, Nielen MM, de Melker HE, et al. Burden of four vaccine preventable diseases in older adults. Vaccine. 2016 Feb 10;34(7):942–49. doi:10.1016/j.vaccine.2015.12.052.
- Shea KM, Edelsberg J, Weycker D, Farkouh RA, Strutton DR, Pelton SI. Rates of pneumococcal disease in adults with chronic medical conditions. Open Forum Infect Dis. 2014 Mar;1(1):ofu024. doi:10.1093/ofid/ofu024.
- Walker TA, Waite B, Thompson MG, McArthur C, Wong C, Baker MG, Wood T, Haubrock J, Roberts S, Gross DK, et al. Risk of severe influenza among adults with chronic medical conditions. J Infect Dis. 2020 Jan 2;221(2):183–90. doi:10.1093/infdis/jiz570.
- La EM, Trantham L, Kurosky SK, Odom D, Aris E, Hogea C. An analysis of factors associated with influenza, pneumoccocal, Tdap, and herpes zoster vaccine uptake in the US adult population and corresponding inter-state variability. Hum Vaccin Immunother. 2018 Feb 1;14(2):430–41. doi:10.1080/21645515.2017.1403697.
- Doherty TM, Del Giudice G, Maggi S. Adult vaccination as part of a healthy lifestyle: moving from medical intervention to health promotion. Ann Med. 2019;51(2):128–40. doi:10.1080/07853890.2019.1588470.
- Tan L. Adult vaccination: now is the time to realize an unfulfilled potential. Hum Vaccin Immunother. 2015;11(9):2158–66. doi:10.4161/21645515.2014.982998.