
ABSTRACT
COVID-19 is a major public health threat associated with increased disease burden, mortality, and economic loss to countries and communities. Safe and efficacious COVID-19 vaccines are key in halting and reversing the pandemic. Low confidence in vaccines has been one of the factors leading to hesitancy. We aimed to assess the COVID-19 vaccine confidence (safety and effectiveness), associated factors, and its effects on vaccine uptake among general community members in Tanzania. This was a community-based cross-sectional survey conducted from December 2021 to April 2022 in six regions of Tanzania mainland and two regions in Zanzibar. Participants were interviewed using an electronic questionnaire. Multiple logistic regression models estimated odds ratios (ORs) and 95% confidence interval (CI) for factors associated with vaccine confidence. All analyses were performed using SPSS version 25.0. The study enrolled 3470 general Tanzanian community members; their mean age was 40.3 (standard deviation ±14.9) years, and 34% were males. The proportion of COVID-19 vaccine confidence was 54.6%. Geographical region, residence area, COVID-19 disease risk perception, and good knowledge of COVID-19 vaccines were significantly associated with COVID-19 vaccine confidence. Confidence in COVID-19 vaccines was associated with over three times higher odds of vaccine uptake. Confidence in COVID-19 vaccines was low in Tanzania. Innovative community engagement strategies and region-specific interventions are needed to improve comprehensive knowledge and address community perceptions and attitudes toward COVID-19 vaccines.
Introduction
Vaccine confidence is an issue of public health concern, especially in the era of emerging and reemerging infectious diseases. It is defined by public perceptions of three components: vaccine safety, effectiveness, and importance.Citation1 Lack of trust and confidence in vaccines is an important determinant of vaccine hesitancy, and it influences uptake, affects national immunization targets, and increases outbreaks of vaccine-preventable diseases.Citation1–3 Hesitancy in available childhood and other vaccines has led to a resurgence of vaccine-preventable diseases such as measles and diarrhea, and in some instances, it has affected polio eradication success efforts, threatening years of progress in the global fight against infectious diseases.Citation4,Citation5 The World Health Organization (WHO) has identified reluctance or refusal to vaccinate as one of the 10 global health security threats in 2019 that need to be tracked and addressed by countries.Citation6
In the era of the COVID-19 pandemic, vaccination is a key intervention in halting and reversing the pandemic.Citation7 Despite evidence of the benefits of the COVID-19 vaccine in averting severe disease, mortality, and community transmission, the uptake is low in African countries.Citation8 While the high uptake of COVID-19 vaccines is high in Europe, America, and South-East Asia where over 100 doses have been administered per 100 population, Sub-Saharan Africa (SSA) countries are lagging in coverage of COVID-19 vaccination, ranging from 40 to 59 doses per 100 population in Eastern African countries including Tanzania.Citation9
COVID-19 vaccines have recently been introduced compared with other vaccines; therefore, public trust and confidence in the new vaccine are important components that influence the uptake of this vaccine. Trust in the product (safety and efficacy) and trust in the government or those who make decisions on vaccine provision have been shown to influence uptake in several settings.Citation2,Citation10 For this, the WHO has called upon African countries to increase vaccination activities six times fold to achieve a herd immunity target of 70% per population.Citation8 Additionally, it has called upon each country to make its target for vaccination coverage.
Tanzania rolled out COVID-19 vaccines later than other East African Community countries due to various factors including inadequate political will and high hesitancy by the public. The first vaccine was officially introduced in July 2021 by H.E. Samia Suluhu Hassan, the President of the United Republic of Tanzania being vaccinated publicly.Citation11 The initial vaccine doses were mainly targeting high-risk populations, including people with comorbidities, the elderly (60 years or more), and health care workers. Later, the eligibility was expanded to include all adults aged more than 18 years. Tanzania is among the countries that have made slow progress in COVID-19 vaccination coverage despite several rounds of campaigns to create awareness and demand. By October 21, 2022, data from the Ministry of Health of Tanzania (MoH) showed that only 44% of the eligible population were fully vaccinated. Studies have shown different reasons for the low uptake of COVID-19 vaccines in SSA including structural, social, and cultural reasons. Specifically, issues around the safety and side effects of vaccines, doubts about the effectiveness of the vaccines, overload and conflicting information from different platforms, misconceptions, and lack of coordinated efforts between stakeholders have been described as the main reasons for vaccine hesitancy and uptake in many African countries including some community members in Tanzania.Citation12
To reach the target by December 2022, the Minister of Health Honorable Ummy A. Mwalimu launched the third round of a massive vaccination campaign along with UN Agencies, Development Partners, and local implementing partners to create awareness and demand with a target to vaccinate 4 million people across all 26 regions of mainland Tanzania.Citation13 Understanding the state of vaccine confidence is, therefore, crucial to inform appropriate interventions and strategies to mitigate vaccine hesitancy in the country. This study assessed confidence in the COVID-19 vaccine safety, effectiveness, associated factors, and its effects on vaccine uptake among general community members in Tanzania.
Materials and methods
Study design, setting, and population
A community-based cross-sectional study was conducted from December 2021 to April 2022. The study was conducted in six (6) regions of mainland Tanzania and two (2) regions of Zanzibar. The regions for the study were selected based on the vaccine wastage rates of September 2021 when the protocol was developed. Two good, two medium, and two poor-performing regions were selected by considering zonal representation. The regions selected in the mainland were Dar es Salaam (Eastern zone), Lindi (Southern zone), Kilimanjaro (Northern zone), Simiyu (Lake zone), Tabora (Western zone), and Mbeya (Southern West Highlands zone). In Zanzibar, Pemba Kaskazini (In Pemba) and Mjini Magharibi (in Unguja) were the study sites. The study population was the general community members across the eight selected regions. Specifically, the general community members included all adult men and women aged 18 years and above, available at a household during data collection, and provided informed consent.
Sample size, sampling, and study procedures
The sample size was calculated using a single proportion formula given as [N = [(Zα/2)2 x p(1-p)]/ε2, where N is the minimum required sample size, Zα/2 is the standard normal value corresponding to the 95% level of confidence, p is the hypothesized proportion of vaccine hesitancy in the general Tanzanian community, and ε is the margin of error. The sample size estimations used a standard normal value of 1.96 under the 95% confidence limit, assumed a 50% proportion of vaccine uptake among the general community members, adding a 20% non-response proportion, and a 3% margin of error. The number was then multiplied by a design effect of two (2) to allow for a complex survey design yielding 2600 participants. After data collection in the first three regions (Dar es Salaam, Mjini Magharibi, and Pemba Kaskazini) it was noted that there was a low uptake of the COVID-19 vaccine than the proportion used in the estimation of sample size. Therefore, the total sample size was increased by 35% in the five remaining regions and Zanzibar, yielding a total of 3470 general community members.
The details of sampling and study procedures have been published elsewhere.Citation14
Measures
The main outcome variable was COVID-19 vaccine confidence. In this study, vaccine confidence was assessed using two components that are safety and effectiveness; ‘COVID-19 vaccines work’ for effectiveness and ‘COVID-19 vaccines are safe for human use’ for safety. Questions were coded using a Likert scale, i.e., strongly agree, agree, neutral, disagree, and strongly disagree. Codes were further categorized into binary components where strongly agree and agree were coded as ‘Yes’ agreeing to the statement that vaccines are safe or effective. Neutral, disagree and strongly disagree were coded as ‘No’ disagreeing with the statements on safety and confidence. To get overall vaccine confidence in safety and effectiveness, a response of ‘Yes’ to both questions pertaining was required.
Knowledge of COVID-19 vaccines was measured using a set of seven questions requiring three responses; yes, no, and don’t know. The questions were ‘COVID-19 vaccines can reduce the risk of being infected?,’ ‘Can a person get infected by vaccination?,’ ‘Can vaccinated person get infected with Covid-19?,’ ‘Covid-19 vaccines can be given to people who had been infected/sick with COVID-19,’ ‘A person who has received COVID-19 vaccine needs to continue following traditional protective measures,’ ‘COVID-19 vaccines can reduce the risk/chance of being infected with COVID-19?,’ ‘COVID-19 vaccines prevent severe infection,’ ‘COVID-19 vaccines reduce deaths due to COVID-19.’ A ‘Yes’ response was given a score of 1 and a ‘No’ or ‘Don’t know’ response was given a score of 0 except for the question; ‘Can a person get infected by vaccination?,’ which was reverse coded. A median score and above was considered good knowledge, and poor knowledge if otherwise.
Vaccine uptake was measured by asking participants if they have taken the COVID-19 vaccine. The question had three responses; ‘I have taken the vaccine,’ ‘I will wait for some time,’ and ‘I will not take the vaccine at all.’ The responses were further coded into ‘yes’ for those who responded, ‘I have taken the vaccine’ and ‘no’ for those who responded, ‘I will wait for some time’ and ‘I will not take the vaccine at all.’ A ‘yes’ response was taken as vaccine uptake.
Data management and analysis
The collected data were transferred from KoboToolbox to an excel spreadsheet. Statistical Package for Social Sciences (SPSS) version 25 was used for data management and analysis. Frequencies and proportions were used to summarize categorical variables and measures of central tendency and dispersion to summarize numerical variables. The chi-square test was used to compare COVID-19 vaccine confidence proportion by geographic region, area residence, sex, age, education level, socio-economic status, perceived risk of COVID-19 infection, and history of COVID-19 infection. A multivariable logistic regression model determined the association between these factors with COVID-19 vaccine confidence. In addition, the model estimated the effect of COVID-19 vaccine confidence on the uptake adjusted for other factors. Statistically significant results were judged at a 5% level (p < .05).
Results
Participants characteristics
A total of 3,503 participants were approached and 3470 (99.1%) agreed to participate and were included in the analysis. The age of the participants ranged from 18 to 91 years, with a mean of 40.3 (SD 14.9) years. Of the 3470 participants, 71.2% were married or cohabiting, 34% were males, 35% had secondary or higher education and were involved in the small-scale business (33%), and farming (27%) for incoming generating activities. Other background characteristics are shown in .
Table 1. Sociodemographic characteristics of study participants (N = 3470).
Awareness and risk perception of COVID-19 disease
More than three-quarters (76.9%) of the 3470 study participants were aware that COVID-19 disease exists in Tanzania. Only 1.9% of all study participants reported ever being infected with COVID-19 disease. Nearly 43.4% perceived not to be at risk of getting COVID-19 infection, 30.3% perceived to be at low risk, and 26.3% to be at medium-very high risk.
Knowledge of COVID-19 vaccines
The majority (93.8%) of the 3470 participants ever heard of COVID-19 vaccines but only 48.4% knew that in Tanzania, all adults above 18 years were eligible to get the COVID-19 vaccine. Nearly 40% of the participants did not know the key advantages of the COVID-19 vaccines, i.e., preventing the chance of getting infected, reducing the risk of severe disease, and reducing the risk of death. Overall, over half, 52.2% of participants had good knowledge of COVID-19 vaccines.
COVID-19 vaccine confidence and perception on COVID-19 vaccines among community members in Tanzania
Of all 3470 participants, 59.9% and 60.9% of participants were confident that the COVID-19 vaccines were effective and safe, respectively. Overall, more than half (54.6%) of the participants had confidence in the COVID-19 vaccine. In addition, 60.3% of participants trusted that the Ministry of Health ensured that the COVID-19 vaccines brought into the country are safe ().
Table 2. Perceptions on COVID-19 vaccines among general community members in Tanzania (N = 3470).
Factors associated with COVID-19 vaccine confidence in Tanzania
Bivariate analysis of COVID-19 vaccine confidence by participants’ characteristics showed a significant association among various factors. Being a male (p = .024), higher education level, being not in a union (single, separated, divorced, and widow) (p = .03), higher level of wealth status, ever being infected with COVID-19 disease, perceiving oneself at risk of COVID-19 disease and having good knowledge on COVID-19 vaccines were significantly associated with having confidence on COVID-19 vaccine ().
Table 3. COVID-19 vaccine confidence among the general community members in Tanzania (N = 3470).
In multivariable analysis, area of residence, COVID-19 disease risk perception, and knowledge of COVID-19 vaccines were significantly associated with COVID-19 vaccine confidence. Participants residing in rural areas had 27% higher odds of having confidence in the COVID-19 vaccine than the ones residing in urban areas (AOR = 1.27, 95% CI 1.05–1.53). The perception of being at risk of acquiring COVID-19 infection was associated with 58% higher odds of having confidence in the vaccine than the ones who did not perceive themselves at risk (AOR = 1.58, 95% CI 1.35–1.85) and those with good knowledge of COVID-19 vaccines had 6.3 times the odds of having confidence in the vaccine than those with poor knowledge (AOR = 6.26, 95% CI 5.35–7.40). In addition, community members who resided in Kilimanjaro, Lindi, Mjini Magharibi, and Pemba Kaskazini had significantly higher odds of having confidence in COVID-19 vaccines than those in Dar es Salaam ().
Table 4. Factors associated with COVID-19 vaccine confidence among general community members in Tanzania (N = 3470).
The effect of COVID-19 vaccine confidence on vaccine uptake
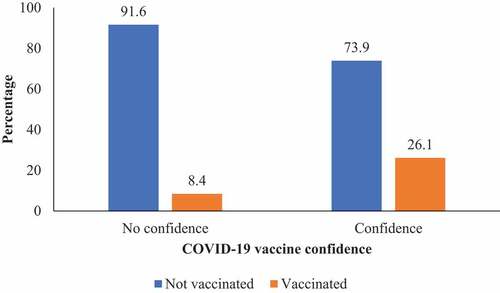
Over a quarter, 26.1% of participants who had confidence in the COVID-19 vaccine were vaccinated compared to 8.4% who had no confidence in the COVID-19 vaccine safety and effectiveness (). A logistic regression analysis showed that adjusted for age, sex, region, residence, disease risk perception, and knowledge of COVID-19 vaccines; participants who had confidence in the COVID-19 vaccine’s safety and effectiveness had nearly four times higher odds of taking the vaccine (OR = 3.9; 95% CI: 3.14–4.74).
Figure 1. Prevalence of COVID-19 vaccine uptake by confidence in vaccine safety and effectiveness among general community members in Tanzania (N = 3470).
Discussion
In this study, we assessed the COVID-19 vaccine confidence on safety and effectiveness and its effect on vaccine uptake among general community members in Tanzania. Overall, 54.6% of the Tanzanians had confidence in both the safety and effectiveness of the vaccine. Geographical regions, residing in rural areas, having a risk perception of acquiring COVID-19 disease, and having good knowledge of COVID-19 vaccines were significant factors associated with COVID-19 vaccine confidence. Importantly, having confidence in the COVID-19 vaccines’ effectiveness and safety increased the odds of higher uptake of the COVID-19 vaccine compared to those who did not have confidence.
The proportion of COVID-19 vaccine confidence (54%) among participants is almost similar to results reported in AustraliaCitation15 whereby, 60% and 20% of participants strongly agreed that vaccines are safe and effective. Results of this study, however, differ from results from Canada, the UK, and Saudi Arabia, where COVID-19 vaccine confidence was higher ranging from 72% to 81%.Citation16–19 The differences in the proportion of confidence intervals may be explained by the methodological variations through which COVID-19 confidence was measured. While our study used the perception of COVID-19 effectiveness and safety as our composite measure of confidence, some included the importance and trust of the doctor’s recommendation apart from safety and effectiveness.Citation17,Citation18 Further, variation in the composition of socio-demographic characteristics may explain the lower levels of COVID-19 confidence in our study. Other studies were composed of a higher proportion of people with older age (mean of 50 years or higher) compared to participants in our study. Data on COVID-19 vaccine confidence are highly limited in the African context, only a protocol for its assessment exists in South Africa.Citation20
Different factors such as risk perception of COVID-19 and knowledge about the COVID-19 vaccine were found to influence confidence in the COVID-19 vaccines in this study. A study in Australia found that those perceiving themselves as at risk had increased confidence in the vaccine hence the likelihood of taking the vaccine.Citation15 Also, in a Canadian study, those who had a fear of the COVID-19 disease had 11% increased chances of having confidence in the COVID-19 disease.Citation17 Similarly, a qualitative study done among health care workers by Tibbels et al.Citation21 found that the high risk-perception increased their confidence in the vaccines’ effectiveness. These findings echo the results from our study whereby, community members perceiving themselves as at risk had 53% increased levels of COVID-19 vaccine confidence. Furthermore, having good knowledge was found to have 6.3 times the odds of having confidence in the COVID-19 vaccine compared to having poor knowledge. It is therefore evident that those with good knowledge of the vaccines are more likely than not to have confidence and be less hesitant in getting the vaccine. Risk perception and level of knowledge tend to influence an individual to decide on whether to vaccinate or not.Citation22 For this reason, the CDC has outlined education as one of its strategies to create vaccine demand and subsequently boost confidence in the vaccines to facilitate uptake among individuals.Citation23
Concerningly, our study found that those residing in rural areas had 27% significantly higher chances of having confidence in the vaccine than those in urban areas. There were also regional variations in vaccine confidence in the country. This could be explained by the fact that urban dwellers do have more access to the internet as a source of information compared to rural dwellers. Internet and social media being the main means of misinformation and disinformation spread, is likely to explain the observed findings. Higher levels of vaccine confidence in Kilimanjaro, Lindi, Mjini Magharibi, and Pemba Kaskazini may be explained by a comparatively higher vaccine uptake than in other regions included in this study. These findings emphasize the need for setting up specific educational campaigns to increase the level of knowledge, confidence, and COVID-19 vaccine uptake.Citation24
Males had higher odds of having COVID-19 vaccine confidence than women. Similar findings were reported in a study done in CanadaCitation17 and by Roy Rillera.Citation18 Females were less likely to have confidence in the COVID-19 vaccines because one of the misinformation in social media was the effect of the vaccine on fertility issues. Hence, addressing this misinformation at the community level is essential to bridge the gender gaps in vaccine uptake in Tanzania.
Importantly, confidence in the COVID-19 vaccines influenced uptake. According to the vaccine hesitancy model by SAGE, confidence is among the 3Cs (confidence, complacency, and convenience) that determines uptake or causes vaccine hesitancy.Citation1 Our study found that having confidence in the COVID-19 vaccines increases uptake by nearly four-fold compared to not having confidence. These findings were consistent with a study done in China whereby participants expressed confidence in the COVID-19 vaccines’ effectiveness in the protection of self and others.Citation25 In contrast, concerns about safety, side effects, and effectiveness, which reflect low confidence in the COVID-19 vaccines’ safety and effectiveness negatively impacted participants’ vaccination uptake in studies done in the UK,Citation16 Saudi Arabia,Citation19 India,Citation26 and Australia.Citation15 This emphasizes the need for multiple or combinations of interventions to improve confidence and knowledge in vaccines to target different groups in the population. These may include animated videos, short mobile messages, free telephone helplines, face-to-face campaigns, radios, and televisions, which have been shown to increase vaccine uptake.Citation27
Study strengths and limitations
The strength of the study lies in the involvement of general community members from different zones in the Tanzania mainland and Zanzibar. It also used a large sample size thus more likely to represent Tanzanian community members. Despite its strength, the study was faced with several limitations. The cross-sectional design limits making causal inferences. Second, we used two items to measure confidence, i.e. safety and effectiveness, while previous studies on childhood vaccine confidence used three items: importance, safety, and confidence.Citation2 We did not have a question on the vaccine importance in our data collection tool and hence might have under or overestimated the reported proportion of COVID-19 vaccine confidence.
Conclusion
In conclusion, only 54.6% of Tanzanian community members had confidence in COVID-19 vaccines. Knowledge of the vaccines, risk perception, and area of residence influenced confidence. There is a need for community engagement in improving comprehensive knowledge of the vaccine and addressing the misconceptions to improve vaccine uptake in the country. Further, there is a need to tailor interventions for specific regions due to the observed regional variations in the COVID-19 vaccine confidence. The need to address misconceptions about the effect of COVID-19 on women and fertility issues needs to be addressed.
Ethics statement
Ethical approval was obtained from the local review board at Kilimanjaro Christian Medical University College (KCMUCo) with approval number 2528 and was also requested from the National Institute for Medical Research (NIMR) and Zanzibar Medical Research and Ethics Committee (ZAMREC). Permission to collect data in Regions and Councils was obtained from the President’s Office – Regional Administration and Local Government (PO-RALG) in Tanzania mainland and the Ministry of Health (MoH) in Zanzibar. Regional and District Medical Officers gave permission to conduct the study in their respective communities. Verbal consent was obtained from each participant before the interviews. Participants were told they were free to withdraw consent at any time and for any reason, whether expressed or not. Interviews were conducted at participant households (quiet corners where quietness and privacy were sought).
Acknowledgments
The authors acknowledge their corresponding institutions for providing support to conduct the study. We recognize the cooperation of all the general community members who participated in this study. We acknowledge the support from the Ministry of Health, the President’s Office-Regional Administration and Local Government, the regional and district medical and vaccine officers, and the medical officers in charge of permission to conduct this study despite the challenges paused by the COVID-19 pandemic. We thank our research assistants for their dedication to conducting this study.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The datasets used in the present study are available from the corresponding author upon reasonable request only.
Additional information
Funding
References
- MacDonald N. The SAGE working group on vaccine hesitancy vaccine hesitancy: definition, scope and determinants. Vaccine. 2015;33:4161–8. doi:10.1016/j.vaccine.2015.04.036. PMID:25896383.
- Larson H, de Figuiredo A, Xiahong Z, Schulz W, Verger P, Johnston I, Cook A, Jones N. The state of vaccine confidence 2016: global insights through a 67-country survey. EBioMedicine. 2016;12:295–301. doi:10.1016/j.ebiom.2016.08.042.
- De Figueiredo A, Karafillakis E, Larson PHJ. State of vaccine confidence in the EU+UK 2020. (Report ECDC). European Commission; 2020. doi:10.2875/06196.
- Hanley SJB, Yoshioka E, Ito Y, Kishi R. HPV vaccination crisis in Japan. Lancet. 2015;385:2571. doi:10.1016/S0140-6736(15)61152-7.
- Brown K, Kroll S, Hudson M, Ramsay M, Green J, Long S, Vincent C, Fraser G, Sevdalis N. Factors underlying parental decisions about combination childhood vaccinations including MMR: a systematic review. Vaccine. 2010;28:4235–48. doi:10.1016/j.vaccine2010.04.052. PMID: 20438879.
- World Health Organization. Ten Threats to global health in 2019. Geneva (Switzeland): World Health Organization; 2019. https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- World Health Organization. COVID-19 advice for the public: getting vaccinated. Geneva (Switzeland): World Health Organization; 2022 [accessed 2022 Nov 24]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice.
- Word Health Organization. Africa needs to ramp up COVID-19 vaccination six-fold | WHO | regional office for Africa; 2022 [accessed 2022 Jul 26]. https://www.afro.who.int/news/africa-needs-ramp-covid-19-vaccination-six-fold.
- OurWorldInData. Total Covid-19 doses administered per 100 people. England and Wales: OurWorldInData; 2022 [accessed 2022 Jul 24]. https://ourworldindata.org/grapher/covid-vaccination-doses-per-capita.
- Mundagowa PT, Tozivepi SN, Chiyaka ET, Mukora-Mutseyekwa F, Makurumidze R. Assessment of COVID-19 vaccine hesitancy among Zimbabweans: a rapid national survey. medRxiv 2021.06.24.21259505; 2021. doi:10.1101/2021.06.24.21259505.
- Voice of Africa. Tanzania president launches COVID-19 vaccination campaign. Africa: Voice of Africa; 2021 [accessed 2023 Feb 21]. https://www.voanews.com/a/covid-19-pandemic_tanzania-president-launches-covid-19-vaccination-campaign/6208855.html.
- Chilongola JO, Rwegoshola KM, Balingumu OH, Semvua HS, Kwigizile ET. COVID-19 knowledge, attitudes, practices, and vaccination hesitancy in Moshi, Kilimanjaro Region, Northern Tanzania. Tanzan J Health Res. 2022;23:1–12. doi:10.4314/thrb.v23i1.3.
- World Health Organization. WHO and partners welcome new drive to push COVID-19 vaccination | WHO | regional office for Africa; 2022 [accessed 2022 Jul 26]. https://www.afro.who.int/countries/united-republic-of-tanzania/news/who-and-partners-welcome-new-drive-push-covid-19-vaccination.
- Msuya S, Manongi R, Jonas N, Mtei M, Amour C, Mgongo M, Bilakwate J, Amour M, Kalolo A, Kapologwe N, et al. COVID-19 vaccine uptake and associated factors in Sub-Saharan Africa: evidence from a community-based survey in Tanzania. Vaccines. 2023;11:1–13. doi:10.3390/vaccines11020465.
- Enticott J, Gill J, Bacon S, Lavoie K, Epstein D, Dawadi S, Teede H, Boyle J. Attitudes towards vaccines and intention to vaccinate against COVID-19: a cross-sectional analysis - implications for public health communications in Australia. BMJ Open. 2022;12:e057127. doi:10.1136/bmjopen-2021-057127.
- Roberts C, Brindle H, Rogers N, Eggo R, Enria L, Lees S. Vaccine confidence and hesitancy at the start of COVID-19 vaccine deployment in the UK: an embedded mixed-methods study. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.745630.
- Nizigiyimana A, Acharya D, Morillon GF, Poder TG. Predictors of vaccine acceptance, confidence, and hesitancy in general, and COVID-19 vaccination refusal in the Province of Quebec, Canada. Patient Prefer Adherence. 2022;16:2181–202. doi:10.2147/PPA.S376103. PMID 36003798.
- Marzo R, Sami W, Alam Z, Acharya S, Jermsittiparsert K, Songwathana K, Pham N, Respati T, Faller E, Baldonado A, et al. Hesitancy in COVID-19 vaccine uptake and its associated factors among the general adult population: a cross-sectional study in six Southeast Asian countries. Trop Med Health. 2022;4:1–10. doi:10.1186/s41182-021-00393-1.
- Barry M, Temsah M, Alhuzaimi A, Alamro N, Al-Eyadhy A, Aljamaan F, Saddik B, Alhaboob A, Alsohime F, Alhasan K, et al. COVID-19 vaccine confidence and hesitancy among health care workers: a cross-sectional survey from a MERS-CoV experienced nation. PLoS One. 2021;16:1–16. doi:10.1371/journal.pone.0244415.
- Oduwole EO, Mahomed H, Ayele BT, Wiysonge CS. Estimating vaccine confidence levels among healthcare students and staff of a tertiary institution in South Africa: protocol of a cross-sectional survey. BMJ Open. 2021;11:e049877. doi:10.1136/bmjopen-2021-049877. PMID:33986069.
- Tibbels N, Dosso A, Fordham C, Benie W, Brou J, Kamara D, Hendrickson Z, Naugle D. “On the last day of the last month, I will go”: a qualitative exploration of COVID-19 vaccine confidence among Ivoirian adults. Vaccine. 2022;40:2028–35. doi:10.1016/j.vaccine.2022.02.032.
- Du M, Tao L, Liu J. The association between risk perception and COVID-19 vaccine hesitancy for children among reproductive women in China: an online survey. Front Med. 2021;8:1–10. doi:10.3389/fmed.2021.741298. PMID:34568394.
- Centres for Disease Control. Building confidence in COVID-19 vaccines. U.S: centres for disease control and prevention; 2022 [accessed 2022 Jul 10]. https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence.html.
- Njoga E, Awoyomi O, Onwumere-Idolor O, Owoyomi P, Igochukwu I, Ozioko S. Persisting vaccine hesitancy in Africa: the whys, global public health consequences and ways-out—COVID-19 vaccination acceptance rates as case-in-point. Vaccines. 2022;10:1934. doi:10.3390/vaccines10111934.
- Wong CL, Leung AWY, Chung OMH, Chien WT. Factors influencing COVID-19 vaccination uptake among community members in Hong Kong: a cross-sectional online survey. BMJ Open. 2022;12:1–11. doi:10.1136/bmjopen-2021-058416. PMID:35217543.
- Mitali S, Smitta D, Arijit R. Knowledge, attitude and practice survey towards COVID-19 vaccination: a mediation analysis. Int J Health Plann Manage. 2022;4:2063–80. doi:10.1002/hpm.3449. PMID: 35229357.
- Davis CJ, Golding M, McKay R. Efficacy information influences intention to take COVID-19 vaccine. Br J Health Psychol. 2022;27:300–19. doi:10.1111/bjhp.12546. PMID: 34250684.